
Abstract
Background
The preferred surgical procedure for treating morbid obesity is debated. Patient-reported outcome measures (PROMs) are relevant for evaluation of the optimal bariatric procedure.
Methods
A total of 113 patients with BMI from 50 to 60 were randomly assigned to standard (n = 57) or distal (n = 56) Roux-en-Y gastric bypass (RYGB). Validated PROMS questionnaires were completed at baseline and 2 years after surgery. Data were analyzed using mixed models for repeated measures and the results are expressed as estimated means and mean changes.
Results
Obesity-related quality of life improved significantly after both procedures, without significant between-group differences (− 0.4 (95% CI = − 8.4, 7.2) points, p = 0.88, ES = 0.06). Both groups had significant reductions in the number of weight-related symptoms and symptom distress score, with a mean group difference (95% CI) of 1.4 (− 0.3, 3.3) symptoms and 5.0 (2.9. 12.8) symptom distress score points. There were no between-group differences for uncontrolled eating (22.0 (17.2–26.7) vs. 28.9 (23.3–34.5) points), cognitive restraint (57.4 (52.0–62.7) vs. 62.1 (57.9–66.2) points), and emotional eating (26.8 (20.5–33.1) vs. 32.6 (25.5–39.7) points).
The prevalence of anxiety was 33% after standard and 25% after distal RYGB (p = 0.53), and for depression 12 and 9%, respectively (p = 0.76).
Conclusions
There were no statistically significant differences between standard and distal RYGB 2 years post surgery regarding weight loss, obesity-related quality of life, weight-related symptoms, anxiety, depression, or eating behavior.
Trial Registration
Clinical Trials.gov number NCT00821197
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Bariatric surgery may induce sustained weight loss, improvement of weight-associated comorbidities, and improved health and well-being [1, 2]. However, the preferred surgical procedure is debated, particularly for patients with a BMI of 50 kg/m2 or more [3].
Roux-en-Y gastric bypass (RYGB) remains widely applied [4]. Several variants of RYGB exist with remarkably consistent effects on weight loss [5,6,7,8]. Changes in size of the pouch [9], stoma [10], and minor changes in the length of the alimentary limb do not seem to impact weight loss [11]. To improve the effectiveness of RYGB, attention has thus been on the length of the common channel or the biliopancreatic limb [12, 13]. The distal RYGB is a variant with a relatively short common channel that may improve weight loss [14].
Most trials assessing bariatric surgery focus on weight loss and resolution of comorbidities. We hypothesized that distal RYGB leads to greater BMI loss 2 years after surgery compared to standard RYGB. However, we found no significant difference in BMI loss between the two procedures [15]. No studies have reported on the effect on health-related quality of life (HRQOL) and well-being, measured by patient-reported outcome measures (PROMs) after distal and proximal RYGB.
PROMs aim to assess the patients’ experience of health and well-being. Such assessment can be performed by using generic- and diagnose-specific questionnaires measuring a broad variety of dimensions of life, e.g., HRQOL, symptom burden, attitudes, and emotions. PROMs are increasingly recognized as important outcome measures after bariatric surgery, but are not systematically applied in trials on bariatric surgery [16].
In the present study, we aimed to compare the effects of standard and distal RYGB on obesity-specific HRQOL, weight-related symptoms, eating behavior, anxiety, and depression.
Methods
Trial Design and Participants
The methodology applied in this double-blind, parallel-group randomized controlled trial of standard versus distal RYGB has previously been described [17]. Briefly, all referred patients aged 18 to 60 years with a BMI of 50 to 60 kg/m2 were assessed for study enrollment at two Norwegian tertiary care centers between May 2011 and April 2013. Patients with previous bariatric or major abdominal surgery, urolithiasis, chronic liver disease, severe somatic illness, psychiatric disease, or substance abuse were excluded. The 2-year follow-up was completed in May 2015.
Eligible patients were randomly assigned to undergo either standard or distal RYGB using a 1:1 allocation ratio. Patients, follow-up study personnel at the outpatient clinic, and clinicians providing outpatient follow-up were all blinded to treatment allocation.
The study was approved by the Regional Ethics Committees for Medical and Health Research and registered in Clinical Trials: www.clinicaltrials.gov Identifier: NCT00821197. All patients provided written and informed consent.
Interventions and Follow-up
An antegastric antecolic Roux-en-Y configuration with a gastric pouch of about 25 ml and a biliopancreatic limb of 50 cm were used in both procedures. The standard RYGB had an alimentary limb of 150 cm, whereas the distal RYGB had a common channel of 150 cm. Questionnaires were self-administered and completed at baseline, and follow-up data were collected at scheduled visits 1 and 2 years after surgery.
Patient-Reported Outcome Measures
Moorhead Ardelt Quality of Life Questionnaire II (Moorhead-Ardelt)
The Moorhead-Ardelt is a validated obesity-specific instrument measuring postoperative outcomes of self-perceived quality of life [18]. It consists of six domains measured on a 10-point scale from − 0.50 to + 0.50. The domains are added into a sum score ranging from − 3.0 to + 3.0, scoring from a very poor to a very good outcome. A sum score corresponding to good or very well is considered satisfactory. The questionnaire was administered at both baseline, and 1- and 2-year follow-up [18].
Obesity and Weight-Loss Quality of Life
The validated obesity-specific Obesity and Weight-Loss Quality of Life (OWLQOL) measures feelings and emotions resulting from being obese and trying to lose weight [20]. The instrument consists of 17 statements rated from zero (“not at all”) to six (“a very great deal) on a 7-point scale. The 17 items form a sum scale ranging from 0 to 102, with higher scores indicating better emotional HRQOL. As proposed by scale authors, the scoring syntax converts the scale to 0–100. The questionnaire was administered at both baseline, 1- and 2-year follow-up [19, 20].
Weight-Related Symptom Measure
The validated obesity-specific Weight-Related Symptom Measure (WRSM) measures 20 symptoms commonly related to being overweight or obese, including foot problems, joint pain, sensitivity to cold, and shortness of breath using two different sets of items [20, 21]. The first set assesses whether or not a patient is experiencing specific symptoms, and the second set rates the level of the distress of the symptoms with values from zero (“not at all”) to six (“bothers a very great deal”). The first set creates an additive scale summing symptoms from 0 to 20, while the second forms a symptom distress scale ranging from 0 to 120. This was administered at both baseline, 1- and 2-year follow-up [19, 20].
Three-Factor Eating Questionnaire-R 21
The validated generic Three-Factor Eating Questionnaire-R 21 (TFEQ-R21) measures eating behavior and has been validated for use in individuals with obesity [22, 23]. It consists of 21 items comprising three domain scores: (1) uncontrolled eating, assessing the tendency to lose control over eating when feeling hungry or when exposed to external stimuli; (2) cognitive restraint, assessing the conscious restriction of food intake to control body weight or body shape; and (3) emotional eating, assessing overeating related to negative mood states. The domain scores were transformed to 0–100 scales to facilitate comparison; a higher score indicates more uncontrolled, restraint, or emotional eating. This questionnaire was administered only at the 2-year follow-up.
Hospital Anxiety and Depression Scale
The validated generic Hospital Anxiety and Depression Scale (HADS) measures symptoms of anxiety and depression using 14 items scored from 0 to 3 [24, 25]. It is decomposed into two domains measuring depression (HADS-D) and anxiety (HADS-A), both consisting of seven items yielding a score from 0 to 21. Norwegian normative data are available [26]. A cutoff point of > 8 yields an adequate sensitivity and specificity for clinically relevant symptoms of depression or anxiety [27]. The form was administered only at the 2-year follow-up.
Statistical Analyses
Continuous variables are described with mean and standard deviation (SD), categorical variables with counts and percentages. Possible differences between groups regarding all continuous outcomes with repeated measurements were modeled using linear mixed models for repeated measurements with unstructured covariance matrix. Each model contained fixed effects for treatment, time (measured in weeks after surgery), treatment × time interaction, and a random intercept. Based on these linear mixed models, we estimated mean treatment group values with 95% confidence intervals (CIs) for all time points: baseline, 1, and 2 years after surgery. In addition, we estimated the mean within-group changes from baseline to 2 years and the between-group difference in change from baseline to 2 years.
Possible differences between treatment groups regarding PROMs available at 2 years only (HADS and TFEQ) were assessed with independent samples t test and Fisher’s exact test. Crude associations between pairs of categorical variables were assessed using Fischer’s exact test when appropriate. Standardized effect sizes (ES) were estimated from independent samples t test as mean change from baseline divided by the pooled standard deviation of the baseline score; we used estimated values from the mixed model when possible. An ES below 0.2 was considered trivial, 0.2 to 0.49 small, 0.50 to 0.79 moderate, and 0.80 and greater large [28]. All tests were two-sided and p values < 0.05 were considered statistically significant.
IBM SPSS Statistics for Windows, Version 21.0, was used for the statistical analyses.
Missing Data
Missing values were not imputed, except where the scoring guidelines for OWLQOL and WRSM described how missing data should be handled. Mixed model estimations do not require full data sets and use all available data to estimate the results, and the covariance matrix handles missing data without requirements for imputation.
Results
A total of 113 patients received the allocated treatment: 57 standard and 56 distal RYGBs. Baseline demographics, education, employment, and anthropometrics were comparable between groups (Table 1). The follow-up rate was 97% (n = 110). Table 2 shows completion rates of PROMs at all study visits with an overall completion rate of 95% on all forms.
All scales had satisfactory internal consistency with Cronbach’s alpha coefficients > 0.7.
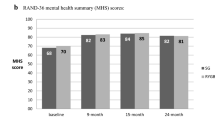
As previously reported at 2 years, the total BMI loss was 17.8 (95% CI, 16.9–18.6) kg/m2 after standard and 17.2 (95% CI, 16.3–18.0) kg/m2 after distal, with no significant between-group differences (p = 0.32). For general health-related quality of life, the physical summary score was improved and the mental summary score was unchanged for both surgical groups, with no significant between-group difference [15].
Table 3 shows baseline, 1-, and 2-year results as well as estimated within-group changes and between-group differences in PROMS concerning obesity-specific HRQOL and weight-related symptoms.
Obesity-Specific HRQOL
Obesity-related quality of life (OWLQOL) improved significantly in both groups, with no significant between-group differences.
Self-perceived quality of life improved significantly for all dimensions except for the work-related dimension after standard RYGB, and general self-esteem after distal RYGB. At baseline, 23% of patients reported a good to very good quality of life while 2 years after surgery, this increased to 51% of patients, with no difference between groups (Table 4).
Weight-Related Symptoms
Patients in both groups experienced a significant reduction in the number of weight-related symptoms and symptom distress score with no significant difference between the groups.
Most of the improvement in HRQOL and weight-related symptoms occurred during the first year, with only small changes between 1 and 2 years after surgery. Figure 1 shows estimated changes in obesity-specific HRQOL and weight-related symptoms over time.

Modeled changes in obesity-specific quality of life and weight-related symptoms after standard and distal RYGB
Eating Behavior
The mean (95% CI) eating behavior scores did not differ significantly between groups after surgery: uncontrolled eating after standard RYGB (22.0 (17.2–26.7)) vs. distal RYGB (28.9 (23.3–34.5), p = 0.06), cognitive restraint (57.4 (52.0–62.7) vs. 62.1 (57.9–66.2) points, p = 0.16), and emotional eating (26.8 (20.5–33.1) vs. 32.6 (25.5–39.7) points, p = 0.22).
Anxiety and Depression
The mean (SD) scores at 2 years for anxiety (HADS-A) were 5.2 (4.1–6.4) points for standard and 5.1 (4.0–6.1) points for distal RYGB, respectively (p = 0.81), and the prevalence of clinically relevant anxiety was 22% after standard and 11% after distal RYGB (p = 0.13). The mean (SD) depression scores were 2.8 (1.8–3.8) points for standard and 2.1 (1.3–3.0) points for distal (p = 0.32), and the prevalence of clinically relevant depression was 9% after standard and 5% after distal (p = 0.49).
Discussion
We found improvements in most PROMs after both standard and distal RYGB, but no significant differences between groups after surgery in regard to obesity-specific HRQOL, weight-related symptoms, anxiety and depression, or eating behavior. There was comparable weight loss between the two groups, and we suspect the amount of weight lost could be a major determinant of improvement in HRQOL and other PROMs after bariatric surgery [13].
To the best of our knowledge, this is the first study assessing changes in HRQOL, health, and well-being after distal RYGB. Studies comparing RYGB with more radical surgical procedures such as duodenal switch have shown comparable results on change in HRQOL, despite increased weight loss and more malabsorption after duodenal switch [29].
The improvement in obesity-specific quality of life is comparable to other studies on RYGB [21]. When looking at effect sizes, there was a small difference (ES = 0.26) for improving weight-related symptoms in favor of distal RYGB; however, the implication of this finding is uncertain.
To the best of our knowledge, this is the first study to assess anxiety and depression when comparing standard and distal RYGB, but the scores for anxiety and depression may be compared to the normal population [26] and studies of other bariatric procedures. The mean scores of anxiety are higher than the population norm of obese patients (BMI > 35 kg/m2). Aasprang et al. published a study on duodenal switch showing improved anxiety from baseline to 2 years and a worsening of symptoms from 2 to 5 years. The mean (95% CI) HADS-A at 2 years in their study was 4.7 (3.7–5.8), slightly lower but comparable to our 2-year results and the scores for anxiety are comparable to their 2-year results [30]. Both results are higher than the Norwegian population for BMI > 35 kg/m2, but high-quality data from patients in the BMI 50–60 kg/m2 range is lacking. Other studies have shown improvement in depression after bariatric surgery [31], and both our groups have mean scores comparable to a non-obese population. Long-term follow-up is needed to adequately study this.
Previous studies describe significant improvements in uncontrolled and emotional eating after both RYGB and duodenal switch, but with no significant differences between groups [32], which is in line with our observations. Previous studies have not shown significant changes in cognitive restraint, and our results are slightly higher for both proximal and distal RYGB than those published by Søvik et al. Although non-significant (p = 0.06), the mean uncontrolled eating score was slightly higher in the distal RYGB group than in the standard RYGB group in the present study. The lack of baseline data makes the clinical implication of this finding uncertain.
Strengths of this study include the double-blind randomized controlled design and standardized surgical procedures. The patients had a BMI in the 50–60 kg/m2 range, creating a homogenous population. Nearly all patients attended follow-up, and the completion rates of questionnaires were high. All patients were recruited from two public hospitals, and treatment provided was independent of health insurance and personal finance.
An important limitation is that evaluation of PROMS was a secondary endpoint. This might induce sample size issues such as type II errors. To evaluate potential differences, we calculated effect sizes to estimate any potentially undetected differences. Only some of the effect sizes are small; all others are trivial suggesting negligible differences. Another limitation is that eating behavior, anxiety, and depression were only measured at 2 years, making comparison of changes impossible. Despite the randomized controlled design, small random differences cannot be excluded.
Standardized reporting of PROMs is gaining more attention and may help patients and clinicians choose appropriate procedures. However, several of the obesity-specific measures of HRQOL are in fact weight dependent and might not differentiate adequately between the adverse effects of surgical procedures. Relevant differences between the procedures with regard to gastrointestinal symptoms and eating quality as well as behavior and specific adverse events are not adequately covered by existing PROMs. The GQLI index measures gastrointestinal symptoms with regard to quality of life [33], but does not explore other post-bariatric problems such as dumping and postprandial hypoglycemia. The development of a symptom measure focusing exclusively on these problems might help clinicians and patients differentiate between different bariatric procedures. However, if differences are subtle and not detectable by existing PROMS, the impact is likely to be small.
The greatest improvement in quality of life and resolution of weight-specific symptoms occur during the first year after bariatric surgery during the greatest weight loss. Weight loss may thus be an important determinant for improvement of quality of life. However, assuming that greater weight loss would improve quality of life even more is not so certain. It could be that the improvement is mostly due to the initial weight loss, and that further weight loss would not lead to further improvement in quality of life. In a study of duodenal switch and RYGB, the increased weight loss after duodenal switch did not translate into increased quality of life [34]. The large initial weight loss may decrease the patients’ feeling of stigma and increase a feeling of normality and this trumps some of the adverse effects of bariatric surgery, at least in short term. Studies have shown that 5-year HRQOL decreased significantly when compared with the scores 1–2 years post surgically [16]. Thus, the 2-year span may not be a sufficient length to detect clinically relevant differences in PROMs.
Our findings cannot be extrapolated to other variants of distal RYGB that might lead to more malabsorption and greater weight loss. At 2 years, we find no evidence to support the use of distal RYGB; however, evaluations following prolonged follow-up may reveal other findings.
Conclusion
In patients with BMI 50–60 kg/m2, both standard and distal RYGB lead to sustained weight loss and improved HRQOL 2 years after surgery. We found no significant differences between the two procedures in regard to obesity-specific HRQOL, weight-related symptoms, anxiety and depression, and eating behavior. Standard RYGB continues to be our first choice in treating patients with BMI above 50 kg/m2.
References
Sundbom M. Laparoscopic revolution in bariatric surgery. World J Gastroenterol. 2014;20:15135–10.
Colquitt JL, Pickett K, Loveman E. Surgery for weight loss in adults. Cochranne Database Syst Rev. 2014;8(8):CD003641. https://doi.org/10.1002/14651858.CD003641.pub4.
Orci L, Chilcott M, Huber O. Short versus long Roux-limb length in Roux-en-Y gastric bypass surgery for the treatment of morbid and super obesity: a systematic review of the literature. Obes Surg. Springer-Verlag. 2011;21:797–804.
Angrisani L, Santonicola A, Iovino P, et al. Bariatric surgery worldwide 2013. Obes Surg. 2015;25:1822–32.
Mehaffey JH, LaPar DJ, Clement KC, et al. 10-year outcomes after Roux-en-Y gastric bypass. Ann Surg. 2016;264:121–6.
Aftab H, Risstad H, Søvik TT, et al. Five-year outcome after gastric bypass for morbid obesity in a Norwegian cohort. SOARD. Elsevier. 2014;10:71–8.
Adams TD, Pendleton RC, Strong MB, et al. Health outcomes of gastric bypass patients compared to nonsurgical, nonintervened severely obese. Obesity. 2012;18:121–30.
Suter M, Donadini A, Romy S, et al. Laparoscopic Roux-en-Y gastric bypass: significant long-term weight loss, improvement of obesity-related comorbidities and quality of life. Ann Surg. 2011;254:267–73.
Edholm D, Ottosson J, Sundbom M. Importance of pouch size in laparoscopic Roux-en-Y gastric bypass: a cohort study of 14,168 patients. Surg Endosc. Springer US. 2015;30:2011–5.
Shope TR, Cooney RN, McLeod J, et al. Early results after laparoscopic gastric bypass: EEA vs GIA stapled gastrojejunal anastomosis. Obes Surg. Springer-Verlag. 2003;13:355–9.
Mahawar KK, Kumar P, Parmar C, et al. Small bowel limb lengths and Roux-en-Y gastric bypass: a systematic review. Obes Surg. 2016;26:660–71.
Stefandis D, Kuwada TS, Gersin KS. The importance of the length of the limbs for gastric bypass patients—an evidence-based review. Obes Surg. 2011;
Kalferantoz F, Skroubis G, Karamanakos S, et al. Biliopancreatic diversion with Roux-en-Y gastric bypass and long limbs: advances in surgical treatment for super-obesity. Obes Surg. 2011;21(12):1849–58.
Brolin RE, LaMarca LB, Kenler HA, et al. Malabsorptive gastric bypass in patients with superobesity. J Gastrointest Surg. 2002;6:195–203. discussion204–5
Risstad H, Svanevik M, Kristinsson JA, et al. Standard vs distal Roux-en-Y gastric bypass in patients with body mass index 50 to 60. JAMA Surg. 2016;151:1146–10.
Andersen JR, Aasprang A, Karlsen T-I, et al. Health-related quality of life after bariatric surgery—a systematic review of prospective long-term studies. SOARD. Elsevier. 2015;11:466–73.
Svanevik M, Risstad H, Hofsø D, et al. Perioperative outcomes of proximal and distal gastric bypass in patients with BMI ranged 50–60 kg/m(2)—a double-blind, randomized controlled trial. Obes Surg. 2015;25:1788–95.
Moorehead MK, Ardelt-Gattinger E, Lechner H, et al. The validation of the Moorehead-Ardelt Quality of Life Questionnaire II. Obes Surg. Springer-Verlag. 2003;13:684–92.
Niero M, Martin M, Finger T, et al. A new approach to multicultural item generation in the development of two obesity-specific measures: the Obesity and Weight Loss Quality of Life (OWLQOL) questionnaire and the Weight-Related Symptom Measure (WRSM). Clin Ther. 2002;24:690–700.
Patrick DL, Bushnell DM, Rothman M. Performance of two self-report measures for evaluating obesity and weight loss. Obes Res. Blackwell Publishing Ltd. 2004;12:48–57.
Karlsen T-I, Lund RSR, Røislien JR, et al. Health related quality of life after gastric bypass or intensive lifestyle intervention: a controlled clinical study. Health Qual Life Outcomes. 2013;11:1–1.
Cappelleri JC, Bushmakin AG, Gerber RA, et al. Psychometric analysis of the Three-Factor Eating Questionnaire-R21: results from a large diverse sample of obese and non-obese participants. Int J Obes (Lond). Nature Publishing Group. 2009;33:611–20.
Karlsson J, Persson LO, Sjöström L, et al. Psychometric properties and factor structure of the Three-Factor Eating Questionnaire (TFEQ) in obese men and women. Results from the Swedish Obese Subjects (SOS) study. Int J Obes Relat Metab Disord. 2000;24:1715–25.
Herrmann C. International experiences with the Hospital Anxiety and Depression Scale—a review of validation data and clinical results. J Psychosom Res. 1997;42:17–41.
Bjelland I, Dahl AA, Haug TT, et al. The validity of the Hospital Anxiety and Depression Scale. An updated literature review. J Psychosom Res. 2002;52:69–77.
Brunes A, Augestad LB, Gudmundsdottir SL. Personality, physical activity, and symptoms of anxiety and depression: the HUNT study. Soc Psychiatry Psychiatr Epidemiol. Springer-Verlag. 2012;48:745–56.
Bjelland I, Lie SA, Dahl AA, et al. A dimensional versus a categorical approach to diagnosis: anxiety and depression in the HUNT 2 study. Int J Methods Psychiatr Res. 2009;18:128–37.
Cohen J. Statistical power analysis for the behavioral sciences Lawrence Earlbaum Associates. Hillsdale; 1988.
Søvik TT, Aasheim ET, Taha O, et al. Weight loss, cardiovascular risk factors, and quality of life after gastric bypass and duodenal switch: a randomized trial. Ann Intern Med. American College of Physicians. 2011;155:281–91.
Aasprang A, Andersen JR, Våge V, et al. Five-year changes in health-related quality of life after biliopancreatic diversion with duodenal switch. Obes Surg. 2013;23:1662–8.
Gade H, Friborg O, Rosenvinge JH, et al. The impact of a preoperative cognitive behavioural therapy (CBT) on dysfunctional eating behaviours, affective symptoms and body weight 1 year after bariatric surgery: a randomised controlled trial. Obes Surg. 2015;25:2112–9.
Søvik TT, Karlsson J, Aasheim ET, et al. Gastrointestinal function and eating behavior after gastric bypass and duodenal switch. SOARD. Elsevier Inc. 2013;9:641–7.
Eypasch E, Williams JI, Wood-Dauphinee S, et al. Gastrointestinal Quality of Life Index: development, validation and application of a new instrument. Br J Surg. 1995;82:216–22.
Risstad H, Søvik TT, Engström M, et al. Five-year outcomes after laparoscopic gastric bypass and laparoscopic duodenal switch in patients with body mass index of 50 to 60. JAMA Surg. American Medical Association. 2015;150:352–10.
Acknowledgements
We thank Linda Mathisen (Vestfold Hospital Trust) and Marianne Sæther (Oslo University Hospital), for general project support, and finally, we thank all the patients for participating in the study.
Funding
Marius Svanevik have received research grant from the South-Eastern Norway Regional Health Authority.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
Dr. Marius Svanevik reports grants from Southern and Eastern Norway Health Authority, during the conduct of the study.
Dr. Hilde Risstad has nothing to disclose.
Dr. Tor-Ivar Karlsen has nothing to disclose.
Dr. Jon A. Kristinsson has nothing to disclose.
Dr. Milada Cvancarova Småstuen has nothing to disclose.
Dr. Ronette L Kolotkin reports personal fees from Morbid Obesity Centre, Vestfold Hospital Trust, Tønsberg, Norway, during the conduct of the study.
Dr. Torgeir T Søvik has nothing to disclose.
Dr. Rune Sandbu has nothing to disclose.
Dr. Tom Mala reports grants from Health Region South East, Norway, during the conduct of the study; other from Medtronic, travel support to congress as invited lecturer outside the submitted work.
Dr. Jøran Hjelmesæth has nothing to disclose.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Human and Animal Rights
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Registration
www.clinicaltrials.gov no: NCT00821197
Additional information
The current study is a work-intensive collaboration between two bariatric centers in South Eastern Norway. All authors fulfill all four ICMJE criteria and have been active in planning and running the study, patient follow-up and treatment, and critical revision of the manuscript.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Svanevik, M., Risstad, H., Karlsen, TI. et al. Patient-Reported Outcome Measures 2 Years After Standard and Distal Gastric Bypass—a Double-Blind Randomized Controlled Trial. OBES SURG 28, 606–614 (2018). https://doi.org/10.1007/s11695-017-2891-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-017-2891-3