
Abstract
Purpose
Weight gain after breast cancer poses health risks. We aimed to identify factors associated with weight gain during adjuvant endocrine therapy (AET).
Methods
Women initiating AET enrolled in a prospective cohort. Participants completed FACT-ES plus PROMIS pain interference, depression, anxiety, fatigue, sleep disturbance and physical function measures at baseline, 3, 6, 12, 24, 36, 48 and 60 months. Treatment-emergent symptoms were defined as changes in scores in the direction indicative of worsening symptoms that exceeded the minimal important difference at 3 and/or 6 months compared to baseline. We used logistic regression to evaluate associations of clinicodemographic features and treatment-emergent symptoms with clinically significant weight gain over 60 months (defined as ≥ 5% compared to baseline) in pre- and post-menopausal participants.
Results
Of 309 participants, 99 (32%) were pre-menopausal. The 60 months cumulative incidence of clinically significant weight gain was greater in pre- than post-menopausal participants (67% vs 43%, p < 0.001). Among pre-menopausal participants, treatment-emergent pain interference (OR 2.49), aromatase inhibitor receipt (OR 2.8), mastectomy, (OR 2.06) and White race (OR 7.13) were associated with weight gain. Among post-menopausal participants, treatment-emergent endocrine symptoms (OR 2.86), higher stage (OR 2.25) and White race (OR 2.29) were associated with weight gain while treatment-emergent physical function decline (OR 0.30) was associated with lower likelihood of weight gain.
Conclusions
Weight gain during AET is common, especially for pre-menopausal women. Clinicodemographic features and early treatment-emergent symptoms may identify at risk individuals.
Implications for cancer survivors
Patients at risk for weight gain can be identified early during AET.
Clinical trials.gov identifier
NCT01937052, registered September 3, 2013.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Obesity, defined as body mass index (BMI) > 30 kg/m2, is common among patients with breast cancer, both at the time of diagnosis and afterwards [1,2,3]. Excess weight is an established risk factor for developing breast cancer in post-menopausal women [4, 5]. Weight gain after breast cancer diagnosis is reported in up to 90% of women, with many studies suggesting pre-menopausal patients are at particular risk for post-diagnosis weight gain [2, 5,6,7,8,9,10,11,12,13,14,15,16,17,18,19]. Weight gain after breast cancer can pose serious health consequences and can cause psychological distress and poor quality of life [10, 20,21,22,23,24,25,26,27,28,29]. Breast cancer survivors with obesity or who gain clinically significant weight face higher risks of recurrence and mortality [4, 10, 26,27,28, 30,31,32,33,34,35,36].
The role of breast cancer therapy in post-diagnosis weight gain is poorly defined. Multiple studies suggest receipt of adjuvant chemotherapy is associated with weight gain; however, whether findings with regard to the association of adjuvant endocrine therapy (AET) and weight gain have been inconsistent [2, 6,7,8,9, 11,12,13,14,15, 17, 18, 28, 37,38,39,40,41,42,43]. Over two thirds of breast cancers are hormone receptor (HR)-positive and at least 5 years of AET reduces recurrence and death in patients with HR-positive disease [39, 44,45,46]. The type of AET administered often differs according to menopausal status, with post-menopausal patients typically receiving an aromatase inhibitor (AI) and pre-menopausal patients receiving either tamoxifen, ovarian function suppression (OFS) with tamoxifen, or OFS with an AI [47,48,49]. While some studies have reported differences in the likelihood of weight gain according to type of AET, others have not, and risk factors for weight gain during AET are not well defined [2, 6,7,8,9, 11,12,13,14].
AET is frequently associated with side effects such as musculoskeletal discomfort, fatigue, sleep disturbance, mood changes, anxiety, and endocrine symptoms including hot flashes and vaginal dryness [29, 47, 50,51,52,53,54,55,56,57,58,59,60,61,62,63,64]. While each of these symptoms may occur with any type of AET, the side effect profile differs somewhat by type of AET, as exemplified by more frequent musculoskeletal symptoms with AIs compared to tamoxifen [11, 50, 65,66,67,68]. Treatment-emergent side effects with AET often develop soon after initiation [69,70,71]. AET and its side effects can affect quality of life, physical activity, sleep, and mood, all of which have been associated with weight gain after breast cancer diagnosis [6, 11, 29, 51,52,53,54,55,56,57,58]. Unfortunately, side effects during AET are not always detected during routine clinical care. The use of patient-reported outcomes (PRO), health assessments from patients without interpretation by a member of the clinical team, typically collected via questionnaires, enhances symptom detection [72,73,74]. To date, evaluation of the association between patient-reported symptoms and weight gain during AET has been limited [6, 11, 29, 38, 51,52,53,54,55,56,57,58].
We report here results of a secondary analysis from a prospective clinic-based cohort of patients with HR-positive breast cancer receiving AET who completed serial PRO symptom assessments over 60 months. Our analysis sheds further light on the association of AET with post-diagnosis weight gain and on risk factors, including patient-reported symptoms, for weight gain during AET. We describe weight trajectories and evaluate associations between clinicodemographic factors and symptoms emerging during the first 6 months of AET with clinically significant weight gain throughout the course of AET. Given prior literature suggesting patterns of weight gain during AET may vary by menopausal status, known differences in the side effect profiles of tamoxifen and AIs and differences in prescribing patterns for these agents according to menopausal status, we conducted analyses separately for pre- and post-menopausal participants[2, 47,48,49,50]. For this secondary analysis, we hypothesized that weight gain during AET is associated with patient-reported treatment-emergent symptoms and that it differs according to menopausal status. Identification of factors associated with weight gain early in the course of AET may allow the opportunity for targeted interventions to prevent weight gain in at-risk breast cancer survivors.
Methods
Study population
Women with HR-positive stage 0-III breast cancer initiating AET with either tamoxifen or an AI were enrolled in an IRB-approved prospective observational clinic-based cohort from March 2012 through December 2016 (ClinicalTrials.gov Identifier: NCT01937052, registered September 3, 2013). The cohort was comprised of a convenience sample of female patients with breast cancer age ≥ 18 years who were seen in medical oncology clinics at Johns Hopkins clinical sites. Potential participants were identified by provider referral or by screening clinic schedules. The type of AET prescribed was at the discretion of the treating provider. In addition to tamoxifen or an AI, pre-menopausal participants could receive concurrent OFS. Participants could enroll when they first started AET or if they were switching from one AET agent to another. Participants were followed until the final PRO questionnaire or the last clinical encounter prior to the date the database was locked (May 15, 2020), whichever was longer. Demographics, cancer characteristics, treatment and menopausal status at diagnosis (classified as pre-menopausal or post-menopausal) were obtained via review of the electronic health record (EHR). Participants were eligible for inclusion in this secondary analysis if baseline weight and at least one follow-up weight were documented in the EHR.
Patient-reported outcomes
PRO measures were administered electronically using the online PatientViewpoint interface [75,76,77]. Questionnaires were administered at baseline and 3, 6, 12, 24, 36, 48 and 60 months later. Measures included in this analysis are the Patient-Reported Outcomes Measurement Information System (PROMIS) Version 1.0 short forms for pain interference, depression, anxiety, fatigue, sleep disturbance and physical function plus the Endocrine Symptom Subscale of the Functional Assessment of Cancer Therapy (FACT-ES) [59, 78,79,80]. We defined treatment-emergent symptoms as changes in PRO scores compared to baseline during the first 6 months of AET (i.e. at the 3 and/or 6-month time points) that met or exceeded the minimal important difference (MID) for each measure in the direction indicative of worsening symptoms. The MID is the change in score on a PRO measure that represents the smallest difference perceived by patients as beneficial or harmful and that would impact clinical management [81]. PROMIS measures are scored with a T-score metric for which 50 is the population mean and 10 is the population standard deviation (SD). A higher score indicates more of the outcome measured. PROMIS measures have been validated in patients with early stage cancer with a MID of 3–5 points [78,79,80, 82, 83]. We considered the mid-point of this range, 4 points, as the MID for the PROMIS questionnaires in this analysis. Scores on the Endocrine Symptom Subscale of the FACT-ES range from 0–76, with lower scores indicative of worse endocrine symptoms. We used 0.5 SD to define a medium effect size as a conservative estimate of the MID for the Endocrine Symptom Subscale of the FACT-ES based on the distribution-based, Effect Size Method of identifying a MID for a PRO measure. In prior studies using the Endocrine Symptom Subscale of the FACT-ES in patients with early stage breast cancer, the reported mean (SD) was 59 (9.7), thus we halved the SD and rounded this estimate to 5 points to identify the MID for this analysis [59, 81, 84].
Weight and body mass index
Weight (in kg) and BMI were obtained from the EHR using measurements assessed during routine clinic visits. BMI was categorized according to the World Health Organization categorization as underweight (< 18.5 kg/m2), normal weight (18.5 kg/m2 – 24.9 kg/m2), overweight (25 kg/m2 – 29.9 kg/m2), or obese (> 30 kg/m2) [3, 85]. Per study protocol, the heaviest weight and BMI documented in the medical record within ± 30 days of questionnaire collection was used in analysis. If a patient did not have a weight or BMI documented in the medical record within ± 30 days of each questionnaire time point, the weight value was missing for that time point. Consistent with the threshold used in many prior studies, we defined clinically significant weight gain as weight gain of ≥ 5% compared to baseline, a weight change that has been associated with increased all-cause mortality after breast cancer [10, 11, 27, 28, 42].
Statistical analysis
Participant demographics, cancer characteristics, cancer treatment, weight, BMI and PRO scores are presented with descriptive statistics including mean (SD), median (range) and proportions. Clinically significant weight gain status was treated as a dichotomous variable indicating whether patients experienced ≥ 5% weight gain from baseline at each time point. Differential changes in weight gain status over time between the pre- and post-menopausal groups were assessed with a mixed effects logistic regression model and corresponding interaction terms. Differences in the proportion of patients with treatment-emergent symptoms according to menopause status were assessed with Fisher’s exact tests.
To estimate the incidence of weight gain during follow-up, time to weight gain was calculated as the time from baseline to either the first study time point where patients experienced ≥ 5% weight gain or last follow-up visit if they did not gain ≥ 5% weight. The cumulative incidence of weight gain was estimated using the Kaplan–Meier method.
We evaluated the association of clinicodemographic factors and symptoms emerging during the first 6 months of AET with clinically significant weight gain using univariate and multivariate logistic regression modeling with generalized estimating equations (GEE) to account for the longitudinal design and correlation of repeated measures within a participant. Univariate associations were estimated separately according to menopause status. Factors differentially associated with weight gain by menopause status were explored using interaction terms in the models. Multivariate models were estimated separately for pre- and post-menopausal participants using a forward and backward stepwise selection approach based on Quasi-likelihood under the Independence model Criterion (QIC)[86]. The models with the lowest QIC were selected. Non-time dependent demographic variables included in the models were age at enrollment, race (White versus Black/Other) and neighborhood poverty (NP) level. NP level was defined as the percentage of persons living in a zip code with a family income below the federal poverty line (based on United States 2010 census data); this was used as a surrogate for socioeconomic status (SES) with NP level > 15% considered an indicator of low SES [87]. Non-time dependent clinical variables included baseline PRO scores, baseline BMI category (overweight/obese compared to normal/underweight), prior radiation (yes/no), prior chemotherapy (yes/no), mastectomy (yes/no), stage (classified as a continuous variable), number of concomitant medications at baseline (self-reported), and type of AET (AI or tamoxifen). Since only 4 pre-menopausal participants received an AI, we conducted a sensitivity analysis re-running the model selection for the pre-menopausal participants excluding the variable for type of AET. There was no formal hypothesis testing nor sample size considerations for this study. The findings presented here are for descriptive purposes and no adjustments for multiple comparisons were made. Analyses were performed with R version 4.0.3 [88].
Results
Participant characteristics
Of the 321 participants in the overall cohort, baseline and at least one follow-up weight were available for 309 participants, who were therefore included in this secondary analysis. The 12 participants excluded from this analysis due to missing weight were generally similar to the 309 who were included (Supplemental Table 1). Among participants included in this analysis, 263 (85.1%) had stage I-II disease, 99 (32%) were pre-menopausal, and 259 (83.8%) were White. Prior to initiating AET, 140 (45.3%) underwent mastectomy, 205 (66.3%) received radiation and 86 (28%) received chemotherapy. More pre-menopausal participants than post-menopausal participants received prior chemotherapy (33.7% versus 25.4%). Overall, 132 (42.7%) participants initiated tamoxifen and 177 (57.3%) initiated an AI. The type of AET differed according to menopausal status. Ninety-five (96%) and 4 (4%) pre-menopausal participants initiated tamoxifen and AI, respectively. In contrast, 37 (17.6%) and 173 (82.4%) post-menopausal participants initiated tamoxifen and AI, respectively. Seventeen (17.2%) pre-menopausal participants received OFS. Only 5 participants enrolled upon switching form one type of AET to another. Median follow-up was 56 months (Table 1).
Mean (SD) BMI at baseline for the entire study population included in this analysis was 27.5 kg/m2 (5.8). Baseline BMI was in the overweight category for 91 (29.4%) participants and in the obese category for 100 (32.2%) participants (Table 1). The distribution of baseline BMI categories differed by menopausal status with 47 (47.4%) pre-menopausal compared to 144 (68.6%) post-menopausal participants having a baseline BMI ≥ 25 kg/m2 (p < 0.001) (Supplemental Table 2). At baseline, 158 (61%) White participants, 24 (75%) Black participants and 9 (50%) participants of other race were overweight or obese.
Weight gain
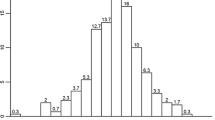
Overall, 121 (39.2%) participants experienced ≥ 5% weight gain compared to baseline on at least one follow-up assessment. Clinically significant weight gain frequently occurred early, with a cumulative incidence of 19% experiencing ≥ 5% weight gain by 12 months after AET initiation, and continued over time, with a cumulative incidence of 52% experiencing ≥ 5% weight gain by 60 months after AET initiation. The proportions of pre-menopausal and post-menopausal participants who gained ≥ 5% weight compared to baseline both increased over the course of follow-up (p-values evaluating weight gain status over time within pre-menopausal and post-menopausal groups both < 0.001). However, compared to post-menopausal participants, significantly more pre-menopausal participants gained ≥ 5% weight over the course of follow-up (interaction p-value < 0.001). By 60 months, the cumulative incidence of ≥ 5% weight gain compared to baseline was 67% for pre-menopausal and 43% for post-menopausal participants (Fig. 1). Mean (SD) weight gain by 60 months for pre- and post-menopausal participants was 3.5 (10.4) kg and 0.6 (6.5) kg, respectively. The number of patients with missing weight measurements increased over time for both pre- and post-menopausal participants (Supplemental Table 3).

Cumulative Incidence of Clinically Significant Weight Gain at Each Time Point by Menopausal Status. Bars indicate the cumulative incidence of experiencing ≥ 5% weight gain compared to baseline at each time point. Gray bars indicate the overall population; blue bars indicate the post-menopausal participants; and orange bars indicate the pre-menopausal participants. Abbreviations: MOS = Months
Scores on PRO measures
Overall, mean scores on each PRO measure at baseline, 3 and 6 months were within one SD of population means. The number of completed questionnaires declined through follow-up (Supplemental Table 4). Treatment-emergent symptoms, defined as changes in PRO scores compared to baseline at the 3 and/or 6-month time points that met or exceeded the MID in the direction indicative of worsening symptoms, were common, each occurring in 23%-42% of the overall study population (Fig. 2). Endocrine symptoms (42%) and sleep disturbance (37%) were the most common treatment-emergent symptoms, followed by fatigue (30%), anxiety (28%) and depression (26%). There were no statistically significant differences in the proportions of pre-menopausal and post-menopausal participants who experienced each type of treatment-emergent symptom (Fisher’s exact test p-values all > 0.05).

Proportions of Participants with Treatment-Emergent Symptoms by Menopausal Status. Bars indicate the proportion of participants who experienced treatment-emergent symptoms, defined as changes in PRO scores compared to baseline at the 3 and/or 6-month time points that met or exceeded the MID in the direction indicative of worsening symptoms; Gray bars indicate the overall population; blue bars indicate the post-menopausal participants; and orange bars indicate the pre-menopausal participants. Abbreviations: PRO = Patient-Reported Outcome, MID = Minimal Important Difference
Association of treatment-emergent symptoms and clinicodemographic factors with weight gain in pre-menopausal and post-menopausal participants
Univariate and multivariate logistic regression analyses of factors associated with ≥ 5% weight gain compared to baseline are shown in Table 2. In univariate analyses among pre-menopausal participants, prior mastectomy (Odds Ratio [OR] 2.23, 95% Confidence Interval (CI) 1.00–4.96, p = 0.05) and White race (OR 6.45, 95% CI 1.18–35.25, p = 0.03) were associated with weight gain while participants with obesity at baseline were less likely to gain ≥ 5% weight compared to baseline than those who were normal weight or underweight at baseline (OR 0.30, 95% CI 0.10–0.93, p = 0.04). In univariate analysis among post-menopausal participants, higher tumor stage (OR 1.84, 95% CI 1.27–2.67, p = 0.001) and treatment-emergent endocrine symptoms (OR 2.05, 95% CI 1.10–3.82, p = 0.02) were associated with greater likelihood of ≥ 5% weight gain while treatment-emergent decline in physical function was associated with lower likelihood of ≥ 5% weight gain (OR 0.36, 95% CI 0.16–0.83, p = 0.02). The associations of treatment-emergent change in physical function and treatment-emergent pain interference with weight gain status differed by menopausal status (interaction p-values both ≤ 0.05).
Different variables were selected for the final multivariate models of factors associated with clinically significant weight gain among pre-and post-menopausal participants. In the final pre-menopausal model, receipt of AI as opposed to tamoxifen (OR 2.8, 95% CI 0.9–8.77, p = 0.08), prior mastectomy (OR 2.06, 95% CI 0.89–4.77, p = 0.09), treatment-emergent pain interference (OR 2.49, 95% CI 0.99–6.24, p = 0.05) and White race (OR 7.13, 95% CI 1.29–39.38, p = 0.02) were associated with greater likelihood of weight gain ≥ 5% compared to baseline. In the final post-menopausal model, treatment-emergent endocrine symptoms (OR 2.86, 95% CI 1.55–5.26, p < 0.001), higher stage (OR 2.25, CI 1.52–3.34, p < 0.001), and White race (OR 2.29, 95% CI 0.82–6.37, p = 0.11) were associated with greater likelihood of ≥ 5% weight gain compared to baseline while treatment-emergent decline in physical function (OR 0.3, 95% CI 0.13–0.68, p = 0.004) was associated with lower likelihood of ≥ 5% weight gain compared to baseline. In addition, compared to post-menopausal participants with baseline BMI < 25 kg/m2, those with baseline BMI ≥ 30 kg/m2 were less likely to gain ≥ 5% weight compared to baseline (OR 0.56, 95% CI 0.27–1.18, p = 0.13). In our sensitivity analysis, after excluding the type of AET as a candidate variable for the model for pre-menopausal participants, the model selected included the same variables with similar effect sizes (Supplemental Table 5).
Discussion
In this study, we confirmed that clinically significant weight gain, defined as ≥ 5% compared to baseline, is an important problem, with a cumulative incidence by 5 years after AET initiation of 52% in our study population. While weight gain began soon after initiation of AET for some participants, it occurred later for others. Although pre-menopausal participants were less likely than post-menopausal participants to have BMI ≥ 25 kg/m2 at baseline, they were more likely to gain ≥ 5% weight by 60 months (67% versus 43%). An additional key finding of our study is that early treatment-emergent symptoms, defined as changes in PRO scores compared to baseline at the 3 and/or 6-month time points that were in the direction indicative of worsening symptoms and that met or exceeded the MID, were frequent, and, in multivariable modeling, were associated with clinically significant weight gain through 5 years of AET in both pre- and post-menopausal participants.
While previous literature has consistently demonstrated an association between adjuvant chemotherapy and weight gain, findings with regard to whether AET is associated with weight gain have been variable across prior studies [6, 7, 13, 17, 37, 41,42,43, 89]. Our study, in which the majority of participants did not receive chemotherapy, confirms that weight gain during AET itself is a clinically important problem, although the observational design precludes determination of causality. The mechanisms behind weight gain during adjuvant therapy for breast cancer are not clearly defined, but may include factors such as reduced physical activity, dietary changes, increased insulin resistance and inflammation [4, 41, 89, 90]. Additionally, treatment-induced menopause, a transition that may impact physiologic fat accumulation and body composition, may explain the greater weight gain we and others have observed among pre-menopausal compared to post-menopausal women [2, 7,8,9, 13, 15, 18, 19, 91,92,93,94]. Furthermore, young women may be at particular risk for weight gain during adjuvant therapy because responsibilities like career and family may take time away from exercise and healthy eating [11].
A novel aspect of our study is that we identified early patient-reported treatment-emergent symptoms (defined as changes in PRO scores compared to baseline at the 3 and/or 6-month time points that met or exceeded the MID in the direction indicative of worsening symptomatology), that, in combination with baseline clinicodemographic factors, were associated with clinically significant weight gain over 5 years of AET. Among participants who were pre-menopausal at diagnosis, patient-reported treatment-emergent pain interference was associated with ~ 2.5-fold higher likelihood of clinically significant weight gain. Although associated with weight gain in univariate analysis in the pre-menopausal participants, treatment-emergent fatigue and depression were not selected for the final model. In post-menopausal participants, patient-reported treatment-emergent endocrine symptoms were associated with 2.86 times higher likelihood of ≥ 5% weight gain while patient-reported treatment-emergent decline in physical function was associated with a 70% lower likelihood of clinically significant weight gain.
Few prior studies have evaluated associations between patient-reported symptoms during AET and weight gain. Available data suggest worsening sexual function, physical activity, endocrine symptoms, sleep disturbance, pain, fatigue and anxiety are associated with weight gain [11, 29, 52, 58, 95,96,97,98]. Weight gain is also associated with changes in patient-reported function [11, 51]. Additionally, avoidance of weight gain and maintenance of physical activity are associated with reduced patient-reported symptoms, improved function and improved quality of life [55, 99]. Our study builds on this limited data by comprehensively evaluating multiple common AET-associated symptoms in one cohort and demonstrating that early treatment-emergent symptoms during AET are associated with weight gain over 5 years of AET. Moreoever, our study demonstrates that the relationship of specific treatment-emergent symptoms with weight gain varies by menopausal status and that MIDs on PRO measures can detect clinically relevant changes in symptom severity early during AET that are associated with weight gain throughout the course of AET. While further research is needed to confirm these associations between early treatment-emergent symptoms and weight gain during AET in pre- and post-menopausal women, our study suggests that treatment-emergent symptoms identified using changes in PRO scores that meet or exceed the MID in the direction indicative of worsening symptoms may be used to identify patients at risk for weight gain during AET.
The mechanisms linking changes in symptoms and weight gain during AET are uncertain. Reduced physical activity due to joint pain while receiving AET may explain the relationship we observed between increased pain interference and weight gain during AET in pre-menopausal participants [11, 29, 95]. The relationship we observed between declining physical function and lower likelihood of weight gain during AET in post-menopausal participants may be attributable to loss of muscle mass in the setting of frailty. Disrupted sleep due to vasomotor symptoms may lead to fatigue, reduced exercise, and weight gain, explaining the relationship we observed between endocrine symptoms and weight gain in post-menopausal participants. Additionally, other endocrine symptoms such as breast tenderness, mood swings and irritability might lead to decreased physical activity and, in turn, to weight gain.
A difference in likelihood of clinically significant weight gain according to race was seen in both pre-menopausal and post-menopausal participants, with > 5% weight gain from baseline more frequent in White participants. Racial differences in weight gain after breast cancer have been mixed in prior studies. [8, 100,101,102,103]. It is possible that differences in weight gain during AET by race are attributable to differences in diet, activity or baseline BMI. While statistically significant, interpretation of differences according to race in this analysis should be made with caution since the majority of participants were White.
Among pre-menopausal participants in our study, prior mastectomy and receipt of AI compared to tamoxifen were also associated with weight gain. Weight gain after mastectomy has previously been reported and may be attributable to post-operative upper extremity and chest wall pain, numbness, and decreased range of motion leading to decreased ability to exercise [9, 104]. While pain interference was associated with weight gain in pre-menopausal women, AI receipt was also independently associated with weight gain potentially due to other side effects not captured on the PROMIS pain interference measure, a tool not specific to joint pain, that may lead to reduced physical activity and weight gain [95]. Additionally, in pre-menopausal women, AI therapy requires induction of menopause via either OFS or ablation which can alter metabolism and lead to weight gain [45, 47, 94, 105].
Among the post-menopausal participants in our study, lower BMI at baseline and higher stage were also associated with weight gain. Lower baseline BMI is a known risk factor for weight gain since 5% body weight in a person with a lower BMI is less absolute weight than in someone with a higher BMI [15, 102, 106]. Our study is consistent with other literature showing patients with higher stage breast cancer are at higher risk of weight gain likely due to different treatment regimens, more intense surgery or radiation treatments which could contribute to the risk of weight gain [2, 9, 18, 106].
Several recent trials have evaluated weight gain prevention and weight loss interventions for patients receiving treatment for breast cancer and for breast cancer survivors, with early data supporting efficacy with regard to weight endpoints [107,108,109,110,111,112,113,114,115,116,117]. Longer term follow-up of these studies and ongoing trials such as the Breast Cancer Weight Loss (BWEL) Study (NCT02750826) will determine if weight loss interventions translate into improvements in breast cancer survival outcomes also. Examples of interventions evaluated to date include face-to-face dietary counseling, telephone dietary counseling, physical exercise regimens and cooking classes, with combined dietary and physical exercise interventions exhibiting the most promising results [107,108,109,110,111,112,113,114,115]. Given the association between treatment-emergent symptoms and weight gain during AET, it is conceivable that symptom management using evidence- based strategies to manage AET-associated symptoms could mitigate weight gain also [50]. However, to successfully implement weight gain prevention strategies during AET, it is critical to identify at risk patients in whom the interventions may be most impactful. Our study indicates that treatment-emergent symptoms, as reported by patients soon after AET initiation, and baseline clinicodemographic variables can identify patients at particular risk for clinically significant weight gain during AET. In the future, this finding may translate into a strategy to identify patients to whom early interventions to prevent weight gain could be targeted. Additionally, this study and our prior publication, in which we reported symptoms over the 5-year course of AET in this cohort, demonstrate that PRO measures can identify clinically meaningful treatment-emergent symptoms during AET, potentially offering the opportunity for enhanced symptom management strategies that may, secondarily, lead to lower likelihood of weight gain [118].
Strengths of our study include use of clinically obtained weight and height assessments (as opposed to patient-reported measures), frequent weight assessment time points, use of a defined threshold for clinically significant weight gain that is supported by prior literature, and longer follow-up than many prior studies that focused on short-term weight gain during AET [2, 9, 11, 12, 15, 17,18,19, 93]. The large sample size and contemporary real-world population are also strengths of this study supporting generalizability of our findings. Additionally, our use of validated PRO measures assessing common symptoms during AET at baseline and early during the course of AET plus our use of MID values to define PRO score changes that represent clinically meaningful treatment-emergent symptoms are strengths of this study. Furthermore, the fact that we built separate models for the factors associated with clinically significant weight gain in pre- and post-menopausal participants and that we used the QIC model selection approach to build the multivariable models are other strengths of this study. The QIC model selection strategy is optimal for use with longitudinal data with repeated measures in individual participants and results in models with overall good correlation structure and fit. It must be stated, however, that the QIC model selection approach is based on model likelihood, thus selection of variables for inclusion in a multivariable model is not driven by a p-value threshold. As such, the QIC model selection approach can yield final models in which variables with p > 0.05 are included as occurred in this study [86]. However, the directionality of the odds ratios in the final models we present supports the relationships between the selected variables and clinically significant weight gain despite some p-values exceeding 0.05.
Our study also has weaknesses. Given that it was performed at a single institution in the United States with a predominantly White population and that few pre-menopausal participants received OFS and/or an AI, generalizability may be limited. In addition, missing PRO data due to incomplete surveys, reasons for which are unknown, and missing weight data, due to the fact that weight assessments were only available if a participant had a routine clinical visit within the designated windows around PRO time points, are limitations. Furthermore, we did not have information about specific concomitant medications, such as anti-depressants, which can influence weight and may potentially confound the relationship between the variables evaluated and weight gain. We also did not have information about diet, physical activity or other comorbid health conditions, all of which may also be associated with weight gain. Nor did we collect data on other body anthropometrics beyond weight and BMI, such as weight circumference or body fat. Additionally, while the fact that we performed analyses separately according to menopausal status is a strength of our study, it must be noted that we assessed menopausal status at diagnosis and did not capture changes in menopausal status over time and differences in patterns of treatment-emergent symptoms by menopausal status may have largely been driven by differences in receipt of AIs versus tamoxifen in pre- and post-menopausal participants. Further, although a change in a PRO score meeting or exceeding the MID is considered clinically meaningful, it is not certain that a change of this extent is necessarily the minimal significant change and MID thresholds may vary in different clinical scenarios [81]. It is possible that, if anchored to weight gain, different MID thresholds on the PRO measures could be identified, strengthening or weakening the associations between early treatment-emergent symptoms and clinically significant weight gain during AET that we identified. Finally, all analyses presented are exploratory and were not pre-specified in the study protocol.
In conclusion, this study confirms that weight gain during AET for early breast cancer is an important clinical problem, especially in pre-menopausal patients. There are almost 4 million breast cancer survivors in the United States and those who are overweight or obese face inferior outcomes with regard to breast cancer, mental health and cardiovascular health [4, 10, 20,21,22,23,24,25,26,27,28, 30, 31, 34,35,36, 119]. Strategies to prevent weight gain in breast cancer survivors are an unmet need. We demonstrated that patient-reported treatment-emergent symptoms early during AET and clinicodemographic factors present at AET initiation are associated with weight gain over the course of AET, indicating that patients at risk for clinically significant weight gain can be identified and potentially targeted for weight gain prevention interventions. Future studies should evaluate use of the factors associated with weight gain identified in this study to select pre- and post-menopausal breast cancer patients receiving AET for weight gain prevention interventions, with the ultimate goal of preventing the adverse health effects associated with weight gain and obesity after breast cancer.
Data availability
The datasets generated during and analyzed during the current study are available from the corresponding author on reasonable request.
References
Nyrop KA, Damone EM, Deal AM, Carey LA, Lorentsen M, Shachar SS, et al. Obesity, comorbidities, and treatment selection in Black and White women with early breast cancer. Cancer. 2021;127:922–30. https://doi.org/10.1002/cncr.33288.
Nyrop KA, Deal AM, Shachar SS, Park J, Choi SK, Lee JT, et al. Weight trajectories in women receiving systemic adjuvant therapy for breast cancer. Breast Cancer Res Treat. 2020;179:709–20. https://doi.org/10.1007/s10549-019-05501-8.
Obesity WC on. Obesity: preventing and managing the global epidemic. Report of a WHO consultation. World Health Organ Tech Rep Ser 2000
Picon-Ruiz M, Morata-Tarifa C, Valle-Goffin JJ, Friedman ER, Slingerland JM. Obesity and adverse breast cancer risk and outcome: Mechanistic insights and strategies for intervention. CA Cancer J Clin. 2017;67:378–97. https://doi.org/10.3322/caac.21405.
Renehan AG, Tyson M, Egger M, Heller RF, Zwahlen M. Body-mass index and incidence of cancer: a systematic review and meta-analysis of prospective observational studies. The Lancet. 2008;371:569–78. https://doi.org/10.1016/S0140-6736(08)60269-X.
Nyrop KA, Williams GR, Muss HB, Shachar SS. Weight gain during adjuvant endocrine treatment for early-stage breast cancer: What is the evidence? Breast Cancer Res Treat. 2016;158:203–17. https://doi.org/10.1007/s10549-016-3874-0.
Vance V, Mourtzakis M, Mccargar L, Hanning R. Weight gain in breast cancer survivors: Prevalence, pattern and health consequences. Obes Rev. 2011;12:282–94. https://doi.org/10.1111/j.1467-789X.2010.00805.x.
Raghavendra A, Sinha AK, Janeiro Valle Y, Shen DT, Barcenas CH. Determinants of Weight Gain during Adjuvant Endocrine Therapy and Association of Such Weight Gain with Recurrence in Long-Term Breast Cancer Survivors. Clin Breast Cancer. 2018;18:7–13. https://doi.org/10.1016/j.physbeh.2017.03.040.
Nyrop KA, Deal AM, Lee JT, Muss HB, Choi SK, Wheless A, et al. Weight gain in hormone receptor-positive (HR+) early-stage breast cancer: is it menopausal status or something else? Breast Cancer Res Treat. 2018;167:235–48. https://doi.org/10.1007/s10549-017-4501-4.
Playdon MC, Bracken MB, Sanft TB, Ligibel JA, Harrigan M, Irwin ML. Weight Gain After Breast Cancer Diagnosis and All-Cause Mortality: Systematic Review and Meta-Analysis. J Natl Cancer Inst. 2015;107:djv275. https://doi.org/10.1093/jnci/djv275.
Meglio AD, Michiels S, Jones LW, El-Mouhebb M, Ferreira AR, Martin E, et al. Changes in weight, physical and psychosocial patient-reported outcomes among obese women receiving treatment for early-stage breast cancer: A nationwide clinical study. Breast. 2020;52:23–32. https://doi.org/10.1016/j.breast.2020.04.002.
Heideman WH, Russell NS, Gundy C, Rookus MA, Voskuil DW. The frequency, magnitude and timing of post-diagnosis body weight gain in Dutch breast cancer survivors. Eur J Cancer. 2009;45:119–26. https://doi.org/10.1016/j.ejca.2008.09.003.
Goodwin PJ, Ennis M, Pritchard KI, Mccready D, Koo J, Sidlofsky S, et al. Adjuvant Treatment and Onset of Menopause Predict Weight Gain After Breast Cancer Diagnosis. 1999 vol. 17
Sadim M, Xu Y, Selig K, Paulus J, Uthe R, Agarwl S, et al. A prospective evaluation of clinical and genetic predictors of weight changes in breast cancer survivors. Cancer. 2017;123:2413–21. https://doi.org/10.1002/cncr.30628.
Makari-Judson G, Judson CH, Mertens WC. Longitudinal Patterns of Weight Gain after Breast Cancer Diagnosis: Observations beyond the First Year. Breast J. 2007;13:258–65. https://doi.org/10.1111/j.1524-4741.2007.00419.x.
Vrieling A, Buck K, Kaaks R, Chang-Claude J. Adult weight gain in relation to breast cancer risk by estrogen and progesterone receptor status: a meta-analysis. Breast Cancer Res Treat. 2010;123:641–9. https://doi.org/10.1007/s10549-010-1116-4.
Nyrop KA, Deal AM, Lee JT, Muss HB, Choi SK, Dixon S, et al. Weight changes in postmenopausal breast cancer survivors over 2 years of endocrine therapy: a retrospective chart review. Breast Cancer Res Treat. 2017;162:375–88. https://doi.org/10.1007/s10549-017-4106-y.
Irwin ML, McTiernan A, Baumgartner RN, Baumgartner KB, Bernstein L, Gilliland FD, et al. Changes in body fat and weight after a breast cancer diagnosis: Influence of demographic, prognostic, and lifestyle factors. J Clin Oncol. 2005;23:774–82. https://doi.org/10.1200/JCO.2005.04.036.
Sella T, Zheng Y, Tan-Wasielewski Z, Rosenberg SM, Poorvu PD, Tayob N, et al. Body weight changes and associated predictors in a prospective cohort of young breast cancer survivors. Cancer. 2022;128:3158–69. https://doi.org/10.1002/cncr.34342.
Howard-Anderson J, Ganz PA, Bower JE, Stanton AL. Quality of life, fertility concerns, and behavioral health outcomes in younger breast cancer survivors: A systematic review. J Natl Cancer Inst. 2012;104:386–405. https://doi.org/10.1093/jnci/djr541.
Pedersen B, Groenkjaer M, Falkmer U, Delmar C. Understanding the Essential Meaning of Measured Changes in Weight and Body Composition among Women during and after Adjuvant Treatment for Breast Cancer: A Mixed-Methods Study. Cancer Nurs. 2017;40:433–44. https://doi.org/10.1097/NCC.0000000000000427.
Rosenberg SM, Tamimi RM, Gelber S, Ruddy KJ, Kereakoglow S, Borges VF, et al. Body image in recently diagnosed young women with early breast cancer. Psychooncology. 2013;22:1849–55. https://doi.org/10.1002/pon.3221.
Feliciano EMC, Kwan ML, Kushi LH, Weltzien EK, Castillo AL, Caan BJ. Adiposity, post-diagnosis weight change, and risk of cardiovascular events among early-stage breast cancer survivors. Breast Cancer Res Treat n.d.;162. https://doi.org/10.1007/s10549-017-4133-8
Gernaat SAM, Boer JMA, van den Bongard DHJ, Maas AHEM, van der Pol CC, Bijlsma RM, et al. The risk of cardiovascular disease following breast cancer by Framingham risk score. Breast Cancer Res Treat. 2018;170:119–27. https://doi.org/10.1007/s10549-018-4723-0.
Herman DR, Ganz PA, Petersen L, Greendale GA. Obesity and cardiovascular risk factors in younger breast cancer survivors: The Cancer and Menopause Study (CAMS). Breast Cancer Res Treat. 2005;93:13–23. https://doi.org/10.1007/s10549-005-2418-9.
Nichols HB, Trentham-Dietz A, Egan KM, Titus-Ernstoff L, Holmes MD, Bersch AJ, et al. Body mass index before and after breast cancer diagnosis: Associations with all-cause, breast cancer, and cardiovascular disease mortality. Cancer Epidemiol Biomarkers Prev. 2009;18:1403–9. https://doi.org/10.1158/1055-9965.EPI-08-1094.
Chan DSM, Vieira AR, Aune D, Bandera EV, Greenwood DC, McTiernan A, et al. Body mass index and survival in women with breast cancer—systematic literature review and meta-analysis of 82 follow-up studies. Ann Oncol. 2014;25:1901–14. https://doi.org/10.1093/annonc/mdu042.
Mutschler NS, Scholz C, Friedl TWP, Zwingers T, Fasching PA, Beckmann MW, et al. Prognostic Impact of Weight Change During Adjuvant Chemotherapy in Patients With High-Risk Early Breast Cancer: Results From the ADEBAR Study. Clin Breast Cancer. 2018;18:175–83. https://doi.org/10.1016/j.clbc.2018.01.008.
Forsythe LP, Alfano CM, George SM, McTiernan A, Baumgartner KB, Bernstein L, et al. Pain in long-term breast cancer survivors: The role of body mass index, physical activity, and sedentary behavior. Breast Cancer Res Treat. 2013;137:617–30. https://doi.org/10.1007/S10549-012-2335-7.
Jiralerspong S, Kim ES, Dong W, Feng L, Hortobagyi GN, Giordano SH. Obesity, diabetes, and survival outcomes in a large cohort of early-stage breast cancer patients. Ann Oncol Off J Eur Soc Med Oncol. 2013;24:2506–14. https://doi.org/10.1093/annonc/mdt224.
Bradshaw PT, Ibrahim JG, Stevens J, Cleveland R, Abrahamson PE, Satia JA, et al. Postdiagnosis change in bodyweight and survival after breast cancer diagnosis. Epidemiol Camb Mass. 2012;23:320–7. https://doi.org/10.1097/EDE.0b013e31824596a1.
Protani M, Coory M, Martin JH. Effect of obesity on survival of women with breast cancer: systematic review and meta-analysis. Breast Cancer Res Treat. 2010;123:627–35. https://doi.org/10.1007/s10549-010-0990-0.
Fedele P, Orlando L, Schiavone P, Quaranta A, Lapolla AM, De Pasquale M, et al. BMI variation increases recurrence risk in women with early-stage breast cancer. Future Oncol. 2014;10:2459–68. https://doi.org/10.2217/fon.14.180.
Nechuta S, Chen WY, Cai H, Poole EM, Kwan ML, Flatt SW, et al. A Pooled Analysis of Post-diagnosis Lifestyle Factors in Association with Late Estrogen-Receptor Positive Breast Cancer Prognosis. Int J Cancer J Int Cancer. 2016;138:2088–97. https://doi.org/10.1002/ijc.29940.
Pang Y, Wei Y, Kartsonaki C. Associations of adiposity and weight change with recurrence and survival in breast cancer patients: a systematic review and meta-analysis. Breast Cancer Tokyo Jpn. 2022;29:575–88. https://doi.org/10.1007/s12282-022-01355-z.
Ewertz M, Jensen M-B, Gunnarsdóttir KÁ, Højris I, Jakobsen EH, Nielsen D, et al. Effect of Obesity on Prognosis After Early-Stage Breast Cancer. J Clin Oncol. 2011;29:25–31. https://doi.org/10.1200/JCO.2010.29.7614.
Berg MMGA, Winkels RM, Kruif JTCM, Laarhoven HWM, Visser M, Vries JHM, et al. Weight change during chemotherapy in breast cancer patients: A meta-analysis. BMC Cancer. 2017;17:259. https://doi.org/10.1186/s12885-017-3242-4.
Kumar N, Allen KA, Riccardi D, Bercu BB, Cantor A, Minton S, et al. Fatigue, weight gain, lethargy and amenorrhea in breast cancer patients on chemotherapy: Is subclinical hypothyroidism the culprit? Breast Cancer Res Treat. 2004;83:149–59. https://doi.org/10.1023/B:BREA.0000010708.99455.e1.
(EBCTCG) EBCTCG. Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials Early. Lancet. 2005;365:1687–717. https://doi.org/10.1016/S0140-6736(05)66544-0.
Sedjo RL, Hines LM, Byers T, Giuliano AR, Marcus A, Vadaparampil S, et al. Long-Term Weight Gain Among Hispanic and Non-Hispanic White Women with and Without Breast Cancer) Long-Term Weight Gain Among Hispanic and Non-Hispanic White Women with and Without. Breast Cancer Nutr Cancer. 2013;65:34–42. https://doi.org/10.1080/01635581.2013.741750.
Makari-Judson G, Braun B, Jerry DJ, Mertens WC. Weight gain following breast cancer diagnosis: Implication and proposed mechanisms. World J Clin Oncol. 2014;5:272–82. https://doi.org/10.5306/wjco.v5.i3.272.
Saquib N, Flatt SW, Natarajan L, Thomson CA, Bardwell WA, Caan B, et al. Weight gain and recovery of pre-cancer weight after breast cancer treatments: Evidence from the women’s healthy eating and living (WHEL) study. Breast Cancer Res Treat. 2007;105:177–86. https://doi.org/10.1007/s10549-006-9442-2.
Sestak I, Harvie M, Howell A, Forbes JF, Dowsett M, Cuzick J. Weight change associated with anastrozole and tamoxifen treatment in postmenopausal women with or at high risk of developing breast cancer. Breast Cancer Res Treat. 2012;134:727–34. https://doi.org/10.1007/s10549-012-2085-6.
Albain K, Anderson S, Arriagada R, Barlow W, Bergh J, Bliss J, et al. Comparisons between different polychemotherapy regimens for early breast cancer: Meta-analyses of long-term outcome among 100 000 women in 123 randomised trials. The Lancet. 2012;379:432–44. https://doi.org/10.1016/S0140-6736(11)61625-5.
Walsh EM, Smith KL, Stearns V. Management of hormone receptor-positive, HER2-negative early breast cancer. Semin Oncol. 2020;47:187–200. https://doi.org/10.1053/j.seminoncol.2020.05.010.
Waks AG, Winer EP. Breast Cancer Treatment: A Review. JAMA. 2019;321:288–300. https://doi.org/10.1001/jama.2018.19323.
Francis PA, Pagani O, Fleming GF, Walley BA, Colleoni M, Láng I, et al. Tailoring Adjuvant Endocrine Therapy for Premenopausal Breast Cancer. N Engl J Med. 2018;379:122–37. https://doi.org/10.1056/NEJMoa1803164.
Pagani O, Francis PA, Fleming GF, Walley BA, Viale G, Colleoni M, et al. Absolute Improvements in Freedom From Distant Recurrence to Tailor Adjuvant Endocrine Therapies for Premenopausal Women: Results From TEXT and SOFT. J Clin Oncol. 2020;38:1293–303. https://doi.org/10.1200/JCO.18.01967.
Cuzick J, Sestak I, Baum M, Buzdar A, Howell A, Dowsett M, et al. Effect of anastrozole and tamoxifen as adjuvant treatment for early-stage breast cancer: 10-year analysis of the ATAC trial. Lancet Oncol. 2010;11:1135–41. https://doi.org/10.1016/S1470-2045(10)70257-6.
San P, Hospital M, Perachino M, Mastro D, Lambertini M, Lambertini M, et al. Evidence-based approaches for the management of side-effects of adjuvant endocrine therapy in patients with breast cancer. Rev Lancet Oncol. 2021;22:303–16. https://doi.org/10.1016/S1470-2045(20)30666-5.
Young A, Weltzien E, Kwan M, Castillo A, Caan B, Kroenke CH. Pre- to post-diagnosis weight change and associations with physical functional limitations in breast cancer survivors. J Cancer Surviv. 2014;8:539–47. https://doi.org/10.1007/S11764-014-0356-4.
Caan BJ, Emond JA, Su HI, Patterson RE, Flatt SW, Gold EB, et al. Effect of Postdiagnosis Weight Change on Hot Flash Status Among Early-Stage Breast Cancer Survivors. J Clin Oncol. 2012;30:1492–7. https://doi.org/10.1200/JCO.2011.36.8597.
Iioka Y, Iwata T, Yamauchi H. Symptoms and QOL in breast cancer patients receiving hormone therapy in Japan. Breast Cancer. 2020;27:62–9. https://doi.org/10.1007/s12282-019-00993-0.
Alfano CM, Lichstein KL, Vander Wal GS, Smith AW, Reeve BB, McTiernan A, et al. Sleep duration change across breast cancer survivorship: Associations with symptoms and health-related quality of life. Breast Cancer Res Treat. 2011;130:243–54. https://doi.org/10.1007/s10549-011-1530-2.
Phillips SM, McAuley E. Associations between self-reported post-diagnosis physical activity changes, body weight changes, and psychosocial well-being in breast cancer survivors. Support Care Cancer. 2015;23:159–67. https://doi.org/10.1007/s00520-014-2346-5.
Raggio GA, Butryn ML, Arigo D, Mikorski R, Palmer SC. Prevalence and correlates of sexual morbidity in long-term breast cancer survivors. Psychol Health. 2014;29:632–50. https://doi.org/10.1080/08870446.2013.879136.
Reinertsen KV, Cvancarova M, Loge JH, Edvardsen H, Wist E, Fosså SD. Predictors and course of chronic fatigue in long-term breast cancer survivors. J Cancer Surviv. 2010;4:405–14. https://doi.org/10.1007/s11764-010-0145-7.
Su HI, Sammel MD, Springer E, Freeman EW, Demichele A, Mao JJ. Weight gain is associated with increased risk of hot flashes in breast cancer survivors on aromatase inhibitors. Breast Cancer Res Treat. 2010;124:205–11. https://doi.org/10.1007/s10549-010-0802-6.
Fallowfield LJ, Leaity SK, Howell A, Benson S, Cella D. Assessment of quality of life in women undergoing hormonal therapy for breast cancer: Validation of an endocrine symptom subscale for the FACT-B. Breast Cancer Res Treat. 1999;55:189–99. https://doi.org/10.1023/a:1006263818115.
Francis PA, Regan MM, Fleming GF, Láng I, Ciruelos E, Bellet M, et al. Adjuvant ovarian suppression in premenopausal breast cancer. N Engl J Med. 2015;372:436–46. https://doi.org/10.1056/NEJMoa1412379.
Pagani O, Regan MM, Walley BA, Fleming GF, Colleoni M, Láng I, et al. Adjuvant Exemestane with Ovarian Suppression in Premenopausal Breast Cancer. N Engl J Med. 2014;371:107–18. https://doi.org/10.1056/NEJMoa1404037.
Bernhard J, Luo W, Ribi K, Colleoni M, Burstein HJ, Tondini C, et al. Patient-reported outcomes with adjuvant exemestane versus tamoxifen in premenopausal women with early breast cancer undergoing ovarian suppression (TEXT and SOFT): A combined analysis of two phase 3 randomised trials. Lancet Oncol. 2015;16:848–58. https://doi.org/10.1016/S1470-2045(15)00049-2.
Aiello Bowles EJ, Boudreau DM, Chubak J, Yu O, Fujii M, Chestnut J, et al. Patient-Reported Discontinuation of Endocrine Therapy and Related Adverse Effects Among Women With Early-Stage Breast Cancer. J Oncol Pract. 2012;8:e149–57. https://doi.org/10.1200/JOP.2012.000543.
Brett J, Fenlon D, Boulton M, Hulbert-Williams NJ, Walter FM, Donnelly P, et al. Factors associated with intentional and unintentional non-adherence to adjuvant endocrine therapy following breast cancer. Eur J Cancer Care (Engl). 2018;27:e12601. https://doi.org/10.1111/ecc.12601.
Nyrop KA, Deal AM, Shachar SS, Basch E, Reeve BB, Choi SK, et al. Patient-Reported Toxicities During Chemotherapy Regimens in Current Clinical Practice for Early. Breast Cancer. 2018. https://doi.org/10.1634/theoncologist.2018-0590.
Howell A, Cuzick J, Baum M, Buzdar A, Dowsett M, Forbes JF, et al. Results of the ATAC (Arimidex, Tamoxifen, Alone or in Combination) trial after completion of 5 years’ adjuvant treatment for breast cancer. Lancet Lond Engl. 2005;365:60–2. https://doi.org/10.1016/S0140-6736(04)17666-6.
van de Velde CJ, Rea D, Seynaeve C, Putter H, Hasenburg A, Vannetzel J-M, et al. Adjuvant tamoxifen and exemestane in early breast cancer (TEAM): a randomised phase 3 trial. The Lancet. 2011;377:321–31. https://doi.org/10.1016/S0140-6736(10)62312-4.
Forbes JF, Sestak I, Howell A, Bonanni B, Bundred N, Levy C, et al. Anastrozole versus tamoxifen for the prevention of locoregional and contralateral breast cancer in postmenopausal women with locally excised ductal carcinoma in situ (IBIS-II DCIS): a double-blind, randomised controlled trial. Lancet Lond Engl. 2016;387:866–73. https://doi.org/10.1016/S0140-6736(15)01129-0.
Kadakia KC, Snyder CF, Kidwell KM, Seewald NJ, Flockhart DA, Skaar TC, et al. Patient-Reported Outcomes and Early Discontinuation in Aromatase Inhibitor-Treated Postmenopausal Women With Early Stage Breast Cancer. Oncologist. 2016;21:539–46. https://doi.org/10.1634/theoncologist.2015-0349.
Wagner LI, Zhao F, Goss PE, Chapman J-AW, Shepherd LE, Whelan TJ, et al. Patient-reported predictors of early treatment discontinuation: Treatment-related symptoms and health-related quality of life among postmenopausal women with primary breast cancer randomized to anastrozole or exemestane on NCIC Clinical Trials Group (CCTG) MA.27 (E1Z03). Breast Cancer Res Treat. 2018;169:537–48. https://doi.org/10.1007/s10549-018-4713-2.
Nabieva N, Fehm T, Häberle L, de Waal J, Rezai M, Baier B, et al. Influence of side-effects on early therapy persistence with letrozole in post-menopausal patients with early breast cancer: Results of the prospective EvAluate-TM study. Eur J Cancer. 2018;96:82–90. https://doi.org/10.1016/j.ejca.2018.03.020.
Snyder CF, Jensen RE, Segal JB, Wu AW. Patient-Reported outcomes (pros): putting the patient perspective in patient-centered outcomes research. Med Care. 2013;51:S73–9. https://doi.org/10.1097/MLR.0b013e31829b1d84.
Basch E, Iasonos A, McDonough T, Barz A, Culkin A, Kris MG, et al. Patient versus clinician symptom reporting using the National Cancer Institute Common Terminology Criteria for Adverse Events: results of a questionnaire-based study. Lancet Oncol. 2006;7:903–9. https://doi.org/10.1016/S1470-2045(06)70910-X.
Oberguggenberger A, Hubalek M, Sztankay M, Meraner V, Beer B, Oberacher H, et al. Is the toxicity of adjuvant aromatase inhibitor therapy underestimated? Complementary information from patient-reported outcomes (PROs). Breast Cancer Res Treat. 2011;128:553–61. https://doi.org/10.1007/s10549-011-1378-5.
Snyder CF, Blackford AL, Wolff AC, Carducci MA, Herman JM, Wu AW. Feasibility and value of PatientViewpoint: a web system for patient-reported outcomes assessment in clinical practice. Psychooncology. 2013;22:895–901. https://doi.org/10.1002/PON.3087.
Snyder CF, Jensen R, Courtin SO, Wu AW. PatientViewpoint: a website for patient-reported outcomes assessment. Qual Life Res. 2009;18(7):793–800. https://doi.org/10.1007/S11136-009-9497-8.
Wu AW, White SM, Blackford AL, Wolff AC, Carducci MA, Herman JM, et al. Improving an electronic system for measuring PROs in routine oncology practice. J Cancer Surviv. 2015;10(3):573–82. https://doi.org/10.1007/S11764-015-0503-6.
Jensen RE, Moinpour CM, Potosky AL, Lobo T, Hahn EA, Hays RD, et al. Responsiveness of 8 Patient-Reported Outcomes Measurement Information System (PROMIS) measures in a large, community-based cancer study cohort. Cancer. 2017;123:327–35. https://doi.org/10.1002/cncr.30354.
Jensen RE, Potosky AL, Moinpour CM, Lobo T, Cella D, Hahn EA, et al. United States population-based estimates of patient-reported outcomes measurement information system symptom and functional status reference values for individuals with cancer. J Clin Oncol. 2017;35:1913–20. https://doi.org/10.1200/JCO.2016.71.4410.
Schalet BD, Pilkonis PA, Yu L, Dodds N, Johnston KL, Yount S, et al. Clinical Validity of PROMIS® Depression, Anxiety, and Anger across Diverse Clinical Samples. J Clin Epidemiol. 2017;73:119–27. https://doi.org/10.1016/j.jclinepi.2015.08.036.
Revicki D, Hays RD, Cella D, Sloan J. Recommended methods for determining responsiveness and minimally important differences for patient-reported outcomes. J Clin Epidemiol. 2008;61:102–9. https://doi.org/10.1016/j.jclinepi.2007.03.012.
Teresi JA, Ocepek-Welikson K, Kleinman M, Ramirez M, Kim G. Measurement Equivalence of the Patient Reported Outcomes Measurement Information System ® (PROMIS ® ) Anxiety Short Forms in Ethnically Diverse Groups HHS Public Access. 2016 vol. 58
Yost KJ, Eton DT, Garcia SF, Cella D. Minimally important differences were estimated for six PROMIS-Cancer scales in advanced-stage cancer patients n.d. https://doi.org/10.1016/j.jclinepi.2010.11.018.
Sloan JA, Dueck A. Issues for Statisticians in Conducting Analyses and Translating Results for Quality of Life End Points in Clinical Trials. J Biopharm Stat. 2004;14:73–96. https://doi.org/10.1081/BIP-120028507.
World Health Organization. The SuRF report 2: surveillance of chronic disease risk factors : country-level data and comparable estimates. Geneva: WHO; 2005.
Pan W. Akaike’s information criterion in generalized estimating equations. Biometrics. 2001;57:120–5. https://doi.org/10.1111/j.0006-341x.2001.00120.x.
Zager S, Mendu ML, Chang D, Bazick HS, Braun AB, Gibbons FK, et al. Neighborhood poverty rate and mortality in patients receiving critical care in the academic medical center setting. Chest. 2011;139:1368–79. https://doi.org/10.1378/chest.10-2594.
R Core Team (2020). — European Environment Agency n.d. https://www.eea.europa.eu/data-and-maps/indicators/oxygen-consuming-substances-in-rivers/r-development-core-team-2006 (accessed May 16, 2022)
Nissen MJ, Shapiro A, Swenson KK. Changes in weight and body composition in women receiving chemotherapy for breast cancer. Clin Breast Cancer. 2011;11:52–60. https://doi.org/10.3816/CBC.2011.n.009.
Makari-Judson G, Viskochil R, Katz D, Barham R, Mertens WC. Insulin resistance and weight gain in women treated for early stage breast cancer. Breast Cancer Res Treat. 2022;194:423–31. https://doi.org/10.1007/s10549-022-06624-1.
Freedman RJ, Aziz N, Albanes D, Hartman T, Danforth D, Hill S, et al. Weight and Body Composition Changes during and after Adjuvant Chemotherapy in Women with Breast Cancer. J Clin Endocrinol Metab. 2004;89:2248–53. https://doi.org/10.1210/jc.2003-031874.
Koo H-Y, Seo Y-G, Cho M-H, Kim M-J, Choi H-C. Weight Change and Associated Factors in Long-Term Breast Cancer Survivors. PloS One. 2016;11:e0159098. https://doi.org/10.1371/journal.pone.0159098.
Pedersen B, Delmar C, Lörincz T, Falkmer U, Grønkjær M. Investigating Changes in Weight and Body Composition Among Women in Adjuvant Treatment for Breast Cancer: A Scoping Review. Cancer Nurs. 2019;42:91–105. https://doi.org/10.1097/NCC.0000000000000590.
Karia PS, Joshu CE, Visvanathan K. Association of oophorectomy and fat and lean body mass: evidence from a population-based sample of US women. Cancer Epidemiol Biomark Prev Publ Am Assoc Cancer Res Cosponsored Am Soc Prev Oncol. 2021;30:1424–32. https://doi.org/10.1158/1055-9965.EPI-20-1849.
Brown JC, Mao JJ, Stricker C, Hwang W-T, Tan K-S, Schmitz KH. Aromatase Inhibitor Associated Musculoskeletal Symptoms are associated with Reduced Physical Activity among Breast Cancer Survivors. Breast J. 2014;20:22–8. https://doi.org/10.1111/tbj.12202.
Ding Y-Y, Yao P, Wu L, Han Z-K, Hong T, Zhu Y-Q, et al. Body mass index and persistent pain after breast cancer surgery: findings from the women’s healthy eating and living study and a meta-analysis. Oncotarget. 2017;8:43332–43. https://doi.org/10.18632/oncotarget.17948.
Voskuil DW, van Nes JGH, Junggeburt JMC, van de Velde CJH, van Leeuwen FE, de Haes JCJM. Maintenance of physical activity and body weight in relation to subsequent quality of life in postmenopausal breast cancer patients. Ann Oncol. 2010;21:2094–101. https://doi.org/10.1093/annonc/mdq151.
Demark-Wahnefried W, Campbell KL, Hayes SC. Weight management and its role in breast cancer rehabilitation. Cancer. 2012;118:2277–87. https://doi.org/10.1002/cncr.27466.
Alfano CM, Smith AW, Irwin ML, Bowen DJ, Sorensen B, Reeve BB, et al. Physical activity, long-term symptoms, and physical health-related quality of life among breast cancer survivors: a prospective analysis. J Cancer Surviv Res Pract. 2007;1:116–28. https://doi.org/10.1007/s11764-007-0014-1.
Taylor CE, Meisel JL. Weighing the influence of race and obesity on outcomes in patients with early-stage breast cancer. Cancer. 2021;127:834–6. https://doi.org/10.1002/cncr.33290.
Sheppard VB, Dash C, Oppong B, Adams-Campbell LL. Weight Changes in Black and White Women Receiving Chemotherapy Treatment for Breast Cancer. J Clin Oncol Res 2015;3
Rock CL, Flatt SW, Newman V, Caan BJ, Haan MN, Stefanick ML, et al. Factors associated with weight gain in women after diagnosis of breast cancer. Women’s Healthy Eating and Living Study Group. J Am Diet Assoc 1999;99:1212–21
Shang L, Hattori M, Fleming G, Jaskowiak N, Hedeker D, Olopade OI, et al. Impact of post-diagnosis weight change on survival outcomes in Black and White breast cancer patients. Breast Cancer Res BCR. 2021;23:18. https://doi.org/10.1186/s13058-021-01397-9.
Gho SA, Steele JR, Jones SC, Munro BJ. Self-reported side effects of breast cancer treatment: a cross-sectional study of incidence, associations, and the influence of exercise. Cancer Causes Control. 2013;24:517–28.
Bradley R, Braybrooke J, Gray R, Hills RK, Liu Z, Pan H, et al. Aromatase inhibitors versus tamoxifen in premenopausal women with oestrogen receptor-positive early-stage breast cancer treated with ovarian suppression: a patient-level meta-analysis of 7030 women from four randomised trials. Lancet Oncol. 2022;23:382–92. https://doi.org/10.1016/S1470-2045(21)00758-0.
Chen X, Lu W, Gu K, Chen Z, Zheng Y, Zheng W, et al. Weight change and its correlates among breast cancer survivors. Nutr Cancer. 2011;63:538–48. https://doi.org/10.1080/01635581.2011.539316.
Thomson ZO, Reeves MM. Can weight gain be prevented in women receiving treatment for breast cancer? A systematic review of intervention studies. Obes Rev. 2017;18:1364–73. https://doi.org/10.1111/obr.12591.
Sheng JY, Santa-Maria CA, Blackford AL, Lim D, Carpenter A, Smith KL, et al. The impact of weight loss on physical function and symptoms in overweight or obese breast cancer survivors: results from POWER-remote. J Cancer Surviv 2021:1–10. https://doi.org/10.1007/s11764-021-01049-z.
Chlebowski RT. Nutrition and physical activity influence on breast cancer incidence and outcome. Breast. 2013;22:S30–7. https://doi.org/10.1016/j.breast.2013.07.006.
Ligibel JA, Basen-Engquist K, Bea JW. Weight Management and Physical Activity for Breast Cancer Prevention and Control. Am Soc Clin Oncol Educ Book 2019:e22–33. https://doi.org/10.1200/edbk_237423.
Santa-Maria CA, Coughlin JW, Sharma D, Armanios M, Blackford AL, Schreyer C, et al. The Effects of a remote-based weight loss program on adipocytokines, metabolic markers, and telomere length in breast cancer survivors: The POWER-remote trial. Clin Cancer Res. 2020;26:3024–34. https://doi.org/10.1158/1078-0432.CCR-19-2935.
Chlebowski RT, Blackburn GL, Thomson CA, Nixon DW, Shapiro A, Hoy MK, et al. Dietary fat reduction and breast cancer outcome: Interim efficacy results from the women’s intervention nutrition study. J Natl Cancer Inst. 2006;98:1767–76. https://doi.org/10.1093/jnci/djj494.
Pierce JP, Natarajan L, Caan BJ, Parker BA, Greenberg ER, Flatt SW, et al. Influence of a diet very high in vegetables, fruit, and fiber and low in fat on prognosis following treatment for breast cancer: The Women’s Healthy Eating and Living (WHEL) randomized trial. J Am Med Assoc. 2007;298:289–98. https://doi.org/10.1001/jama.298.3.289.
Janni W, Rack B, Friedl T, Müller V, Lorenz R, Rezai M, et al. Abstract GS5–03: Lifestyle Intervention and Effect on Disease-free Survival in Early Breast Cancer Pts: Interim Analysis from the Randomized SUCCESS C Study. Cancer Res., vol. 79, American Association for Cancer Research (AACR); 2019, p. GS5–03-GS5–03. https://doi.org/10.1158/1538-7445.sabcs18-gs5-03.
Rack B, Andergassen U, Neugebauer J, Salmen J, Hepp P, Sommer H, et al. The german SUCCESS C study - The first European lifestyle study on breast cancer. Breast Care. 2010;5:395–400. https://doi.org/10.1159/000322677.
Ligibel JA, Bohlke K, May AM, Clinton SK, Demark-Wahnefried W, Gilchrist SC, et al. Exercise, Diet, and Weight Management During Cancer Treatment: ASCO Guideline. J Clin Oncol Off J Am Soc Clin Oncol. 2022;40:2491–507. https://doi.org/10.1200/JCO.22.00687.
Playdon M, Thomas G, Sanft T, Harrigan M, Ligibel J, Irwin M. Weight Loss Intervention for Breast Cancer Survivors: A Systematic Review. Curr Breast Cancer Rep. 2013;5:222–46. https://doi.org/10.1007/s12609-013-0113-0.
Smith KL, Verma N, Blackford AL, Lehman J, Westbrook K, Lim D, et al. Association of treatment-emergent symptoms identified by patient-reported outcomes with adjuvant endocrine therapy discontinuation. NPJ Breast Cancer. 2022;8:53. https://doi.org/10.1038/s41523-022-00414-0.
Miller KD, Nogueira L, Mariotto AB, Rowland JH, Yabroff KR, Alfano CM, et al. Cancer treatment and survivorship statistics, 2019. CA Cancer J Clin. 2019;69:363–85. https://doi.org/10.3322/caac.21565.
Acknowledgements
The views expressed do not necessarily reflect the official policies of the Department of Health and Human Services, nor does the mention of trade names, commercial practices, or organizations endorsed by the U.S. Government.
Funding
This work was supported by funding from Susan G. Komen Foundation, Centers for Disease Control and Prevention (5 NU58DP006673) and the Johns Hopkins Sidney Kimmel Comprehensive Cancer Center Support Grant (P30CA006973).
Author information
Authors and Affiliations
Contributions
Conceptualization: Karen Smith.
Methodology: Karen Smith, Vered Stearns, Claire Snyder.
Formal analysis and investigation: Amanda Blackford, Jennifer Lehman.
Writing—original draft preparation: Anna-Carson Uhelski.
Writing—review and editing: Anna-Carson Uhelski, Karen Smith, Jennifer Sheng, Kala Visvanathan, Claire Snyder.
Funding acquisition: Vered Stearns.
Resources: Vered Stearns, Claire Snyder, Karen Smith.
Supervision: Vered Stearns, Karen Smith.
Approval of final manuscript: All authors.
Corresponding author
Ethics declarations
Competing interests
Claire Snyder MHS PhD reports research funding to the institution from Genentech and Pfizer, and consulting fees from Janssen (via Health Outcomes Solutions).
Kala Visvanathan MD MHS reports funding from Cepheid and non-financial support from Optra Health Inc.
Vered Stearns MD reports research funding to institution from Abbvie, Biocept, Novartis, Pfizer, Puma Biotechnology and QUE Oncology. Vered Stearns also served on an advisory board for Novartis 10/25/2021. In addition, Vered Stearns is Chair of a data safety monitoring board for AstraZeneca and received non-financial support from Foundation Medicine for study assays.
Karen Lisa Smith MD MPH has received research support (to institution) from Pfizer. Karen Lisa Smith’s spouse has stock ownership in ABT Labs and Abbvie.
The following authors declare that they have no conflicts of interest:
Anna-Carson Rimer Uhelski MD.
Amanda L. Blackford ScM.
Jennifer Y. Sheng MD
Jennifer Lehman BS
David Lim MS
Ethics approval
This study was approved by the Johns Hopkins Institutional Review Board.
Consent to participate
All participants provided informed consent.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Uhelski, AC.R., Blackford, A.L., Sheng, J.Y. et al. Factors associated with weight gain in pre- and post-menopausal women receiving adjuvant endocrine therapy for breast cancer. J Cancer Surviv 18, 1683–1696 (2024). https://doi.org/10.1007/s11764-023-01408-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11764-023-01408-y