
Abstract
Purpose
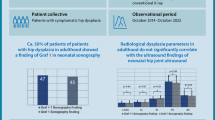
One goal of neonatal screening for developmental dysplasia of the hip (DDH) is the prevention of late surgery. However, the majority of patients with acetabular dysplasia at skeletal maturity are not diagnosed with DDH during infancy. Selective ultrasound screening may identify patients with neonatal hip instability, but may be ineffective for the prevention of dysplasia presenting in adulthood. The purpose of this study is to identify the prevalence of risk factors for DDH that would have warranted selective ultrasound screening in patients with symptomatic acetabular dysplasia after skeletal maturity.
Methods
A prospective hip specialty center registry was used to identify 68 consecutive skeletally mature patients undergoing corrective osteotomy for symptomatic acetabular dysplasia. Risk factors for DDH evaluated in all patients included sex, family history of hip osteoarthritis or DDH, breech, method of delivery, previous hip treatments, and birth order. Radiographs [lateral center edge angle (CEA), anterior CEA, Tönnis grade, and Tönnis angle] were measured preoperatively.
Results
Sixty-seven females and one male were identified. No patients were previously diagnosed with DDH or received treatment for their hips. The majority of patients (85.3 %) did not meet selective ultrasound screening guidelines following a stable neonatal hip exam and, therefore, would not have been screened in a selective screening program. Of the findings outside of screening guidelines, 98.5 % were females, 52.9 % were first born, and 36.8 % had a family history of hip osteoarthritis.
Conclusions
The majority (85.3 %) of patients with symptomatic acetabular dysplasia at skeletal maturity would not have met current recommendations for selective ultrasound screening in the USA had they been born today.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Acetabular dysplasia is a common cause of hip osteoarthritis and the most common cause of hip arthroplasty in women younger than 50 years of age. [1, 2]. Hip instability and acetabular dysplasia affects up to 4 % of newborn infants [3–6]. Untreated or undetected developmental dysplasia of the hip (DDH) may result in abnormal acetabular development during infancy, and this may lead to an increased risk of symptomatic acetabular dysplasia at later ages [7, 8]. Neonatal hip screening protocols, including both physical examination and/or imaging studies, have been implemented in many countries to promote early diagnosis of DDH, allowing for less invasive treatments, and possibly reducing the rate of late open surgery [5–11]. Some centers recommend universal screening to further decrease the burden of hip dysplasia in later life [7, 8].
Serial clinical examination is widely accepted for all newborns to improve early detection of DDH; however, recommendations for ultrasound screening have considerable regional variation [5, 6, 9]. Selective ultrasound screening in high-risk newborns following a normal neonatal examination has been recommended in the USA by organizations such as the American Academy of Pediatrics (AAP) as an alternative to universal ultrasound screening [9, 12, 13]. Selective secondary ultrasound screening is specifically recommended for infants born in the breech position or with a positive family history for DDH. The reports of selective screening are mixed: some studies indicate a decrease in late dysplasia surgery, while others conclude no effect on the incidence of late surgery compared to physical exam alone [6, 12, 14, 15]. Additionally, some series have concluded that a large percentage of children with the need for late open surgery would be missed by current selective screening recommendations [10, 15, 16].
The majority of current studies have focused on the impact of selective ultrasound screening on late surgery in skeletally immature patients. The effect of selective ultrasound screening on operative intervention for dysplasia identified at skeletal maturity has been less frequently studied [3, 5, 7, 8, 14, 15, 17–20]. The purpose of this study is to identify the prevalence of risk factors for neonatal DDH that would have warranted selective ultrasound screening in a consecutive series of skeletally mature patients with symptomatic acetabular dysplasia.
Materials and methods
Patients were enrolled in this study through our prospective single-center hip preservation registry, which was established at our institution in March 2010. We serve as a tertiary referral center for hip disorders and hip preservation surgery. All patients undergoing surgery, including hip arthroscopy, periacetabular osteotomy (PAO), femoral osteotomy, and surgical hip dislocation (SHD), are enrolled prospectively from four surgeons performing procedures at our institution. Patients with symptomatic acetabular dysplasia presenting between June 2011 and December 2013 were eligible for this study. Radiographic criteria for acetabular dysplasia utilized in this cohort were a lateral center edge angle (CEA) on the anteroposterior radiograph ≤20° and/or an anterior CEA ≤20° on the false-profile radiograph. Exclusion criteria included patients with neuromuscular dysplasia, teratologic hip dislocation, or inability to confirm birth history.
Based on our inclusion criteria, we retrospectively identified a consecutive series of 68 skeletally mature patients recommended to have corrective osteotomy for symptomatic hip dysplasia. The surgical decision was based on a careful history, exam, plain radiographs, magnetic resonance imaging (MRI), and computed tomography (CT) scan to confirm hip dysplasia as the etiology of hip symptoms. Prospective data were collected at the time of initial consultation from all patients including a questionnaire regarding their birth history and risk factors for DDH including: family history of hip pain in first- or second-degree relatives, hip surgery, or DDH; whether they were breech, method of delivery, previous treatment or surgery on their hips, and birth order. A follow-up call was performed to confirm this documented history prior to the study.
Radiographic studies (radiographs, MRI, and CT) were analyzed for each patient at the time of their initial consultation. Patients with a lateral CEA, anterior CEA, Tönnis grade, and Tönnis angle were recorded by the interviewing surgeon (ELS) from plain radiographs in a standard fashion.
Continuous variables are presented as the mean ± standard deviation or mean (range), as indicated. Categorical variables are presented as the percentage of the total cohort as having the described features (SAS version 9.3, SAS Institute, Cary, NC).
Results
There were 68 patients included in the study (Table 1). The average age was 26.4 years (range 13–47 years). There were 67 (98.5 %) females and 1 (1.5 %) male. The left hip presented as the symptomatic hip in 21 (30.9 %) cases, and the right hip in 47 (69.1 %) cases. The duration of pain was 6 months to 288 months (median 24 months). The mean lateral CEA was 14.7 ± 6.2° and the mean anterior CEA was 14.5 ± 9.3° (Table 2). The Tönnis grade was zero in 48.5 %, one in 41.2 %, and two in 10.3 %. The mean Tönnis angle was 16.8 ± 6.5°.
The questionnaire results about risk factors for hip disease are shown in Table 3. Eight patients (11.8 %) were confirmed breech. A family history of DDH was present in two additional patients (2.9 %). Therefore, current guidelines would recommend selective ultrasound screening in 10/68 patients (14.7 %) of this cohort.
Characteristics that were identified but are not current indications for selective ultrasound screening included 36 patients (52.9 %) that were first born, 25 patients (36.8 %) with a family history of hip osteoarthritis in a first- or second-degree relative (but not confirmed by the family as DDH), and 5 patients (7.4 %) who were born premature. Despite the presence of symptomatic hip dysplasia at skeletal maturity, no patients in this series were diagnosed with DDH as children or received any treatment for their hips.
Discussion
Skeletally mature patients with symptomatic acetabular dysplasia, despite current protocols for early identification and treatment of DDH, may result from inadequate infantile screening methods, inadequate screening protocols, or treatment failure. It is also possible that adult acetabular dysplasia represents a different disease process than infantile DDH, with a later onset of development outside of the current screening period [21, 22]. In this consecutive series of skeletally mature hips with symptomatic acetabular dysplasia, only 10/68 patients (14.7 %) had risk factors for DDH at birth that would be evaluated by current selective ultrasound screening recommendations in neonates with a stable hip exam. Therefore, 85.3 % of the patients in this cohort would have been undetected by current selective ultrasound screening recommendations.
The overall goal of screening is to decrease the incidence of late acetabular dysplasia and hip instability that requires surgical treatment. Early diagnosis of DDH in the newborn period allows less invasive treatment such as Pavlik harness, and this may decrease the risk of future invasive surgery for acetabular dysplasia [8, 11, 19, 20, 23]. Early detection and intervention of neonatal DDH may decrease the risk for development of acetabular dysplasia in skeletally mature patients. The role of selective ultrasound screening in patients with risk factors remains controversial. In 2006, the US Preventive Services Task Force concluded, based on its systematic review, that there was not enough evidence to recommend routine screening in the neonatal period (clinical or ultrasound) [11]. The Canadian task force reported that routine clinical exam in the newborn period for hip instability decreased late operative rates; however, the addition of selective ultrasound screening did not result in further reductions [6]. Recently, Sanghrajka et al. [10] reported a series of patients treated with late surgery at their center in England and concluded that only a minority of patients (23 %) would have been identified using selective ultrasound screening based on risk factors. Cost-effectiveness is critical to any screening protocols. A decision analysis study by Mahan et al. [13] suggested that selective ultrasound screening (breech, family history of DDH) with universal physical examination screening may be the most cost-effective strategy in the USA, unless the rate of missed dysplasia was greater than 4/1,000.
Current screening recommendations may have little impact on changing the incidence of symptomatic acetabular dysplasia after skeletal maturity. Breech position and family history of DDH are the two major risk factors included in recommendations for selective screening in the USA [9, 11, 24–26]. In our study, patients with acetabular dysplasia at skeletal maturity rarely reported a positive family history of DDH (2/68 patients). In contrast, a family history of hip osteoarthritis in any first- or second-degree relative was common in this population (25/68). This is consistent with the findings of Schiffern et al. [27] and Lee et al. [21], which suggest an increased association of hip osteoarthritis amongst first- and second-degree relatives of patients with acetabular dysplasia. Expanding the definition from a family history of DDH to any family history of hip pain and osteoarthritis in first- and second-degree relatives may increase the percentage of neonatal diagnoses with selective screening. Another major risk factor in DDH is female sex [11, 24]. Our cohort of patients with adult dysplasia requiring treatment was almost exclusively female. Expanding current selective ultrasound screening protocols to include all females, or at least all first-born females, may increase early identification of these patients. Male patients are less likely to need treatment after selective or general ultrasound screening; thus, expanding screening in males beyond current recommendations appears unnecessary [28, 29].
Another possible explanation for acetabular dysplasia after skeletal maturity is ineffective diagnostic measures. Current protocols of serial clinical exams and ultrasound screening for DDH are primarily focused on detecting neonatal hip instability, but instability resolves spontaneously in many cases. These approaches may not address cases involving stable acetabular dysplasia without evidence of hip instability. New approaches to diagnosis and treatment may be needed to detect more subtle cases of stable hip acetabular dysplasia in infancy. Acetabular dysplasia is common in Scandinavian countries, and routine radiographs of the pelvis at 4–5 years of age have been suggested in order to treat dysplasia before the onset of arthritis [30]. Whether early treatment would benefit patients with more subtle stable acetabular dysplasia is an unresolved question; however, there is evidence in canines and in humans that proper positioning of the hips during the neonatal period may benefit acetabular development [31].
Acetabular dysplasia after skeletal maturity may have developed post-infancy and represents a distinct disease entity from infantile DDH that may not be affected by screening more of the population in infancy [21, 22]. Lee et al. [21] found that male sex, bilateral hip pathology, and family history of early total hip arthroplasty (<65 years of age) was more common in adult- or adolescent-onset acetabular dysplasia relative to a population of patients with infantile DDH, who tended to have a family history of DDH and were predominantly female. The authors suggested that infantile DDH and adult- or adolescent-onset DDH may represent separate disease entities; however, inadequate selective screening criteria could still explain the low rates of a family history of DDH seen in the adult dysplasia group [21]. Additionally, our data does not support the male predominance in adult acetabular dysplasia found by Lee et al., suggesting differences in our patient populations or referral patterns. Universal ultrasound screening has been reported in Austria to reduce the incidence of late surgery for all ages, including patients aged 15–35 years, which suggests that expanded ultrasound screening and higher treatment rates in neonates may have an impact on the incidence of skeletally mature dysplasia [18]. Our study suggests that selective ultrasound screening may be inadequate to identify delayed development of dysplasia outside of the neonatal period. Despite these findings, further studies examining the origins of infantile DDH and adolescent/adult hip dysplasia are needed in order to determine the contribution of missed screening versus post-infancy development of adult hip dysplasia.
There are several limitations to this study. Patients in this study presented to a tertiary referral center with hip pain and concomitant acetabular dysplasia. The diagnosis was based on a detailed physical exam, radiographs (anteroposterior and false-profile radiographs), MRI of the hip, and 3D CT scan. There are limits to a broad population-based conclusion with this study, since these were only symptomatic patients that presented to the authors’ center. It is unclear whether asymptomatic patients with adult dysplasia would have different characteristics to this population. Even if the patients in this cohort were theoretically screened, they may still present with symptoms attributed to dysplasia due to a failure of the screening mechanism, such as misinterpreted clinical examination or ultrasound findings, or, as previously mentioned, a lack of acetabular development that may not be recognizable in the infant hip.
In summary, only 14.7 % of skeletally mature patients presenting with symptomatic acetabular dysplasia would meet current criteria for selective ultrasound screening for a stable hip. Current screening may improve the incidence of early diagnosis and treatment of hip dysplasia in the high-risk group (breech and family history of DDH), but it may not have a significant impact on the incidence of skeletally mature acetabular dysplasia. Expanding selective ultrasound screening criteria to include any family history of hip osteoarthritis and/or female sex, especially first-born females, may further identify a significant group of patients who have risk factors for developing acetabular dysplasia at skeletal maturity. Additionally, the role of expanding screening modalities to older age groups in patients at increased risk for adult dysplasia should continue to be investigated in the future. It remains unclear whether increased identification and treatment of patients with infantile DDH would decrease the rates of symptomatic acetabular dysplasia in skeletally mature adults. Further studies are needed in order to fully define appropriate screening protocols.
References
Clohisy JC, Dobson MA, Robison JF, Warth LC, Zheng J, Liu SS, Yehyawi TM, Callaghan JJ (2011) Radiographic structural abnormalities associated with premature, natural hip-joint failure. J Bone Joint Surg Am 93(Suppl 2):3–9
Engesæter IØ, Lehmann T, Laborie LB, Lie SA, Rosendahl K, Engesæter LB (2011) Total hip replacement in young adults with hip dysplasia: age at diagnosis, previous treatment, quality of life, and validation of diagnoses reported to the Norwegian Arthroplasty Register between 1987 and 2007. Acta Orthop 82:149–154
Godward S, Dezateux C (1998) Surgery for congenital dislocation of the hip in the UK as a measure of outcome of screening. MRC Working Party on Congenital Dislocation of the Hip. Medical Research Council. Lancet 351:1149–1152
Bialik V, Bialik GM, Blazer S, Sujov P, Wiener F, Berant M (1999) Developmental dysplasia of the hip: a new approach to incidence. Pediatrics 103:93–99
Chan A, Cundy PJ, Foster BK, Keane RJ, Byron-Scott R (1999) Late diagnosis of congenital dislocation of the hip and presence of a screening programme: South Australian population-based study. Lancet 354:1514–1517
Patel H; Canadian Task Force on Preventive Health Care (2001) Preventive health care, 2001 update: screening and management of developmental dysplasia of the hip in newborns. CMAJ 164:1669–1677
von Kries R, Ihme N, Oberle D, Lorani A, Stark R, Altenhofen L, Niethard FU (2003) Effect of ultrasound screening on the rate of first operative procedures for developmental hip dysplasia in Germany. Lancet 362:1883–1887
Wirth T, Stratmann L, Hinrichs F (2004) Evolution of late presenting developmental dysplasia of the hip and associated surgical procedures after 14 years of neonatal ultrasound screening. J Bone Joint Surg Br 86:585–589
[No authors listed] (2000) Clinical practice guideline: early detection of developmental dysplasia of the hip. Committee on Quality Improvement, Subcommittee on Developmental Dysplasia of the Hip. American Academy of Pediatrics. Pediatrics 105:896–905
Sanghrajka AP, Murnaghan CF, Shekkeris A, Eastwood DM (2013) Open reduction for developmental dysplasia of the hip: failures of screening or failures of treatment? Ann R Coll Surg Engl 95:113–117
Shipman SA, Helfand M, Moyer VA, Yawn BP (2006) Screening for developmental dysplasia of the hip: a systematic literature review for the US Preventive Services Task Force. Pediatrics 117:e557–e576
Laborie LB, Engesæter IØ, Lehmann TG, Eastwood DM, Engesæter LB, Rosendahl K (2013) Screening strategies for hip dysplasia: long-term outcome of a randomized controlled trial. Pediatrics 132:492–501
Mahan ST, Katz JN, Kim YJ (2009) To screen or not to screen? A decision analysis of the utility of screening for developmental dysplasia of the hip. J Bone Joint Surg Am 91:1705–1719
Rosendahl K, Markestad T, Lie RT (1994) Ultrasound screening for developmental dysplasia of the hip in the neonate: the effect on treatment rate and prevalence of late cases. Pediatrics 94(1):47–52
Zenios M, Wilson B, Galasko CS (2000) The effect of selective ultrasound screening on late presenting DDH. J Pediatr Orthop B 9:244–247
Paton RW, Srinivasan MS, Shah B, Hollis S (1999) Ultrasound screening for hips at risk in developmental dysplasia. Is it worth it? J Bone Joint Surg Br 81:255–258
Marks DS, Clegg J, al-Chalabi AN (1994) Routine ultrasound screening for neonatal hip instability. Can it abolish late-presenting congenital dislocation of the hip? J Bone Joint Surg Br 76:534–538
Thaler M, Biedermann R, Lair J, Krismer M, Landauer F (2011) Cost-effectiveness of universal ultrasound screening compared with clinical examination alone in the diagnosis and treatment of neonatal hip dysplasia in Austria. J Bone Joint Surg Br 93:1126–1130
Treiber M, Tomazic T, Tekauc-Golob A, Zolger J, Korpar B, Burja S, Takac I, Sikosek A (2008) Ultrasound screening for developmental dysplasia of the hip in the newborn: a population-based study in the Maribor region, 1997–2005. Wien Klin Wochenschr 120:31–36
von Kries R, Ihme N, Altenhofen L, Niethard FU, Krauspe R, Rückinger S (2012) General ultrasound screening reduces the rate of first operative procedures for developmental dysplasia of the hip: a case–control study. J Pediatr 160:271–275
Lee CB, Mata-Fink A, Millis MB, Kim YJ (2013) Demographic differences in adolescent-diagnosed and adult-diagnosed acetabular dysplasia compared with infantile developmental dysplasia of the hip. J Pediatr Orthop 33:107–111
Wynne-Davies R (1970) Acetabular dysplasia and familial joint laxity: two etiological factors in congenital dislocation of the hip. A review of 589 patients and their families. J Bone Joint Surg Br 52(4):704–716
Price KR, Dove R, Hunter JB (2013) Current screening recommendations for developmental dysplasia of the hip may lead to an increase in open reduction. Bone Joint J 95-B(6):846–850
de Hundt M, Vlemmix F, Bais JM, Hutton EK, de Groot CJ, Mol BW, Kok M (2012) Risk factors for developmental dysplasia of the hip: a meta-analysis. Eur J Obstet Gynecol Reprod Biol 165:8–17
Hinderaker T, Daltveit AK, Irgens LM, Udén A, Reikerås O (1994) The impact of intra-uterine factors on neonatal hip instability. An analysis of 1,059,479 children in Norway. Acta Orthop Scand 65:239–242
Stevenson DA, Mineau G, Kerber RA, Viskochil DH, Schaefer C, Roach JW (2009) Familial predisposition to developmental dysplasia of the hip. J Pediatr Orthop 29:463–466
Schiffern AN, Stevenson DA, Carroll KL, Pimentel R, Mineau G, Viskochil DH, Roach JW (2012) Total hip arthroplasty, hip osteoarthritis, total knee arthroplasty, and knee osteoarthritis in patients with developmental dysplasia of the hip and their family members: a kinship analysis report. J Pediatr Orthop 32:609–612
Omeroğlu H (2014) Use of ultrasonography in developmental dysplasia of the hip. J Child Orthop 8(2):105–113
Talbot CL, Paton RW (2013) Screening of selected risk factors in developmental dysplasia of the hip: an observational study. Arch Dis Child 98:692–696
Hvid I (2008) Neonatal hip instability, developmental dysplasia of the acetabulum, and the risk of early osteoarthrosis. Acta Orthop 79:311–312
Ferrer-Torrelles M, Ceballos T, Ferrer-Loewinsohn A (1990) Development of the hip joint in relation to congenital dislocation. Acta Orthop Belg 56:13–22
Author information
Authors and Affiliations
Corresponding author
Additional information
Conflict of interest
There are no conflicts of interest directly related to this manuscript. One author (ELS) receives consulting fees from Pivot Medical unrelated to this manuscript. All other authors have no conflict of interest to declare.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Sink, E.L., Ricciardi, B.F., Torre, K.D. et al. Selective ultrasound screening is inadequate to identify patients who present with symptomatic adult acetabular dysplasia. J Child Orthop 8, 451–455 (2014). https://doi.org/10.1007/s11832-014-0620-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11832-014-0620-1