
Abstract
Background
Swedish adjustable gastric banding (SAGB) is an effective treatment for morbid obesity. The aim of this study was to assess the efficacy and safety of SAGB in older patients aged ≥50 years.
Methods
Between January 1996 and January 2006, 134 patients (102 women, 32 men) of 785 consecutive patients who underwent SAGB during the study period were aged ≥50 years. Two groups of patients were analyzed: Group 50 (n = 107) patients aged 50–59 years and Group 60 (n = 27) patients aged 60–69 years. All data (demographic and morphologic data, operative data, and follow-up data) were prospectively collected in a computerized databank.
Results
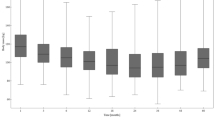
One hundred thirty-four patients (17.1%) out of 785 entered the study. Mean percentage of excess weight loss (%EWL) was 37.5 at 1 year and 48.8 at 7 years, body mass index (BMI) fell from 43.3 to 33.1 at 7 years. In the 134 patients, there were 65 patients with 121 complications (48.5%) and 69 patients with no complication (51.5%). The most common complications were esophagitis (27%), esophageal dilation (16%), port problems (11%), pouch dilation (11%), band leakage (9%), and band migration (7%). Overall, 46 patients (34%) needed a reoperation. In Group 50, mean %EWL was 38.4 at 1 year and 54.9 at 7 years. BMI fell from 42.9 to 33.1 at 7 years. In the 107 patients, there were 55 patients with 99 complications (51%) and a reoperation rate of 35.5%. In Group 60, mean %EWL was 32.8 at 1 year and 41.2 at 7 years. BMI fell from 44.3 to 34 at 7 years. In the 27 patients, there were ten patients with 22 complications (37%) and a reoperation rate of 29.6%. There was no mortality.
Conclusions
At 7-year follow-up, for older patients, SAGB is an effective bariatric procedure for achieving weight loss. Nevertheless, based on the high complication and reoperation rate, a gastric band-specific patient selection will be necessary.


Similar content being viewed by others

References
Buettner T. Sex differentials in old-age mortality. Popul Bull UN 1995;39:18–44.
Andrews GR. Demographic and health issues in rural aging: a global perspective. J Rural Health 2001;17:323–7.
Mittermair R, Weiss H, Nehoda H, et al. Laparoscopic Swedish adjustable gastric banding: 6-year follow-up and comparison to other laparoscopic bariatric procedures. Obes Surg. 2003;13:412–7.
Deitel M, Crosby RD, Gagner M. The first international consensus summit for sleeve gastrectomy. Obes Surg. 2008;18:487–96.
Wittgrove AC, Clark GW, Schubert KR. Laparoscopic gastric bypass, Roux-en-Y 500 patients: technique and results, with 3–60 months follow-up. Obes Surg. 2000;10:233–9.
Ren CJ, Patterson E, Gagner M. Eraly results of laparoscopic biliopancreatic diversion with duodenal switch. Obes Surg. 2000;10:514–23.
Milone L, Daud A, Durak E, et al. Esophageal dilation after laparoscopic adjustable gastric banding. Surg Endosc. 2008;22:1482–6.
Chevallier JM, Zinzindohoue F, Douard R, et al. Complications after laparoscopic adjustable gastric banding for morbid obesity: experience with 1,000 patients over 7 years. Obes Surg. 2004;14:407–14.
Weiner R, Blanco-Endert R, Weiner S, et al. Outcome after laparoscopic adjustable gastric banding – 8 years experience. Obes Surg. 2003;13:427–34.
Kennedy RL, Chokkalingham K, Srinivasan R. Obesity in the elderly: who should be treating, and why and how? Curr Opin Clin Nutr Metab Care 2004;7:3–9.
Silecchia G, Greco F, Bacci V, et al. Results after laparoscopic adjustable gastric banding in patients over 55 years of age. Obes Surg 2005;15:351–6.
Sugermann HJ, DeMaria EJ, Kellum JM, et al. Effects of bariatric surgery in older patients. Ann Surg 2004;240:243–7.
Papaavas PK, Gagne DJ, Kelly J, et al. Laparoscopic Roux-en-Y gastric bypass is a safe and effective operation for the treatment of morbid obesity in patients older than 55 years. Obes Surg 2004;14:1045–61.
Taylor CJ, Layani L. Laparoscopic adjustable gastric banding in patients ≥60 years old. Obes Surg. 2006;16:1579–83.
Balsiger B, Ernst D, Giachino D, et al. Prospective evaluation and 7-year follow-up of Swedish adjustable gastric banding in adults with extreme obesity. J Gastrointest Surg. 2007;11:1470–7.
Naef M, Naef U, Mouton W, et al. Outcome and complications after laparoscopic Swedish adjustable gastric banding: 5-year results of a prospective clinical trial. Obes Surg. 2007;17:195–201.
Tolonen P, Victorzon M, Mäkelä J. 11-year experience with laparoscopic adjustable gastric banding for morbid obesity –What happend to the first 123 patients? Obes Surg. 2008;18:251–5.
Biagini J, Karam L. Ten years experience with laparoscopic adjustable gastric banding. Obes Surg. 2008;18:573–7.
Iannelli A, Dainese R, Piche T, et al. Laparoscopic sleeve gastrectomy for morbid obesity. World J Gastroenterol 2008;14:821–7.
Himpens J, Dapri G, Cadiere GB. A prospective randomized study between laparoscopic gastric banding and laparoscopic isolated sleeve gastrectomy. Obes Surg. 2006;16:1450–6.
Gutschow CA, Collet P, Prenzel K, et al. Long-term results and gastroesophageal reflux in a series of laparoscopic adjustable gastric banding. J Gastrointest Surg 2005;9:941–8.
Westling A, Bjurling K, Ohrvall M, et al. Silicone adjustable gastric banding: disappointing results. Obes Surg 1998;8:467–74.
Klaus A, Gruber I, Wetscher G, et al. Prevalent esophageal body motility disorders underlie aggravation of GERD symptoms in morbidly obese patients following adjustable gastric banding. Arch Surg. 2006;141:247–51.
Klaus A, Weiss H. Is preoperative manometry in restrictive bariatric procedures necessary? Obes Surg. 2008;18:1039–42.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Mittermair, R.P., Aigner, F. & Obermüller, S. Results and Complications After Swedish Adjustable Gastric Banding in Older Patients. OBES SURG 18, 1558–1562 (2008). https://doi.org/10.1007/s11695-008-9709-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11695-008-9709-2