
Abstract
Introduction
Single-anastomosis duodeno-ileal bypass with sleeve gastrectomy (SADI-S) surgery is a modification of the traditional duodenal switch (DS) surgery. SADI-S is relatively a new bariatric surgical procedure and has gone by many names depending on the length of the common channel. In this study, we report our initial experience with this novel technique in the Australian population.
Methods
The medical records of 91 patients who underwent laparoscopic primary SADI-S surgery by one surgeon at a single Australian center from January 2017 through May 2019 were retrospectively studied.
Results
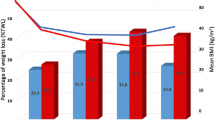
Ninety-one patients were identified for analysis. The mean age and preoperative body mass index (BMI) was 46.2 ± 9 years and 43.2 ± 5.7 kg/m2, respectively. The mean operative time and length of stay were 121.8+/- 25 minutes and 1.4 ± 0.8 days, respectively. At 12 and 24 months, the patients lost an average BMI of 15.2 ± 5.2 kg/m2 and 17.2 ± 5.9 kg/m2, respectively. The short-term and long-term complication rates were 4.3% and 0%, respectively. The mortality rate was 0%. Postoperatively, the obstructive sleep apnea, type 2 diabetes, hyperlipidemia, hypertension, and gastroesophageal reflux disease resolution rates were 94, 94, 75, 68, and 13%, respectively. There was no statistically significant difference between most of the preoperative and postoperative nutritional data.
Conclusions
SADI-S appears to be a safe bariatric surgical procedure with favorable outcomes at 2 years in the Australian population.


Similar content being viewed by others


References
Surve A, Cottam D, Sanchez-Pernaute A, et al. The incidence of complications associated with loop duodeno-ileostomy after single-anastomosis duodenal switch procedures among 1328 patients: a multicenter experience. Surg Obes Relat Dis. 2018;
Surve A, Zaveri H, Cottam D, et al. A retrospective comparison of biliopancreatic diversion with duodenal switch with single anastomosis duodenal switch (SIPS-stomach intestinal pylorus sparing surgery) at a single institution with two year follow-up. Surg Obes Relat Dis. 2017;13(3):415–22.
Cottam A, Cottam D, Portenier D, et al. A matched cohort analysis of stomach intestinal pylorus saving (SIPS) surgery versus biliopancreatic diversion with duodenal switch with two-year follow-up. Obes Surg. 2017;27(2):454–61.
Mitzman B, Cottam D, Goriparthi R, et al. Stomach intestinal pylorus sparing (SIPS) surgery for morbid obesity: retrospective analyses of our preliminary experience. Obes Surg. 2016;26(9):2098–104.
Sánchez-Pernaute A, Rubio MA, Pérez-Aguirre E, et al. Single-anastomosis duodenoileal bypass with sleeve gastrectomy: metabolic improvement and weight loss in first 100 patients. Surg Obes Relat Dis. 2013;9:731–5.
Cottam A, Cottam D, Roslin M, et al. A matched cohort analysis of sleeve gastrectomy with and without 300 cm loop duodenal switch with 18-month follow-up. Obes Surg. 2016;26(10):2363–9.
Cottam A, Cottam D, Medlin W, et al. A matched cohort analysis of single anastomosis loop duodenal switch versus Roux-en-Y gastric bypass with 18 month follow up. Surg Endosc. 2016;30(9):3958–64.
Surve A, Zaveri H, Cottam D, et al. Mid-term outcomes of gastric bypass weight loss failure to duodenal switch. Surg Obes Relat Dis. 2016;12(9):1663–70.
Neichoy BT, Schniederjan B, Cottam DR, et al. Stomach intestinal pylorus-sparing surgery for morbid obesity. JSLS. 2018;22(1)
Surve A, Zaveri H, Cottam D. A step-by-step surgical technique video with two reported cases of common channel lengthening in patients with previous stomach intestinal pylorus sparing surgery to treat chronic diarrhea. Surg Obes Relat Dis. 2017;13(4):706–9.
Sánchez-Pernaute A, Rubio MÁ, Cabrerizo L, et al. Single-anastomosis duodenoileal bypass with sleeve gastrectomy (SADI-S) for obese diabetic patients. Surg Obes Relat Dis. 2015;11(5):1092–8.
Surve A, Zaveri H, Cottam D. Retrograde filling of the afferent limb as a cause of chronic nausea after single anastomosis loop duodenal switch. Surg Obes Relat Dis. 2016;12(4):e39–42.
Moon RC, Kirkpatrick V, Gaskins L, et al. Safety and effectiveness of single- versus double-anastomosis duodenal switch at a single institution. Surg Obes Relat Dis. 2019;15(2):245–52.
Surve A, Zaveri H, Cottam D, et al. Laparoscopic stomach intestinal pylorus-sparing surgery as a revisional option after failed adjustable gastric banding: a report of 27 cases with 36-month follow-up. Surg Obes Relat Dis. 2018;
Topart P, Becouarn G. The single anastomosis duodenal switch modifications: a review of the current literature on outcomes. Surg Obes Relat Dis. 2017;13(8):1306–12.
Martini F, Paolino L, Marzano E, et al. Single-anastomosis pylorus-preserving bariatric procedures: review of the literature. Obes Surg. 2016;26(10):2503–15.
Brethauer SA, Kim J, El Chaar M, et al. ASMBS clinical issues committee. Standardized outcomes reporting in metabolic and bariatric surgery. Obes Surg. 2015;25:587–606.
American Diabetes Association. 2. Classification and diagnosis of diabetes: standards of medical care in diabetes-2019. Diabetes Care. 2019;42:S13.
Doyle DJ, Garmon EH. American Society of Anesthesiologists Classification (ASA class). Treasure Island: StatPearls Publishing LLC; 2017.
Aills L, Blankenship J, Buffington C, et al. ASMBS allied health nutritional guidelines for the surgical weight loss patient. Surg Obes Relat Dis. 2008;4:S73–S108.
R Core Team. R: a language and environment for statistical computing. Vienna: R Foundation for statistical computing; 2013. URL http://www.R-project.org/
Surve A, Zaveri H, Cottam D. A safer and simpler technique of duodenal dissection and transection of the duodenal bulb for duodenal switch. Surg Obes Relat Dis. 2016;12(4):923–4.
Nelson L, Moon RC, Teixeira AF, et al. Safety and effectiveness of single anastomosis duodenal switch procedure: preliminary results from a single institution. Arq Bras Cir Dig. 2016;29(Suppl 1):80–4.
Shoar S, Poliakin L, Rubenstein R, et al. A single anastomosis duodeno-ileal switch (SADIS): a systematic review of efficacy and safety. Obes Surg. 2018;28(1):104–13.
Modi A, Agrawal A, Morgan F. Euglycemic diabetic ketoacidosis. Curr Diabetes Rev. 2017;13:315–21.
Ogawa W, Sakaguchi K. Euglycemic diabetic ketoacidosis induced by SGLT2 inhibitors: possible mechanism and contributing factors. J Diabetes Investig. 2016;7:135–8.
Lupoli R, Lembo E, Saldalamacchia G, et al. Bariatric surgery and long-term nutritional issues. World J Diabetes. 2017;8(11):464–74.
Enochs P. The laparoscopic stomach, intestinal and pylorus sparing (SIPS) procedure: a single center analysis of our first 100 patients. Surg Obes Relat Dis. 2015;11(6):S165–6.
Nelson L, Moon RC, Teixeira AF, et al. Safety and effectiveness of single anastomosis duodenal switch procedure: preliminary result from a single institution. Arq Bras Cir Dig. 2016;29Suppl 1(Suppl 1):80–4.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Statement of Human and Animal Rights
I certify that the manuscript did not involve the use of animal or human subjects.
Since this is a retrospective study, formal consent is not required for this type of study.
Conflict of Interest
Author 3, the corresponding author, reports personal fees and other from Medtronic and GI Windows, outside the submitted work.
All other authors have no conflicts of interests to declare.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic Supplementary Material
ESM 1
(DOCX 16 kb)
Rights and permissions
About this article

Cite this article
Surve, A., Rao, R., Cottam, D. et al. Early Outcomes of Primary SADI-S: an Australian Experience. OBES SURG 30, 1429–1436 (2020). https://doi.org/10.1007/s11695-019-04312-6
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-019-04312-6