
Abstract
Purpose
A systematic review regarding clinical studies on Hegemann’s disease and fishtail deformity was performed with the aims to: (1) formulate the most up-to-date theory on aetiology in order to better define these conditions, (2) summarise the most frequent radiographic descriptions on radiographs and (3) give an overview of different treatment options.
Methods
A systematic review of studies to date on Hegemann’s disease and fishtail deformity was performed. Studies were eligible if: (1) the article provides a description of Hegemann’s disease or fishtail deformity, (2) original data of at least one patient was available, (3) the article was written in English, German or Dutch and (4) a full manuscript was available. Animal studies, reviews and expert opinions were not included.
Results
We included a total of 22 articles: seven regarding Hegemann’s disease including eight patients and 15 regarding fishtail deformity including 58 patients.
Conclusions
Fishtail deformity and Hegemann’s disease seem to be a spectrum of vascular disorders of the distal humerus, varying from a benign mild vascular disorder to a complete avascular necrosis after fractures. Additional imaging is advised to confirm the presence of a fishtail deformity, intra-articular loose bodies and signs of osteoarthritis to decide if, and what, operative treatment is needed. As long as no clear aetiology for both diseases exist and the clinical symptoms and radiographic appearance are difficult to distinguish, both entities should preferably be named as ‘vascular disturbance of the trochlear growth plate’ to overcome confusing definitions and discussions.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Osteochondrosis is used to describe more than 50 different conditions affecting the immature skeleton [1]. In 1951, Dr. Gerd Hegemann described the radiographic changes of the humeral trochlea in the young adult; therefore, osteochondrosis of the humeral trochlea is known as Hegemann’s disease [2]. Studies so far report that osteochondrosis goes through stages, similar to Perthes' disease [3]. Reports on patients with Hegemann’s disease are very rare [2]. Fishtail deformity of the elbow is a rare complication after fracture of the distal humerus, usually following a supracondylar, a lateral condyle, a medial condyle or even after Salter–Harris type I epiphyseal fractures in childhood [4].
Aetiology as well as optimal treatment for Hegemann’s disease and fishtail deformity are subjects of ongoing debate. A systematic review regarding clinical studies on Hegemann’s disease and fishtail deformity was performed with the aims to: (1) formulate the most up-to-date theory on aetiology in order to better define these conditions, (2) summarise the most frequent radiographic descriptions on radiographs and (3) give an overview of different treatment options.
Materials and methods
Search strategy
To identify studies focusing on Hegemann’s disease and fishtail deformity, the following databases (up to 27th August 2014) were searched: EMBASE, MEDLINE OvidSP, Web of Science, Cochrane Central, PubMed Publisher, Scopus and Google Scholar (Table 1). The EMBASE search strategy was transferred into similar search strategies for the other databases. References of the included articles were also searched to identify more potentially relevant literature.
Study selection
Study selection was assessed by two independent reviewers (FC and JL). Disagreements were solved by consensus. If no consensus was reached, a third reviewer (MB) solved the disagreement. Studies were eligible if: (1) the article provides a description of Hegemann’s disease and/or fishtail deformity, (2) original data of at least one patient were available, (3) the article was written in English, German or Dutch and (4) a full-text article was available. Animal studies, (systematic) reviews and expert opinions were not included.
Methodological quality assessment
Two reviewers (FC and JL) independently assessed the methodological quality of all the included studies. Important aspects of methodology were noted: study design, follow-up time and outcomes, e.g. because all studies were case reports, no pre-printed selection forms or an overall scoring system to evaluate methodological quality was used [5].
Data extraction
Data extraction was performed by the first author (FC). The following data were extracted: study population, patient characteristics, design of study, aetiology, clinical presentation and physical examination, radiological evaluation, treatment and outcome measures.
Results
Literature search
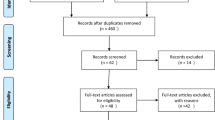
A total of 22 studies were included in the current review (Fig. 1), comprising seven studies regarding Hegemann’s disease and 15 studies regarding fishtail deformity.

Flow diagram of the study selection and exclusion stages
Hegemann’s disease
Seven case reports regarding Hegemann’s disease, including eight patients, were analysed [1, 2, 6–10]. The study and patient characteristics are shown in Table 2.
Aetiology
In six case reports, the aetiology of Hegemann’s disease was described [1, 2, 6–9]. Two cases reported contusion of the elbow (25 %) [2, 7] and in two patients, a fracture in the past history was described (25 %) [1, 7]. In two patients, no trauma were reported in the history (25 %) [9, 10] and in one case, Hegemann’s disease presented in a gymnast (13 %) [8].
Patient characteristics
In all eight case reports, the patient characteristics were described. Seven of the eight patients were male (88 %) and the average age was 11 years (range 7–15 years).
Clinical presentation and physical examination
All included studies described the symptoms and findings at physical examination. In five patients, a swelling of the elbow was noted (50 %) [2, 6, 7]. Pain in the elbow was presented in five patients (63 %) [2, 6, 7, 9]. A limited range of motion at presentation was described in all seven case reports (100 %), and an extension contracture of about 15° at presentation was seen in four patients (50 %) [7–9]. In one patient, progressive bowing of the elbow was noted (13 %) [10]. Beyer et al. described a patient with a 15° flexion limitation and 20° varus deformity (13 %) [1]. In one patient, a flexion and extension limitation at presentation was noted (13 %) [6].
Radiological evaluation
In all reports, conventional radiography was used for diagnosing Hegemann’s disease. Irregularity of the trochlea was described in six patients (75 %) [2, 6–9] and sclerosis of the trochlea was shown in three case reports (38 %) [6, 9, 10]. Szepesi noted a fragmented trochlea (13 %) [9]. Irregularity of the epiphysis was seen in two patients (22 %) [6, 9]. Flattening of the trochlear ossific nucleus was described in one patient (11 %) [10]. Beyer et al. [1] noted osteolysis of the trochlea (11 %), and in the patient reported by Martin and Ehrenpfordt, a progressive increase of trochlea surface was seen (13 %) [7].
Treatment
In four case reports, the treatment for Hegemann’s disease was described. A conservative treatment was recommended [2, 6, 7, 9]. In three patients, rest was described as the treatment for Hegemann’s disease (60 %) [7, 9]. Szepesi advised less physical activities, Martin and Ehrenpfordt recommended less movement and Ito et al. advised to avoid vigorous sports activities by the epiphyseal closure and to avoid certain forms of sports involving hanging and throwing exercises [6, 7, 9].
Outcome (measures)
Six case reports described the outcome measurements. The average follow-up time was 32 months (range 12–16 months).
Radiography was used as an outcome measurement in all six studies [1, 2, 6, 7, 9, 10]. In one patient, a reduced size of the trochlea, with the radius being longer than the ulna at the proximal radio-ulnar joint, was shown (17 %) [6].
Clinical symptoms were used as an outcome measurement in five patients [2, 6, 7, 9]. No elbow pain after treatment was reported in four patients (80 %) [6, 7, 9], although Hegemann described a case in which the patient still had intermittent pain (17 %) [2].
In two patients, function of the elbow was used as the outcome measurement [2, 9]. In the case presented by Hegemann, a range of motion restriction still existed [2] and loss of extension of the elbow was shown in one patient [9].
Fishtail deformity
Fifteen case reports regarding fishtail deformity including 58 patients were analysed [11–25]. The study and patient characteristics are shown in Table 3.
Patient characteristics
In all case reports, the patient characteristics were described. The average age at injury was 7.8 years (range 2–15 years) [12–17, 21–24]. In nine studies, the sex of the patient was noted [12, 13, 16, 17, 20–23, 25]. Most patients were male (74 %). Twenty-eight patients had a lateral humeral condyle fracture (48 %) [11, 13–15, 17, 18, 20, 24], 18 patients had a supracondylar fracture (31 %) [11, 16, 17, 21, 22], three patients had a capitellum fracture (5 %) [12], three patients had a medial humeral condyle fracture (5 %) [21, 23, 25], one patient had an external humeral condyle fracture (2 %) [19], in four patients the exact location of the fracture was unknown (7 %) [17, 21] and in one patient the injury is unknown (2 %) [17]. The average follow-up time was 69 months [12–21, 23–25].
Clinical presentation and physical examination
In only one study was the clinical presentation and physical examination described [17]. Pain and limited range of motion was shown in 12 of the 14 patients evaluated in this study (86 %). Varus alignment was noted in five patients (range 3–8°), valgus in six patients (range 6–18°) and neutral in three patients. The average loss of extension is 12° (range 0–40°) and the average flexion loss is 11° (range 0–40°).
Radiological evaluation
In all studies, a radiograph was done to diagnose fishtail deformity [11–25]. Computed tomography (CT) and magnetic resonance imaging (MRI) are advised to diagnose the severity of fishtail deformity and its complications [17].
Treatment
Only one study described the treatment for fishtail deformity [17]. Glotzbecker et al. [17] recommended observational therapy in patients with a range of motion of 25–130° and minimal pain. In the case of progressive pain or increase in loss of range of motion, painful cracking symptoms or presence of symptomatic loose bodies, arthroscopic joint debridement was advised.
Outcome (measures)
In all 15 studies, radiographs are used to measure the fishtail deformity [11–25]. The average follow-up time was 69 months (range 18–168 months). Range of motion was used as the outcome measure in seven studies [12, 14, 16, 19, 21, 24, 25]. Loss of extension was seen in 12 patients (67 %) [12, 14, 16, 21, 25] and a valgus deformity was seen in seven patients (39 %) [12, 14, 16, 18, 24]. Clinical symptoms were described in 11 patients [13, 16, 21, 24]. Movement pain was seen in seven patients (64 %) [13, 16, 21], a cracking joint was shown in two patients (18 %) [16] and an arm length difference was seen in one patient (9 %) [21].
Glotzbecker et al. recommended conservative treatment for patients with a small impairment of range of motion and a symptomatic cracking of the joint. For the patients with progressive pain or increase in loss of range of motion, painful cracking symptoms or presence of symptomatic loose bodies, operative debridement was advised. In the operated patients, pain relief was seen in 85 % of the patients, and in 100 % of the patients, an increase in range of motion was noticed, with an average gain of 35° (range 25–50°) [17].
Discussion
Reports on patients with Hegemann’s disease and fishtail deformity are very rare.
To our knowledge, this systematic review regarding Hegemann’s disease and fishtail deformity is the first to summarise current knowledge on aetiology, radiographic findings and different treatment modalities.
Studies so far report that osteochondrosis goes through stages, similar to Perthes’ disease [3]. The aetiology of Hegemann’s disease remains unclear, although traumatic events may play a role, as in five of eight cases, a contusion, fracture or chronic repetitive micro-trauma are described. It is known that traumatic events in children may sometimes be overlooked or under-reported; therefore, a traumatic origin in the other three cases may play a role as well [26].
The trochlear epiphysis ossification centre appears after 5 years of age and develops between 8 and 13 years of age in boys. The ossification centre fuses with the metaphysis of the humerus between 13 and 16 years of age [6, 27]. The trochlear blood supply comes from two end arterioles. The lateral aspect of the medial crista, the trochlear groove and the trochlear apex are relatively hypovascular. So those structures are prone to disturbances in the blood supply and the development of avascular necrosis [4]. Trochlear avascular necrosis is characterised by disturbance of growth involving the centres of ossification of the trochlea. Therefore, fishtail deformity could be a result of avascular necrosis of the vessels supplying the lateral trochlea [4, 28]. If the lateral trochlear ossification centre development is disturbed and the remaining normal physis continues to grow, the distal humerus assumes a typical V shape: the fishtail [4, 21].
Hegemann’s disease is often diagnosed by radiography months or years after trauma [7, 10, 29]. This makes Hegemann’s disease prone to confusion with a ‘fishtail deformity.’ Fishtail deformity of the elbow is an uncommon complication usually following a distal humeral fracture in childhood [4]. Usually, the term ‘Hegemann’s disease’ is used for spontaneous or idiopathic osteonecrosis of the humeral trochlea. You can question if a disease can be called Hegemann’s disease if it is not of idiopathic origin.
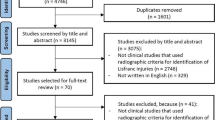
In all reports, standard radiographs were used for diagnosing Hegemann’s disease and fishtail deformity. There is no gold standard for diagnosing Hegemann’s disease and fishtail deformity. However, signs of fishtail deformity are shown earlier on CT and MRI, although at the time Hegemann’s disease was first diagnosed neither CT nor MRI were available. Therefore, the fishtail deformity could be another (next) stage of Hegemann’s disease, which is benign after a mild vascular disorder. A complete avascular necrosis could develop after traumatic events. Alternatively Hegemann’s disease is a benign, self-limiting stage of fishtail deformity after unrecognised injury or (repetitive) micro-trauma. Hegemann’s disease is characterised by irregularity of the trochlea and sclerosis. Schumacher et al. [30] classified Hegemann’s disease into five different stages based on radiographs: stage 1: initial loss of density and later plaque-shaped sclerosis of the centre of epiphyseal ossification; stage 2: reduction in size and condensation of the ossification centre; stage 3: loosening, accompanied by onset of new ossification; stage 4: regeneration and enlargement of the ossification centre; and stage 5: final stage (complete or partial recovery) (Fig. 2). A central deficiency of the distal humeral epiphysis is characteristic for fishtail deformity [4]. Radiographs should always be compared to the asymptomatic elbow, as the appearance of the growth plate of the trochlea differs between individuals.

Stages of Hegemann’s disease
Whilst Hegemann’s disease was initially presumed to be a benign condition, in four of the six cases where follow-up was done, no full recovery was seen. In early stages, rest and a total ban on all sports activities and exemption from participation in certain forms of sport involving hanging, propping and throwing exercises, together with apparatus gymnastics, have been advised until the epiphysis is closed. It is questionable if a total ban on all physical activities is mandatory in these young children; possibly, a symptom-related adjustment of activities could be enough. CT and MRI scans are helpful to confirm the presence of a premature fishtail deformity, intra-articular loose bodies and signs of osteoarthritis. If intra-articular loose bodies are found and occur with locking symptoms of the elbow, arthroscopic debridement may be indicated. Long-term follow-up studies showed that patients with fishtail deformity are probably prone to functional impairment, ongoing pain and the development of early osteoarthritis [16, 21]. It is unknown whether or not early arthroscopic debridement of the joint prevents osteoarthritis in the future.
Based on this systematic review, many aetiological aspects of Hegemann’s disease and fishtail deformity remain unclear. It is presumable that fishtail deformity is a stage of Hegemann’s disease or Hegemann’s disease is a benign stage of fishtail deformity after unrecognised injury or (repetitive) micro-trauma. Additional imaging is advised to confirm the presence of a premature fishtail deformity, intra-articular loose bodies and signs of osteoarthritis to decide if operative treatment is indicated.
There are several weaknesses in the included studies of this systematic review. The review is based on case reports, and the number of included patients in each study was low and, therefore, the strength of evidence is limited by the quality of the available studies.
Since Hegemann’s disease and fishtail deformity are very rare, higher quality studies are not likely to be performed and, thus, this systematic review provides the best level of evidence on what is known about Hegemann’s disease.
Conclusion
Future studies on Hegemann’s disease and fishtail deformity should ideally investigate the aetiology to prevent those diseases. As long as no clear aetiology for both diseases exist and the clinical symptoms and radiographic appearance are difficult to distinguish, both entities should preferably be named a ‘vascular disturbance of the trochlear growth plate’ to overcome confusing definitions and discussions.
References
Beyer WF, Heppt P, Glückert K, Willauschus W (1990) Aseptic osteonecrosis of the humeral trochlea (Hegemann’s disease). Arch Orthop Trauma Surg 110(1):45–48
Hegemann G (1951) Spontaneous aseptic bone necrosis of the elbow. Fortschr Geb Rontgenstr 75(1):89–92
Davidsson L, Halme EA (1964) Osteochondrosis of the capitulum humeri (Panner’s disease). Ann Chir Gynaecol Fenn 53:156–159
Hayter CL, Giuffre BM, Hughes JS (2010) Pictorial review: ‘fishtail deformity’ of the elbow. J Med Imaging Radiat Oncol 54(5):450–456
Kwan J, Sandercock P (2004) In-hospital care pathways for stroke. Cochrane Database Syst Rev. 4:CD002924. doi:10.1002/14651858.CD002924.pub2
Ito K, Ogino T, Aoki M, Wada T, Ishii S (2004) Growth disturbance in aseptic osteonecrosis of the humeral trochlea (Hegemann’s Disease): a case report with developmental distal radioulnar joint incongruency. J Pediatr Orthop 24(2):201–204
Martin F, Ehrenpfordt A (1984) Aseptic necrosis of the trochlea of the humerus (Hegemann disease). Beitr Orthop Traumatol 31(5):261–267
Mueller B, Haehnel H (1976) Osteochondropathies in children and adolescents taking part in gymnastics. Med Sport 16(10):325–332
Szepesi K (1971) Ein Fall einer zweiseitigen Osteochondritis juvenilis der Trochlea Humeri. Arch Orthop Trauma Surg 70(4):340–343. doi:10.1007/BF00416454
Osebold WR, El-Khoury G, Ponseti IV (1977) Aseptic necrosis of the humeral trochlea: a case report. Clin Orthop Relat Res 127:161–163
McDonnell DP, Wilson JC (1948) Fractures of the lower end of the humerus in children. J Bone Joint Surg Am 30A(2):347–358
Wadsworth TG (1964) Premature epiphysial fusion after injury of the capitulum. J Bone Joint Surg Br 46:46–49
Jakob R, Fowles JV, Rang M, Kassab MT (1975) Observations concerning fractures of the lateral humeral condyle in children. J Bone Joint Surg Br 57(4):430–436
Rutherford A (1985) Fractures of the lateral humeral condyle in children. J Bone Joint Surg Am 67(6):851–856
Skak SV, Olsen SD, Smaabrekke A (2001) Deformity after fracture of the lateral humeral condyle in children. J Pediatr Orthop B 10(2):142–152
Bronfen CE, Geffard B, Mallet JF (2007) Dissolution of the trochlea after supracondylar fracture of the humerus in childhood: an analysis of six cases. J Pediatr Orthop 27(5):547–550
Glotzbecker MP, Bae DS, Links AC, Waters PM (2013) Fishtail deformity of the distal humerus: a report of 15 cases. J Pediatr Orthop 33(6):592–597
Amgwerd M, Sacher P (1990) Treatment of fractures of the radial condyle of the humerus in children. Z Unfallchir Versicherungsmed 83(1):49–53
Valdiserri L, Venturi B, Busanelli L (1993) External humeral condylar fracture in children. A long-term review of 30 cases operated. Chir Organi Mov 78(2):105–109
Hasler C, von Laer L (1998) Screw osteosynthesis in dislocated fractures of the radial condyle of the humerus in the growth period. A prospective long-term study. Unfallchirurg 101(4):280–286
Nwakama AC, Peterson HA, Shaughnessy WJ (2000) Fishtail deformity following fracture of the distal humerus in children: historical review, case presentations, discussion of etiology, and thoughts on treatment. J Pediatr Orthop B 9(4):309–318
Schulte DW, Ramseier LE (2009) Fishtail deformity as a result of a non-displaced supracondylar fracture of the humerus. Acta Orthop Belg 75(3):408–410
Namba J, Tsujimoto T, Temporin K, Yamamoto K (2011) Medial condyle fracture of the distal humerus in an adolescent with pre-existing fishtail deformity. A case report. Emerg Radiol 18(6):507–511. doi:10.1007/s10140-011-0985-0
Cates RA, Mehlman CT (2012) Growth arrest of the capitellar physis after displaced lateral condyle fractures in children. J Pediatr Orthop 32(8):e57–e62. doi:10.1097/BPO.0b013e31826bb0d5
Sağlam N, Saka G, Kurtulmuş T, Cem Coşkun A, Türker M (2014) Medial humeral condyle fractures in adolescents: treatment and complications. Eur J Orthop Surg Traumatol 24(7):1101–1105. doi:10.1007/s00590-013-1288-9
Arundel D, Williams P, Townend W (2014) Deriving the East Riding Elbow Rule (ER2): a maximally sensitive decision tool for elbow injury. Emerg Med J 31(5):380–383. doi:10.1136/emermed-2012-202169
Haraldsson S (1959) On osteochondrosis deformas juvenilis capituli humeri including investigation of intra-osseous vasculature in distal humerus. Acta Orthop Scand Suppl 38:1–232
Marshall KW, Marshall DL, Busch MT, Williams JP (2009) Osteochondral lesions of the humeral trochlea in the young athlete. Skeletal Radiol 38(5):479–491
Okuda K, Takahara M, Onda K (1965) Koehler’s disease and Panner’s disease. Rinsho Hoshasen 10:172–173
Schumacher R, Müller U, Schuster W (1981) Rare localisation of osteochondrosis juvenilis (author’s transl). Radiologe 21:165–174
Acknowledgements
The authors thank W. Bramer, medical librarian of the Erasmus Medical Center, and B. Berenschot, medical librarian of the Onze Lieve Vrouwe Gasthuis, for their assistance in performing the literature search. No sources of funding were used to assist in the preparation of this review. The authors have no potential conflicts of interest that are directly relevant to the content of this review. FMAP Claessen has received an unrestricted research grant from the Prins Bernhard Cultuurfonds foundation, Trust Foundation, VSB Foundation and Van Beek-Donner Foundation. For the remaining authors, none were declared.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Claessen, F.M.A.P., Louwerens, J.K.G., Doornberg, J.N. et al. Hegemann’s disease and fishtail deformity: aetiopathogenesis, radiographic appearance and clinical outcome. J Child Orthop 9, 1–8 (2015). https://doi.org/10.1007/s11832-014-0630-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11832-014-0630-z