
Abstract
Background
The problem of loneliness has garnered increased attention from policymakers, payors, and providers due to higher rates during the pandemic, particularly among seniors. Prior systematic reviews have in general not been able to reach conclusions about effectiveness of interventions.
Methods
Computerized databases were searched using broad terms such as “loneliness” or “lonely” or “social isolation” or “social support” from Jan 1, 2011 to June 23, 2021. We reference mined existing systematic reviews for additional and older studies. The Social Interventions Research & Evaluation Network database and Google were searched for gray literature on Feb 4, 2022. Eligible studies were RCTs and observational studies of interventions to reduce loneliness in community-living adults that used a validated loneliness scale; studies from low- or middle-income countries were excluded, and studies were excluded if restricted to populations where all persons had the same disease (such as loneliness in persons with dementia).
Results
A total of 5971 titles were reviewed and 60 studies were included in the analysis, 36 RCTs and 24 observational studies. Eleven RCTs and 5 observational studies provided moderate certainty evidence that group-based treatment was associated with reduced loneliness (standardized mean difference for RCTs = − 0.27, 95% CI − 0.48, − 0.08). Five RCTs and 5 observational studies provided moderate certainty evidence that internet training was associated with reduced loneliness (standardized mean difference for RCTs = − 0.22, 95% CI − 0.30, − 0.14). Low certainty evidence suggested that group exercises may be associated with very small reductions in loneliness. Evidence was insufficient to reach conclusions about group-based activities, individual in-person interactions, internet-delivered interventions, and telephone-delivered interventions.
Discussion
Low-to-moderate certainty evidence exists that group-based treatments, internet training, and possibly group exercises are associated with modest reductions in loneliness in community-living older adults. These findings can inform the design of supplemental benefits and the implementation of evidence-based interventions to address loneliness.
Systematic Review Registration Number
PROSPERO (CRD42021272305)
Similar content being viewed by others

Avoid common mistakes on your manuscript.
INTRODUCTION
Loneliness is common in community-dwelling seniors, with clear evidence of increasing prevalence during the pandemic.1 Numerous studies have found strong associations between loneliness and health outcomes. For example, loneliness or social isolation is associated with a 29% increased risk of heart disease, a 32% increased risk of stroke, and a 50% increased risk of dementia.2 Beginning in 2019, the US Centers for Medicare and Medicaid Services (CMS) has allowed Medicare Advantage (MA) plans to target supplemental benefits to beneficiaries’ individual health needs, including more flexibility in the definition of “primarily health-related” and new “non-primarily health-related” benefits.3 MA supplemental benefits intended to directly or indirectly address loneliness include in-home support services, group fitness or social classes/memberships, adult day care services, transportation for non-medical needs, and other supports to increase autonomy or functional status.4
Evidence to guide which interventions to offer is needed. In recognition of these needs, the US National Academies of Sciences, Engineering, and Medicine (NASEM) released a report in 2020 about social isolation and loneliness in older adults.2 As part of this, the Committee reviewed the literature on interventions, citing 7 existing “large scale reviews”.5,6,7,8,9,10,11 From these and data from some individual studies, the Committee concluded that “a variety of interventions have been proposed….however there is not enough evidence to identify the most effective interventions”; and “many intervention studies do not use a validated tool.” Until recently prior systematic reviews have either been narrative,5,6,7,8,9, 11 or if meta-analytic have been very broad in population (for example, statistically combining studies of interventions for children in the third grade with interventions for older adults living in nursing homes),10 or narrowly focused on intervention, specifically computer and internet use or information and communication technology,12,13,14,15,16 or were a scoping review.17, 18 To address these limitations, our goal was to conduct a systematic review and meta-analysis of diverse interventions to reduce loneliness in a more homogeneous population, namely older community-living adults, with loneliness being measured with a validated measure.
METHODS
This review is reported using Preferred Reporting Items for Systematic Reviews and Meta-analyses criteria. The funder participated in setting the scope of the review and the interpretation of the results. The public was not involved.
Data Sources and Searches
Interventions to reduce loneliness have been the subject of numerous prior reviews. Therefore, we adopted a 3-phase search strategy: search the references (reference mine) in existing systematic reviews; new searches for published literature; and then gray literature searches. We started with the seven reviews5,6,7,8,9,10,11 cited in the NASEM report.2 To this, we added the rapid review by the US Agency for Healthcare Research and Quality,19 and six other systematic reviews identified on a preliminary search.12, 16, 20,21,22,23 We reference mined all these reviews. We then used articles contained in these reviews to construct a search strategy that would find more articles similarly indexed. We used this strategy to query Ovid Medline and the Cochrane Library from January 1, 2011, to June 23, 2021, using terms such as “loneliness or lonely or friendship or solitude or aloneness” or “social support or social isolation” (see eTable 1 for the full search strategy). To this, we then added a search of the Social Interventions Research & Evaluation Network (SIREN) database and 7 searches on Google for additional published and gray literature (searched on February 4, 2022). Finally, we searched for studies via reference mining which included original research studies and expert consultation, with no restriction on publication date.
Study Selection
Two authors (PGS and IML) independently screened titles, abstracts, and full texts, with disagreements reconciled through team discussion. Studies were initially eligible if they (1) were focused on community-living adults; (2) had an intervention whose intent was to reduce loneliness; and (3) reported loneliness outcomes. Later, we added an additional criterion, that the duration of follow-up had be greater than 4 weeks. Randomized and observational studies (but not cross-sectional or case-control studies) were included. Studies in children or adolescents were excluded. Since there is not a bright line for what constitutes “older” adults, we did not enforce an age threshold other than adults, but almost all studies were about adults older than age 50. Studies of adults living in nursing homes were excluded, but adults living independently in congregate living facilities were included. Studies where the target population were selected because of some particular health condition, such as blindness24 or dementia,25 were excluded because we judged that generalizing to other populations would be difficult. Due to the perceived importance of context in who is lonely and the availability of potential interventions to reduce the risk of loneliness, we excluded studies from low- and middle-income countries.26 We excluded studies that were not originally designed as interventions to reduce loneliness, such as a study of Meals On Wheels,27 because we judged these to be at high risk for selective outcome reporting. After performing the initial screening, and when considering the meta-analysis, we restricted eligibility to studies that used one of two validated loneliness scales described in the NASEM report as measuring essentially the same aspects of loneliness: the UCLA scale28 or the deJong Gierveld scale,29 which together accounted for about 84% of all studies reporting loneliness outcomes. We also included 2 articles that used outcome measures that provided evidence that they were correlated at least 70% with either the UCLA scale or the deJong Gierveld scale.30, 31 Lastly, we excluded 8 studies who met all the other eligibility criteria because they did not report quantitative data sufficient to be used in the meta-analysis (for example, a study only reported “no differences” in loneliness between the pre- and post-test evaluation).32
Data Extraction and Quality Assessment
Data elements extracted in duplicate included study design, intervention characteristics, population characteristics, and follow-up. We assessed whether enrolled populations were at increased risk of loneliness via selection due to life circumstance (such as bereavement) or by using a tool screening for loneliness. For risk of bias, we used the Cochrane Risk of Bias Tool,33 the Risk of Bias in Non-Randomized Studies of Interventions tool,34 or a modification of the NIH tool for Pre-Post studies.35 Data on outcomes were extracted by the statistician and checked by a second author.
Data Synthesis and Grading
There is no standard method for grouping interventions to reduce loneliness into categories sufficiently similar to support meta-analysis. Ideally, we would like interventions within a group to be identical, for example, the way pharmaceutical interventions can be considered to be identical. Unfortunately, since only two interventions were the subject of more than one study,36,37,38,39,40 this would result in four dozen different categories, nearly all with only a single study in it, and thus, no meta-analysis would be possible. The most common way of grouping studies in prior systematic reviews has been whether interventions were delivered via a “group” or “one-to-one.”18 We adopted this scheme in general, but additionally separated “group” interventions into those that included some kind of mental or cognitive treatment (such as “participatory group-based care management,”41 “group-based educational, cognitive, and social support,”42 or “discussions guided by Self-management of Well-being theory”43) versus those that involved only an activity (such as group-based dance, or singing in a chorus44) versus studies that were only group-based exercises (Tai Chi,45 aerobics,46 or a structured supervised exercise program).47 For “one-to-one” (which we call “individual in-person interactions”), we separated these into whether they were in-person, or delivered over the internet, or by telephone (see Fig. 1). We kept as its own category 10 studies of interventions that trained older adults in how to use the internet and/or social media. Lastly, there remained 8 studies of interventions that did not fit into any of the above categories, they being an eclectic mix such as volunteering as a foster grandparent, writing about one’s life experiences, or a computer-tailored intervention designed to stimulate cognitive function and increase physical activity.

Categories of loneliness interventions.
The majority of studies reported continuous outcomes so we report the results as standardized mean differences. We kept studies using a randomized design separate from observational studies. Each has its relative strengths and weaknesses in terms of internal validity and external generalizability. When sufficient studies existed (three or more) within each intervention and study design category, we pooled them using a random effects meta-analysis. We use the Hartung-Knapp-Sidik-Jonkman48,49,50,51 method for our random effects meta-analysis. This method has been preferred when the number of studies pooled is small and when there is evidence of heterogeneity.51 We used the I2 statistic52 to assess the level of heterogeneity. Egger’s regression asymmetry test53 and Begg’s rank correlation54 were used to examine publication bias. All analyses were conducted in R.4.0.2 using the metafor package.
We rated certainty of the evidence using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) system.55
RESULTS
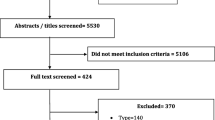
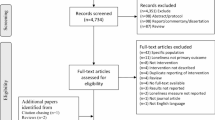
After screening 5971 titles and adding 175 full text articles from reference mining existing systematic reviews and 16 studies from our gray literature search, we identified 88 potentially eligible studies (see eFigure 1). After rejecting 14 studies because they did not use either the UCLA or the DeJong Gierveld loneliness scale56,57,58,59,60,61,62,63,64,65,66,67,68,69 or a scale shown to be highly correlated with either, five studies for short follow-up time,70,71,72,73,74 and a further eight studies because of insufficient data (see eTable 2),32, 75,76,77,78,79,80,81,82 and one study because we judged its 4% follow-up rate to be so low that no valid conclusions could be drawn,83 there were 60 full text articles that were included in our quantitative analysis (see eTable 3 for a list of excluded studies).
Description of the Evidence
Of the 60 studies, 36 were randomized trials and 24 were observational studies. All but four studies were either restricted to adults that were at least aged 50 or older or had a mean age that was over age 50.39, 40, 84, 85 Nineteen studies were done in the USA, twelve studies were done in the Netherlands, five studies were done in the UK, four studies each were done in Canada and Australia, and the remainder came from Israel, Spain, Sweden, Finland, Italy, Switzerland, Hong Kong, and Japan.
Risk of Bias Assessment
The assessments of the Cochrane Risk of Bias criteria for the randomized trials are in eTable 4 and of the Risk Of Bias in Non-randomized Studies of Interventions criteria in eTable 5; and the adaptation of the NIH tool is in eTable 6. These types of interventions are essentially impossible to blind, and the assessments reflect this. However, we did not place much weight on blinding when assessing a study’s limitations. Since studies were selected only if they were intended to reduce loneliness and used a validated scale, all studies were judged to be at low risk of bias for selective reporting and in measurement of the outcome. Thus, studies were discriminated primarily on design, and then on details of how subjects were selected and offered different treatments, the attrition rate, and the sample size.
Group-Based Treatment
We identified 16 studies of group-based treatment, 11 randomized trials41,42,43, 84, 86,87,88,89,90,91,92 and 5 observational studies.36,37,38, 93, 94 Twelve studies enrolled populations selected for increased risk of loneliness, and four studies had unselected populations. In all but one study enrollment criteria or the mean age of subjects was 50 years of age or older. The content of the treatment was heterogeneous across studies but was in general based on psychological theories or principles (such as cognitive behavioral therapy, mindfulness, participatory group-based care management, discussion topics that were “based on the social cohesion approach of social capital theory,” feminism, “re-evaluation counseling,” etc.) (see Table 1). In some interventions, there were also practical topics about day-to-day matters, like nutrition and food, and healthy aging. A few also included exercises (yoga, group exercises). What all interventions had in common was they involved bringing together small groups of subjects for regular group sessions, usually for 2–4 months in duration, and the sessions were in general led by a trained moderator. The random effects pooled estimate of effect for the 11 RCTs or the 5 observational studies both showed that there was less loneliness in the group-based treatment subjects (standardized mean difference of 11 RCTs: − 0.25 (95% confidence interval − 0.42, − 0.08); standardized mean difference of 5 observational studies: − 0.46 (95% confidence interval − 0.86, − 0.07)) (see Fig. 2). One test assessing the possibility of publication bias was statistically significant (Egger’s regression test for RCT pooled result = 0.01); however, Begg’s rank correlation test for the RCT result and neither test for the observational study results were statistically significant.

Forest plot of group-based interventions to reduce loneliness.
Group-Based Exercises
We identified 4 studies of group-based exercises, 1 RCT45 and 3 observational studies.46, 47, 95 All were of subjects unselected for increased risk of loneliness. All studies enrolled subjects who were 60 years or older or whose mean age was greater than 60. The exercises in these 4 studies consisted of Tai Chi, a “structured supervised exercise program,” a personalized plan and group sessions to sustain the plan, and aerobic exercises, stretching and toning (see Table 2). The one RCT reported less loneliness in the exercise group (standardized mean difference of − 0.52, 95% confidence interval − 1.20, 0.16). The random effects pooled estimate of effect for the 3 observational studies showed there was less loneliness in the exercise group (standardized mean difference − 0.13 (95% confidence interval − 0.28, 0.01)) (see Fig. 2). There was no evidence of publication bias.
Internet Training
We identified 10 studies of internet training, 5 randomized trials40, 96,97,98,99,100 and 5 observational studies.101,102,103,104,105 Only 1 study enrolled a population selected to be at increased risk of loneliness.97 In all studies, the subjects were restricted to or had a mean age of 60 years or older. In older studies, the training consisted of basic computer skills, internet use, email competency, etc. More recent studies included training regarding social media, photographs, and video chat applications. For studies with a concurrent comparison group, comparators received no intervention or activities other than internet training (like sewing or painting) or, in one study, a binder with the same printed content as in the training (see Table 3). The random effects pooled estimates of effect for the 5 RCTs and for the 5 observational studies showed less loneliness in the internet training group (standardized mean difference for 5 RCT studies = − 0.22 (95% confidence interval − 0.30, − 0.14); standardized mean difference for 5 observational studies = − 0.33 (95% confidence interval − 0.86, 0.21)) (see Fig. 3). There was no evidence of publication bias.

Forest plot of miscellaneous interventions to reduce loneliness.
Internet-Delivered Interventions
We identified 7 studies of internet-delivered interventions, all of which were RCTs.39, 40, 85, 106,107,108,109 Five of the seven studies enrolled populations selected to be at increased risk for loneliness. Four of the studies had mean ages of enrolled subjects less than 65 years.39, 40, 85, 106 Three studies assessed internet-delivered cognitive behavioral therapy (CBT);39, 40, 106 the remainder had content unique to the study (see eTable 7). The random effects pooled estimate of effect for the 7 RCTs (using the CBT arm of the study by Kall 2021 as the intervention) showed less loneliness in the intervention groups (standardized mean difference = − 0.27 (95% CI − 0.53, − 0.01)). There was no evidence of publication bias. The point estimates of effect for the 3 RCTs of CBT were higher than the point estimates for any of the other internet-delivered interventions.
Results for Other Interventions, Head-to-Head Studies, and Sensitivity Analyses
Other interventions
Six studies of individual in-person interactions110,111,112,113,114,115, 4 studies of telephone-based interventions (all 4 of which were individual one-on-one, one study also included group phone calls),30,116,117,118 and 8 studies unable to be classified with any of the other groups119,120,121,122,123,124,125,126 provided signals that they may have associations with less loneliness, but individually and meta-analytically their results were not as strong as the four interventions discussed in detail. One RCT31 and four observational studies44,127,128,129 of group activities provided no evidence of an effect on loneliness. See Figs. 2 and 3, and eTables 8–11 for additional details of these studies.
Head-to-head studies
We identified one study that compared different interventions for loneliness. This study randomized 170 lonely adults with mean age of 47.5 years, and of whom, 76% were women to either internet-delivered cognitive behavioral therapy (iCBT) or interpersonal psychotherapy (iIPT) or a wait-list control. At 4 months, with 61 subjects lost to follow-up, there was a greater reduction in loneliness as measured by the UCLA scale for subjects treated with iCBT than with iIPT.39
Assessing for effect modifiers
An attempt at meta-regression to assess the potential for effect modification due to selection of subjects at increased risk of loneliness was not possible due to very strong correlations between type of intervention and such selection.
Studies excluded due to outcome measure
We did not include 14 studies in our analysis due to their outcomes measure being something other than the UCLA loneliness scale or the deJong Gierveld loneliness scale. Eight of these studies used outcome measures that were dichotomous (e.g., “Are you lonely?”) or categorical,60,61,62,63,64,65, 67, 69 for which we were able to calculate an odds ratio for six.60,61,62, 64, 67, 69 This included one study that used the deJong Gierveld scale but then analyzed it as a dichotomous outcome.67 The remaining six studies56,57,58,59, 66, 68 used scales for which we calculated an SMD. Appendix eTable 12 gives details about these studies and shows forest plots of loneliness outcomes, by the type of intervention. Inclusion of any of these studies would not materially change any of our conclusions.
Certainty of Evidence
We judged the certainty of evidence that group-based treatment is associated with lower levels of loneliness as moderate, reduced from high due to serious inconsistency. We judged the certainty of evidence that internet training is associated with lower levels of loneliness as moderate, again reduced from high due to serious inconsistency. While we did not consider the observational study evidence in either case when assessing the certainty of evidence using GRADE, in both cases, we considered the agreement in pooled results between data from RCTs and from observational studies to strengthen the conclusion. We judged the evidence that group-based exercise therapy is associated with lower levels of loneliness as low, reduced due to serious concerns about study risk of bias and serious imprecision (eTable 13). Although the pooled estimate of effect for internet-delivered interventions was similar to the pooled estimate of effect for the above interventions, we judged the certainty of evidence as very low due to increased heterogeneity in the content of interventions and increased indirectness in the population. All other potential associations are judged as being very low certainty.
DISCUSSION
The principal finding of this systematic review is that there are interventions associated with lower levels of loneliness in community-living older adults, in specific group-based treatment and internet/social media training. Group-based exercises may possibly also be associated with lower levels of loneliness. The effect size for association for any of these interventions is modest, using standard yardsticks to assess the meaning of an effect size. Nevertheless, to put this in perspective, the size of this effect on loneliness is roughly similar to the lower end of pooled estimates of the effect of oral antidiabetic agents on hemoglobin A1c levels,130 which is not an effect that is clinically insignificant.
Strengths of our review are that we included more RCTs and more studies in general than prior reviews, the classification of interventions into categories based on content and delivery, and the comparison and contrast of results from RCTs with results from observational studies, which tend to support each other. The key limitations to this review are that we may not have identified all of the relevant evidence, and residual heterogeneity among the evidence we did find. Regarding the former point, any potentially eligible studies we missed must in turn have been missed by all systematic reviews we reference mined and missed by the 2020 National Academies of Sciences, Engineering, and Medicine report, and missed by the recent comprehensive review by Hoang and colleagues.131 Unpublished studies also fall within the category of missing evidence, and while we did not find definitive evidence of the presence of publication bias, the statistical tests for it are known to be underpowered and so we always assume that some unpublished studies must exist. Their effect on our results is speculative. Furthermore, it is likely that as a result of the pandemic more loneliness research has been recently published and will be published in the future. Regarding residual heterogeneity, there is certainly heterogeneity among included studies within our intervention categories—without tolerating some heterogeneity, no pooled analysis would have been possible. We grouped studies using variables similar to those used by other review authors,18 but acknowledge that within a single intervention category, such as group-based treatment, there are potential differences in effectiveness between interventions. Whether differences in individual study outcomes are due to differences in the content of their group treatment, or difference in the populations studied, or just randomness, is impossible at this point to tell. Nevertheless, the demonstration that across a possibly heterogeneous collection of group-based treatment studies there is a significant association with less loneliness should provide the impetus for more precise studies trying to identify the most effective components and how this may differ between different populations, what dosage is most effective, and for how long it may last.
Our results go beyond and extend the findings of prior systematic reviews and the conclusions of the NASEM report. In general, prior reviews have been unable to reach conclusions about effectiveness, being narrative and citing the paucity and methodologic limitations of the primary studies, with the concomitant call for more and better research. The NASEM report mirrored these conclusions. Recently, as our review process was being completed, there was published another review of interventions for loneliness in older adults. While there are some similarities between the review by Hoang and colleagues131 and our review—for example, both are focused on older adults, both have meta-analytic results for community-living subjects—there are also important differences (see eTable 14). While in the review by Hoang and colleagues all their conclusions were judged as very low certainty evidence, such was not the case in our review.
We may speculate about why some interventions seemed to be more effective than others. While acknowledging that there are no head-to-head trials to prove the superiority of one class of interventions over another, our results suggest the framing of the intervention matters, possibly as a mechanism to reduce the stress, hypervigilance, and vulnerability experienced by states of loneliness.132 Group treatments may be more effective than group activities like exercise because in the former people are forced by the treatment itself to verbally interact with their fellow subjects and may find the concept of a treatment more reassuring than an activity. In group activities, a person could engage less fully, and the perceptions of vulnerability that created the subjective experience of loneliness may create additional barriers to full participation. Internet training may work better than internet-delivered therapies because internet training fosters more agency among lonely patients, as well as facilitating engagement in social media and self-directed learning as compared with an internet therapy that feels more scripted and more like “work.” Again, the framing of the intervention may enhance engagement and deeper participation, the former engenders more enthusiasm while the latter may feel like a chore.
These findings have important implications for payors, providers, and policymakers. For policymakers, these results reaffirm the importance of flexibility in offering programs (either as benefits or directly provided) to address health-related social needs such as loneliness. While further research is needed to assess the relationship between interventions to improve loneliness and health outcomes (such as mental or physical health) or costs, these findings underscore the promise in these interventions to address the underlying social need. Additional studies are needed to better understand whether specific interventions are more effective in certain population subgroups, such as those at increased risk of loneliness, which will improve overall effectiveness of these efforts.
CONCLUSIONS
This systematic review and meta-analysis found moderate certainty evidence that two types of interventions—group-based treatment and training to use the internet (including social media) are associated with lower levels of loneliness in populations that are mainly community-living older adults. These findings can inform the design of supplemental benefits or programs and the implementation of evidence-based interventions to address loneliness.
Data Availability
All data used in the analysis are presented in the article or the supplemental material.
References
O'Sullivan R, Burns A, Leavey G, et al. Impact of the COVID-19 pandemic on loneliness and social isolation: a multi-country study. Int J Environ Res Public Health. 2021;18(19):9982.
National Academies of Sciences, Engineering, and Medicine. Social Isolation and Loneliness in Older Adults: Opportunities for the Health Care System. Washington, DC: The National Academies Press; 2020.
Implementing Supplemental Benefits for Chronically Ill Enrollees. 2019. https://www.cms.gov/Medicare/Health-Plans/HealthPlansGenInfo/Downloads/Supplemental_Benefits_Chronically_Ill_HPMS_042419.pdf
Kornfield T, Kazan M, Frieder M, Duddy-Tenbrunsel R, Donthi S, Fix A. Medicare advantage plans offering expanded supplemental benefits: a look at availability and enrollment. Available at: https://www.commonwealthfund.org/publications/issue-briefs/2021/feb/medicare-advantage-plans-supplementalbenefits. Accessed October 4, 2023.
Gardiner C, Geldenhuys G, Gott M. Interventions to reduce social isolation and loneliness among older people: an integrative review. Health Soc Care Commun. 2018;26(2):147-157. https://doi.org/10.1111/hsc.12367.
Cohen-Mansfield J, Perach R. Interventions for alleviating loneliness among older persons: a critical review. Am J Health Promot AJHP. 2015;29(3):e109-25. https://doi.org/10.4278/ajhp.130418-LIT-182.
Findlay RA. Interventions to reduce social isolation amongst older people: where is the evidence?. Ageing Soc. 2003;23(5):647–658.
Cattan M, White M, Bond J, Learmouth A. Preventing social isolation and loneliness among older people: A systematic review of health promotion interventions. Ageing Soc. 2005;25(1):41–67.
Dickens AP, Richards SH, Greaves CJ, Campbell JL. Interventions targeting social isolation in older people: a systematic review. BMC Public Health. 2011;11:647.
Masi CM, Chen HY, Hawkley LC, Cacioppo JT. A meta-analysis of interventions to reduce loneliness. Pers Soc Psychol Rev. 2011;15(3):219-66. https://doi.org/10.1177/1088868310377394.
Centre for Policy on Ageing. Rapid review: Loneliness—Evidence of the effectiveness of interventions. 2014. http://www.cpa.org.uk/information/reviews/CPA-Rapid-Review-Loneliness.pdf
Casanova G, Zaccaria D, Rolandi E, Guaita A. The effect of information and communication technology and social networking site use on older people’s well-being in relation to loneliness: review of experimental studies. J Med Internet Res. 2021;23(3):e23588. https://doi.org/10.2196/23588.
Chipps J, Jarvis MA, Ramlall S. The effectiveness of e-Interventions on reducing social isolation in older persons: a systematic review of systematic reviews. J Telemed Telecare. 2017;23(10):817-827. https://doi.org/10.1177/1357633X17733773.
Chen Y-RR, Schulz PJ. The effect of information communication technology interventions on reducing social isolation in the elderly: a systematic review. J Med Internet Res. 2016;18(1):e18. https://doi.org/10.2196/jmir.4596.
Ibarra F, Baez M, Cernuzzi L, Casati F. A systematic review on technology-supported interventions to improve old-age social wellbeing: loneliness, social isolation, and connectedness. J Healthc Eng. 2020;2020:2036842. https://doi.org/10.1155/2020/2036842.
Choi M, Kong S, Jung D. Computer and internet interventions for loneliness and depression in older adults: a meta-analysis. Healthc Inform Res. 2012;18(3):191-8. https://doi.org/10.4258/hir.2012.18.3.191.
Lee C, Kuhn I, McGrath M, et al. A systematic scoping review of community-based interventions for the prevention of mental ill-health and the promotion of mental health in older adults in the UK. Health Soc Care Community. 2022;30(1):27–57
Fakoya OA, McCorry NK, Donnelly M. Loneliness and social isolation interventions for older adults: a scoping review of reviews. BMC Public Health. 2020;20(1):129. https://doi.org/10.1186/s12889-020-8251-6.
Veazie S, Gilbert J, Winchell K, Paynter R, Guise JM. Addressing social isolation to improve the health of older adults: a rapid review. Available at: https://pubmed.ncbi.nlm.nih.gov/30830728/. Accessed October 4, 2023.
O'Rourke HM, Collins L, Sidani S. Interventions to address social connectedness and loneliness for older adults: a scoping review. BMC Geriatr. 2018;18(1):214. https://doi.org/10.1186/s12877-018-0897-x.
Poscia A, Stojanovic J, La Milia DI, et al. Interventions targeting loneliness and social isolation among the older people: an update systematic review. Exp Gerontol. 2018;102:133-144. https://doi.org/10.1016/j.exger.2017.11.017.
Viswanathan M, Kennedy S, Eder M, Webber E, Bean S, Cairo A, Martinez L, Millet B, Gottlieb L. Social needs interventions to improve health outcomes: Review and evidence map. Available at https://www.pcori.org/sites/default/files/PCORI-Social-Needs-Interventions-to-Improve-Health-Outcomes-Scoping-Review-Evidence-Map-Report.pdf. Accessed October 4, 2023.
Pu L, Moyle W, Jones C, Todorovic M. The effectiveness of social robots for older adults: a systematic review and meta-analysis of randomized controlled studies. Gerontologist. 2019;59(1):e37-e51. https://doi.org/10.1093/geront/gny046.
Evans RL, Jaureguy BM. Phone therapy outreach for blind elderly. Gerontologist. 1982;22(1):32–5.
Passmore T LD, Tapps T, Gibson H. Impact of participation in community-based recreation program on reported loneliness and feelings of usefulness of individuals diagnoses with early stage Alzheimer’s disease. Am J Recreat Ther. 2007;6:27–39.
Alaviani M, Khosravan S, Alami A, Moshki M. The effect of a multi-strategy program on developing social behaviors based on pender’s health promotion model to prevent loneliness of old women referred to gonabad urban health centers. Int J Community Based Nurs Midwifery. 2015;3(2):132.
Thomas KS, Akobundu U, Dosa D. More than a meal? A randomized control trial comparing the effects of home-delivered meals programs on participants’ feelings of loneliness. J Gerontol B Psychol Sci Soc Sci. 2016;71(6):1049-1058.
Russell D, Peplau LA, Cutrona CE. The revised UCLA Loneliness Scale: concurrent and discriminant validity evidence. J Pers Soc Psychol. 1980;39(3):472-80. https://doi.org/10.1037//0022-3514.39.3.472.
de Jong Gierveld J, Kamphuis F. The development of a Rasch-type loneliness scale. Appl Psychol Meas. 1985;9(3):289–299.
Heller K, Thompson MG, Trueba PE, Hogg JR, Vlachos-Weber I. Peer support telephone dyads for elderly women: was this the wrong intervention? Am J Commun Psychol. 1991;19(1):53-74.
Johnson JK, Stewart AL, Acree M, et al. A community choir intervention to promote well-being among diverse older adults: results from the community of voices trial. J Gerontol B Psychol Sci Soc Sci. 2020;75(3):549-559. https://doi.org/10.1093/geronb/gby132.
Davidson JW, McNamara B, Rosenwax L, Lange A, Jenkins S, Lewin G. Evaluating the potential of group singing to enhance the well-being of older people. Australas J Ageing. 2014;33:99-104.
Cochrane Methods Bias. RoB 2: A revised Cochrane risk-of-bias tool for randomized trials. https://methods.cochrane.org/bias/resources/rob-2-revised-cochrane-risk-bias-tool-randomized-trials
Sterne JA, Hernan MA, Reeves BC, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016;355:i4919. https://doi.org/10.1136/bmj.i4919.
National Heart Lung, and Blood Institute. Study Quality Assessment Tools. https://www.nhlbi.nih.gov/health-topics/study-quality-assessment-tools
Martina CSM, Stevens NL. Breaking the cycle of loneliness? Psychological effects of a friendship enrichment program for older women. Aging Ment Health. 2006;10:467–475.
Stevens N. Combating loneliness: a friendship enrichment programme for older women. Ageing Soc. 2001;21(2):183–202.
Tilburg NS. Stimulating friendship in later life : a strategy for reducing loneliness among older women. Educ Gerontol. 2000;26(1):15–35.
Kall A, Back M, Welin C, et al. Therapist-guided internet-based treatments for loneliness: a randomized controlled three-arm trial comparing cognitive behavioral therapy and interpersonal psychotherapy. Psychother Psychosom. 2021;90(5):351-358. https://doi.org/10.1159/000516989.
Kall A, Jagholm S, Hesser H, et al. Internet-based cognitive behavior therapy for loneliness: a pilot randomized controlled trial. Behav Ther. 2020;51(1):54-68. https://doi.org/10.1016/j.beth.2019.05.001.
Ristolainen H, Kannasoja S, Tiilikainen E, Hakala M, Narhi K, Rissanen S. Effects of ‘participatory group-based care management’ on wellbeing of older people living alone: a randomized controlled trial. Arch Gerontol Geriatr. 2020;89:104095. https://doi.org/10.1016/j.archger.2020.104095.
Saito T, Kai I, Takizawa A. Effects of a program to prevent social isolation on loneliness, depression, and subjective well-being of older adults: a randomized trial among older migrants in Japan. Arch Gerontol Geriatr. 2012;55:539–547.
Kremers IP SN, Albersnagel FA, Slaets JPJ. Improved self-management ability and well-being in older women after a short group intervention. Aging Ment Health 2006;10:476–484.
Cohen GD PS, Chapline J, et al. The impact of professionally conducted cultural programs on the physical health, mental health, and social functioning of older adults. Gerontologist. 2006;46:726-734.
Chan AW, Yu DS, Choi KC. Effects of tai chi qigong on psychosocial well-being among hidden elderly, using elderly neighborhood volunteer approach: a pilot randomized controlled trial. Clin Interv Aging. 2017;12:85-96. https://doi.org/10.2147/CIA.S124604.
McAuley E, Blissmer B, Marquez DX, Jerome GJ, Kramer AF, Katula J. Social relations, physical activity, and well-being in older adults. Prev Med. 2000;31(5):608–17.
Levinger P, Panisset M, Dunn J, et al. Exercise interveNtion outdoor proJect in the cOmmunitY for older people - results from the ENJOY Seniors Exercise Park project translation research in the community. BMC Geriatr. 2020;20(1):446. https://doi.org/10.1186/s12877-020-01824-0.
Hartung J. An alternative method for meta-analysis. Biom J. 1999;41:901–916.
Hartung J, Knapp G. A refined method for the meta-analysis of controlled clinical trials with binary outcome. Stat Med. 2001;20(24):3875-89. https://doi.org/10.1002/sim.1009.
Sidik K, Jonkman J. Robust variance estimation for random effects meta-analysis. Comput Stat Data Anal. 2006;50(12):3681–3701.
IntHout J, Ioannidis JP, Borm GF. The Hartung-Knapp-Sidik-Jonkman method for random effects meta-analysis is straightforward and considerably outperforms the standard DerSimonian-Laird method. BMC Med Res Methodol. 2014;14:25. https://doi.org/10.1186/1471-2288-14-25.
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557-60. https://doi.org/10.1136/bmj.327.7414.557.
Egger M, Davey Smith G, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315(7109):629-34. https://doi.org/10.1136/bmj.315.7109.
Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics. 1994;50(4):1088-101.
GRADE Working Group. Grading of recommendations assessment, development and evaluation (GRADE). Available at https://www.gradeworkinggroup.org/. Accessed October 4, 2023.
Hopman-Rock M, Westhoff MH. Development and evaluation of “aging well and healthily”: a health-education and exercise program for community-living older adults. J Aging Phys Act. 2002;10(4):364–81.
Morrow-Howell N, Becker-Kemppainen S, Lee J. Evaluating an intervention for the elderly at increased risk of suicide. Res Soc Work Pract. 1998;8(1):28-46.
Stewart M, Craig D, MacPherson K, Alexander S. Promoting positive affect and diminishing loneliness of widowed seniors through a support intervention. Public Health Nurs. 2001;18(1):54-63.
Cox EO GK, Hobart K, et al. Strengthening the late-life care process: effects of two forms of a care-receiver efficacy intervention. Gerontologist 2007;47:388-397.
Ollonqvist K PH, Aaltonen T, et al. Alleviating loneliness among frail older people—findings from a randomised controlled trial. Int J Ment Health Promot. 2008;10:26–34.
Rosen CE, Rosen S. Evaluating an intervention program for the elderly. Community Ment Health J. 1982;18(1):21-33.
Sørensen KH, Sivertsen J. Follow-up three years after intervention to relieve unmet medical and social needs of old people. Compr Gerontol B Behav Soc Appl Sci. 1988;2(2):85-91.
Theunissen I, Spinhoven, P, van der Does. Omgaan met alleenstaan : Evaluatie van een groepscursus voor ouderen weduwen [Coping with loneliness : evaluation of a group course for elderly widows]. Tijdschr Gerontol Geriatr. 1994;25(6):250–4.
Pynnonen K, Tormakangas T, Rantanen T, Tiikkainen P, Kallinen M. Effect of a social intervention of choice vs. control on depressive symptoms, melancholy, feeling of loneliness, and perceived togetherness in older Finnish people: a randomized controlled trial. Aging Ment Health. 2018;22(1):77–84. https://doi.org/10.1080/13607863.2016.1232367.
Blazun H, Saranto K, Rissanen S. Impact of computer training courses on reduction of loneliness of older people in Finland and Slovenia. Comput Hum Behav. 2012;28(4):1202–1212.
Bruce ML, Pepin R, Marti CN, Stevens CJ, Choi NG. One year impact on social connectedness for homebound older adults: randomized controlled trial of tele-delivered behavioral activation versus tele-delivered friendly visits. Am J Geriatr Psychiatry. 2021;29(8):771–6.
Fields J, Cemballi AG, Michalec C, et al. In-home technology training among socially isolated older adults: findings from the tech allies program. J Appl Gerontol. 2021;40(5):489-499. https://doi.org/10.1177/0733464820910028.
Choi NG, Pepin R, Marti CN, Stevens CJ, Bruce ML. Improving Social Connectedness for Homebound Older Adults: Randomized Controlled Trial of Tele-Delivered Behavioral Activation Versus Tele-Delivered Friendly Visits. The American journal of geriatric psychiatry : official journal of the American Association for Geriatric Psychiatry. 2020;28(7):698–708. Comment in: Am J Geriatr Psychiatry. 2020 Jul;28(7):709–711; https://www.ncbi.nlm.nih.gov/pubmed/32303405. https://doi.org/10.1016/j.jagp.2020.02.008.
Gustafsson S, Berglund H, Faronbi J, Barenfeld E, Ottenvall Hammar I. Minor positive effects of health-promoting senior meetings for older community-dwelling persons on loneliness, social network, and social support. Clin Interv Aging. 2017;12:1867-1877. https://doi.org/10.2147/CIA.S143994.
Gaggioli A, Morganti L, Bonfiglio S, Scaratti C, Cipresso P, Serino S, Riva G. Intergenerational group reminiscence: a potentially effective intervention to enhance elderly psychosocial wellbeing and to improve Children’s perception of aging. Educ Gerontol. 2014;40:486–498.
Hansen P, Main C, Hartling L. Dance intervention affects social connections and body appreciation among older adults in the long term despite COVID-19 social isolation: a mixed methods pilot study. Front Psychol. 2021;12:635938. https://doi.org/10.3389/fpsyg.2021.635938.
Bartlett MY, Arpin SN. Gratitude and loneliness: enhancing health and well-being in older adults. Res Aging. 2019;41(8):772-793. https://doi.org/10.1177/0164027519845354.
Wang DS. Feasibility of a yoga intervention for enhancing the mental well-being and physical functioning of older adults living in the community. Activities, Adaptation & Aging. 2010;34(2):85–97.
Sidner CL, Bickmore T, Nooraie B, et al. Creating new technologies for companionable agents to support isolated older adults. ACM Trans Interact Intell Syst. 2018;8(3):1–27. https://doi.org/10.1145/3213050.
van Rossum E, Frederiks CM, Philipsen H, Portengen K, Wiskerke J, Knipschild P. Effects of preventive home visits to elderly people. Br Med J. 1993;307:27–32.
Bickmore TW CL, Clough-Gorr K, Heeren T. ‘It’s just like you talk to a friend’ relational agents for older adults. Interact Comput. 2005;17:711-735.
Nicholson NR, Shellman, J. Decreasing social isolation in older adults: effects of an empowerment intervention offered through the CARELINK program. Res Gerontol Nurs. 2013;6:89-97.
Mullins LB, Skemp L, Reed D, Emerson M. Internet programming to reduce loneliness and social isolation in aging. Res Gerontol Nurs. 2020;13(5):233-242. https://doi.org/10.3928/19404921-20200320-01.
Myhre JW, Mehl MR, Glisky EL. Cognitive benefits of online social networking for healthy older adults. Controlled Clinical Trial; Journal Article. J Gerontol B Psychol Sci Soc Sci. 2017;72(5):752‐760. https://doi.org/10.1093/geronb/gbw025.
Fields J, Cemballi A, Michalec C, et al. In-home technology training to reduce social isolation and improve tablet use among older adults: findings from the tech allies program. Journal: Conference Abstract. J Gen Intern Med. 2019;34(2):S258‐S259. https://doi.org/10.1007/11606.1525-1497.
Fokkema CM, van Tilburg TG. [Loneliness interventions among older adults: sense or nonsense?]. Tijdschr Gerontol Geriatr. 2007;38(4):185–203. Zin en onzin van eenzaamheidsinterventies bij ouderen.
Laron M, Mannheim I, Cohen Y, Weiss D, Kagya, S. The Project to Reduce and Cope with Feelings of Loneliness among Older Adults A Formative Evaluation. Available at https://brookdale.jdc.org.il/en/publication/reducing-coping-loneliness-older-adults/. Accessed October 4, 2023.
Foster A, Thompson J, Holding E, et al. Impact of social prescribing to address loneliness: A mixed methods evaluation of a national social prescribing programme. Health Soc Care Community. 2021;29(5):1439-1449. https://doi.org/10.1111/hsc.13200.
Haslam C, Cruwys T, Chang MXL, et al. GROUPS 4 HEALTH reduces loneliness and social anxiety in adults with psychological distress: Findings from a randomized controlled trial. J Consult Clin Psychol. 2019;87(9):787-801. https://doi.org/10.1037/ccp0000427.
Hill W, Weinert C, Cudney S. Influence of a computer intervention on the psychological status of chronically ill rural women: preliminary results. Nurs Res. 2006;55(1):34-42. https://doi.org/10.1097/00006199-200601000-00005.
Rodriguez-Romero R, Herranz-Rodriguez C, Kostov B, Gene-Badia J, Siso-Almirall A. Intervention to reduce perceived loneliness in community-dwelling older people. Scand J Caring Sci. 2021;35(2):366-374. https://doi.org/10.1111/scs.12852.
Shapira S, Yeshua-Katz D, Cohn-Schwartz E, Aharonson-Daniel L, Sarid O, Clarfield AM. A pilot randomized controlled trial of a group intervention via Zoom to relieve loneliness and depressive symptoms among older persons during the COVID-19 outbreak. Internet Interv. 2021;24:100368. https://doi.org/10.1016/j.invent.2021.100368.
Mountain G, Windle G, Hind D, et al. A preventative lifestyle intervention for older adults (lifestyle matters): a randomised controlled trial. Age Ageing. 2017;46(4):627-634. https://doi.org/10.1093/ageing/afx021.
Creswell JD, Irwin MR, Burklund LJ, et al. Mindfulness-Based Stress Reduction training reduces loneliness and pro-inflammatory gene expression in older adults: a small randomized controlled trial. Brain Behav Immun. 2012;26(7):1095-101. https://doi.org/10.1016/j.bbi.2012.07.006.
Routasalo PE, Tilvis R, Kautiainen H, Pitkala KH. Effects of psychosocial group rehabilitation on social functioning, loneliness and well-being of lonely, older people: randomized controlled trial. J Adv Nurs. 2009;65:297–305.
Theeke LA, Mallow JA, Moore J, McBurney A, Rellick S, VanGilder R. Effectiveness of LISTEN on loneliness, neuroimmunological stress response, psychosocial functioning, quality of life, and physical health measures of chronic illness. Int J Nurs Sci. 2016;3(3):242-251. https://doi.org/10.1016/j.ijnss.2016.08.004.
Chow AYM, Caserta M, Lund D, et al. Dual-Process Bereavement Group Intervention (DPBGI) for Widowed Older Adults. The Gerontologist. 2019;59(5):983-994. https://doi.org/10.1093/geront/gny095
Coll-Planas L, Del Valle Gomez G, Bonilla P, Masat T, Puig T, Monteserin R. Promoting social capital to alleviate loneliness and improve health among older people in Spain. Health Soc Care Commun. 2017;25(1):145-157. https://doi.org/10.1111/hsc.12284.
Collins CC, Benedict J. Evaluation of a community-based health promotion program for the elderly: lessons from Seniors CAN. Am J Health Promot. 2006;21:45-48.
McKay H, Nettlefold L, Bauman A, et al. Implementation of a co-designed physical activity program for older adults: positive impact when delivered at scale. BMC Public Health. 2018;18(1):1289. https://doi.org/10.1186/s12889-018-6210-2.
Rolandi E, Vaccaro R, Abbondanza S, et al. Loneliness and social engagement in older adults based in lombardy during the COVID-19 lockdown: the long-term effects of a course on social networking sites use. Int J Environ Res Public Health. 2020;17(21):7912.
Czaja SJ, Boot WR, Charness N, Rogers WA, Sharit J. Improving social support for older adults through technology: findings from the PRISM randomized controlled trial. Gerontologist. 2018;58(3):467-477. https://doi.org/10.1093/geront/gnw249.
Woodward AT FP, Blaschke-Thompson CM, Wishart DJ, Bakk L, Kobayashi R, et al. Technology and aging project: training outcomes and efficacy from a randomized field trial. Ageing Int. 2011;36(1):46-65.
Slegers K VBM, Jolles J. Effects of computer training and internet usage on the well-being and quality of life of older adults: a randomized, controlled study. J Gerontol Ser B-Psychol Sci Soc Sci. 2008;63:P176–P184.
White H, McConnell E, Clipp E, et al. A randomized controlled trial of the psychosocial impact of providing internet training and access to older adults. Aging Ment Health. 2002;6(3):213–21.
Neil-Sztramko SE, Coletta G, Dobbins M, Marr S. Impact of the AGE-ON tablet training program on social isolation, loneliness, and attitudes toward technology in older adults: single-group pre-post study. JMIR aging. 2020;3(1):e18398. https://doi.org/10.2196/18398.
Jones RB, Emily J, Jo A, Barbara D. Older people going online: its value and before-after evaluation\nof volunteer support. J Med Internet Res. 2015;17:122-134.
Fokkema T, Knipscheer K. Escape loneliness by going digital: a quantitative and qualitative evaluation of a Dutch experiment in using ECT to overcome loneliness among older adults. Aging Ment Health. 2007;11:496-504.
Shapira N, Barak A, Gal I. Promoting older adults’ well-being through internet training and use. . Aging Ment Health. 2007;11:477–484.
White H, McConnell E, Clipp E, Bynum L, Teague, C, Navas L, Halbrecht H. Surfing the net in later life. J Appl Gerontol. 1999;18(3):358–78.
Brodbeck J, Berger T, Biesold N, Rockstroh F, Znoj HJ. Evaluation of a guided internet-based self-help intervention for older adults after spousal bereavement or separation/divorce: a randomised controlled trial. J Affect Disord. 2019;252:440-449. https://doi.org/10.1016/j.jad.2019.04.008.
Larsson E, Padyab M, Larsson-Lund M, Nilsson I. Effects of a social internet-based intervention programme for older adults: an explorative randomised crossover study. Academic Journal. Br J Occup Ther. 2016;79(10):629‐636. https://doi.org/10.1177/0308022616641701.
Baez M, Khaghani Far I, Ibarra F, Ferron M, Didino D, Casati F. Effects of online group exercises for older adults on physical, psychological and social wellbeing: a randomized pilot trial. PeerJ. 2017;5:e3150. https://doi.org/10.7717/peerj.3150.
Dodge HH, Zhu J, Mattek NC, et al. Web-enabled conversational interactions as a method to improve cognitive functions: results of a 6-week randomized controlled trial. Journal: Article. Alzheimer’s and Dementia: Translational Research and Clinical Interventions. 2015;1(1):1‐12. https://doi.org/10.1016/j.trci.2015.01.001.
de Craen AJM GJ, Blauw GJ, et al. Randomised controlled trial of unsolicited occupational therapy in community-dwelling elderly people: the LOTIS trial. PLoS Clin Trials. 2006;1:e2.
Hall N, Debeck P, Johnson D, MacKinnon K, Gutman G, Glick N. Randomized trial of a health promotion program for frail elders. Canadian Journal on Aging-Revue Canadienne du Vieillissement. 1992;11(1):72-91.
Lai DWL, Li J, Ou X, Li CYP. Effectiveness of a peer-based intervention on loneliness and social isolation of older Chinese immigrants in Canada: a randomized controlled trial. BMC Geriatr. 2020;20(1):356. https://doi.org/10.1186/s12877-020-01756-9.
Weiss LA, Oude Voshaar MAH, Bohlmeijer ET, Westerhof GJ. The long and winding road to happiness: A randomized controlled trial and cost-effectiveness analysis of a positive psychology intervention for lonely people with health problems and a low socio-economic status. Health Qual Life Outcomes. 2020;18(1):162. https://doi.org/10.1186/s12955-020-01416-x.
van den Elzen AJ, Fokkema CM. [Home visits to the elderly in Leiden: an investigation into the effect on loneliness]. Tijdschr Gerontol Geriatr. 2006;37(4):142–6. Huisbezoeken bij ouderen in Leiden: een onderzoek naar het effect op eenzaamheid.
Roberts JR, Windle G. Evaluation of an intervention targeting loneliness and isolation for older people in North Wales. Perspect Public Health. 2020;140(3):153-161. https://doi.org/10.1177/1757913919868752.
Hind D, Mountain G, Gossage-Worrall R, Walters SJ, Duncan R, Newbould L, Rex S, Jones C, Bowling A, Cattan M, Cairns A, Cooper C, Goyder EC, Edwards RT. Putting Life in Years (PLINY): a randomised controlled trial and mixedmethods process evaluation of a telephone friendship intervention to improve mental well-being in independently living older people. Public Heal Res. 2014;2:1–252.
Kahlon MK, Aksan N, Aubrey R, et al. Effect of layperson-delivered, empathy-focused program of telephone calls on loneliness, depression, and anxiety among adults during the COVID-19 pandemic: a randomized clinical trial. JAMA Psychiatry. 2021;78(6):616-622. https://doi.org/10.1001/jamapsychiatry.2021.0113.
Juang C, Huh JWT, Iyer S, Beaudreau SA, Gould CE. Feasibility, acceptance, and initial evaluation of a telephone-based program designed to increase socialization in older veterans. J Geriatr Psychiatry Neurol. 2020:891988720944242. https://doi.org/10.1177/0891988720944242.
Rook KS, Sorkin D. Fostering social ties through a volunteer role: implications for older-adults’ psychological health. Int J Aging Hum Dev. 2003;57:313–337.
Boekhout JM, Volders E, Bolman CAW, de Groot RHM, Lechner L. Long-term effects on loneliness of a computer-tailored intervention for older adults with chronic diseases: a randomized controlled trial. J Aging Health. 2021;33(10):865–76.
Cohen-Mansfield J, Hazan H, Lerman Y, Shalom V, Birkenfeld S, Cohen R. Efficacy of the I-SOCIAL intervention for loneliness in old age: Lessons from a randomized controlled trial. J Psychiatr Res. 2018;99:69-75. https://doi.org/10.1016/j.jpsychires.2018.01.014.
Moieni M, Seeman TE, Robles TF, et al. Generativity and social well-being in older women: expectations regarding aging matter. Journal: Article in Press. J Gerontol B Psychol Sci Soc Sci. 2020. https://doi.org/10.1093/geronb/gbaa022.
Honigh-de Vlaming R. Healthy Ageing: prevention of loneliness among elderly people: evaluation of complex intervention in public health practice. Wageningen, Netherlands: Wageningen University and Research; 2013.
Low LF, Baker JR, Harrison F, Jeon YH, Haertsch M, Camp C, Skropeta M. The lifestyle engagement activity program (LEAP): implementing social and recreational activity into case-managed home care. J Am Med Dir Assoc. 2015;16:1069–1076.
Van Der Heide LA, Willems CG, Spreeuwenberg MD, Rietman J, De Witte LP. Implementation of CareTV in care for the elderly: the effects on feelings of loneliness and safety and future challenges. Technol Disabil. 2012;24:283–291.
Gonyea JG, Burnes K. Aging well at home: evaluation of a neighborhood-based pilot project to “put connection back into community”. J Hous Elderly. 2013;27(4):333–47.
Winstead V, Yost EA, Cotten SR, Berkowsky RW, Anderson WA. The impact of activity interventions on the well-being of older adults in continuing care communities. J Appl Gerontol. 2014;33(7):888-911. https://doi.org/10.1177/0733464814537701.
Bartlett H, Warburton J, Lui CW, Peach L, Carroll M. Preventing social isolation in later life: findings and insights from a pilot Queensland intervention study. Ageing Soc. 2013;33(7):1167–89.
Vella-Burrows T, Pickard A, Wilson L, Clift S, Whitfield L. ‘Dance to Health’: an evaluation of health, social and dance interest outcomes of a dance programme for the prevention of falls. Arts Health. 2019:1–15. https://doi.org/10.1080/17533015.2019.1662461.
Sherifali D, Nerenberg K, Pullenayegum E, Cheng JE, Gerstein HC. The effect of oral antidiabetic agents on A1C levels: a systematic review and meta-analysis. Diabetes Care. 2010;33(8):1859-64. https://doi.org/10.2337/dc09-1727.
Hoang P, King JA, Moore S, et al. Interventions Associated With Reduced Loneliness and Social Isolation in Older Adults: A Systematic Review and Meta-analysis. JAMA Netw Open. 2022;5(10):e2236676. https://doi.org/10.1001/jamanetworkopen.2022.36676.
Hawkley LC, Cacioppo JT. Loneliness matters: a theoretical and empirical review of consequences and mechanisms. Ann Behav Med. 2010;40(2):218-27. https://doi.org/10.1007/s12160-010-9210-8.
Funding
Dr. Shekelle, Dr. Miake-Lye, Ms. Begashaw, and Ms. Booth were supported by a grant from Humana to their respective institutions to conduct this work. The contents are those of the author(s) and do not necessarily represent the official views of, nor an endorsement, by the U.S. Government.
Author information
Authors and Affiliations
Contributions
Dr. Shekelle had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Concept and design: Shekelle, Miake-Lye, Lowery, Shrank.
Acquisition, analysis, or interpretation of data: Shekelle, Miake-Lye, Begashaw, Booth, Myers, Lowery, Shrank
Drafting of the manuscript: Shekelle.
Critical revision of the manuscript for important intellectual content: Shekelle, Miake-Lye, Begashaw, Booth, Myers, Lowery, Shrank.
Obtained funding: Shrank.
Administrative, technical, or material support: Begashaw.
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they do not have a conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Shekelle, P.G., Miake-Lye, I.M., Begashaw, M.M. et al. Interventions to Reduce Loneliness in Community-Living Older Adults: a Systematic Review and Meta-analysis. J GEN INTERN MED 39, 1015–1028 (2024). https://doi.org/10.1007/s11606-023-08517-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-023-08517-5