
Abstract
Background
Posterior dislocation fractures of the humerus occur as impression fractures of the humeral head (reverse Hill–Sachs fracture) and posteriorly dislocated proximal humeral (PH) fractures with a subcapital component. This study evaluated fracture patterns, current treatment, and revision rates.
Methods
Data of patients who underwent surgical treatment for PH dislocation fractures in two level-I trauma centers between 2010 and 2018 were retrospectively reviewed.
Results
We identified 41 shoulders in 37 patients (n = 12 female, n = 25 male; average age 52 [25–91] years) with open surgical treatment of PH posterior dislocation fractures. In 14 patients, the cause was convulsive seizure or electrical accident, in 23 patients, a fall or high-energy trauma. There were 22 shoulders with impression fractures without a subcapital aspect; 19 shoulders had a posteriorly dislocated subcapital fracture. All patients were treated surgically via a deltopectoral approach. Five of the impression type fractures were treated prosthetically; the other 17 impression type fractures had humeral head-preserving reconstruction. The 19 cases of subcapital dislocation fractures were treated with open reduction and internal fixation with a PHILOS plate (n = 13) or with a prosthesis (n = 6). Within a mean follow-up period of 4.3 (1–9) years, the overall revision rate was 15% (6/41). Four patients underwent elective arthroscopic capsulotomy and implant removal. Two patients required revision surgery due to loss of reduction or humeral head necrosis.
Conclusion
Impression type fractures were slightly more common than posteriorly dislocated PH fractures with a subcapital fracture component. In 73% of cases (n = 30), humeral head-preserving reconstruction was performed. The overall mid-term revision rate was 15% with a low-rate of secondary conversion to total shoulder arthroplasty (3%). Longer term functional outcomes of the patients are needed to better evaluate the treatment concept.
Zusammenfassung
Hintergrund
Dorsale Luxationsfrakturen des proximalen Humerus (PH) treten als Impressionsfrakturen des Humeruskopfs (reverse Hill-Sachs-Fraktur) sowie als nach dorsal luxierte Frakturen mit subkapitaler Komponente auf. Ziel dieser Studie war es, Frakturmuster, Therapie und Revisionsraten zu evaluieren.
Methoden
Alle zwischen 2010 und 2018 an 2 überregionalen Traumazentren behandelten Patienten mit dorsalen PH-Luxationsfrakturen wurden retrospektiv erfasst.
Ergebnisse
Operativ via deltoideopektoralem Zugang behandelt wurden bei Luxationsfraktur des Humeruskopfs 41 Schultern bei 37 Patienten (12 w.; 25 m., Durchschnittsalter 52 [25–91] Jahre). Bei 14 Patienten lag der Verletzung ein Krampfanfall oder Stromunfall, bei 23 ein Sturz oder Hochrasanztrauma zugrunde. Eine Impressionsfraktur ohne subkapitale Frakturkomponente bestand bei 22 Schultern; bei 19 eine dorsale Luxationsfraktur mit subkapitaler Komponente vom Typ 5GL (n = 17) oder Typ 5G (n = 2) nach Resch. Ein endoprothetischer Ersatz erfolgte bei 5 Schultern mit Impressionsfraktur, bei den übrigen 17 Schultern erfolgte eine humeruskopferhaltende Therapie. Bei 6 der 19 Schultern mit subkapitaler Frakturkomponente wurde eine Endoprothese implantiert, bei 13 erfolgte eine winkelstabile Plattenosteosynthese. Durchschnittlich 4,3 (1–9) Jahre postoperativ betrug die Gesamtrevisionsrate 15% (6/41). Durchschnittlich 11 Monate postoperativ erfolgte bei 4 Patienten eine elektive arthroskopische Arthrolyse mit Implantatentfernung. Bei 2 Patienten wurde eine Revision bei ossärer Komplikation erforderlich.
Schlussfolgerung
Reine Impressionsfrakturen waren etwas häufiger als dorsale Luxationsfrakturen des PH mit subkapitaler Komponente. In 73 % der Fälle (n = 30) erfolgte eine humeruskopferhaltende Therapie. Die mittelfristige Revisionsrate betrug 15 % bei insgesamt niedriger Konversionsrate zur sekundären Prothese (3 %). Funktionelle Langzeitergebnisse sind erforderlich, um das Behandlungskonzept besser beurteilen zu können.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Shoulder dislocations are the most common joint dislocations in humans with an incidence of 24/100,000 patient years [1]. In the literature, more than 90% of these are ascribed to anterior dislocations of the shoulder, while only 2–4% of cases are posterior shoulder dislocations [2,3,4]. The combination of a posterior shoulder dislocation with a fracture of the proximal humerus occurs even less frequently. In most cases, the cause of these combination injuries is convulsive seizure, high-energy trauma such as a traffic accident, or electrical accident [5,6,7,8,9]. A common complication following a posterior fracture dislocation of the humerus is a locked position of the joint surface on the posterior glenoid rim [10, 11]. When presented in the emergency room, this situation often remains undiagnosed [12,13,14,15,16,17,18,19,20]. This adds to the already complex nature of the posterior dislocation fracture of the humerus, which requires an elaborate open reduction and internal fixation. Humeral head necrosis is a feared complication in such complex fractures [21].
Impression type fractures, usually presenting with an osteochondral impression of the ventromedial joint surface of the humerus (so-called reverse Hill–Sachs lesion or Malgaigne fracture [RHSL]), must be distinguished from fractures with a subcapital component [22]. In previous studies, a high occurrence of complications, and therefore poor functional outcomes, was reported [23, 24]. Surgical options include joint replacement as well as surgical treatments that aim to preserve the humeral head by open reduction and internal fixation, with the use of auto- or allografts [12, 14, 25,26,27,28,29,30,31,32,33,34]. More recent publications have been primarily case reports, while larger case series often date back more than 10 years [31, 32, 34, 35].
The aim of this study was to evaluate fracture types and the surgical treatment reality of posterior humeral dislocation fractures, including revision rates, in two level-1 trauma centers.
Patients and methods
A retrospective data evaluation of posterior humeral dislocation fractures treated surgically between January 2010 and January 2018 was performed from the clinical databases of two level-I trauma centers (Department of Trauma, Hand and Reconstructive Surgery, University Hospital Münster, Münster, Germany; Department of Trauma and Orthopedic Surgery, Diakovere Friederikenstift GmbH, Hannover, Germany). Only patients who were treated operatively within 3 weeks of the trauma were included in this study. These fractures were subcategorized into impression type fractures and fractures with a subcapital component. The date and cause of trauma were identified, as well as the initial treatment.
The fractures were subdivided by choice of treatment and the date of surgery was recorded. For both fracture types, a distinction was made between fractures that were treated surgically with a humeral head-preserving reconstruction (e.g. plate or screw fixation, allograft, autograft) and those that were treated with arthroplasty. To define the extent of the impression type fractures (RHSL), the gamma angle was measured on axial computed tomography (CT) scans as described by Moroder et al. [36] The fractures with a subcapital component were classified according to Resch [37]. Head-split fractures, as well as those with an RHSL, were identified. Data was also collected on whether CT imaging was performed, and which surgical approach was carried out. The operative procedures were analyzed with a focus on the use of allografts and autografts, the type of fixation, and arthroplasty. The duration of surgery and the experience of the surgeon were recorded. Complications, both during the stay on the ward as well as in the ambulatory sector, were studied. The last follow-up appointment and the last known clinical examination results, including level of pain and range of motion (ROM) of the affected shoulder, were identified. Finally, the last radiographic examination was analyzed.
The fractures were subcategorized into the following groups: (1) isolated impression type fracture with an RHSL, and (2) posterior dislocation fracture with a subcapital element of the humerus.
Follow-up regarding revision surgeries was obtained using the hospitals medical record system. A mandatory follow-up period of at least 12 months was set in order to evaluate secondary surgical interventions. Those interventions were further subdivided into implant-related revisions to remove the metal implants and revisions to address non-implant-related complications.
Statistical differences were calculated with a two-tailed t test and the significance level was set at <0.05.
Results
In total, 41 shoulders in 37 patients (n = 12 female, n = 25 male) with open surgical treatment of posterior humeral head dislocation fractures were identified in the 8‑year period. Two fractures (5%) were initially treated conservatively in other hospitals and were referred to one of the aforementioned trauma centers for re-evaluation. Four patients incurred bilateral fractures, all of which resulted from convulsive seizure or electrical accident. The mean age of the patients at the time of the injury was 52 (range: 25–91) years. The mechanism of trauma was a direct fall on the affected shoulder in 21 patients, convulsive seizure in 12 patients, electrical accident in two patients, and direct high-force trauma in two cases. Moreover, 22 shoulders (n = 18 male, n = 4 female; average age: 48 years, range: 27–81 years) presented with impression type fractures without a subcapital fracture of the humerus (Fig. 1). There were 19 shoulders (n = 10 male, n = 9 female; median age: 55 years, range: 25–91 years) with posteriorly dislocated subcapital fractures, of which 17 presented with a 5GL (G = greater tuberosity affected, L = lower tuberosity affected) type fracture (Figs. 2 and 3c, d), and two with a 5G type fracture, according to the Resch classification [37].

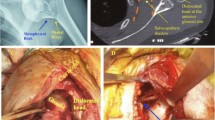
A 68-year-old patient with bilateral posterior humeral dislocation fracture after convulsive seizure. Right side, impression type fracture (reverse Hill–Sachs lesion): preoperative radiograph (a), computed tomography scan (b), 3D volume rendering technique (c)

A 68-year-old patient with bilateral posterior humeral dislocation fracture after convulsive seizure. Preoperative computed tomography scans of right shoulder, subcapital fracture, Resch 5GL: sagittal view (a), axial view (b)

A 68-year-old patient with bilateral posterior humeral dislocation fracture after convulsive seizure. Intraoperative findings: a, b right humeral head with impression type fracture with significant reverse Hill–Sachs lesion; c, d left humeral head with subcapital fracture, 5GL
All patients had conventional radiographs taken of the affected shoulder in anteroposterior and y‑views and/or axillary view. Furthermore, all fractures were evaluated with additional CT scans of the affected shoulder. On average, operative treatment for subcapital fractures was performed 5 days (range: 0–21 days) after completion of diagnostics, and after 6 days (range: 1–20 days) for the impression type fractures. Patients were treated with open surgery via a deltopectoral approach.
Five of the impression type fractures were treated prosthetically (n = 2 Hemicap implant, n = 3 reverse shoulder replacement, average age: 40 years), while the other 17 impression type fractures were treated with a humeral-head preserving reconstruction (77%, average age: 68 years; Fig. 4a, b). Those patients who were treated with an arthroplasty were significantly older than patients receiving a humeral head-preserving therapy (mean age 68 vs. 42 years; p = 0.0004). In 15 of these 17 cases (88%), this was achieved by a combination approach of initial reconstruction of the bony lesion and filling of the defect with an allo- and/or autograft (n = 9 allograft, n = 1 autograft, n = 5 auto- + allograft) and subsequent fixation of the fragment with plate or screw fixation. Two patients (11%) were treated with sole plate or screw fixation without an allo- or autograft, and in another four cases (19%), the bony lesion was filled by an allo- or autograft without a plate or screw osteosynthesis. Bio-compression screws were used in five surgeries. The defect size of the RHSL had a gamma angle of 105° (range: 90°–135°) on average (average alpha angle = 75° [range: 45°–120°], average beta angle = 30° [range: −20°–70°]). The average duration of surgery for the impression type fractures was 98 min.

A 68-year-old patient with bilateral posterior humeral dislocation fracture after convulsive seizure. Initial postoperative radiographs: a (anteroposterior), b (y-view) right shoulder: status after arthroplasty (LIMA SMR); c (anteroposterior), d (y-view) left shoulder: status after PHILOS plate osteosynthesis, autograft, allograft
The 19 patients with subcapital dislocation fractures were either treated with open reduction and internal fixation with a PHILOS plate (n = 13, 68%, average age, 48 years) or with arthroplasty (n = 5 reverse shoulder replacement, n = 1 anatomical hemi-arthroplasty; 32%, average age, 71 years; Fig. 4c, d). Similar to the impression type fracture group, the patients with a subcapital fracture who were treated with an arthroplasty were significantly older than those patients treated with plate osteosynthesis (mean age 71 years versus 48 years; p = 0.011). Among the 13 cases with PHILOS plating, six patients (55%) also required an allo- and/or autograft for the bony lesion of the humerus. In total, 63% of fractures presented with a head-split fracture. The average duration of surgery for the subcapital fractures was 148 min.
All surgeries were performed by experienced surgeons (n = 29 by a consultant [71%], n = 12 by the head of trauma surgery [29%]). Of the patients, 60% (22/37 patients) had follow-up appointments at the out-patient clinics after dismissal and were clinically and radiographically evaluated. On average, the last follow-up appointment took place 37 weeks after surgery (range: 1–241 weeks). At these appointments, the last documented ROM for surgically treated affected shoulders with impression type fractures had an average external rotation of 36° (range: 20–60°), abduction of 118° (range: 65–180°), and forward flexion of 116° (range: 35–180°). The last documented ROM for affected shoulders with subcapital fractures was 42° (range: 30–70°) in external rotation, 77° (range: 30–160°) in abduction, and 85° (range: 20–160°) in forward flexion on average.
In contrast, for all patients who received an arthroplasty, a mean external rotation of 35°, abduction of 80°, and forward flexion of 85° was observed.
There were no complications that emerged during the postoperative stay on the ward. Most patients showed no signs of secondary displacement, failure of the implants, or need for further surgery (16 out of 22 follow-up patients, 73%; Fig. 5). The mean follow-up period regarding revision surgeries was 4.3 (1–9) years. In four cases (11%), the patients underwent an elective arthroscopic removal of metal implants and arthrolysis of the shoulder joint. Two patients (5%) required revision surgery because of non-implant-related, biologic complications. One of these patients presented with a loss of reduction 6 months postoperatively, while the other patient was diagnosed with a humeral head necrosis 22 months after primary surgery. With the first patient, the implants were removed and a corrective osteotomy via re-osteosynthesis with a PHILOS plate and autograft was performed. The second patient received an arthroplasty after removal of the implants.

A 68-year-old patient with bilateral posterior humeral dislocation fracture after convulsive seizure. Radiographs 9 months after surgery: a (anteroposterior), b (y-view) right shoulder, no secondary dislocations; c (anteroposterior), d (y-view) left shoulder, no secondary dislocations
Discussion
The analysis of our databases revealed four major findings. First, regarding the morphology of the fractures in the cases that we identified, there was a relatively even distribution between impression type fractures (54%) and fractures with a subcapital component (46%). Second, in 73% of the cases, the humeral head was preserved. Third, there was a significant difference in age distribution between those patients treated with arthroplasty and those receiving a humeral head-preserving surgery. Finally, convulsive seizures and electrical accidents were more likely to lead to a posterior humeral dislocation fracture of the impression type (50% of impression type fractures) than to a subcapital fracture (37%) when compared with the fractures caused by a fall on the shoulder or a high-energy trauma.
When discussing surgical treatment, there are several factors to take into account. There is no definitive treatment guideline for these lesions because of their scarcity. As these fractures are frequently overlooked, the time frame becomes an important factor in deciding on surgical treatment. The time frame also plays a key role in determining whether closed reduction is an option for initial reduction because fractures that have been dislocated for more than 48 h may not be good candidates for closed reduction. Hawkins et al. reported that the average time between trauma and diagnosis was 1 year in their study [12]. While we also identified fractures that were not initially diagnosed or overlooked, most fractures were diagnosed and operated on within 1 week of the injury (n = 29, 71%).
Schnetzke et al. investigated the rate of avascular necrosis (AVN) of the humeral head after proximal humerus fracture dislocations [38]. After evaluating 30 patients with dislocation fractures of the proximal humerus, they observed symptomatic AVN in 33% of their patients, with a fivefold increased relative risk (RR) for AVN in patients who underwent late surgery (>48 h after trauma). Accordingly, their conclusion is that early surgery within 48 h of trauma significantly decreases the risk of AVN. In our study, 47% of patients (n = 9) with a subcapital fracture were treated within 48 h of trauma, while only 18% (n = 4) of patients with an impression type fracture underwent surgery within that same time frame. The difference can be partially explained by the late onset of diagnosis of the impression type fractures [15].
Impression type fractures (RHSL)
One of the main factors in deciding on the appropriate surgical treatment is the defect size, since a large humeral head defect creates instability of the joint (Fig. 3a, b).
For the impression type fractures, there are three options for surgical treatment. First there is anatomical reduction, which involves elevating the defect of the humerus and filling the bony defect with autologous bone or allogeneic bone material [16]. Second, if elevation of the bony defect is not successful, there are non-anatomical treatment options such as the McLaughlin procedure [39]. Schliemann et al. described an algorithm to choose the appropriate surgical treatment [15]. The algorithm focuses on the humeral defect size [40]. They recommend treating a fracture with a defect size under 45% with an open reduction and an anatomic reconstruction via bone graft, allograft, McLaughlin procedure, or a transfer of the minor tuberosity. Similarly, Kowalsky et al. recommend open reduction in patients with a humeral head defect of more than 20–25% of the articular surface [18]. Schliemann et al. suggest treating an impression fracture with a defect size greater than 45% with arthroplasty, the third surgical option for these impression type fractures [15].
The different surgical techniques appear to be good treatment options when treating an impression type fracture, as several case reports claim [28, 41]. Nevertheless, the surgical approach is still a matter of debate. In our study, we most commonly used a technique that is similarly used in the surgical approach of tibial plateau fractures with depression of the tibial joint surface. In most cases (n = 16, 73%), the reduction was performed by elevating the impressed humeral surface and filling the bony defect with an allo- or autograft. If an autograft was performed, trabecular bone was obtained from the ipsilateral iliac crest or from the site of surgery (n = 8, 50%). For the allograft, trabecular bone material, e.g., Tutoplast (RTI surgical, Marquette, MI, USA), was used. These techniques were also described in several case reports as surgical approaches for the impression type fracture with a prominent RHSL lesion [4, 42, 43].
To evaluate the characteristics of the defect size in relation to the proximal humerus, the alpha, beta, and gamma angles were measured according to the method described by Moroder et al. [36]. The average gamma angle was 105° (range: 90°–135°). In the aforementioned study, Moroder et al. calculated the critical gamma angle value at approximately 90°, at which point the humeral defect is susceptible to engagement with the posterior glenoid rim and therefore requires surgical treatment. Our results support this argument, as the average measured gamma angle was 105°, and all measured gamma angles were 90° or higher. Similarly, Knierzinger et al. reported five patients with an RHSL with gamma angles between 84.6° and 141.7° who were treated surgically by segment reconstruction via allo- or autograft [44]. The range of beta angles between −20° and 70° demonstrates the variability in location of the RHSL, but the relatively small average beta angle of 30° underlines that in most cases the RHSL can be found in close proximity to the bicipital groove of the long head of the biceps, which is located at 0°.
Posterior subcapital dislocation fractures and arthroplasty
In the impression type fracture group as well as in the group of fractures with a subcapital element, there was a significant difference in age distribution (p < 0.05). This is reflected in the general recommendation to treat multifragmentary proximal humeral fractures in patients over the age of 70, who also have an insufficient rotator cuff, fatty degeneration of the rotator cuff, and/or poor bone quality, with an arthroplasty [45, 46]. Where anatomical reduction and rigid fixation could be accomplished, some authors reported satisfactory results [25]. Similarly, a few retrospective case studies showed that the use of open reduction and internal fixation was associated with a relatively low risk of postoperative complications, and the functional outcome was generally favorable [3, 47].
While patient age is an important factor in deciding to opt for arthroplasty, there are other factors to indicate its use. Robinson et al. recommend arthroplasty in valgus impacted four-part dislocation fractures in the elderly, dislocated multifragmentary fractures with a completely isolated humeral head fragment and therefore high risk of humeral head necrosis, as well as fractures with a distinct valgus malposition and wide dislocation on the medial hinge [48]. In our study, 36% of patients treated with an arthroplasty were under the age of 70. In these cases, the decision to treat via arthroplasty was not based on age, but instead was due to a large humeral head defect size in the impression type fractures (>45%) or due to a multifragmentary subcapital dislocation fracture with the aforementioned features. Wooten et al. compared the results of arthroplasty for posterior humeral dislocation fractures with arthroplasty for treatment of glenohumeral osteoarthritis and found that, while the arthroplasty provided pain relief, improved shoulder external rotation, and had a low risk of recurrent instability, the overall rate of satisfaction was inferior [32]. The results of this study support that argument. While patients with a subcapital fracture who were treated with a plate fixation showed an average of 86° in abduction and 95° in forward flexion, patients treated via arthroplasty presented with an inferior ROM of 55° in abduction and 50° in forward flexion. This underlines the complexity of posterior dislocation fractures. Another case study found that total shoulder arthroplasty reliably decreased the patients’ level of pain, improved their ROM, and significantly improved their level of function, and therefore reported positive results [29]. One study reported acceptable outcomes with surgical treatment for two-part lesser tuberosity fractures with locked posterior shoulder dislocations [47]. Ide et al. even found excellent functional results in a case report at an 11-year follow-up, and radiographic and magnetic resonance imaging (MRI) investigations revealed the absence of avascular necrosis of the humeral head [49].
In summary, there are few and mixed results regarding treatment via arthroplasty of the posterior humeral dislocation fracture and further studies are necessary to investigate the functional outcome of these patients.
Limitations
The retrospective character is the biggest limitation to this study, as it is solely based on a retrospective analysis of two clinical databases. Such retrospective analysis of patient records does not provide information regarding functional outcome. The ROM values were recorded for only 60% of patients (22 out of 37), and of those, complete ROM evaluations were only available for 15 patients (42%). Accordingly, the final functional and radiographic outcomes remain unclear in most cases, such that clear treatment implications cannot be derived from the present study. Furthermore, the rate of complications might be higher than the databases suggest. Therefore, further investigations are planned in order to develop treatment algorithms for these fractures.
Practical conclusion
-
Impression type fractures were slightly more common than posteriorly dislocated proximal humeral fractures with a subcapital fracture component.
-
In 73% of the shoulders (n = 30), a humeral head-preserving reconstruction was performed.
-
Longer term functional outcomes of the patients should be obtained to better evaluate the treatment concept.
References
Zacchilli MA, Owens BD (2010) Epidemiology of shoulder dislocations presenting to emergency departments in the United States. J Bone Joint Surg Am 92(3):542–549. https://doi.org/10.2106/JBJS.I.00450
Alkaduhimi H, van der Linde JA, Flipsen M, van Deurzen DFP, van den Bekerom MPJ (2016) A systematic and technical guide on how to reduce a shoulder dislocation. Turk J Emerg Med 16(4):155–168. https://doi.org/10.1016/j.tjem.2016.09.008
Robinson CM, Akhtar A, Mitchell M, Beavis C (2007) Complex posterior fracture dislocation of the shoulder. Epidemiology, injury patterns, and results of operative treatment. J Bone Joint Surg Am 89:1454–1466
Bock P, Kluger R, Hintermann B (2007) Anatomical reconstruction for Reverse Hill-Sachs lesions after posterior locked shoulder dislocation fracture: a case series of six patients. Arch Orthop Trauma Surg 127:543–548
Brackstone M, Patterson SD, Kertesz A (2001) Triple “E” syndrome: bilateral locked posterior fracture dislocation of the shoulders. Neurology 56(10):1403–1404. https://doi.org/10.1212/WNL.56.10.1403
Pushpakumara J, Sivathiran S, Roshan L, Gunatilake S (2015) Bilateral posterior fracture-dislocation of the shoulders following epileptic seizures: a case report and review of the literature. BMC Res Notes. https://doi.org/10.1186/s13104-015-1674-y
Mouzopoulos G (2010) The “Mouzopoulos” sign: a radiographic sign of posterior shoulder dislocation. Emerg Radiol 17:317–320
Robinson CM, Aderinto J (2005) Posterior shoulder dislocations and fracture dislocations. J Bone Joint Surg Am 87:639–650
Mastrokalos DS, Panagopoulos GN, Galanopoulos IP, Papagelopoulos PJ (2017) Posterior shoulder dislocation with a reverse Hill-Sachs lesion treated with frozen femoral head bone allograft combined with osteochondral autograft transfer. Knee Surg Sports Traumatol Arthrosc 25:3285–3288
Lill H, Scheibel M, Voigt C (eds) (2014) Die proximale Humerusfraktur. Springer, Berlin, Heidelberg, pp 1–237 https://doi.org/10.1007/978-3-642-35257-7
Moroder P, Runer A et al (2015) Influence of defect size and localization on the engagement of reverse Hill-Sachs lesions. Am J Sports Med 43(3):542–548. https://doi.org/10.1177/0363546514561747
Hawkins RJ, Neer CS 2nd, Pianta RM, Mendoza FX (1987) Locked posterior dislocation of the shoulder. J Bone Joint Surg Am 69:9–18
Neer CS 2nd (1970) Displaced proximal humeral fractures. II. Treatment of three-part and four-part displacement. J Bone Joint Surg Am 52:1090–1103
de Oliveira CTB, da Graça E, Fanelli VA (2018) Posterior four-part fracture-dislocations of the proximal humerus: clinical and functional evaluation of osteosynthesis treatment. Rev Bras Ortop 53(3):350–356. https://doi.org/10.1016/j.rboe.2018.03.010
Schliemann B, Muder D, Gessmann J, Schildhauer TA, Seybold D (2011) Locked posterior shoulder dislocation: treatment options and clinical outcomes. Arch Orthop Trauma Surg 131:1127–1134
Diklic ID, Ganic ZD, Blagojevic ZD, Nho SJ, Romeo AA (2010) Treatment of locked chronic posterior dislocation of the shoulder by reconstruction of the defect in the humeral head with an allograft. J Bone Joint Surg Br 92:71–76
Robinson CM, Seah M, Akhtar MA (2011) The epidemiology, risk of recurrence, and functional outcome after an acute traumatic posterior dislocation of the shoulder. J Bone Joint Surg Am 93:1605–1613
Kowalsky MS, Levine WN (2008) Traumatic posterior glenohumeral dislocation: classification, pathoanatomy, diagnosis, and treatment. Orthop Clin North Am 39(4):519–533. https://doi.org/10.1016/j.ocl.2008.05.008
Gosens T, Poels PJE, Rondhuis JJ (2000) Posterior dislocation fractures of the shoulder in seizure disorders—two case reports and a review of literature. Seizure 9(6):446–448. https://doi.org/10.1053/seiz.2000.0418
Claro R, Sousa R, Massada M, Ramos J, Lourenço JM (2009) Bilateral posterior fracture-dislocation of the shoulder: report of two cases. Int J Shoulder Surg 3(2):415
Godenèche A, Freychet B, Gunst S, Daggett M, Viste A, Walch G (2017) Arthroscopic reduction of acute traumatic posterior glenohumeral dislocation and anatomic neck fracture without internal fixation: 2‑year follow-up. Orthop J Sports Med 5(12):2325967117745486. https://doi.org/10.1177/2325967117745486
Iannotti JP, Williams GR Jr., Miniaci A, Zuckerman JD (2013) Disorders of the shoulder: diagnosis and management package. Lippincott Williams & Wilkins, Philadelphia, PA, USA
Spross C, Platz A, Erschbamer M, Lattmann T, Dietrich M (2011) Surgical treatment of Neer group VI proximal humeral fractures: retrospective comparison of PHILOS® and Hemiarthroplasty. Clin Orthop Relat Res 470(7):2035–2042. https://doi.org/10.1007/s11999-011-2207-1
Rouleau DM, Hebert-Davies J (2012) Incidence of associated injury in posterior shoulder dislocation: systematic review of the literature. J Orthop Trauma. https://doi.org/10.1097/BOT.0b013e3182243909
Soliman OA, Koptan WM (2013) Four-part fracture dislocations of the proximal humerus in young adults: results of fixation. Injury 44:442–447
Jacquot F, Costil V, Werther JR et al (2013) Balloon treatment of posterior shoulder dislocation with reverse Hill-Sachs injury: description of a new technique. Int Orthop 37:1291–1295
Kokkalis ZT, Mavrogenis AF, Ballas EG, Papanastasiou J, Papagelopoulos PJ (2013) Modified McLaughlin technique for neglected locked posterior dislocation of the shoulder. Orthopedics 36:e912–e916
Martinez AA, Navarro E, Iglesias D et al (2013) Long-term follow-up of allograft reconstruction of segmental defects of the humeral head associated with posterior dislocation of the shoulder. Injury 44:488–491
Cheng SL, Mackay MB, Richards RR (1997) Treatment of locked posterior fracture dislocations of the shoulder by total shoulder arthroplasty. J Shoulder Elbow Surg 6:11–17
Konda SR, Fisher N, Gage M, Egol KA (2017) Posterior fracture dislocation of the shoulder: a modified mcLaughlin procedure. J Orthop Trauma 31:S36–S37
Fiorentino G, Cepparulo R et al (2016) Posterior shoulder fracture-dislocation: double approach treatment. Our experience. Acta Biomed 87(2):184–190
Wooten C, Klika B et al (2014) Anatomic shoulder arthroplasty as treatment for locked posterior dislocation of the shoulder. J Bone Joint Surg 96(3):e19. https://doi.org/10.2106/JBJS.L.01588
De Wall M, Lervick G, Marsh JL (2005) Posterior fracture-dislocation of the proximal humerus: treatment by closed reduction and limited fixation: a report of four cases. J Orthop Trauma 19:48–51
Kaar TK, Wirth MA, Rockwood CA Jr. (1999) Missed posterior fracture-dislocation of the humeral head. A case report with a fifteen-year follow-up after delayed open reduction and internal fixation. J Bone Joint Surg Am 81(5):708–710
Gokkus K, Sagtas E, Kara H, Aydin AT (2018) Posterior shoulder dislocation associated with the head (splitting) and humeral neck fracture: impact of understanding radiologic signs and experience with an extended Deltopectoral approach. Tech Hand Up Extrem Surg 22(2):57–64. https://doi.org/10.1097/BTH.0000000000000190
Moroder P, Runer A, Kraemer M, Fierlbeck J, Niederberger A, Cotofana S, Resch H et al (2015) Influence of Defect Size and Localization on the Engagement of Reverse Hill-Sachs Lesions. Am J Sports Med 43(3):542–548. https://doi.org/10.1177/0363546514561747
Resch H, Tauber M, Neviaser RJ, Neviaser AS, Majed A, Halsey T, Hirzinger C, Al-Yassari G, Zyto K, Moroder P (2016) Classification of proximal humeral fractures based on a pathomorphologic analysis. J Shoulder Elbow Surg 25(3):455–462. https://doi.org/10.1016/j.jse.2015.08.006
Schnetzke M, Bockmeyer J, Loew M, Studier-Fischer S, Grützner P‑A, Guehring T (2018) Rate of avascular necrosis after fracture dislocations of the proximal humerus. Obere Extremität 13:273. https://doi.org/10.1007/s11678-018-0452-6
McLaughlin HL (1952) Posterior dislocation of the shoulder. J Bone Joint Surg Am 24A(3):584–590
Schliemann B, Schildhauer TA, Seybold D (2010) Die dorsal verhakte Schulterluxation; Diagnostik und Behandlungsstrategien. Obere Extremität 5. https://doi.org/10.1007/s11678-010-0092-y
Walch G, Boileau P, Martin B, Dejour H (1990) Unreduced posterior luxations and fractures-luxations of the shoulder. Apropos of 30 cases. Rev Chir Orthop Reparatrice Appar Mot 76(8):546–558
Khayal T, Wild M, Windolf J (2009) Reconstruction of the articular surface of the humeral head after locked posterior shoulder dislocation: a case report. Arch Orthop Trauma Surg 129:515. https://doi.org/10.1007/s00402-008-0762-z
Rodia F, Ventura A, Touloupakis G, Theodorakis E, Ceretti M (2012) Missed posterior shoulder dislocation and McLaughlin lesion after an electrocution accident. Chin J Traumatol 15(6):376–378. https://doi.org/10.3760/cma.j.issn.1008-1275.2012.06.014
Knierzinger D, Euler SA, Hengg C et al (2017) Obere Extremität 12:96. https://doi.org/10.1007/s11678-017-0405-5
Gallinet D, Clappaz P, Garbuio P, Tropet Y, Obert L (2009) Three or four parts complex proximal humerus fractures: hemiarthroplasty versus reverse prosthesis: a comparative study of 40 cases. Orthop Traumatol Surg Res 95(1):48–55. https://doi.org/10.1016/j.otsr.2008.09.002
Ogawa K, Yoshida A, Inokuchi W (1999) Posterior shoulder dislocation associated with fracture of the humeral anatomic neck: treatment guidelines and long-term outcome. Trauma Injury Infect Crit Care 46(2):318–323
Liu X, Zhu Y, Lu Y, Li F, Wu G, Jiang C (2015) Locked posterior shoulder dislocation associated with isolated fractures of the lesser tuberosity: a clinical study of 22 cases with a minimum of 2‑year follow-up. J Orthop Trauma 29(6):271–275. https://doi.org/10.1097/BOT.0000000000000276
Robinson CM, Amin AK, Godley KC, Murray IR, White TO (2011) Modern perspectives of open reduction and plate fixation of proximal humerus fractures. J Orthop Trauma 25(10):618–629. https://doi.org/10.1097/BOT.0b013e31821c0a2
Ide J, Honda K, Takagi K (2003) Posterior dislocation of the shoulder associated with fracture of the humeral anatomical neck with 11-year follow-up after early open reduction and internal fixation. Arch Orthop Trauma Surg 123(2–3):118–120
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
J. C. Katthagen is an advisor for Arthrex GmbH. M.J. Raschke is a consultant for DePuy Synthes. H. Lill is a consultant for DePuy Synthes and Arthrex GmbH. L.F. Heilmann, B. Schliemann, H. El Bajjati, G. Jensen, and R.-O. Dey-Hazra declare that they have no competing interests.
All procedures performed in studies involving human participants or on human tissue were in accordance with the ethical standards of the institutional and/or national research committee and with the 1975 Helsinki declaration and its later amendments or comparable ethical standards. A positive vote by the ethics committee was given for performing this study.
Rights and permissions
Open Access. This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Heilmann, L.F., Katthagen, J.C., Raschke, M.J. et al. Posterior fracture dislocation of the proximal humerus. Obere Extremität 14, 110–117 (2019). https://doi.org/10.1007/s11678-019-0522-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11678-019-0522-4
Keywords
- Shoulder
- Impression type fracture of the humerus
- Reverse Hill–Sachs lesion
- Subcapital fracture of the humerus
- Posterior shoulder dislocation