
Abstract
Background
Weight loss interventions for obesity, such as bariatric surgery, are associated with reductions in bone mineral density and may increase the risk of fractures. We undertook a systematic review and meta-analysis of bariatric surgery and lifestyle weight management programs (WMPs) with fracture outcomes.
Methods
We searched MEDLINE, Embase, the Cochrane Central Register of Controlled Trials from 1966 to 2018, and our trial registry of WMP randomized controlled trials (RCTs). We included RCTs, non-randomized trials, and observational studies of bariatric surgery, and RCTs of WMPs. Studies had follow-up ≥ 12 months, mean group body mass index ≥ 30 kg/m2. The primary outcome measure was incidence of any type of fracture in participants, and the secondary outcome was weight change. We used random effects meta-analysis for trial data.
Results
Fifteen studies were included. Three small trials provided short-term evidence of the association between bariatric surgery and participants with any fracture (365 participants; RR 0.82; 95% CI 0.29 to 2.35). Four out of six observational studies of bariatric surgery demonstrated significantly increased fracture risk. Six RCTs of WMPs with 6214 participants, the longest follow-up 11.3 years, showed no clear effect on any type of fracture (RR 1.04; 95% CI 0.91 to 1.18), although authors of the largest RCT reported an increased risk of frailty fracture by their definition (RR 1.40; 95% CI 1.04 to 1.90).
Conclusion
Bariatric surgery appears to increase the risk of any fracture; however, longer-term trial data are needed. The effect of lifestyle WMPs on the risk of any fracture is currently unclear.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
While bariatric surgery for adults with obesity is effective for weight loss and reduces many obesity-related diseases, reports on long-term complications beyond mortality are currently limited [1]. Risk of malnutrition and malabsorption of fat-soluble vitamins including vitamin D, as well as increased bone turnover and reduced bone mineral density (BMD) after surgery [2, 3], could increase the risk of fracture. Lifestyle weight management programs (WMPs), consisting of a variety of diets with or without exercise advice, are reported to be associated with a small reduction in total hip but not lumbar spine BMD measurements in observational data [4].
We undertook a systematic review of fracture outcome data from studies of bariatric surgery and lifestyle WMPs. Our aim was to examine whether weight loss increased the risk of participants sustaining any fracture, compared to adults with obesity who did not undergo bariatric surgery or undertake WMPs.
Materials and Methods
We used a pre-specified protocol and followed PRISMA (Preferred Reporting Items for Systematic reviews and Meta-analyses) guidelines.
Selection Criteria
Bariatric Surgery Studies
There are presently few randomized controlled trials (RCTs) reporting fracture data post-bariatric surgery compared to no surgery; therefore, we included non-randomized controlled trials and observational studies in adults (≥ 18 years), with mean pre-surgery group body mass index (BMI) ≥ 30 kg/m2. Studies had a minimum follow-up ≥ 1 year.
Lifestyle Weight Management Programs
We included RCTs of WMPs of reducing diets with or without physical activity advice and/or programs to attend, versus usual care/no intervention. Studies had minimum follow-up ≥ 1 year, mean baseline group BMI ≥ 30 kg/m2, and mean group age ≥ 18 years.
Outcomes
Our primary outcome was participants with any fracture and our secondary outcome was weight change.
Search Strategy
We searched full texts of trial reports in our database of long-term RCTs of lifestyle WMPs for adults, compiled from MEDLINE, Embase, and the Cochrane Central Register of Controlled Trials, from 1966 to 2016 [5, 6]. We performed an updated search from 2016 to July 2018 for WMP RCTs. Details of the search strategy (including for bariatric surgery) in MEDLINE can be found in Appendix A, which was adapted for other databases. We contacted the authors of eight WMP and bariatric surgery RCTs with bone mineral density data to request any additional unpublished fracture data.
Data Analysis
AA and ADA/BRB independently confirmed study eligibility. ADA extracted data, which were checked by AA. AA and ADA independently assessed quality of RCTs and non-randomized trials using the Cochrane risk of bias tool [7] and for observational studies using the Newcastle-Ottawa Quality Assessment Scale [8]. All differences were resolved by discussion.
Owing to limited data, we combined data from RCTs and non-randomized controlled trials of bariatric surgery in meta-analyses, using Review Manager Software version 5.3. Risk ratios (RR) and 95% confidence intervals (95% CI) were calculated for dichotomous outcomes. Heterogeneity was assessed using the I2 test (I2 > 50% was considered significant heterogeneity) in conjunction with the chi-squared test. Random effects meta-analysis was used to pool outcome data, due to known heterogeneity in weight loss interventions. We estimated mean differences (MD) and 95% CI for weight data, giving preference to follow-up data for all participants or data taking account of drop-outs (preferentially baseline observation carried forward) if these were provided. Missing standard deviations (SD) were derived using previously described methods [5].
Data from observational studies of bariatric surgery were not combined, but are discussed in a narrative review.
No external funding was provided. No ethical approval was required.
Results
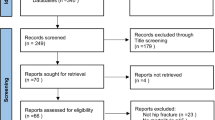
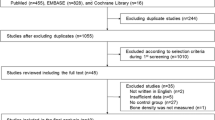
We screened 1174 full-text trial reports and 4153 titles and abstracts, as outlined in Fig. 1.

Study selection
Quality Assessment
Bariatric Surgery Trials
Appendix Table 3 provides our full risk of bias assessments for the three trials, two of which were RCTs. None were judged to be at low risk of bias for outcome assessment. We judged that there was a high risk of bias for incomplete outcome data due to high drop-out rates [9, 10], and the non-randomized controlled trial was potentially at a high risk of other bias due to the study being funded by industry [11].
All six observational studies of surgery (Appendix Table 4) were judged to be moderately representative of the average obese person in their communities. We judged the comparability of all of the studies in terms of controlling for factors associated with fractures to be acceptable; however, two of the studies failed to report numerical BMI data [12, 13].
Lifestyle Intervention Studies
Three of the RCTs (see Appendix Table 3) were judged to be at low risk of bias for outcome assessment [14,15,16]. Three trials were also at low risk for both incomplete outcome data and selective reporting [15,16,17]. Two trials were judged to be potentially at high risk of bias due to premature termination [15] and industry sponsorship [18].
Study Characteristics
Bariatric Surgery Trials
Two RCTs (Table 1) were from the USA [9, 10] and one non-randomized controlled trial was from Norway [11], involving a total of 365 adults, mostly women (see Table 1). Roux-en-Y gastric bypass (RYGB) was used in all three trials, laparoscopic adjustable gastric banding (LAGB) in one [9] and laparoscopic sleeve gastrectomy (LSG) in one [10]. Both of the RCTs included participants with type 2 diabetes and associated comorbidities, and 27% of participants in the non-randomized trial had type 2 diabetes. At baseline, prior to bariatric surgical intervention, mean group ages ranged from 42.8–50.0 years and mean group BMI ranged from 35.3–46.7 kg/m2. The maximum follow-up was only 2 years.
Bariatric Surgery Observational Studies
Table 2 provides details of the observational studies of bariatric surgery. There were 1872 fractures in 59,930 patients who underwent bariatric surgery versus 5408 fractures in 223,110 control patients, from the UK, Taiwan, and North America in one case-control study [13] and five cohort studies [7, 12, 20,21,22,23]. Each of the studies included patients undergoing a variety of restrictive and malabsorptive procedures, with the exception of one study of gastric bypass surgery only [20]. Trial participants had a wide range of comorbidities and were predominantly female. Where reported, group mean BMI was ≥ 40 kg/m2 and group mean age < 50 years before surgery.
Lifestyle WMP RCTs
Table 1 provides details of the six WMP RCTs involving 6214 adult participants [14,15,16,17,18,19]. The Look AHEAD trial [15] was the largest study by far, with 5145 participants with type 2 diabetes followed for 11.3 years.
Five RCTs provided both diet and exercise advice (≥ 150 min of moderate physical activity per week) [14,15,16,17, 19] and one diet advice only [18]. Three trials [15,16,17] provided exercise programs for participants to attend. Two RCTs prescribed a calorie restriction of 1200–1800 kcal/day, which lasted between 27 and 115 months [15, 18]; two RCTs a calorie deficit of 500–1000 kcal/day [17, 19]; and two RCTs were unclear as to the calorie content prescribed [14, 16].
All six trials recruited participants with pre-existing comorbidities, with one trial enrolling participants with uncontrolled asthma where 32.1% of patients reported systemic corticosteroid use [19]. Five RCTs were conducted in the USA [14,15,16,17, 19] and one in Germany [18]. Two trials at baseline had group mean BMI ≤ 35 kg/m2 [14, 18]. The studies recruited predominantly middle-aged adults, with the exception of Villareal and colleagues who recruited older adults (mean group age 69–70 years) [17]. Follow-up was usually ≤ 2 years, with the exception of the Look AHEAD trial with follow-up of 11.3 years [15]. The mean drop-out rate ranged from 3.4 to 38.0%, with the highest drop-out rate reported in the trial from Ditschuneit and colleagues [18].
Data Analyses
Appendix Table 5 provides details of the fractures reported and definitions of osteoporotic or frailty fractures, as defined by the investigators.
Bariatric Surgery RCTs
For our primary outcome, the results of our meta-analysis of trials revealed no significant association between bariatric surgery and participants developing any fracture (n = 3 trials; 13 events; RR 0.82; 95% CI 0.29 to 2.35; I2 = 0%) (Fig. 2). For our secondary outcome, bariatric surgery led to marked weight loss, with high heterogeneity between studies (n = 3 trials; MD − 22.2 kg; 95% CI − 31.6 to − 12.8; I2 = 93%) (Fig. 3).

Meta-analysis of weight loss intervention and incidence of fractures

Meta-analysis of weight loss intervention and sustained weight loss
Bariatric Surgery Observational Studies
Four out of the six observational studies reported a statistically significant association between bariatric surgery and an increased likelihood of fracture (Table 2). The studies which reported an association between bariatric surgery and fracture incidence had longer periods of observation than the 3 years follow-up of the studies which reported no association. All studies adjusted for risk factors associated with fractures, such as fracture history, comorbidities, and age. However, Lalmohamed and colleagues, who observed no association between bariatric surgery and fracture, adjusted for a broader range of confounders, such as inflammatory bowel disease, glucocorticoids, proton pump inhibitors, and calcium and vitamin D supplementation [22].
Axelsson and colleagues [20] reported an increased risk of osteoporotic and hip fractures post-bariatric surgery. Lu and colleagues [12] had fewer events and did not find a statistically significant increase in osteoporotic or hip fractures. The increased risk post-surgery in the study by Rousseau and colleagues appeared to mainly relate to biliopancreatic diversion [13], which is rarely used today. Nakamura and colleagues reported an increased risk of fractures at traditional osteoporotic sites compared to community controls, matched for age and sex but not BMI [23].
Lifestyle WMP RCTs
In the lifestyle WMP RCTs, our meta-analysis showed no significant association between WMPs and participants developing any fracture (n = 6 trials; 746 events; RR 1.04; 95% CI 0.91 to 1.19; I2 = 0%) (Fig. 2). However, the largest trial, with follow-up of 5145 participants with diabetes, reported an increased risk of frailty fractures, a composite of hip, pelvis, upper arm, and shoulder fractures (hazard ratio 1.39; 95% CI 1.02 to 1.89). Weight loss at final follow-up showed high heterogeneity (n = 6 trials; MD − 4.15; 95% CI − 6.41 to −1.89; I2 = 92%).
Discussion
We found that bariatric surgery, predominantly malabsorptive in nature [12, 20], was associated with an increased risk of fracture compared to people of similar starting weight who did not undergo surgery. However, it is unclear whether the risk of fracture for adults post-bariatric surgery at their lower weight exceeds people of similar weight in the general population. Lifestyle WMPs were not associated with an increased risk of any fracture. However, there was some evidence from the Look AHEAD trial [15] to suggest that the risk of frailty fractures might be increased, but this trial did not report vertebral fractures and only around half of frailty fractures appeared to be related to low trauma. In the Look AHEAD trial, frailty fractures related to a composite of the first occurrence of a hip, upper arm, or shoulder fracture [15].
Weight loss programs, with or without bariatric surgery, are generally associated with advice to increase physical activity with or without exercise programs to attend. Thus, the effects of weight reduction on fracture risk cannot be separated in our studies from the possibility that a sudden increase in physical activity alone may have resulted in an increased propensity for injury.
There have been a number of systematic reviews and meta-analyses reporting on the association between bariatric surgery, particularly malabsorptive surgery, and significant BMD loss at the hip with less consistent results for the lumbar spine [2, 24,25,26]. However, the studies were sometimes without comparator groups and are difficult to interpret due to imaging limitations in severe obesity [27]. In a meta-analysis of five cohort studies and one RCT, Zhang and colleagues reported that bariatric surgery was associated with fractures at non-vertebral sites, especially upper limb fractures [28]. In contrast, in our meta-analysis of trials alone, the fractures reported were predominantly lower limb fractures such as tarsal and metatarsal fractures, but also included phalangeal fractures, suggesting short-term fractures secondary to physical activity [9,10,11]. Lu and colleagues in particular reported an increased risk of foot fractures, along with other sites not normally associated with osteoporosis [12].
The potential mechanisms underlying reductions in bone density and strength from weight loss which may precipitate bone fracture include mechanical, hormonal changes, and malabsorptive factors [27]. The reduction in force placed upon bones due to weight loss leads to higher levels of sclerostin, which inhibits osteoblastic activity and bone formation [27], while markers of bone turnover are considerably increased [4, 27]. Furthermore, estrogen and androgen status may decline particularly in postmenopausal women after bariatric surgery [29]. Bariatric procedures such as Roux-en-Y may lead to malabsorption of micronutrients required to maintain BMD [30]. Malabsorption of micronutrients including vitamin D, protein, and calcium, particularly after certain bypass procedures, may therefore require supplementation, e.g., vitamin D supplementation, to prevent secondary hyperparathyroidism [31]. Despite recommendations for patients post-bariatric surgery to take additional nutrient supplementation [31, 32], adherence is poor, e.g., vitamin D supplementation has been reported to be as low as 33% at 1 year [33], with factors such as male sex and working full-time associated with poor concordance [34]. BMD loss due to these factors, when additionally compounded by a sudden rise in physical activity in a previously sedentary adult, may place the bone under increased stress while also increasing the opportunities for the bone to fracture.
We attempted to identify all studies of WMPs and surgical RCTs which reported fractures, including contacting authors who had published BMD data to seek additional fracture data. However, the fracture data in the trials were often only reported as adverse events, and it is likely that fracture outcome data in other trials are unreported in the literature. Trials were often underpowered with short follow-up periods, such that it would be unlikely for changes in BMD to manifest as fractures.
In order for trials to meaningfully assess the long-term risk of fractures in bariatric patients, results from observational studies suggest that it is imperative that follow-up periods are sufficiently long [12, 13, 23], for example, Nakamura and colleagues reported that the median time to first fracture was 13 years [23]. It is important to acknowledge the difficulty maintaining prolonged follow-up in this patient group, but routine data collection through health records would allow evaluation. In a nationwide cohort study of 16,620 patients, Thereaux and colleagues observed that follow-up rates at 1 year and 5 years decreased from 87.1 to 29.6% [33]. Factors such as male sex and younger age were predictors of poor 5-year follow-up [33].
There is growing evidence to suggest that very large weight losses produced by bariatric surgery are associated with an increased risk of fracture. High rates of loss to follow-up in this patient group may hinder accurate evaluation; nevertheless, there remains a concerning lack of reporting on this adverse outcome. We suggest that bariatric surgery studies habitually report the presence (or absence) of fractures during long-term follow-up, including information on patient characteristics and types of fractures.
References
Morgan DJR, Ho KM, Armstrong J, et al. Long-term clinical outcomes and health care utilization after bariatric surgery: a population-based study. Ann Surg. 2015;262:86–92.
Liu C, Wu D, Zhang JF, et al. Changes in bone metabolism in morbidly obese patients after bariatric surgery: a meta-analysis. Obes Surg. 2016;26:91–7.
Schafer AL, Kazakia GJ, Vittinghoff E, et al. Effects of gastric bypass surgery on bone mass and microarchitecture occur early and particularly impact postmenopausal women. J Bone Miner Res. 2018;33:975–86.
Zibellini J, Seimon R, Lee C, et al. Does diet-induced weight loss lead to bone loss in overweight or obese adults? A systematic review and meta-analysis of clinical trials. J Bone Miner Res. 2015;30:2168–78.
Avenell A, Broom J, Brown T, et al. Systematic review of the long-term effects and economic consequences of treatments for obesity and implications for health improvement. Health Technol Assess. 2004;8:1–182.
Robertson C, Archibald D, Avenell A, et al. Systematic reviews of and integrated report on the quantitative, qualitative and economic evidence base for the management of obesity in men. Health Technol Assess. 2014;18:1–424.
Higgins JPT, Altman DG, Gøtzsche PC, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:1–9.
Wells G, Shea B, O’Connell D, et al. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses [Internet]. [cited 2018 May 1]. Available from: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp.
Courcoulas AP, Goodpaster BH, Eagleton JK, et al. Surgical vs medical treatments for type 2 diabetes mellitus: a randomized clinical trial. JAMA Surg. 2014;149:707–15.
Maghrabi AH, Wolski K, Abood B, et al. Two-year outcomes on bone density and fracture incidence in patients with T2DM randomized to bariatric surgery versus intensive medical therapy. Obesity. 2015;23:2344–8.
Hofsø D, Nordstrand N, Johnson LK, et al. Obesity-related cardiovascular risk factors after weight loss: a clinical trial comparing gastric bypass surgery and intensive lifestyle intervention. Eur J Endocrinol. 2010;163:735–45.
Lu CW, Chang YK, Chang HH, et al. Fracture risk after bariatric surgery: a 12-year nationwide cohort study. Medicine (Baltimore). 2015;94:1–7.
Rousseau C, Jean S, Gamache P, et al. Change in fracture risk and fracture pattern after bariatric surgery: nested case-control study. BMJ. 2016;354:1–12.
Ma J, Yank V, Xiao L, et al. Translating the diabetes prevention program lifestyle intervention for weight loss into primary care: a randomized trial. JAMA Intern Med. 2013;173:113–21.
Johnson KC, Bray GA, Cheskin LJ, et al. The effect of intentional weight loss on fracture risk in persons with diabetes: results from the Look AHEAD randomized clinical trial. J Bone Miner Res. 2017;32:2278–87.
Daumit GL, Dickerson FB, Wang N-Y, et al. A behavioral weight-loss intervention in persons with serious mental illness. N Engl J Med. 2013;368:1594–602.
Villareal DT, Chode S, Parimi N, et al. Weight loss, exercise, or both and physical function in obese older adults. N Engl J Med. 2011;364:1218–29.
Ditschuneit HH, Flechtner-Mors M, Johnson TD, et al. Metabolic and weight-loss effects of a long-term dietary intervention in obese patients. Am J Clin Nutr. 1999;69:198–204.
Ma J, Strub P, Xiao L, et al. Behavioral weight loss and physical activity intervention in obese adults with asthma: a randomized trial. Ann Am Thorac Soc. 2015;12:1–11.
Axelsson KF, Werling M, Eliasson B, et al. Fracture risk after gastric bypass surgery: a retrospective cohort study. J Bone Miner Res. 2018;33:2122–31.
Douglas IJ, Bhaskaran K, Batterham RL, et al. Bariatric surgery in the United Kingdom: a cohort study of weight loss and clinical outcomes in routine clinical care. PLoS Med. 2015;12:1–18.
Lalmohamed A, De Vries F, Bazelier MT, et al. Risk of fracture after bariatric surgery in the United Kingdom: population based, retrospective cohort study. BMJ. 2012;345:1–11.
Nakamura KM, Haglind EGC, Clowes JA, et al. Fracture risk following bariatric surgery: a population-based study. Osteoporos Int. 2014;25:151–8.
Rodríguez-Carmona Y, López-Alavez FJ, González-Garay AG, et al. Bone mineral density after bariatric surgery: a systematic review. Int J Surg. 2014;12:976–82.
Ko BJ, Myung SK, Cho KH, et al. Relationship between bariatric surgery and bone mineral density: a meta-analysis. Obes Surg. 2016;26:1414–21.
Marcil G, Bourget-Murray J, Shinde S, et al. The incidence of fractures following bariatric surgery: a systematic review. Int J Surg Open. 2018;14:9–14.
Gagnon C, Schafer AL. Bone health after bariatric surgery. J Bone Miner Res PLUS. 2018;2:121–33.
Zhang Q, Chen Y, Li J, et al. A meta-analysis of the effects of bariatric surgery on fracture risk. Obes Rev. 2018;19:728–36.
Yu E. Bariatric surgery: weighing in on bone loss. J Bone Miner Res. 2018;33:973–4.
Bal B, Koch TR, Finelli FC, et al. Managing medical and surgical disorders after divided Roux-en-Y gastric bypass surgery. Nat Rev Gastroenterol Hepatol. 2010;7:320–34.
Bal BS, Finelli FC, Shope TR, et al. Nutritional deficiencies after bariatric surgery. Nat Rev Endocrinol. 2012;8:544–56.
Schweitzer DH, Posthuma EF. Prevention of vitamin and mineral deficiencies after bariatric surgery: evidence and algorithms. Obes Surg. 2008;18:1485–8.
Thereaux J, Lesuffleur T, Païta M, et al. Long-term follow-up after bariatric surgery in a national cohort. Br J Surg. 2017;104:1362–71.
Sunil S, Santiago VA, Gougeon L, et al. Predictors of vitamin adherence after bariatric surgery. Obes Surg. 2017;27:416–23.
Acknowledgements
We thank Cynthia Fraser, Health Services Research Unit, University of Aberdeen, Scotland, for her help with literature searching. We thank Mark Bolland and Andrew Grey, University of Auckland, New Zealand, for their advice.
Funding
The Health Services Research Unit is funded by the Chief Scientist Office of the Scottish Government Health and Social Care Directorates.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix A. Search Strategy in MEDLINE
Appendix A. Search Strategy in MEDLINE
-
1.
exp Obesity/
-
2.
weight loss/ or overweight/
-
3.
obes$.tw.
-
4.
(weight adj1 (los$ or reduc$ or maint$ or control)).tw.
-
5.
1 or 2 or 3 or 4
-
6.
diet therapy/ or caloric restriction/ or diet, carbohydrate-restricted/ or diet, fat-restricted/ or diet, reducing/
-
7.
diet$.tw.
-
8.
((calori$ or fat or carbohydrate) adj3 (reduc$ or restrict$ or limit$)).tw.
-
9.
surger$.ti
-
10.
6 or 7 or 8 or 9
-
11.
Bone Density/
-
12.
exp Fractures, Bone/
-
13.
Osteoporosis/
-
14.
(bone adj3 (density or loss or reduc$)).tw.
-
15.
Osteopor$.tw.
-
16.
Postoperative Complications/
-
17.
11 or 12 or 13 or 14 or 15 or 16
-
18.
5 and 10 and 17
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Ablett, A.D., Boyle, B.R. & Avenell, A. Fractures in Adults After Weight Loss from Bariatric Surgery and Weight Management Programs for Obesity: Systematic Review and Meta-analysis. OBES SURG 29, 1327–1342 (2019). https://doi.org/10.1007/s11695-018-03685-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-018-03685-4