
Abstract
Background
Half of women undergoing mammography have dense breasts. Mandatory dense breast notification and educational materials have been shown to confuse women, rather than empower them.
Objective
This study used a mixed method, multi-stakeholder approach to assess acceptability of an interactive, computer-animated agent that provided breast density information to women and changes in knowledge, satisfaction, and informational needs.
Design
A pre-post survey and qualitative focus groups assessed the acceptability of the computer-animated agent among women. An anonymous, online survey measuring acceptability was delivered to a multi-stakeholder group.
Participants
English-speaking, mammography-eligible women ages 40–74 were invited and 44 women participated in one of nine focus groups. In addition, 14 stakeholders representing primary care, radiology, patient advocates, public health practitioners, and researchers completed the online survey.
Interventions
A prototype of a computer-animated agent was delivered to women in a group setting; stakeholders viewed the prototype independently.
Main Measures
Data collected included open-ended qualitative questions that guided discussion about the content and form of the computer-animated agent. Structured surveys included domains related to knowledge, acceptability, and satisfaction. Stakeholder acceptability was measured with a series of statements about aspects of the intervention and delivery approach and are reported as the proportion of respondents who endorsed each statement.
Key Results
Six of 12 knowledge items demonstrated improvement post-intervention, satisfaction with the agent was high (81%), but the number of unanswered questions did not improve (67% vs. 54%, p = 0.37). Understanding of the distinction between connective and fatty tissue in the breast did not increase (30% vs. 26%, p = 0.48). Results of the multi-stakeholder survey suggest broad acceptability of the approach and agent.
Conclusions
Findings highlight the benefits of a brief interactive educational exposure as well as misperceptions that persisted. Results demonstrate the need for an evidence-based, accessible intervention that is easy to understand for patients.
Similar content being viewed by others


BACKGROUND
Over 27 million women in the USA have mammographically dense breasts, representing 40–50% of women undergoing mammography.1 Women with heterogeneously or extremely dense breasts are at 1.2–2.3 times greater risk of breast cancer compared to women with scattered fibroglandular density.2 Dense breasts are associated with higher rates of interval cancers,3 those identified between routine screenings, in part due to reduced mammography sensitivity.4 Breast density also varies by race, with black women more likely to have high breast density.5 Over 36 states have passed laws requiring that women receive written notification of their breast density post-mammogram,6 and the FDA has proposed regulations to set a national dense breast reporting standard.7 Currently, mandated dense breast notification content and its complexity varies by state.8 Notifications are intended to increase individual awareness of risk and support informed decision-making for supplemental screening, but early indications are that these laws do not fulfill this potential. Many women feel confused or anxious after receiving notifications, gain little knowledge, and are not clear on what to do based on notifications.9,10,11,12
The balance of risks and benefits of supplemental screening among women with high density remains unclear.13 As evidence on appropriate screening for women with dense breasts accrues, many recommend situating breast density within the context of overall breast cancer risk to determine need for supplemental screening.14, 15 Yet, primary care providers feel ill-prepared to counsel women about dense breasts and few report using risk assessment tools to determine appropriate supplemental screening,16,17,18 despite available guidance on risk stratification for women with dense breasts to inform choices.14, 15, 19 Thus, awareness of breast density and associated risks remains low.9, 20,21,22,23,24
Improvements in communication and education are needed for both patients and providers, but the field has yet to rigorously develop educational tools that address known misperceptions. Our previous work shows women want to be told of their breast density and require more information to make informed decisions.12, 25 This study aimed to (1) develop a prototype interactive tool for patients to supplement breast density notifications using a community-engaged approach; (2) test the impact of the prototype on breast density knowledge, informational needs, and satisfaction among a mammography-eligible women; and (3) assess acceptability among a multi-stakeholder group including patients, public health professionals, and providers from primary care and radiology.
METHODS
Overview
This cross-sectional study assessed acceptability and changes in knowledge with the use of an interactive, computer-animated agent that provided breast density information. We used surveys and qualitative focus groups to evaluate the agent developed in partnership with a local breast cancer advocacy group. Data collection occurred from April through June 2019. This research was reviewed and approved by the Boston Medical Center Institutional Review Board.
Educational Material Development
We aimed to develop materials that would address the known knowledge gaps in breast density notifications and be focused on user needs. We sought to include minority women in the development, as minority women are less often aware of breast density,26 yet are more likely to have dense breasts5 and experience poorer cancer outcomes.27, 28 Thus, we partnered with the Pink and Black Education and Support Network, a group of black breast cancer survivors who lead education and outreach efforts. We held two facilitated feedback sessions with Pink and Black members (n = 10) during which we identified their top priorities for breast density education using a cognitive priming task. Women rated a series of statements and their relative importance. Their highest stated priorities included (1) knowing what they could do about dense breasts, (2) being able to ask questions, and (3) getting information quickly.
Based on prior work developing conversational agent systems that are responsive to patient health information needs,29,30,31,32 we created a prototype computer-animated agent that simulates a face-to-face conversation with a health educator (Fig. 1). Computer-animated agents address women’s desire for accessibility and interactivity as they adapt messages to individual patient responses and the immediate context of the conversation. They also provide information in a consistent manner and in a low-pressure environment, outside of the time-constrained clinical encounter, so that patients may take as much time as they need to fully understand the information.33 The information in the current prototype was adapted from patient educational materials on breast density, and modeled into a conversational, interactive form. Salient topics and descriptions were identified as desirable by Pink and Black Education and Support Network members who provided feedback prior to prototype development.34, 35

Screenshot of prototype computer-animated agent, Danya.
The prototype, Danya, was presented to women through two sample interactions displayed as videos: a 30-s greeting introduced Danya as a virtual health counselor and a 3-min sample in which Danya presented information about breast density. The sample interaction reviewed when women could expect results, displayed a sample breast density notification letter, reassured women, explained breast density using pictures, and described some possible next steps. Both videos included demonstrations of Danya’s interactive elements, with an off-screen user providing responses to Danya’s prompts.
Study Population
We tested the prototype among 44 mammography-eligible English-speaking women ages 40–74. Study information cards and flyers were posted in primary care and radiology clinics, as well as distributed by Pink and Black advocates within community venues. Interested participants contacted the study team, who verified eligibility and scheduled women into one of nine focus groups. Additionally, stakeholders representing primary care clinicians, radiologists, patient advocates, public health practitioners, and researchers were identified through the authors’ professional networks. Stakeholders received an email invitation to view the online prototype and complete a survey about the content.
Focus Group Data Collection
Data from mammography-eligible women was collected through 90–120 min focus groups with associated surveys administered before and after exposure to the computer-animated agent. Study activities took place at Boston Medical Center or community centers. Upon arrival, women reviewed a study information sheet and completed a baseline survey covering knowledge about breast density, mammogram history, satisfaction with information related to mammogram results, and demographics. All women agreed to audio-recording of the focus group, which was later transcribed. Focus groups were facilitated by an investigator, with at least one research assistant taking notes. Facilitators presented the computer-animated agent 30-s greeting and elicited impressions about the style and substance. The 3-min breast density education clip was then shown, again followed by guided discussion about the content and form. After conclusion of the focus group, women completed a second survey covering knowledge about breast density, and satisfaction. Women received a $40 debit card for their participation at the conclusion of study activities.
Multi-stakeholder Data Collection
Surveys measuring acceptability of the agent and delivery strategy were collected online. Stakeholders were invited by email to review the computer-animated agent prototype and provide feedback via a structured survey. Data were collected and managed using REDCap (Research Electronic Data Capture) hosted at Boston University, CTSI UL1TR001430.36
Measures
Data collected from mammography-eligible women included open-ended qualitative questions that guided discussion about the content and form of the computer-animated agent. Structured surveys included domains related to knowledge, acceptability, and satisfaction. Three scales were compared pre-post: (1) Knowledge, measured by 12 true/false statements about key information in the breast density video; (2) Unmet informational needs comprised of three items, measuring women’s satisfaction with the level and amount of information and whether there were remaining questions; (3) Satisfaction, measured on a 5-point Likert scale (Very Satisfied to Very Dissatisfied). We hypothesized that the computer-animated agent would increase knowledge and satisfaction, while decreasing unmet informational needs.
The online stakeholder surveys included an initial question to determine whether the respondent was a clinical provider, which determined branching logic. All respondents were asked about acceptability either for themselves (non-clinicians) or their patients (clinician stakeholders) related to the computer-animated agent and delivery approach. Measures are reported as percent agreement for each statement.
Analysis
Qualitative analysis included creating a taxonomy of potential issues related to the prototype’s content, context, and format that guided analysis37 using NVivo qualitative software. One author primarily coded transcripts to develop a codebook and reviewed it with the study team. Using constant comparison techniques,38 we ensured that fidelity was maintained by having a second author review coded transcripts to ensure transparency and quality in coding. Any clarifications in coding were resolved through study team discussion.
Descriptive statistics (means, medians, frequencies) were generated for each of the survey measures of satisfaction, informational needs, and breast density knowledge. Pre-post comparisons using McNemar’s tests with an exact function to account for small cell sizes, explored pre-post changes in satisfaction, informational needs, and knowledge. Statistical significance was set at the level of p < 0.05. Stakeholder surveys descriptively summarized acceptability for all stakeholder groups.
RESULTS
Focus Group Participant Characteristics
As displayed in Table 1, focus group participants had a mean age of 59 years (SD = 7.7) and were predominantly black (73%, n = 32). Educational backgrounds were diverse with 14% (n = 6) completing less than high school, 34% (n = 15) with a high school degree or GED, 20% (n = 9) attended some college, and 32% had an Associate’s degree or higher. Most women were either very (57%, n = 25) or somewhat (23%, n = 10) satisfied with the mammogram results information they had received in the past, although focus groups later uncovered uncertainty and confusion about mammography concepts. One-third of participants (32%, n = 14) reported they had been told they have dense breasts; one-quarter were unsure (25%, n = 11). When asked about sources of breast density information, the most common response was that they had received no breast density information (45%, n = 20), followed by receiving information from a primary care doctor (30%, n = 13).
Focus Group Results
As displayed in Table 2, most participants reported they were satisfied with the computer-animated agent, Danya (68%, n = 30), she was easy to understand (75%, n = 33), they were confident in her ability to help them (64%, n = 28), and would follow her advice (55%, n = 24). Half felt comfortable with Danya or would like to continue working with her (50%, n = 22). Additionally, Danya made 40% (n = 18) of participants less nervous about dense breasts. Women described experiencing heightened anxiety while awaiting results, and felt Danya could support them in this period: “You will panic if you don’t hear from them, ‘Oh, it’s been a week.’ So for her to be able to give [women] that information, I definitely think that was good.” Women were split in expressing strong preferences for communication with a doctor or nurse over the computer-animated agent: 57% (n = 25) strongly agreed or agreed with the statement “I would rather talk to my doctor than Danya,” while 43% (n = 19) did so for a similar statement about their nurse. One theme that emerged was a preference for being able to ask questions from a credible source without judgment, a need many women felt Danya could meet: “[Danya] would be good because maybe you have things you don’t want anybody else to know. Just to be able to answer and you can get a better idea.” Confidentially asking questions was contrasted with preferences for having information shared with the woman’s physician team, especially for those who did not have timely access to their doctor:
“A lot of us, don’t know how to advocate for [ourselves]… we always forget to ask the doctor something, and to be able to do that and have the doctor see that question, and to be able to have the doctor or someone working with the doctor be able to respond to that question.”
The impression that the computer-animated agent could improve communication between the health care team and patient was appealing, but tempered slightly by women’s concerns about privacy:
“I have mixed opinions about [Danya] because I kind of feel like it is just me and her. If it is just the two of us just talking, I feel a little bit safer… but once I report to her, who is going to transcribe all of this? If it wasn’t such pertinent information, if it was just “how are you doing, we got your results back.” Okay, [that’s] fine, good.”
Discussions about privacy and data sharing were the primary source of concerns raised by women across focus groups.
Changes in Satisfaction, Information Needs, and Knowledge
After reviewing the computer-animated agent prototype, women had greater satisfaction with the amount and quality of breast density information than before, and had greater breast density knowledge (Table 3). Among 24 women that had received breast density information prior to focus group participation, there was higher satisfaction with both the amount (21%, n = 5 versus 67%, n = 29; p < 0.01) and quality (17%, n = 4 versus 64%, n = 27; p < 0.01) of breast density information after the intervention compared to prior. In the post-intervention period, 81% respondents (35/43) were “very satisfied” with breast density information overall (data not shown). There was no significant change in the proportion of participants with unanswered questions about breast density (pre: 67%, n = 16, post: 54%, n = 13; p = 0.37), contrary to our hypothesis. This was confirmed in qualitative responses, where women indicated several areas of new questions they had not previously considered: “Her explanation leads to more questions… She said you have fatty tissue, then she used the word something else. That just raised more questions because what if we don’t know what connective tissues are.” Understanding the role of fatty versus connected tissue was most difficult for women to understand based on the information presented.
Table 3 displays the percent of women who agreed with each knowledge item pre- and post-, along with representative quotes, which highlight some of the challenges in communicating about these concepts to women. The proportion of correct responses significantly increased for six of 12 true/false knowledge questions in the post-intervention period. Women were more likely to report that having dense breasts increases risk for cancer (42 to 74%, p < 0.01), almost half of women have dense breasts (37 to 72%, p = 0.02), having dense breasts makes it harder to see cancer on a mammogram (58 to 81%, p = 0.03), and having dense breast may mean they should have other screening tests (70 to 91%, p = 0.01). More women correctly reported that breast density cannot be felt in the post-test, but the proportion remained modest (pre: 26%, n = 11, post: 54%, n = 23; p < 0.01). Women demonstrated continued confusion about whether breast density changes as they get older, dense tissue is made up of fat, or whether lower breast density means a woman will not get breast cancer.
Multi-stakeholder Acceptability Survey
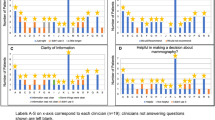
Clinician (n = 5) and non-clinician (n = 9) stakeholders provided positive feedback on Danya and the education strategy (Table 4). Most reported that the agent would be easy for them or their patients to use (79%, n = 11) and understand (86%, n = 12). The most commonly endorsed uses of the computer agent were to learn information about the mammography process (64%, n = 9), or learn more about (mammogram) results (50%, n = 7). Most stakeholders felt that a patient education strategy including a computer-animated agent was better than current practice (86%, n = 12), would help them/their patients make more informed decisions (64%, n = 9), and would generate more benefit than harm (79%, n = 11). Fewer stakeholders felt that the strategy would save time (36%, n = 5), or among non-clinicians only, would help them worry less (29%, n = 4).
DISCUSSION
This study tested the acceptability of a computer-animated agent prototype to deliver breast density information among a multi-stakeholder group and its impact on women’s knowledge, informational needs, and satisfaction. We found that knowledge for many items improved and satisfaction was high, but some misconceptions persisted. Results of the stakeholder survey suggest initial acceptability of the prototype. Our findings point to several areas where breast density information provision can be improved for diverse populations using technology-based, interactive solutions.
Qualitative and quantitative results underscore that breast density is not an intuitive concept for many women. Most focus group participants (75%) rated Danya as easy to understand, yet qualitative data demonstrated that women struggled to explain foundational concepts communicated in the prototype. The computer-animated agent did improve knowledge about breast density as a risk factor for cancer, with 75% of women understanding this in the post-intervention assessment. This rate is higher than other studies examining knowledge after dense breast notifications where 37–53% understand this concept after reading the notification.9, 12, 25 While the prototype described breast density in what is considered common terminology (i.e., the amount of fatty tissue relative to connective tissue in the breast), participants clearly had lingering questions about this definition and its meaning after a brief exposure. We will thus refine the agent to include question prompts to elicit understanding and respond with alternative explanations, clarifications, and use additional supportive images to explain breast density. The flexibility of the computer-animated agent’s approach fits with data suggesting that personal relevance, context, and readiness are important considerations in learning new health concepts.39
Women highlighted that learning about mammography results, usually outside of the doctor’s office, heightens anxiety when results include new terminology. Anxiety and worry have long been associated with breast cancer screening40,41,42,43 and breast density notification.21 However, interventions that comprehensively address both informational and psychosocial needs over the course of the entire screening process—from referral to diagnostic resolution—are limited. Computer-animated agents are responsive to this problem in that they deliver information on personally relevant screening topics and interact with women to provide emotional support. They have been shown to reduce anxiety, boost confidence,31 and support shared decision-making32 across health topics. Most mammography results dissemination continues to be done outside of the context of a visit, does not satisfy women’s informational needs,44, 45 and is accompanied by provider reticence to comprehensively counsel on breast density,16,17,18 including risk assessment.46,47,48,49 The agent has the potential to effectively address these challenges that inhibit informed discussions about supplemental screening. More robust explanations about breast density and identifying when provider contact is needed may improve trust in the agent and reduce the number of individuals who reported they wanted to talk to their doctor after using the prototype, which was high at 57%. We believe this primarily reflects the brevity of exposure to new content and lack of personalized information available in the current version. Future applications of this technology will incorporate personal risk assessment and integrate with the medical record so that patient confidence and clinical care could be improved. This study has demonstrated preliminary acceptability of this approach among a diverse set of stakeholders including clinicians, and addressing areas of modest satisfaction will enhance this prototype.
Results from the stakeholder survey indicate that this group of clinician and non-clinician professionals views the computer-animated agent as an information conduit for women; 64% endorsed the agent for providing information about mammography. Fewer supported the modality for learning about results (50%) or learning about their risk (36%). Given the time constraints and difficulty of using online risk calculators, which require high levels of health literacy skills to complete,50 we expected higher levels of endorsement of these activities. Yet, responses may reflect concerns about patients interacting with risk assessments without clinical guidance. These include the inherent uncertainty in risk estimates, especially in light of their modest discriminatory accuracy; the proliferation of commercial risk tools with persuasive messaging; and a lack of data on the effects of online tools for underserved populations.51,52,53 To achieve meaningful evidence-based decision-making for women with dense breasts, a computer-animated agent intervention must address these shortcomings of online, stand-alone tools by coordinating with health systems and providing physician support. Integration must be balanced with patient privacy concerns that were raised, underscoring the need to carefully consider where and how the computer-animated agent connects with other systems and minimize the transfer of protected health information. Optimizing these features, including integration within clinical practice and minimizing provider burden after agent interactions, will be the focus in future iterations. In addition, the fully interactive conversational agent uses fully constrained user input, enabling its advice to be completely validated (unlike chatbots and conversational assistants that use unconstrained natural language input.54
There are several limitations to this research. As a pilot study, the sample sizes across women and stakeholders are modest, limiting our explanatory power in the pre-post survey analysis. However, we see several important differences in knowledge for women, and these results are bolstered by the extensive qualitative data collection from nine focus groups. We tested the prototype in a group setting at a single time point, and we were unable to test the interactive nature of the system, which is discordant with how women will ultimately use the intervention (i.e., alone, longitudinally, and interactively). Further, we did not have sufficient sample sizes to examine stakeholder survey data by stakeholder type. We did see generally high levels of agreement across acceptability metrics, which suggests marginal utility of group comparisons, although results may be subject to some social desirability bias. Finally, our sample was predominantly black, which may not be representative of other groups’ informational needs. However, the disproportionate mortality from breast cancer among black women speaks to the importance of engaging minority women in understanding their own cancer risk and evidence-based screening practices, especially given their underrepresentation in cancer control and prevention research.55, 56
CONCLUSIONS
This study demonstrated initial acceptability of a computer-animated agent to deliver breast density information with a positive impact on knowledge. Findings can inform breast density education efforts in highlighting misperceptions that persisted following a brief educational exposure using commonly delivered information. Results reported by multiple stakeholders demonstrate the need for an integrated, evidence-based intervention that is easy to understand, yet maintains patient privacy. Future work should focus on how interactive interventions can be uniquely tailored to meet both the informational and psychosocial needs of women undergoing mammography across the entire diagnostic process.
References
Sprague BL, Gangnon RE, Burt V, et al. Prevalence of Mammographically Dense Breasts in the United States. Journal of the National Cancer Institute. 2014;106(10).
Wang AT, Vachon CM, Brandt KR, Ghosh K. Breast density and breast cancer risk: a practical review. Mayo Clin Proc. 2014;89(4):548–557.
Porter PL, El-Bastawissi AY, Mandelson MT, et al. Breast Tumor Characteristics as Predictors of Mammographic Detection: Comparison of Interval- and Screen-Detected Cancers. JNCI: Journal of the National Cancer Institute. 1999;91(23):2020–2028.
Mandelson MT, Oestreicher N, Porter PL, et al. Breast density as a predictor of mammographic detection: comparison of interval- and screen-detected cancers. J Natl Cancer Inst. 2000;92(13):1081–1087.
McCarthy AM, Keller BM, Pantalone LM, et al. Racial Differences in Quantitative Measures of Area and Volumetric Breast Density. JNCI: Journal of the National Cancer Institute. 2016;108(10):dwj104.
Dense Breast Info, Inc. 2017; http://densebreast-info.org/legislation.aspx#. .
Proposed Rule: Mammography Quality Standards Act. 2019; https://www.federalregister.gov/documents/2019/03/28/2019-05803/mammography-quality-standards-act.
Kressin N, Gunn C, Battaglia T. Content, Readability, and Understandability of Dense Breast Notifications by State JAMA. 2016;315(16):1786–1787.
Rhodes DJ, Breitkopf CR, Ziegenfuss JY, Jenkins SM, Vachon CM. Awareness of Breast Density and Its Impact on Breast Cancer Detection and Risk. Journal of Clinical Oncology. 2015;33(10):1143–1150.
Yeh VM, Schnur JB, Margolies L, Montgomery GH. Dense breast tissue notification: impact on women's perceived risk, anxiety, and intentions for future breast cancer screening. Journal of the American College of Radiology : JACR. 2015;12(3):261–266.
Trinh L, Ikeda DM, Miyake KK, et al. Patient awareness of breast density and interest in supplemental screening tests: comparison of an academic facility and a county hospital. Journal of the American College of Radiology : JACR. 2015;12(3):249–255.
Gunn C, Battaglia T, Paasche-Orlow M, West A, Kressin N. Women’s Perceptions of Dense Breast Notifications: “So what is that supposed to mean?”. Patient Educ Couns. 2018;101(6):1123–1129.
Melnikow J, Fenton JJ, Whitlock EP, et al. Supplemental Screening for Breast Cancer in Women With Dense Breasts: A Systematic Review for the U.S. Preventive Services Task Force. Annals of Internal Medicine. 2016;164(4):268–278.
Freer P, Slanetz P, Haas J, et al. Breast cancer screening in the era of density notification legislation: Summary of 2014 Massachusetts experience and suggestion of an evidence-based management algorithm by multi-disciplinary expert panel. Breast Cancer Res Treat. 2015;153(2):455–464.
Price ER, Hargreaves J, Lipson JA, et al. The California Breast Density Information Group: A Collaborative Response to the Issues of Breast Density, Breast Cancer Risk, and Breast Density Notification Legislation. Radiology. 2013;269(3):887–892.
Gunn CM, Kressin NR, Cooper K, Marturano C, Freund KM, Battaglia TA. Primary Care Provider Experience with Breast Density Legislation in Massachusetts. Journal of Women's Health. 2018;27(5):615–622.
Brown J, Soukas C, Lin JJ, Margolies L, Santiago-Rivas M, Jandorf L. Physician Knowledge, Attitudes, and Practices Regarding Breast Density. J Women's Health. 2019;28(9):1193–1199.
Maimone S, McDonough MD, Hines SL. Breast Density Reporting Laws and Supplemental Screening—A Survey of Referring Providers’ Experiences and Understanding. Current Problems in Diagnostic Radiology. 2017;46(2):105–109.
Kerlikowske K, Sprague BL, Tosteson ANA, et al. Strategies to Identify Women at High Risk of Advanced Breast Cancer During Routine Screening for Discussion of Supplemental Imaging JAMA Internal Medicine. 2019;179(9):1230–1239.
O’Neill SC, Leventhal KG, Scarles M, et al. Mammographic Breast Density as a Risk Factor for Breast Cancer: Awareness in a Recently Screened Clinical Sample. Women's Health Issues. 2014;24(3):e321-e326.
Manning M, Albrecht TL, Yilmaz-Saab Z, Shultz J, Purrington K. Influences of race and breast density on related cognitive and emotion outcomes before mandated breast density notification. Social Science & Medicine. 2016;169:171–179.
Davis TC, Arnold C, Berkel H, Nandy I, Jackson RH, Glass J. Knowledge and attitude on screening mammography among low-literate, low-income women. Cancer. 1996;78(9):1912–1920.
Orom H, Kiviniemi MT, Shavers VL, Ross L, Underwood W, 3rd. Perceived risk for breast cancer and its relationship to mammography in Blacks, Hispanics, and Whites. Journal of behavioral medicine. 2013;36(5):466–476.
Pagan JA, Brown CJ, Asch DA, Armstrong K, Bastida E, Guerra C. Health literacy and breast cancer screening among Mexican American women in South Texas. Journal of cancer education : the official journal of the American Association for Cancer Education. 2012;27(1):132–137.
Miles RC, Lehman C, Warner E, Tuttle A, Saksena M. Patient-Reported Breast Density Awareness and Knowledge after Breast Density Legislation Passage. Acad Radiol. 2019;26(6):726–731.
Manning M, Purrington K, Penner L, Duric N, Albrecht TL. Between-race differences in the effects of breast density information and information about new imaging technology on breast-health decision-making. Patient Education and Counseling. 2016;99(6):1002–1010.
Hunt BR, Whitman S, Hurlbert MS. Increasing Black:White disparities in breast cancer mortality in the 50 largest cities in the United States. Cancer epidemiology. 2014;38(2):118–123.
Jemal A, Ward EM, Johnson CJ, et al. Annual Report to the Nation on the Status of Cancer, 1975–2014, Featuring Survival. JNCI: Journal of the National Cancer Institute. 2017;109(9):djx030.
Bickmore TW, Pfeifer LM, Paasche-Orlow MK. Using computer agents to explain medical documents to patients with low health literacy. Patient education and counseling. 2009;75(3):315–320.
Cauell J, Bickmore T, Campbell L, Vihjalmsson H. Designing Embodied Conversational Agents. Cambridge, MA: MIT Press; 2000.
Olafsson S, O'Leary T, Bickmore T. Coerced Change-talk with Conversational Agents Promotes Confidence in Behavior Change. Proceedings of the 13th EAI International Conference on Pervasive Computing Technologies for Healthcare; 2019; Trento, Italy.
Zhang Z, Bickmore TW. Medical Shared Decision Making with a Virtual Agent. In Proceedings of Intelligent Virtual Agents. ACM; 2018; Sydney, Australia.
Bickmore TW, Silliman RA, Nelson K, et al. A Randomized Controlled Trial of an Automated Exercise Coach for Older Adults. Journal of the American Geriatrics Society. 2013;61(10):1676–1683.
Abstracts from the 2019 Annual Meeting of the Society of General Internal Medicine. Journal of General Internal Medicine. 2019;34(2):99–867.
Gunn C, Kennedy M, Maschke A, Fishman M, Hopkins M, Warner E. Partnering with Advocates to Assess Breast Density Education Materials. Paper presented at: Society for General Internal Medicine2019; Washington, DC.
Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)—A metadata-driven methodology and workflow process for providing translational research informatics support. Journal of Biomedical Informatics. 2009;42(2):377–381.
Knafl K, Deatrick J, Gallo A, et al. The Analysis and Interpretation of Cognitive Interviews for Instrument Development. Research in Nursing and Health. 2007;30:224–234.
Ridolfo H, Schoua-Glusberg A. Analyzing Cognitive Interview Data Using the Constant Comparative Method of Analysis to Understand Cross-Cultural Patterns in Survey Data. Field Methods. 2011;23(4):420–438.
Bastable SB. Health professional as educator : principles of teaching and learning. Sudbury, MA: Sudbury, MA : Jones & Bartlett Learning; 2011.
Consedine NS, Magai C, Krivoshekova YS, Ryzewicz L, Neugut AI. Fear, Anxiety, Worry, and Breast Cancer Screening Behavior: A Critical Review. Cancer Epidemiology Biomarkers & Prevention. 2004;13(4):501–510.
Watson EK, Henderson BJ, Brett J, Bankhead C, Austoker J. The psychological impact of mammographic screening on women with a family history of breast cancer—a systematic review. Psycho-Oncology. 2005;14(11):939–948.
Lerman C, Trock B, Rimer BK, Jepson C, Brody D, Boyce A. Psychological side effects of breast cancer screening. Health psychology : official journal of the Division of Health Psychology, American Psychological Association. 1991;10(4):259–267.
Tosteson AN, Fryback DG, Hammond CS, et al. Consequences of false-positive screening mammograms. JAMA Intern Med. 2014;174(6):954–961.
Dolan NC, Feinglass J, Priyanath A, Haviley C, Sorensen AV, Venta LA. Measuring Satisfaction with Mammography Results Reporting. Journal of General Internal Medicine. 2001;16(3):157–162.
Karliner LS, Kaplan CP, Juarbe T, Pasick R, Pérez-Stable EJ. Poor Patient Comprehension of Abnormal Mammography Results. Journal of General Internal Medicine. 2005;20(5):432–437.
Anderson EE, Hoskins KJ. Individual Breast Cancer Risk Assessment in Underserved Populations: Integrating Empirical Bioethics and Health Disparities Research. Journal of Health Care for the Poor and Underserved. 2012;23(4):34–46.
Kaplan CP, Livaudais-Toman J, Tice JA, et al. A Randomized, Controlled Trial to Increase Discussion of Breast Cancer in Primary Care. Cancer Epidemiology Biomarkers & Prevention. 2014;23(7):1245–1253.
Nayak L, Miyake KK, Leung JWT, et al. Impact of Breast Density Legislation on Breast Cancer Risk Assessment and Supplemental Screening: A Survey of 110 Radiology Facilities. The Breast Journal. 2016;22(5):493–500.
Sabatino SA, McCarthy EP, Phillips RS, Burns RB. Breast cancer risk assessment and management in primary care: Provider attitudes, practices, and barriers. Cancer Detection and Prevention. 2007;31(5):375–383.
Cortez S, Milbrandt M, Kaphingst KA, James A, Colditz G. The readability of online breast cancer risk assessment tools. Breast Cancer Res Treat. 2015;154(1):191–199.
Hesse-Biber S, Flynn B, Farrelly K. The Pink Underside: The Commercialization of Medical Risk Assessment and Decision-Making Tools for Hereditary Breast Cancer Risk. Qualitative Health Research. 2018;28(10):1523–1538.
Joseph G, Beattie M, Lee R, et al. Pre-counseling Education for Low Literacy Women at Risk of Hereditary Breast and Ovarian Cancer (HBOC): Patient Experiences Using the Cancer Risk Education Intervention Tool (CREdIT). Journal of Genetic Counseling. 2010;19:447–462.
Joseph-Williams N, Newcombe R, Politi M, et al. Toward minimum standards for certifying patient decision aids: A modified Delphi consensus process. Medical Decision Making. 2014;34:699–710.
Bickmore T, Trinh H, Olafsson S, et al. Patient and Consumer Safety Risks When Using Conversational Assistants for Medical Information: An Observational Study of Siri, Alexa, and Google Assistant. Journal of Medical Internet Research. 2018;20(9):e11510.
George S, Duran N, Norris K. A Systematic Review of Barriers and Facilitators to Minority Research Participation Among African Americans, Latinos, Asian Americans, and Pacific Islanders. American Journal of Public Health. 2014;104(2):e16-e31.
Watts T, Merrell J, Murphy F, Williams A. Breast health information needs of women from minority ethnic groups. Journal of Advanced Nursing. 2004;47(5):526–535.
Acknowledgments
The authors would like to thank members of the Pink and Black Education and Support Network in Boston, MA, for their thoughtful feedback and contribution to the design of the computer-animated agent.
Funding
Funding for this work was provided by the American Cancer Society (IRG-17-176-39). Dr. Gunn’s effort was supported in part by the National Cancer Institute (1K07CA221899). Dr. Warner’s work was supported in part by the National Cancer Institute (K01CA188075).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
This research was reviewed and approved by the Boston Medical Center Institutional Review Board.
Conflict of Interest
The following authors have no conflicts of interest: Dr. Christine Gunn, Ms. Ariel Maschke, Dr. Timothy Bickmore, Mr. Mark Kennedy, Ms. Margaret Hopkins, Dr. Michael Paashe-Orlow, and Dr. Erica Warner. Dr. Michael Fishman is a consultant for Zebra Medical Vision and a member of the Scientific Advisory Board for Hologic.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Prior Presentations: Preliminary results were previously presented at the International Breast Density and Cancer Risk Assessment Workshop on June 6, 2019, in Honolulu, Hawaii, and at the Society for General Internal Medicine Annual Meeting on May 9, 2019, in Washington D.C.
Rights and permissions
About this article

Cite this article
Gunn, C., Maschke, A., Bickmore, T. et al. Acceptability of an Interactive Computer-Animated Agent to Promote Patient-Provider Communication About Breast Density: a Mixed Method Pilot Study. J GEN INTERN MED 35, 1069–1077 (2020). https://doi.org/10.1007/s11606-019-05622-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-019-05622-2