
Abstract
Purpose
The effectiveness of endoscopic management of twisting of the gastric pouch after sleeve gastrectomy.
Methods
This was a retrospective study on Ain Shams University Hospital. Patients who had obstructive symptoms and diagnosed with twist after gastric sleeve were included in this study.
Results
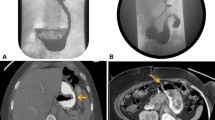
From May 2017 to January 2019, 860 patients underwent LSG as a definitive procedure. Thirty-two (3.7%) patients developed symptoms of gastric obstruction. Twenty-two (2.5%) patients diagnosed with sleeve axial twist were included in this study after excluding 11 patients with sleeve stricture. A total of 72% (16 out of 22) of patients were female, with a mean age of 41. The mean time of presentation was 40 days (20–60 days) after surgery. Gastrografin contrast study was positive in 14 (63%) patients. 3D contrast CT was positive in 100% of cases. The timing of endoscopic intervention was 40 ± 20 days (20–60) after surgery. Endoscopic treatment was successful in 20 patients (91%). Recovery was uneventful in 19 patients; 1 patient had esophageal stricture at the upper end of the stent, which necessitated a session of dilation. The success of endoscopic intervention was 91% with complete relief of symptoms and correction of the gastric pouch axis. Endoscopic intervention failed in only 2 patients (9%) who necessitated laparoscopic exploration after stent removal.
Conclusion
Gastric pouch twisting is a rare complication; however, it has a rising incidence. Endoscopic stent insertion is highly effective on the management of twisting after SG and it should be tried before any further surgical intervention.




Similar content being viewed by others


References
Himpens J, Dobbeleir J, Peeters G. Long-term results of laparoscopic sleeve gastrectomy for obesity. Ann Surg. 2010;252:319–24.
Burgos AM, Csendes A, Braghetto I. Gastric stenosis after laparoscopic sleeve gastrectomy in morbidly obese patients. Obes Surg. 2013;23(9):14811486.
Gluck B, Movitz B, Jansma S, et al. Laparoscopic sleeve gastrectomy is a safe and effective bariatric procedure for the lower BMI (35.0–43.0 kg/m2) population. Obes Surg. 2011;21(8):1168–71.
Elias S et al. Gastric twist after laparoscopic sleeve gastrectomy, diagnosis and management: a case series and discussion. Diabetes Obes Int J. 2017;2(3):000159.
Rebibo L, Hakim S, Dhahri A, et al. Gastric stenosis after laparoscopic sleeve gastrectomy: diagnosis and management. Obes Surg. 2016;26(5):995–1001.
Parikh A, Alley JB, Peterson RM, et al. Management options for symptomatic stenosis after laparoscopic vertical sleeve gastrectomy in the morbidly obese. Surg Endosc. 2012;26(3):738–46.
Subhas G, Gupta A, Sabir M, et al. Gastric remnant twist in the immediate post-operative period following laparoscopic sleeve gastrectomy. World J Gastrointest Surg. 2015;7(11):345–8.
Romero RJ, Kosanovic R, Rabaza JR, et al. Robotic sleeve gastrectomy: experience of 134 cases and comparison with a systematic review of the laparoscopic approach. Obes Surg. 2013;23(11):1743–52.
Abd Ellatif ME, Abbas A, El Nakeeb A, et al. Management options for twisted gastric tube after laparoscopic sleeve gastrectomy. Obes Surg. 2017;27:2404–9.
Murcia CH, Quintero PG, Rabaza J, Gonzalez A (2014) Laparoscopic management of gastric torsion after sleeve gastrectomy. CRSLS.00143.
de Godoy EP, Coelho D. Gastric sleeve fixation strategy in laparoscopic vertical sleeve gastrectomy. Arq Bras Cir Dig. 2013;26(Suppl 1):79–82.
Eubanks S, Edwards CA, Fearing NM, et al. Use of endoscopic stents to treat anastomotic complications after bariatric surgery. J Am Coll Surg. 2008;206(5):93.
Marquez M, Ayza FM, Belda LR, et al. Gastric leak after laparoscopic sleeve gastrectomy. Obes Surg. 2010;20:1306–11.
Shnell M, Fishman S, Eldar S, et al. Balloon dilatation for symptomatic gastric sleeve stricture. Gastrointest Endosc. 2014;79:521–4.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Conflict of Interest
The authors declare that they have no conflict of interest.
Informed Consent
Informed consent was obtained from all individuals who participated in the study.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Hassan, M.I., Khalifa, M.S., Elsayed, M.A. et al. Role of Endoscopic Stent Insertion on Management of Gastric Twist after Sleeve Gastrectomy. OBES SURG 30, 2877–2882 (2020). https://doi.org/10.1007/s11695-020-04641-x
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-020-04641-x