
Abstract
Background
This is the first study, to our knowledge, to assess uptake of oral antiviral treatment (OAV) for COVID-19 in the US and assess whether it is reaching recommended groups.
Objective
The study evaluated uptake among persons of all ages, with emphasis on utilization among individuals ages 65 + who comprise 75% of all COVID-19 deaths. To maximize public health outreach and benefit, we sought to understand reasons for use and non-use of OAV among individuals 65 + with at least mild COVID-19 symptoms.
Design
Data were collected from phase 3.5 of the US Census Household Pulse Survey, during three 2022 time periods: June 1–13, June 29–July 11, and July 27–August 8.
Participants
Respondents (n = 12,299) were ages 18 + with active or resolved COVID-19 within the last 4 weeks of their survey participation.
Main Measure(s)
Comparisons of demographic variables were made for OAV uptake using the chi-square test of independence. A logistic regression was conducted to identify characteristics of participants independently associated with receipt of an OAV. Comparisons were made with chi-square testing, between those ages 65 + with at least mild symptoms who endorsed one of a number of specific reasons for not using OAV.
Key Results
Utilization was low—17.9% of all respondents, 20.5% of respondents ages 50–64, and 33.9% of respondents 65 years and older received guideline-concordant treatment for their infection. Receipt did not differ by income or sex. The average response across the three phases was 5.4%. Most common reasons for not receiving treatment included having minimal symptoms, not thinking that they needed treatment, and not receiving a recommendation from their healthcare provider.
Conclusions
A minority of increased-risk US residents have accessed early therapy for COVID-19 despite being made available without cost. Responses suggest that efforts to improve patient and provider knowledge could improve utilization to mitigate future COVID-19 hospitalizations.
Similar content being viewed by others


In December 2021, the US Food and Drug Administration (FDA) authorized two oral antiviral therapies (OAV)—nirmatrelvir co-administered with ritonavir (Paxlovid), and molnupiravir, after clinical trials showed significant reductions in hospitalisations and serious illness[1]. They were approved for those ages 12 + with mild or moderate disease for outpatient therapy of early COVID-19 to prevent onset of severe disease, within 5 days of symptom onset[2]. Initially, this approval coincided with a worldwide Omicron wave, increasing demand for OAV in short supply and leading to rationing of these therapies for the most vulnerable[3].
By February 2022, the United States (US) had adequate supply of OAV to meet demand and many jurisdictions had under-utilized inventories. This prompted the Centers for Disease Control and Prevention (CDC)[4], the Guidelines Panel of the National Institutes of Health, and many professional societies[5] to recommend prompt therapy to the at-risk 40% of the US population as estimated by the FDA. On May 24, 2022, the CDC issued a Health Alert Network (HAN) Health Advisory to update healthcare providers, public health departments, and the public, stating that “Paxlovid continues to be recommended for early-stage treatment of mild to moderate COVID-19 among persons at high risk for progression to severe disease”. On June 11, the CDC provided further interim guidance stating that clinicians should consider oral COVID-19 treatment in non-hospitalized patients who meet all of the following: (a) test positive for SARS-CoV-2 (with PCR or antigen test, including at-home tests), (b) have symptoms consistent with mild to moderate COVID-19, (c) are within 5 days of symptom onset, and (d) have one or more risk factors for severe COVID-19. Risk factors for severe COVID-19 included (a) age over 50 years, with risk increasing substantially at age ≥ 65 years; (b) being unvaccinated or not being up to date on COVID-19 vaccinations; and (c) specific medical conditions and behaviors.
To our knowledge, there have been no studies in the US or elsewhere to assess uptake of OAV and whether it is reaching recommended groups. Hence, we first evaluated uptake among persons of all ages, then sought to determine utilization specifically among individuals ages 65 + who comprise 75% of all COVID-19 deaths[6]. We also sought to understand reasons for use and non-use of OAV among individuals ages 65 + with at least mild symptoms to direct approaches to maximize public health benefit.
METHODS
We accessed individual-level data from the US Census Bureau’s Household Pulse Survey (HPS). This online survey invites a random sample of US adults (ages 18 +) to understand how the pandemic has impacted their daily lives. HPS full technical documentation regarding data collection as well as the questions included in the survey can be found on the Census Bureau’s website[7].
New in phase 3.5 of HPS, participants diagnosed with COVID-19 in the prior 4 weeks were asked about their use of OAV and reasons for non-use. Data were collected during three 2022 time periods: June 1–13, June 29–July 11, and July 27–August 8. The average response rate of 5.4% is comparable to response rates used in published literature with the HPS dataset[8,9,10]. Respondents included participants with active or resolved COVID-19 and individuals with or without conditions making them eligible for Emergency Use Authorization OAV.
In a first step, comparisons of demographic and health variables were made between those who did and did not receive OAV, using the chi-square test of independence to identify significant differences (α = 0.05). Subsequently, a logistic regression was conducted to identify characteristics of participants independently associated with receipt of an OAV. In a second step limited to those aged 65 + years and with at least self-reported mild symptoms, comparisons were made, with chi-square testing, between those who did (and did not) endorse one of a number of specific reasons for not using OAV.
RESULTS
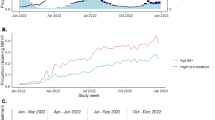
Of the 167,931 respondents, 12,299 who tested positive for COVID-19 within the last 4 weeks of their survey participation were included in the analysis. Of those, 17.9% (n = 2208) received OAV, including 11.3% of those 18–49, 20.5% of those 50–64, and 33.9% of those ages 65 + . There was little improvement in uptake for individuals ages 65 + across the three phases, increasing from 30.2% in phase 1 to 34% in phase 2 and 36% in phase 3.
Participants most likely to be treated were aged 65 + years, Black, Northeast residents, with public health insurance (which includes Medicare, Medicaid, Medical Assistance, or VA Health Care), fully vaccinated, had no prior history of a COVID-19 infection, had mobility difficulties, and reported severe COVID-19 symptoms. No differences were seen in sex and household income. Full sample characteristics are presented in Table 1.
In a multivariable analysis, older age, income, race, insurance, greater COVID-19 symptom severity, and mobility difficulties were associated with receipt of OAV. Sex and vaccination status were not associated with receipt of OAV in the multivariate model despite being independently associated with OAV receipt, while race was approaching significance. Compared with respondents aged 18 to 49 years, middle-aged and older individuals had increased odds of receiving OAV, adjusted odds ratio (aOR) of 1.80 (95% confidence interval [CI] 1.58 to 2.06) and 3.45 (2.90 to 4.09) for age 50 to 64 and age 65 + years, respectively. Those with moderate (1.71 (1.13 to 2.57)) or severe symptoms (2.46 (1.60 to 3.78)) were more likely to report receipt of OAV. Individuals reporting mobility difficulties were also more likely to receive OAV, 1.35 (1.19 to 1.59). Full results are presented in Table 2.
Of the 2344 respondents aged 65 + with at least mild symptoms, 1476 did not receive therapy; 1234 of them (84%) provided a reason for not receiving treatment, including having minimal symptoms (20.6%), not thinking that they needed treatment (16.4%), not receiving a recommendation from their healthcare provider (14.5%), and not perceiving themselves to be a member of a high-risk group (4.9%).
Participants offering reasons for not needing treatment differed by sex, race, income, insurance, mobility difficulties, and symptom severity; not sick/no symptoms differed by race, income, insurance, mobility difficulties, and symptom severity; not being offered or recommended treatment differed by insurance; and not seeing oneself as a member of a high-risk group differed by income, insurance, and mobility difficulties. Full sample characteristics are presented in Table 3.
DISCUSSION
New CDC guidance states that individuals aged 50 years and above are at greater risk of severe COVID-19 disease, with risk increasing substantially by age 65. However, in this nationwide sample of Americans diagnosed with COVID-19 in May through August 2022, only 17.9% of all respondents, 20.5% of respondents ages 50–64, and 33.9% of respondents 65 years and older received guideline-concordant treatment for their infection. Notably, 2/3 of those in the highest risk age group, 65 + , did not receive treatment. Receipt did not differ by income or sex. Most common reasons for not receiving treatment included having minimal symptoms, not thinking that they needed treatment, and not receiving a recommendation from their healthcare provider.
While OAV is most effective in early COVID-19 when symptoms are still mild, a number of respondents ages 65 + with mild symptoms indicated limited symptoms as a reason for not receiving treatment. Low utilization may be a by-product of the early eligibility messaging limiting therapy to the most vulnerable when supply was limited. Since supply has become more available, the White House has implemented the Test to Treat program, and acknowledged in April 2022 that patient and provider education is needed to clarify actual eligibility based on FDA authorization versus CDC/NIH rationing guidelines in order to increase uptake[11]. Utilization also may be limited by concerns on the part of professionals and the public over rebound infections with OAV use, although such infections are not associated with higher mortality or more frequent hospitalization[4]. Some estimates show that nearly 40% of Americans given their age or health conditions qualify as high risk for COVID-19[12]. Educational messages encouraging treatment even when symptoms are mild could be effective.
Additionally, accessing OAVs may be a daunting challenge for COVID-19-positive patients. Getting access to a doctor within the key 5-day window may not always be possible, and others may not know where to turn to begin the process of getting a prescription. While pharmacists may be a convenient local option for some, one can question whether it is good public health practice to encourage COVID-19-positive patients to break the recommended 5-day isolation. As well, without recent documentation of normal liver and kidney function, a pharmacist is unable to prescribe an OAV. Despite the great benefits of OAVs, many lingering barriers remain.
There are limitations to this study. First, data are self-reported, requiring participants to self-assess their symptom severity and risk status. Categorical definitions for these items are not provided in the survey and could have led to inaccurate reporting. Although respondents were asked to recall information from the past 4 weeks, there is the possibility of bias in their reporting. Furthermore, low response rates for the survey, while consistent with other recent surveys, may have led to study samples with limited representation of the general population.
This study provides a crucial first benchmark prior to a more aggressive national roll-out and use of pharmacists to prescribe and offer OAV. Across all ages, uptake of OAV is low, with suboptimal utilization reported those at highest risk by age, i.e., those 50 + and particularly 65 + with COVID-19. More dedicated patient and provider education is essential to ensure that those who are eligible receive this effective treatment. However, further research is required to determine if there are other salient reasons why individuals with COVID-19 are not seeking treatment as uptake among those at greatest risk of severe disease has improved only slightly. A more precise understanding of the roadblocks to utilization is a prerequisite for new educational messaging and campaigns.
References
Mahase E. Covid-19: Pfizer’s paxlovid is 89% effective in patients at risk of serious illness, company reports. BMJ. 2021;375:n2713. https://doi.org/10.1136/bmj.n2713
Centers for Disease Control and Prevention. COVID-19 and Your Health. Centers for Disease Control and Prevention. Published February 11, 2020. Accessed August 15, 2022. https://www.cdc.gov/coronavirus/2019-ncov/your-health/treatments-for-severe-illness.html
Evans JW Jared S Hopkins and Melanie. Patients Go Without Covid-19 Treatments Amid Drug Shortage. WSJ. Published February 1, 2022. Accessed July 29, 2022. https://www.wsj.com/articles/patients-go-without-covid-19-treatments-amid-drug-shortage-11643736496
Centers for Disease Control and Prevention. HAN Archive - 00467 | Health Alert Network (HAN). Published May 24, 2022. Accessed July 29, 2022. https://emergency.cdc.gov/han/2022/han00467.asp
National Institute of Health. Ritonavir-Boosted Nirmatrelvir (Paxlovid). COVID-19 Treatment Guidelines. Accessed August 4, 2022. https://www.covid19treatmentguidelines.nih.gov/therapies/antiviral-therapy/ritonavir-boosted-nirmatrelvir--paxlovid-/
Simon S. Elderly people make up 75% of COVID-19 deaths. Many more have died from isolation. NPR. https://www.npr.org/2022/02/19/1081948849/elderly-people-make-up-75-of-covid-19-deaths-partially-due-to-loneliness. Published February 19, 2022. Accessed September 5, 2022.
US Census Bureau. Household Pulse Survey: Measuring Social and Economic Impacts during the Coronavirus Pandemic. Census.gov. Accessed July 29, 2022. https://www.census.gov/householdpulse
Pew Research Center. Assessing the Representativeness of Public Opinion Surveys | Pew Research Center. Accessed July 29, 2022. https://www.pewresearch.org/politics/2012/05/15/assessing-the-representativeness-of-public-opinion-surveys/
Hsieh YL, Rak S, SteelFisher GK, Bauhoff S. Effect of the suspension of the J&J COVID-19 vaccine on vaccine hesitancy in the United States. Vaccine. 2022;40(3):424-427. doi:https://doi.org/10.1016/j.vaccine.2021.11.085
Pew Research Center. What Low Response Rates Mean for Telephone Surveys. Pew Research Center Methods. Published May 15, 2017. Accessed July 29, 2022. https://www.pewresearch.org/methods/2017/05/15/what-low-response-rates-mean-for-telephone-surveys/
The White House. Background Press Call by Senior Administration Officials on New Actions to Increase Access to COVID-19 Treatments and Boost Patient and Provider Awareness. The White House. Published April 25, 2022. Accessed August 4, 2022. https://www.whitehouse.gov/briefing-room/press-briefings/2022/04/25/background-press-call-by-senior-administration-officials-on-new-actions-to-increase-access-to-covid-19-treatments-and-boost-patient-and-provider-awareness/
Claxton G, 2020. How Many Adults Are at Risk of Serious Illness If Infected with Coronavirus? Updated Data. KFF. Published April 23, 2020. Accessed August 4, 2022. https://www.kff.org/coronavirus-covid-19/issue-brief/how-many-adults-are-at-risk-of-serious-illness-if-infected-with-coronavirus/
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they do not have a conflict of interest.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Benchimol-Elkaim, B., Dryden-Peterson, S., Miller, D.R. et al. Oral Antiviral Therapy Utilization Among Adults with Recent COVID-19 in the United States. J GEN INTERN MED 38, 1717–1721 (2023). https://doi.org/10.1007/s11606-023-08106-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-023-08106-6