
Abstract
Background
Adequate sleep is of great importance in recovering from and preparing for training and competition.
Objective
This study aimed to investigate subjective sleep quality and daytime sleepiness of the German women’s junior national ice hockey team before and after a training camp immediately preceding the World Championship Division IA tournament.
Materials and methods
Twenty athletes (16.40 ± 0.68 years) completed German paper–pencil versions of the Pittsburgh Sleep Quality Index (PSQI) and the Epworth Sleepiness Scale (ESS) before the training camp (T1, day 1) and on the final day of the training camp (T2, day 7).
Results
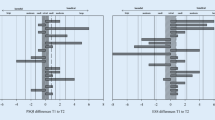
Paired t-tests indicated a significant decrease in PSQI global scores from pre- to post-training camp assessments (t = 2.33, p = 0.031, df = 19), with a medium effect size (d = 0.52). Regarding ESS global scores, results of the paired t-test indicated no significant pre- to post-training camp differences (t = 0.67, p = 0.510, df = 19) and the effect size was trivial (d = 0.15). Mean scores were reduced for both PSQI (T1 = 5.90 ± 2.36, T2 = 4.65 ± 2.18) and ESS (T1 = 9.00 ± 3.58, T2 = 8.60 ± 4.04) after the training camp. When analyzed according to the position of the players, no statistically significant intergroup differences were found.
Conclusion
This study underlines the need for monitoring and screening youth athletes’ sleep before special sports events in order to identify a potential need for intervention as early as possible, to prevent serious consequences for athletes’ performance capability and well-being.
Zusammenfassung
Hintergrund
Adäquater Schlaf ist für die Erholung von und die Vorbereitung auf Training und Wettkampf von enormer Bedeutung.
Ziel der Arbeit
Es erfolgte die Untersuchung der subjektiven Schlafqualität und Tagesschläfrigkeit der deutschen Nachwuchs-Frauen-Eishockey-Nationalmannschaft vor und nach einem Trainingslager unmittelbar vor Beginn der Weltmeisterschaft Division IA.
Material und Methoden
Dazu füllten 20 Athletinnen (16,40 ± 0,68 Jahre) die deutschen Paper-Pencil-Versionen des Pittsburgh Sleep Quality Index (PSQI) und der Epworth Sleepiness Scale (ESS) vor Beginn des Trainingslagers (T1, Tag 1) und am letzten Tag des Trainingslagers (T2, Tag 7) aus.
Ergebnisse
Gepaarte t-Tests wiesen eine signifikante Abnahme im PSQI-Globalwert von der Erhebung vor dem Trainingslager zu der Erhebung nach dem Trainingslager (t = 2,33; p = 0,031; df = 19) mit einer mittleren Effektstärke (d = 0,52) auf. Bezüglich der ESS-Globalwerte zeigten die Ergebnisse des gepaarten t-Tests keinen signifikanten Prä-Post Unterschied (t = 0,67; p = 0,510; df = 19), die Effektstärke war trivial (d = 0,15). Die Mittelwerte verringerten sich sowohl für den PSQI (T1 = 5,90 ± 2,36; T2 = 4,65 ± 2,18) als auch für die ESS (T1 = 9,00 ± 3,58; T2 = 8,60 ± 4,04). Eine Analyse unter Berücksichtigung der Positionen der Spielerinnen ergab keine statistisch signifikanten Unterschiede zwischen den Gruppen.
Schlussfolgerung
Die Studie verdeutlicht die Notwendigkeit eines Monitorings und Screenings des Schlafs von Nachwuchsathleten und -athletinnen vor sportlichen Großereignissen, um einen potenziellen Interventionsbedarf frühzeitig zu identifizieren und gravierende Auswirkungen auf die Leistungsfähigkeit und das Wohlbefinden der Athleten und Athletinnen zu verhindern.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Sleep is considered essential for ensuring athletes’ health and well-being [30]. In ice hockey, adequate sleep appears to be of particular importance to prevent injuries and ensure performance readiness [23]. A previous study in German male youth national ice hockey athletes stated an urgent need for further studies on sleep in ice hockey [14]. This study thus assessed subjective sleep quality and daytime sleepiness of the German women’s junior national ice hockey team during preparation for the World Championship Division IA tournament, to gain a better understanding of athletes’ sleep-related needs.
Adequate sleep is central in recovering from and preparing for training and competition as well as for ensuring athletes’ physiological and psychological performance capability and well-being [6, 30]. The general importance of sleep for athletes is evidenced by considering potential consequences of sleep loss, including performance- and heath-affecting factors [30]. As one regeneration approach, sleep is considered essential for general well-being and physiological and psychological recovery [17]. Ice hockey is a highly intermittent contact sport characterized by high intensity, speed, and pace, requiring technical skills and quick recovery after and during intense exercise [1, 19]. Women’s ice hockey is characterized by player contact, collisions, and high speed and velocity [2], whereby performance-related and physical demands on female elite ice hockey athletes seem to be position-specific [9, 13]. Considered as a high-risk sport due to the physicality and risk of injury, and also due to the required mental and physical performance readiness, adequate recovery and thus monitoring of sleep and recovery in ice hockey athletes has become highly relevant [1, 8, 20]. Considering that Milewski et al. found an association between sleep duration and injury risks in adolescent student athletes and that the injury risk was 1.7 times higher in those athletes that slept less than 8 h per night, sleep and recovery can also be relevant and essential to injury prevention [23].
Athletes’ actual sleep, however, is often characterized by poor sleep quality, short sleep duration, and daytime sleepiness, and sleeping conditions are often not ideal [27, 30]. Alongside stress and anxiety induced by competition and other athlete-specific psychosocial stressors, the timing and intensity of training and competition as well as training stress potentially hinder sleep [24, 26]. In a sample of 175 highly trained team sport athletes, poor sleep quality was found in 50%, while excessive daytime sleepiness was found in 28% [29]. In a sample of elite winter team athletes, 32% were reported to exhibit poor sleep quality [4]. A recent study examined daytime sleepiness and sleep quality in German male youth national ice hockey players during preparation for the World Championship Division IA using the Pittsburgh Sleep Quality Index (PSQI) [5] and the Epworth Sleepiness Scale (ESS) [15]. At the start of a pre-tournament training camp, 42.9% of athletes were found to show poor sleep quality and 28.6% showed severe daytime sleepiness [14]. In the evening before the first game, which was also the last day of the preparation camp, 33.3% showed poor sleep quality and 28.6% showed severe daytime sleepiness. Derived from this, the authors stated an urgent need for further studies on sleep in ice hockey athletes to gain a better understanding of their demands and recovery as well as sleep-related needs. The current study examined sleep quality and daytime sleepiness in German female youth national ice hockey athletes in a comparable setting and age group. An additional research question was whether differences in players’ sleep quality and daytime sleepiness exist according to position-specific performance demands. This investigation was aimed at assessing subjective sleep quality and daytime sleepiness in the German women’s junior national ice hockey team during preparation for the World Championship Division IA tournament.
Materials and methods
Study design and investigation methods
The analyzed sample comprised the 20 athletes nominated for the final tournament team, with a mean age of 16.40 ± 0.68 years. The team consisted of 12 forwards (F), two goalkeepers (G), and six defenders (D). A pre-tournament training camp (TC) was scheduled during the 7 days preceding the tournament (from the end of December until the beginning of January). The tournament was hosted in Germany, and the German national team was already on site for the preparation camp. Players changed hotels before the tournament started (T7), but sleeping conditions remained the same during the entire period covering the TC and the tournament. Two teammates shared a double room and there was a scheduled bedtime routine including predetermined sleep and getting-up times that had to be adhered to. At bedtime (22:00; on late game days 24:00), mobile phones were collected and guided relaxation techniques were implemented for the whole team shortly before going to bed, except for on three evenings on which late games were scheduled, so as not to delay bedtime any further.
Procedure
The purpose of the TC was to ensure and increase athletes’ performance capability in the World Championship games. The study objective of an assessment of sleep was intended to identify potential sleeping problems. On the day of arrival, a short presentation was given to the players to inform about the purpose of the study and data collection processes. The pseudonymized collection of data and the obligation to maintain professional confidentiality were assured and explained to all athletes, in order to reduce concerns and increase compliance. All athletes completed the German paper–pencil versions of the PSQI [5] and the ESS [15], once on the arrival day of the TC (T1, day 1) and once again on the final day of the TC, which was simultaneously the last day before the start of the tournament (T2, day 7). During the 7‑day period of the TC, the training schedule included one to two training sessions per day, whereby two test games replaced the respective training sessions and there was one rest day without any exercise. All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975 (in its most recently amended version). Written informed consent was obtained from all participants included in the study and from the parents of minor athletes. Furthermore, ethical approval was obtained from the local ethics committee prior to the assessment.
Questionnaires
The PSQI was used to assess athletes’ perceived sleep quality. The self-evaluation questionnaire contains 19 items covering different components of sleep quality over the period of the past month. Component scores are built by clustering the items into seven scores including subjective sleep quality, sleep duration, or sleep latency. The component score sum then forms a global PSQI score ranging from 0 to 21, with scores higher than 5 indicating poor sleep quality [5]. The instrument’s reliability and validity have been confirmed, with a reported specificity of 86.5% and sensitivity of 89.6% or even higher [3, 5]. The PSQI is not only frequently applied in research and clinical contexts, but is also established in sports [4, 10].
The ESS assesses the subjectively perceived level of daytime sleepiness. Based on the evaluation of eight items, a sum score can be built ranging from 0 to 24. Generally, scores exceeding 10 are suggested to indicate excessive daytime sleepiness [15]. Quality criteria of reliability, simplicity, and internal consistency were fulfilled [16]. The ESS also finds application in the field of sports [10, 11, 21].
Statistical analysis
Statistical analysis was performed using SPSS v.26 (IBM Corporation, Armonk, NY, USA). Descriptive statistics are presented as mean ± standard deviation. Global scores were built for both questionnaires, and component scores of ’subjective sleep quality’ and ’sleep duration’ of the PSQI were analyzed in more detail to examine whether sleep duration had changed, or whether the main effect is subjective sleep quality. Kolmogorov–Smirnov tests were performed to assess the normal distribution of global scores and their difference values (p > 0.05). All four global scores were normally distributed, while both difference values depicting pre- to post-TC differences for the ESS and PSQI and their difference values, as well as selected component scores and their difference values, did not meet the normal distribution criterium. Therefore, nonparametric Wilcoxon signed-rank tests were first calculated to compare pre- to post-TC assessments, followed by paired t-tests. Statistical results did not differ between the Wilcoxon signed-rank tests and paired t-tests. As t-tests are considered a robust statistical procedure resistant to violation of the normal distribution assumption [28], paired t-tests were performed to enable a more detailed and accurate analysis and to allow for an indication and calculation of effect sizes. The statistical significance level was set at 0.05. Cohen’s effect sizes (d) were calculated between T1 and T2 for both questionnaires and were evaluated according to the categorization of 0.2, 0.5, and 0.8, indicating small, moderate, and large effects, respectively [7]. For assessing test–retest reliability, Spearman correlations were used. For a position-specific comparison of players, athletes were divided into two main groups: offense and defense. The offense group (OG) included all 12 F, while the defense group (DG) consisted of the six D and the two G. With regard to small sample sizes and the partly violated normal distribution assumption, nonparametric Mann–Whitney U tests were conducted for testing differences between OG and DG.
Results
Descriptive statistics, which are presented in Table 1, showed that the mean PSQI global score at T1 exceeded the corresponding score at T2, indicating a reduction from the first to the second measurement. Paired t-test results indicated a significant change in PSQI global scores from pre- to post-TC assessments (t = 2.33, p = 0.031, df = 19), with a medium effect size (d = 0.52). The test–retest reliability of PSQI scores, however, was rather small, with a moderate correlation (rs = 0.471, p = 0.036). Descriptively, the division into categories dividing good from poor sleepers on the basis of the PSQI global score indicated a change from pre- to post-TC measurements, as can be seen from Fig. 1. At T1, 50% of players were identified as good sleepers, while 45% were categorized as poor sleepers and 5% were categorized as showing very poor sleep quality (PSQI scores > 10). The proportion of good sleepers increased at T2, with 65% categorized as good sleepers and 35% identified as having poor sleep quality.

Frequencies of players’ categorizations according to the PSQI. PSQI Pittsburgh Sleep Quality Index, T1 first measurement (arrival day of the training camp), T2 second measurement (final day of the training camp)
Focusing on the PSQI component scores for ’subjective sleep quality,’ paired t-test results indicated no significant change from T1 (1.05 ± 0.51) to T2 (1.10 ± 0.64; t = −0.57, p = 0.577, df = 19), and the effect size was trivial (d = 0.13). Regarding the component scores for ’sleep duration,’ there was a significant difference between T1 (0.30 ± 0.57) and T2 (0.00 ± 0.00; t = 2.35, p = 0.030, df = 19), with a medium effect size (d = 0.53).
Regarding the descriptive statistics in Table 1, the ESS global score before TC was slightly higher than the post-TC ESS mean score. Regarding ESS global scores, results of the paired t-test indicated no significant pre- to post-TC difference (t = 0.67, p = 0.510, df = 19), and the effect size was trivial (d = 0.15). The test–retest reliability of ESS scores was nearly acceptable, with a moderate correlation (rs = 0.647, p = 0.002). As can be seen from Fig. 2, at T1, ESS scores were in a normal range of daytime sleepiness for 65% of players, while the remaining 35% showed excessive daytime sleepiness (ESS scores > 10). At T2, 75% showed normal daytime sleepiness, while 25% exceeded a score of 10 and were thus categorized as exhibiting excessive daytime sleepiness.

Frequencies of players’ categorizations according to the ESS. ESS Epworth Sleepiness Scale, T1 first measurement (arrival day of the training camp), T2 second measurement (final day of the training camp)
As can be seen from Table 2, descriptive data differed between the OG and DG. At both measurements, T1 and T2, the mean PSQI score of F was higher than the corresponding score of D and G. Concerning the ESS, a different pattern emerged: while the ESS score of F slightly exceeded the DG score at T1, at T2, in contrast, the score was lower in the OG compared to the DG. When divided by position, no intergroup differences were found, neither for the PSQI and ESS global scores at T1 and T2 nor for their difference scores depicting changes over time, as Mann–Whitney U test results were not statistically significant (p > 0.1).
Discussion
The aim of this study was to assess subjective sleep quality and daytime sleepiness in German female youth national ice hockey athletes at the start and end of a TC immediately preceding the World Championship Division IA tournament. Results imply a significant increase in subjectively perceived sleep quality over the course of the TC. Based on the results of the component score analyses, this increase appears to be due to increased sleep duration over the course of the TC rather than due to an increase in subjective sleep quality. There was no statistically significant trend for the sample’s daytime sleepiness. Descriptively, there was a reduction in daytime sleepiness from the start of the TC to the end. Thus, a pre-tournament TC seems to be an effective and beneficial measure to ensure an improvement in sleep quality and decline of sleepiness, as a prerequisite for performance readiness in an upcoming tournament. The reduction in training intensity during the TC and the temporary reduction of the double burden of school and training due to the Christmas holiday period might have been major influencing factors in this improvement of sleep quality and daytime sleepiness [25]. The implementation of guided relaxation techniques before bedtime, the absence of smartphone use before going to sleep, and scheduled bedtimes, which all constitute sleep hygiene interventions [10], probably promoted more restful sleep. Anecdotal reports from athletes indicated a beneficial effect of relaxation techniques, which should be systematically assessed in future studies on the effects of sleep hygiene interventions. TC conditions of short distances between the hotel and ice stadium, having meals together, and the common bedtime routine potentially promoted stress reduction and (social) recovery, which, in turn, positively affected sleep and sleepiness [17, 22]. For some athletes the opposite trend was observed, as they showed an increase in daytime sleepiness or a decrease in sleep quality from pre- to post-TC measurements. The unfamiliar sleep environment of the hotel, the fact of sharing bedrooms with a teammate, and different sleeping conditions might have interfered with sleep in these players more than for others [18], and/or they may be more sensitive or already slightly disturbed sleepers. Performance pressure and nervousness due to the nomination process and the upcoming tournament constitute other possible factors that might have contributed to the impairment of sleep quality and daytime sleepiness in some players. These individual deviations from the average trend in the team underline the individuality of sleep and sleeping behavior, requiring an individual assessment and evaluation of sleep [14, 30].
Comparison with other studies that examined sleep in athletes shows that the average PSQI and ESS scores of the sample were quite similar to those reported in previous studies on male and female winter Canadian national team athletes, highly trained team sport athletes, and collegiate student athletes (e.g., female student athletes, female field hockey players) [4, 21, 29]. The sample’s mean scores and their decrease over time were very similar to those reported for the men’s junior national team [14]. In case of the male ice hockey players, however, there were no interventions addressing sleeping conditions as for the current sample of female youth athletes. Like the men’s youth ice hockey team, the German team won the tournament, although one quarter of the team showed excessive daytime sleepiness and poor sleep quality was found in a third of all players at the end of the TC. The cause for these striking values could be a lack of sleep quality characteristics and sleep duration. Whether further improvement of performance could have been achieved by greater improvement in sleep parameters or whether a temporal neglect of sleep quality during tournament phases is tolerable needs to be specifically examined [14]. Follow-up assessments including frequent measurements covering season and off-season phases as well as pre- and post-competition periods would provide a more comprehensive view of players’ sleep and daytime sleepiness. This would in turn enable a differentiation between temporary sleepiness and impaired sleep quality during (preparation for) championship periods and continuous and long-lasting disturbed sleep going beyond tournament phases.
Regarding position-specific differences, the lower sleep quality in F compared to D and G at both measurements might be explainable by their higher performance demands causing potentially stronger interference with sleep quality due to higher levels of post-practice or post-competition muscle soreness or pain [12], and possibly due to a higher level of responsibility. As with sleep quality, the daytime sleepiness of F was slightly higher at the first measurement. The development of daytime sleepiness of D and G over time, however, was contrary to the development observed in F and the whole team, as it increased at the end of the TC. Possibly, the D and G experienced training sessions or test games during the TC as more intense and demanding than the group of F, which may have caused an increase in daytime sleepiness and fatigue but did not interfere with sleep quality. The possible effects of performance demands and training intensity on sleep should be investigated in more detail in future research, considering and integrating objective training parameters. The chosen group formation of building the DG out of D and G might have been another influencing factor, as the demands of G and D differ [13]. Differences between player positions should be assessed in a larger sample of female athletes, including young and adult athletes and a sufficient number of players in all three positions. Furthermore, differences in performance demands might be reflected in different recovery patterns and needs, rather than having a direct effect on sleep. Therefore, future research on the interactions between performance demands, recovery, and sleep is required.
Limitations
Even though the PSQI and ESS have been frequently applied in sporting contexts, future studies should additionally include sport-specific questionnaires such as the Athlete Sleep Behavior Questionnaire [11] considering athlete-specific sleep challenges [14]. The ESS was validated for sleep apnea patients and not for young athletes, which should be considered concerning the psychometric criteria of the questionnaire and its suitability [15]. The questionnaires were chosen for comparison purposes and due to being time effective and capturing the subjective perception of sleep while affecting athletes’ sleeping conditions as little as possible. However, data do not allow statements on sleep stages, sleep parameters, or the diagnosis of sleep disorders [30]. The assessment served as a pre-screening to identify potentially vulnerable athletes for whom objective methods including polysomnography and actigraphy would then need to be applied to examine sleep architecture and sleep parameters in more detail. Significant parameters such as subjective and objective information on sleep duration, further assessments of sleep quality using other sleep questionnaires, and information on other relevant factors such as chronotype would have been valuable additions. The questionnaire-based assessment should be kept in mind when interpreting the results, as should the small and selective sample, which might be one factor contributing to the low test–retest reliability of the PSQI. Furthermore, the PSQI refers to the period of the past month; the assessment, however, was conducted within 1 week, which is rather short to include significant changes. Thus, time-specific instructions for the PSQI should be applied to comparable studies using this questionnaire. Results are based on group means which do not provide information on individual players’ sleep and reaction to tournament conditions and applied sleep hygiene measures, which should always be examined in view of the high interindividual variability in athletes’ sleep and recovery [14, 17].
Conclusion
This study is of high practical relevance due to data collection during the preparation camp of the IIHF U18 Women’s World Championship Division IA tournament. This study underscores the need for monitoring and screening athletes’ sleep during special and decisive sports events, in order to identify a possible need for intervention as early as possible to prevent serious and career-affecting consequences for athletes’ performance capability and well-being. Subjectively perceived sleep quality and daytime sleepiness were assessed using the PSQI and the ESS, which should be complemented by additional parameters relevant for the evaluation of sleep. Generally, sleep management strategies and sleep education should be implemented in elite and high-performance sports to raise athletes’ and coaches’ awareness of the importance of adequate sleep and sleep management.
Practical conclusion
-
Monitoring athletes’ subjectively perceived sleep and recovery is of great importance, especially during special sports events, to identify deviations as early as possible to then apply objective measures to examine sleep parameters and sleep architecture in more detail.
-
Assessments of sleep quality and daytime sleepiness should contain complementary parameters and measurement procedures for comprehensive information on sleep.
-
A pre-tournament preparation camp seems to be an effective and beneficial measure to ensure more adequate sleep as a prerequisite for performance readiness in an upcoming tournament.
-
Sleep management strategies and sleep education should be implemented in elite and high-performance sports.
References
Adams S, Mason CW, Robidoux MA (2015) ‘If you don’t want to get hurt, don’t play hockey’: the uneasy efforts of hockey injury prevention in Canada. Sociol Sport J 32:248–265
Agel J, Dick R, Nelson B, Marshall SW, Dompier TP (2007) Descriptive epidemiology of collegiate women’s ice hockey injuries: National Collegiate Athletic Association Injury Surveillance System, 2000–2001 through 2003–2004. J Athl Train 42:249–254
Backhaus J, Junghanns K, Broocks A, Riemann D, Hohagen F (2002) Test-retest reliability and validity of the Pittsburgh Sleep Quality Index in primary insomnia. J Psychosom 53:737–740
Bender AM, Van Dongen H, Samuels CH (2019) Sleep quality and chronotype differences between elite athletes and non-athlete controls. Clocks Sleep 1:3–12
Buysse DJ, Reynolds CF III, Monk TH, Berman SR, Kupfer DJ (1989) The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res 28:193–213
Caia J, Kelly VG, Halson SL (2018) The role of sleep in maximising performance in elite athletes. In: Kellmann M, Beckmann J (eds) Sport, recovery, and performance: interdisciplinary insights. Routledge, pp 151–167
Cohen J (1988) Statistical power analysis for the behavioral sciences. Lawrence Erlbaum
Cox MH, Miles DS, Verde TJ, Rhodes EC (1995) Applied physiology of ice hockey. Sports Med 19:184–201
Douglas A, Rotondi MA, Baker J, Jamnik VK, Macpherson AK (2019) On-ice physical demands of world-class women’s ice hockey: from training to competition. Int J Sports Physiol Perform 14:1227–1232
Driller MW, Lastella M, Sharp AP (2019) Individualized sleep education improves subjective and objective sleep indices in elite cricket athletes: a pilot study. J Sports Sci 37:2021–2025
Driller MW, Mah CD, Halson SL (2018) Development of the athlete sleep behavior questionnaire: a tool for identifying maladaptive sleep practices in elite athletes. Sleep Sci 11:37–44
Fullagar HH, Duffield R, Skorski S, Coutts AJ, Julian R, Meyer T (2015) Sleep and recovery in team sport: current sleep-related issues facing professional team-sport athletes. Int J Sports Physiol Perform 10:950–957
Geithner CA, Lee AM, Bracko MR (2006) Physical and performance differences among forwards, defensemen, and goalies in elite women’s ice hockey. J Strength Cond Res 20:500–505
Hof zum Berge A, Loch F, Schwarzenbrunner K, Ferrauti A, Meyer T, Pfeiffer M, Kellmann M (2021) Assessment of sleep quality and daytime sleepiness in German national ice hockey players preparing for the World Championship. Ger J Exerc Sport Res 51:94–101
Johns MW (1991) A new method for measuring daytime sleepiness: the Epworth Sleepiness Scale. Sleep 14:540–545
Johns MW (1992) Reliability and factor analysis of the Epworth Sleepiness Scale. Sleep 15:376–381
Kellmann M, Bertollo M, Bosquet L, Brink M, Coutts AJ, Duffield R, Erlacher D, Halson SL, Hecksteden A, Heidari J, Kallus KW, Meeusen R, Mujika I, Robazza C, Skorski S, Venter R, Beckmann J (2018) Recovery and performance in sport: consensus statement. Int J Sports Physiol Perform 13:240–245
Kölling S, Duffield R, Erlacher D, Venter R, Halson SL (2019) Sleep-related issues for recovery and performance in athletes. Int J Sports Physiol Perform 14:144–148
Lignell E, Fransson D, Krustrup P, Mohr M (2018) Analysis of high-intensity skating in top-class ice hockey match-play in relation to training status and muscle damage. J Strength Cond Res 32:1303–1310
Loch F, Hof zum Berge A, Ferrauti A, Meyer T, Pfeiffer M, Kellmann M (2020) Acute effects of mental recovery strategies after a mentally fatiguing task. Front Psychol 11:558856
Mah CD, Kezirian EJ, Marcello BM, Dement WC (2018) Poor sleep quality and insufficient sleep of a collegiate student-athlete population. Sleep Health 4:251–257
Martire VL, Caruso D, Palagini L, Zoccoli G, Bastianini S (2020) Stress & sleep: a relationship lasting a lifetime. Neurosci Biobehav Rev 117:65–77
Milewski MD, Skaggs DL, Bishop GA, Pace JL, Ibrahim DA, Wren TAL, Barzdukas A (2014) Chronic lack of sleep is associated with increased sports injuries in adolescent athletes. J Pediatr 34:129–133
Nédélec M, Aloulou A, Duforez F, Meyer T, Dupont G (2018) The variability of sleep among elite athletes. Sports Med 4:34
Riederer MF (2020) How sleep impacts performance in youth athletes. Curr Sports Med Rep 19:463–467
Roberts SSH, Teo W‑P, Warmington SA (2019) Effects of training and competition on the sleep of elite athletes: a systematic review and meta-analysis. Br J Sports Med 53:513–522
Sargent C, Lastella M, Halson SL, Roach GD (2014) The impact of training schedules on the sleep and fatigue of elite athletes. Chronobiol Int 31:1160–1168
Schäfer T (2016) Unterschiede zwischen zwei Gruppen: der t‑Test [Differences between two groups: the t‑test]. In: Methodenlehre und Statistik Basiswissen Psychologie [Methodology and statistics Basic knowledge Psychology]. Springer, Berlin Heidelberg, pp 205–215
Swinbourne R, Gill N, Vaile J, Smart D (2016) Prevalence of poor sleep quality, sleepiness and obstructive sleep apnoea risk factors in athletes. Eur J Sport Sci 16:850–858
Walsh NP, Halson SL, Sargent C, Roach GD, Nédélec M, Gupta L, Leeder J, Fullagar HH, Coutts AJ, Edwards BJ, Pullinger SA, Robertson CM, Burniston JG, Lastella M, Le Meur Y, Hausswirth C, Bender AM, Grandner MA, Samuels CH (2021) Sleep and the athlete: Narrative review and 2021 expert consensus recommendations. Br J Sports Med 55:356–368
Acknowledgements
The authors would like to thank all players, staff members, and the German Ice Hockey Federation for their contribution to the study.
Funding
The research was realized within “Analysis and Optimization of Recovery Management of Female Ice Hockey Players during the Qualification for the Olympic Games” (072001/19-20).
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
A. Kiel, A. Hof zum Berge, K. Schwarzenbrunner, K. Otto, F. Loch, M. Kellmann, and S. Jakowski declare that they have no competing interests.
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975 (in its most recently amended version). Written informed consent was obtained from all participants included in the study and the parents of minor athletes.
Additional information

Scan QR code & read article online
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kiel, A., Hof zum Berge, A., Schwarzenbrunner, K. et al. Sleep in German female youth national ice hockey athletes. Somnologie 26, 232–238 (2022). https://doi.org/10.1007/s11818-022-00390-4
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11818-022-00390-4