
Abstract
Background
Bariatric approach to obesity provides substantial weight loss and comorbidity resolution. Our unique service includes pre- and postoperative visits to the Health and Nutrition Clinic headed by a specialist in gastroenterology and nutrition. We compared patients attending regular clinic routine with those who were lost to follow-up with regard to anthropometry, comorbidity, quality of life, and food tolerance and determined who benefited most from the operation.
Methods
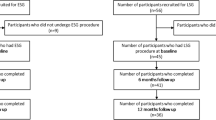
A retrospective review was performed on patients 30 months after undergoing sleeve gastrectomy. Body mass index was used to report weight loss. Bariatric Analysis and Reporting Outcome System (BAROS) and Food Tolerance Score were (FTS) completed by all patients at the 30-month follow-up visit and compared between two groups (group I—30 months of active postoperative follow-up; group II—without).
Results
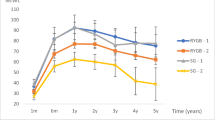
A total of 119 patients participated in the study. For groups I and II, the mean percentage of excess BMI loss at 30 months was 82.08 ± 9.83 and 74.88 ± 8.75, respectively, with better comorbidity improvement in group I. BAROS scores were 7.62 ± 0.72 and 6.92 ± 0.92. FTS was 24.30 ± 2.09 and 22.55 ± 2.27, respectively.
Conclusions
From our experience, getting the most from the sleeve is attributed to two main factors: surgery and nutrition. Surgery results in optimal restriction and improved satiety, whereas nutrition relies on a professional medical team providing constant, ongoing patient support throughout all the bariatric process stages. These teams of surgeons and gastroenterologists specializing in nutrition, working side by side, each in their area of specialty, are the main pillars leading to the success of the sleeve.
Similar content being viewed by others

References
James PT, Rigby N, Leach R. International Obesity Task Force—The obesity epidemic, metabolic syndrome and future prevention strategies. Eur J Cardiovasc Prev Rehabil. 2004;11(1):3–8.
Overweight, obesity, health risk: National Task Force on the prevention and treatment of obesity. Arch Intern Med 2000;160:898–904.
Mizuno T, Shu IW, Makimura H, et al. Obesity over the life course. Sci Aging Knowledge Environ. 2004;16(24):4.
Fontaine KR, Redden DT, Wang C, et al. Years of life lost due to obesity. JAMA. 2003;289(2):187–93.
Goodrick GK, Poston 2nd WS, Foreyt JP. Methods for voluntary weight loss and control: update. Nutrition. 1996;12:672–6.
Oluseun AS, Yood SM, Courtney J, et al. Natural history of morbid obesity without surgical intervention. Surg Obes Relat Dis. 2007;3:73–7.
Karlsson J, Taft C, Ryden A, et al. Ten-year trends in health related quality of life after surgical and conventional treatment for severe obesity: the SOS intervention study. Int J Obes Lond. 2007;31:1248–61.
Buchwald H, Avidor Y, Braunwald E, et al. Bariatric surgery, a systematic review and meta-analysis. JAMA. 2004;292:1724–8.
Vidal J, Ibarzabal A, Nicolau J, et al. Short-term effects of sleeve gastrectomy on type 2 diabetes mellitus in severely obese subjects. Obes Surg. 2007;17:1069–74.
Karamanakos SN, Vagenas K, Kalfarentzos F, et al. Weight loss, appetite suppression, and changes in fasting and postprandial ghrelin and peptide-YY levels after Roux-en-Y gastric bypass and sleeve gastrectomy: a prospective, double blind study. Ann Surg. 2008;247(3):408–10.
Akkary E, Duffy A, Bell R. Deciphering the sleeve: technique, indications, efficacy, and safety of sleeve gastrectomy. Obes Surg. 2008;18(10):1323–9.
Oria HE. Moorehead MK Updated Bariatric Analysis and Reporting Outcome System (BAROS). Surg Obes Relat Dis. 2009;5(1):60–6.
Deitel M, Greenstein RJ. Recommendations for reporting weight loss. Obes Surg. 2003;13:159–60.
Suter M, Calmes JM, Paroz A, et al. A new questionnaire for quick assessment of food tolerance after bariatric surgery. Obes Surg. 2007;17:2–8.
World Health Organization. Overweight and obesity. Factsheet no. 311. Geneva: World Health Organization; 2006.
Avenell A, Broom J, Brown TJ, et al. Systematic review of the long-term effects and economic consequences of treatments for obesity and implications for health improvement. Health Technol Assess. 2004;8:1–194.
Avenell A, Sattar N, Lean M. Management: part I—behaviour change, diet, and activity. BMJ. 2006;333:740–3.
Kral JG. Management: part III—surgery. BMJ. 2006;333:900–3.
US Preventive Services Task Force. Screening for obesity in adults: recommendations and rationale. Ann Intern Med. 2003;139:930–2.
Deitel M, Gawdat K, Melissas J. Reporting weight loss. Obes Surg. 2007;17:565–8.
Greenstein R. Reporting weight loss. Obes Surg. 2007;17:1275–6.
Baltasar A, Deitel M, Greenstein R. Letter to the Editor. Weight loss reporting. Obes Surg. 2008;18:761–2.
Dixon J, Phail T, O’Brien PE. Minimal reporting requirements for weight loss: current methods not ideal. Obes Surg. 2005;15:1034–9.
National Institute for Health and Clinical Excellence. Obesity—guidance on the prevention, identification, assessment and management of overweight and obesity in adults and children. London: The Stationery Office; 2006. Clinical Guideline 43.
Cottam D, Qureshi FG, Mattar SG, et al. Laparoscopic sleeve gastrectomy as an initial weight-loss procedure for high-risk patients with morbid obesity. Surg Endosc. 2006;20:859–63.
Stroh C, Birk D, Flade-Kuthe R, et al. Results of sleeve gastrectomy—data from a nationwide survey on bariatric surgery in Germany. Obes Surg. 2009;19:105–12.
Vidal J, Ibarzabal A,Romero, et al. Type 2 diabetes mellitus and the severely obese subjects. Obes Surg 2008;18(9):1077e82.
Sánchez-Santos R, Masdevall C, Baltasar A, et al. Short and midterm outcomes of sleeve gastrectomy for morbid obesity: the experience of the Spanish National Registry. Obes Surg 2009;19:1203–1210.
Mejía-Rivas M, Remes-Troche J, Montaño-Loza A, et al. Gastric capacity is related to body mass index in obese patients. A study using the water load test. Rev Gastroenterol Mex. 2009;74(1):71–3.
Weiner RA, Weiner S, Pomhoff I, et al. Laparoscopic sleeve gastrectomy—influence of sleeve size and resected gastric volume. Obes Surg. 2007;17:1297–305.
Langer FB, Reza Hoda MA, Bohdjalian A, et al. Sleeve gastrectomy and gastric banding: effects on plasma ghrelin levels. Obes Surg. 2005;15:1024–9.
Abu-Jaish W, Ramirez A, Patel S et al. Prevalence of nutritional deficiencies after laparoscopic sleeve gastrectomy as a final step in morbidly obese patients. Presented at the ASMBS 26th Annual Meeting. Grapevine, TX, USA, 21–26 June, 2009.
John Melissas IFSO Guidelines for Safety, Quality, and Excellence in Bariatric Surgery Obes Surg 2008;18:497–500.
Kafri N, Valfer R, Nativ O, et al. Health behavior, food tolerance, and satisfaction after laparoscopic sleeve gastrectomy. Surg Obes Relat Dis. 2011;7(1):82–8.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Keren, D., Matter, I., Rainis, T. et al. Getting the Most from the Sleeve: The Importance of Post-Operative Follow-up. OBES SURG 21, 1887–1893 (2011). https://doi.org/10.1007/s11695-011-0481-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-011-0481-3