
Abstract
Background
A challenge to reducing overuse of health services is communicating recommendations against unnecessary health services to patients. The predominant approach has been to highlight the limited benefit and potential harm of such services for that patient, but the prudent use of health resources can also benefit others. Whether appealing to patient altruism can reduce overuse is unknown.
Objective
To determine whether altruistic appeals reduce hypothetical requests for overused services and affect physician ratings.
Design
Experimental survey using hypothetical vignettes describing three overused health services (antibiotics for acute sinusitis, imaging for acute low back pain, and annual exams for healthy adults).
Participants
U.S. adults recruited from Research Now, an online panel of individuals compensated for performing academic and marketing research surveys.
Interventions
In the control version of the vignettes, the physician’s rationale for recommending against the service was the minimal benefit and potential for harm. In the altruism version, the rationale additionally included potential benefit to others by forgoing that service.
Main Measures
Differences in requests for overused services and physician ratings between participants randomized to the control and altruism versions of the vignettes.
Key Results
A total of 1001 participants were included in the final analyses. There were no significant differences in requests for overused services for any of the clinical scenarios (P values ranged from 0.183 to 0.547). Physician ratings were lower in the altruism version for the acute sinusitis (6.68 vs. 7.03, P = 0.012) and back pain scenarios (6.14 vs. 6.83, P < 0.001), and marginally lower for the healthy adult scenario (5.27 vs. 5.57, P = 0.084).
Conclusions
In this experimental survey, altruistic appeals delivered by physicians did not reduce requests for overused services, and resulted in more negative physician ratings. Further studies are warranted to determine whether alternative methods of appealing to patient altruism can reduce overuse.
Similar content being viewed by others


INTRODUCTION
Containing health care costs and improving quality are important goals of ongoing health care reforms.1 One approach to achieving these goals is reducing overuse—services provided under circumstances in which the potential for harm exceeds the possible benefit.2 Payment reform models such as bundled payments and accountable care organizations aim to reduce structural incentives for overuse.3 Additionally, sustained efforts to highlight the lack of benefit of some common practices are ongoing. Notably, in the Choosing Wisely Campaign, professional societies have created lists of specific services that are often unnecessary.4
A major obstacle to reducing overuse is getting patients and physicians to forgo those services.5 , 6 Patients may assume that more health care is better,7 and patient satisfaction is increasingly being used as a metric to judge physicians’ quality of care, so physicians may be hesitant to say “no.”8 , 9 The approach taken thus far by Choosing Wisely and other educational campaigns has been to appeal to the enlightened self-interest of patients: greater knowledge about what actually improves their health will reduce patient demand for unnecessary medical care. However, most of the tests and treatments highlighted by Choosing Wisely are not overtly harmful, and instead are equivocal or have trivial benefits.10 Early evidence on the effect of the Choosing Wisely campaign has not been promising,11 and one factor may be the difficulty in convincing patients to accept the notion that forgoing “unnecessary” care is actually in their best interest.
A complementary approach to appealing to patients’ self-interest would be to appeal to the impact of their health care choices on the well-being of others—an appeal to patient altruism. Altruism plays a role in vaccination,12 blood and organ donation,13 and participation in clinical research,14 but it rarely plays a role in routine medical practice. Some might be concerned that encouraging patient altruism would conflict with medicine’s long-standing ethic of the primacy of individual patient well-being. However, Choosing Wisely was motivated in part by the Charter on Medical Professionalism,15 which includes a commitment to just distribution of finite resources,16 so Choosing Wisely was implicitly motivated by improving societal well-being, not just the well-being of particular patients. Ethicists have argued that altruistic patient decisions could reflect a number of legitimate motivations and should be respected.17 Moreover, it is increasingly recognized that patients should play a role in the stewardship of limited resources.18
Whether explicit appeals to patient altruism would be effective in reducing overuse and would be acceptable to patients is unknown. To examine this question, we conducted an experimental survey with hypothetical vignettes where physicians explained the rationale to forgo an overused service with exclusively self-interested reasons or additionally highlighted the potential benefit to others. We hypothesized that altruistic appeals would reduce requests for overused health services and would result in non-inferior physician ratings.
METHODS
Participants
Study participants were U.S. adults aged 18 years and older recruited through the online research company Research Now. Research Now has enrolled a panel of participants and compensates them using a points-based reward program for completing academic and marketing research surveys. Research Now samples have been used in other published health-related studies.19 , 20 We used quota sampling based on geography, gender, age, race, and ethnicity to recruit a sample that approximated the U.S. population on these measures. Additional demographics and self-reported health status were also obtained.
Survey Instrument and Development
After answering demographic questions, participants were shown three vignettes asking them to imagine that they were seeing a physician about a common health condition. We chose scenarios that were common and applicable to both genders and all age ranges (antibiotics for acute sinusitis, imaging for acute low back pain, and annual exams for healthy adults). The full text of the vignette about antibiotics for acute sinusitis is shown in the Text Box, and the others are shown in the Online Appendix. Each scenario was based on a Choosing Wisely recommendation.21
Text Box Clinical Vignette about Antibiotics for Acute Sinusitis

In each vignette, the physician discussed the overused health service and ultimately recommended against it, while emphasizing that receiving the service was ultimately the patient’s decision. In the control version of the vignettes, the physician’s rationale for the recommendation focused exclusively on the patient’s self-interest, explaining that the service offered minimal benefits and a potential for harm. For example, in the antibiotics for acute sinusitis scenario, the physician highlighted the high prevalence of viral infections for which antibiotics would be ineffective and the risk for upset stomach and diarrhea from taking antibiotics. In the altruism version, the physician’s rationale included the same language as the control version, as well as a short statement highlighting the potential to benefit others by forgoing the service. In the antibiotics case, the physician highlighted that limiting unnecessary antibiotic use would reduce antibiotic resistance. We asked participants to indicate whether they would request the service using a four-point Likert scale (definitely yes, probably yes, probably no, definitely no) and to rate the physician on a scale of 0 to 10 (using a question adapted from the Consumer Assessment of Healthcare Providers and Systems survey22). Participants were randomized in a 1:1 ratio to the control and altruism versions of the vignettes. Participants were shown the same version of all three vignettes in varying order. After each vignette, we asked participants whether they had personal experience with the condition and treatment.
After the vignettes, we asked follow-up questions about values and attitudes that might moderate the effect of altruistic appeals. We asked four questions about attitudes regarding health care costs. Since individuals who are generally more altruistic may be more receptive to altruistic appeals, we asked four questions about altruism attitudes using items from the General Social Survey.23 Those questions used a five-point Likert scale, and responses were used to construct an altruism attitudes score that ranged from 4 (least altruistic) to 20 (most altruistic).
The survey required a response to all items, with the exception of the option to choose “prefer not to answer” for several of the demographics questions. All data collection was managed by Research Now. Surveys were excluded if they were started but not completed. Surveys were also excluded on the basis of quality assurance if they were completed in less than one-third of the median completion time (<1.9 min). This study was ruled exempt by the institutional review board at the Johns Hopkins Bloomberg School of Public Health.
The clinical vignettes and questions about attitudes on health care costs were developed by the authors for this study. We performed cognitive interviews to assess for clarity and interpretation, and pilot-tested the questions using a convenience panel from Amazon Mechanical Turk to assess for floor and ceiling effects.
Statistical Analysis
We tested whether participant characteristics matched U.S. population characteristics using chi-square tests. We also tested the effectiveness of randomization by comparing characteristics of participants in the experimental and control arms of the study with two-sample t tests for continuous variables and chi-square tests for categorical variables.
To determine the effectiveness of altruistic appeals in reducing respondent requests for overused health services, we compared respondent requests in the control and altruism versions using the Wilcoxon rank-sum test (for non-parametric ordinal data), with two-sided P < 0.05 considered statistically significant. Each vignette was evaluated separately.
To determine the effect of altruistic appeals on physician ratings, we compared physician ratings in the control and altruism versions. Since our hypothesis was that the ratings would be equivalent, our primary analysis was for non-inferiority.24 The non-inferiority margin was set at an absolute difference of 0.4. This value was chosen to correspond with a Cohen’s d (difference of means divided by standard deviation) of 0.2, which is consistent with a small effect size.25 Our estimate of standard deviation was based on the standard deviation of this measure in a prior study.26 The criterion for non-inferiority was that the lower bound of the 95% confidence interval of between-group effect sizes should fall within this range. We also performed a superiority analysis using the t test, with two-sided P < 0.05 considered significant. Each vignette was evaluated separately.
We also performed several exploratory analyses. To determine whether respondent characteristics were associated with requests for overused services, we constructed logistic regression models with dichotomized outcome (did or did not request service) that included the characteristic of interest and adjusted for age, sex, race/ethnicity, altruism randomization group, and clinical scenario. To determine whether respondent characteristics were associated with physician ratings, we constructed linear regression models that included the characteristic of interest and adjusted for age, sex, race/ethnicity, altruism randomization group, and clinical scenario. To determine whether respondent characteristics moderated the effect of appealing to altruism, we repeated the above analyses and included an interaction variable between altruism randomization group and the characteristic of interest. In order to increase the power for these exploratory analyses, we combined responses across the three clinical scenarios. All models accounted for clustering of responses to the clinical scenarios among individual participants. We used the two-sided Wald test to determine whether the interaction parameter was statistically significant, with P < 0.05 considered significant. All analyses were performed using Stata version 13.1 software (StataCorp LP, College Station, TX).
RESULTS
The final analyses included 1001 participants. Responses were not included from 4025 participants who answered screening demographic questions and were not invited to complete the survey because of the quota or failure to meet age eligibility, 153 participants who started the survey but did not complete it, and 9 participants who completed the survey but did so too quickly.
Respondent characteristics are shown in Table 1 and Online Appendix Table 1. All characteristics were balanced between the control and altruism groups except for political ideology (altruism group was 39.4% conservative vs. 31.4% control, P < 0.05). In general, our sample closely resembled the U.S. population in age, gender, race and ethnicity, and geography, although our sample was wealthier and more educated than the general population (data not shown).
The effect of altruistic appeals on the request for overused services is shown in Table 2. There was no significant difference between the control and altruism versions for any of the clinical scenarios (P values ranged from 0.183 to 0.547).
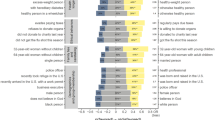
The effect of altruistic appeals on physician ratings is shown in Figure 1. Non-inferiority for the altruism group was not achieved for any of the clinical scenarios. In superiority testing, physician ratings were lower in the altruism group for the acute sinusitis (6.68 vs. 7.03, P = 0.012) and back pain scenarios (6.14 vs. 6.83, P < 0.001), and marginally lower for the healthy adults scenario (5.27 vs. 5.57, P = 0.084).

Physician ratings in hypothetical clinical vignettes. The dotted line represents the non-inferiority margin.
Responses to the questions about cost attitudes are shown in Table 3. There was strong agreement with statements indicating that cost is a major problem, that both physicians and patients should play a role in containing costs, and that patients can help contain costs by not using tests and treatments with limited benefits, with at least 75% of participants somewhat or strongly agreeing with each question.
The results of our exploratory analyses are shown in Online Appendix Tables 2 and 3. Notably, prior experience with the overused service was associated with a higher likelihood of requesting the overused service, and agreement with each cost attitude statement except “Health care costs are a major problem in the U.S.” was associated with a lower likelihood of requesting the overused services and higher physician ratings in adjusted analyses. There was no evidence of effect modification by any of the respondent characteristics for either the requests for overused services (P values ranged from 0.118 to 0.944) or physician ratings (P values ranged from 0.070 to 0.890, data not shown).
DISCUSSION
In this experimental survey study, altruistic appeals that highlighted the potential benefit to others by forgoing common overused health services did not reduce requests for these services. Contrary to our hypothesis, the altruistic appeals resulted in more negative physician ratings.
While altruistic appeals had no effect on hypothetical decisions in this study, they have shown the potential to alter behavior in other health care situations. For example, in one experimental survey, participants were more likely to indicate that they would receive a vaccination as the potential to benefit others (through herd immunity) increased.27 In another study, blood donors exposed to messaging that highlighted the altruistic reasons for donating blood just prior to their donation were more likely to indicate their likelihood to donate again than those exposed to messaging that highlighted personal benefits of donating.28
We offer several possible explanations for the lack of effect of altruistic appeals on treatment decisions in the current study. First, appeals to altruistic or prosocial motives are more likely to be effective when the “costs” are relatively low.29 In the above examples, the cost of altruism was additional action (i.e., receipt of vaccination or donation of blood) with a small potential downside. In contrast, the cost of altruism in the current study involved giving up some potential health benefit. Patients may be more sensitive to the costs of altruism (however small) when they involve giving up a treatment versus taking positive action, corresponding to the behavioral economics principle of loss aversion.30
Second, considering others in personal health care decisions may not be a widely accepted norm. Appeals to altruism can affect decisions by highlighting norms that people already recognize as important (norm salience).29 For example, signs that discourage littering are effective in part because of the widely accepted norm against littering.31 The fact that over 75% of participants agreed that patients should not request tests and treatments that are unlikely to be beneficial as a means of controlling costs suggests that such an altruistic norm may exist. However, the attitude questions were asked after the vignettes, potentially introducing social desirability bias.
Our finding that altruistic appeals resulted in lower physician ratings has several explanations. Participants may have felt that the altruistic appeals were motivated by cost considerations. Only one of the altruism rationales included an explicit cost consideration (the back pain scenario), although participants may have assumed that the other altruism rationales included implicit cost considerations. While more than 75% of participants agreed that it is “okay” for physicians to recommend against tests and treatments that are unlikely to be beneficial in order to help control health care costs, prior studies have shown that patients may feel uncomfortable with their physicians considering societal costs.32 Alternatively, participants may not have been accustomed to receiving altruistic appeals from physicians, and found them judgmental or moralistic, or just “unusual” behavior for physicians that warranted a lower rating. Altruistic messages may be better received coming from someone other than the physician.
Several of the findings in our exploratory analyses have important policy implications. While the public has long expressed concern about rising national health care costs, and media coverage has emphasized the problem of cost growth, participants’ belief that health care costs are a problem was not associated with a decreased likelihood of requesting the overused service. Conversely, participants’ attitudes corresponding to the permissibility of physicians considering costs, the responsibility of patients to consider costs, and individual self-efficacy to positively impact costs through wise use of resources were each associated with reduced likelihood of requesting overused services. Although we did not test the causal effect of more nuanced messages highlighting these themes, it is possible that these messages would be more effective in inducing the public to “choose wisely.”
Additionally, we found that prior receipt of the overused services was strongly associated with requesting that service in the vignette. The therapeutic illusion33—the false belief that an ineffective treatment was responsible for a positive outcome—can contribute to a cycle that reinforces demand for overused services. Therefore, efforts to avoid overuse in one instance could also reduce future overuse. Research is needed to identify strategies for addressing the therapeutic illusion among patients who have previously had positive experiences with unnecessary services.
The high rate of hypothetical requests for overused services in this study underscores the urgent need for more research on effective methods for physicians to communicate recommendations against equivocal services. It is not surprising that annual exams were requested by approximately 80% of participants. The Society of General Internal Medicine’s recommendation against routine general health checks for asymptomatic adults was met with some controversy among physicians34 , 35 and even the society itself.36 On the other hand, it is arguably more concerning that nearly 40% of participants would request antibiotics for acute sinusitis even if their physician recommended against them, given that the CDC and other groups have been engaged in public education campaigns since the 1990s.37
This study has several limitations. First, responses to hypothetical scenarios may not correspond with actual decisions that patients would make when facing these clinical problems, or the attitudes they would have toward physicians communicating to them about altruism in the context of clinical interactions. However, using hypothetical scenarios allows for isolating the effect of subtle changes in communication that would be difficult in actual clinical encounters. Second, we included only three clinical scenarios, and our findings may not represent the effect of altruistic appeals in other situations. We chose common services that would be familiar, but a tradeoff for familiarity may be preconceived notions about the services that information in a short vignette is not able to change. Third, we developed the clinical scenarios for this study, and the self-interested and altruistic factors that we highlighted may not reflect the factors that most patients consider important for their clinical decision-making. We attempted to present a realistic description of risks and benefits, and present the benefits to others that we believed to be most salient, although presenting different information about these factors could lead to different results.
CONCLUSION
In this study, altruistic appeals delivered by physicians did not reduce requests for overused services, and resulted in more negative physician ratings. However, reducing overuse remains a priority for improving quality and controlling health care costs, and appealing to patient altruism remains a relatively unexplored strategy for reducing overuse. Further studies are warranted to determine whether alternative methods of appealing to patient altruism can reduce overuse while fostering positive patient–physician relationships.
References
Berwick DM, Nolan TW, Whittington J. The triple aim: care, health, and cost. Health Aff (Millwood). 2008;27(3):759–69.
Chassin MR, Galvin RW, National Roundtable on Health Care Quality. The urgent need to improve health care quality: institute of medicine national roundtable on health care quality. JAMA. 1998;280(11):1000–5.
Fisher ES, Shortell SM. Accountable care organizations: accountable for what, to whom, and how. JAMA. 2010;304(15):1715–6.
Cassel CK, Guest JA. Choosing wisely: helping physicians and patients make smart decisions about their care. JAMA. 2012;307(17):1801–2.
Roman BR, Asch DA. Faded promises: the challenge of deadopting low-value care. Ann Intern Med. 2014;161(2):149–50.
Ubel PA, Asch DA. Creating value in health by understanding and overcoming resistance to de-innovation. Health Aff (Millwood). 2015;34(2):239–44.
Carman KL, Maurer M, Yegian JM, et al. Evidence that consumers are skeptical about evidence-based health care. Health Aff (Millwood). 2010;29(7):1400–6.
Brett AS, McCullough LB. Addressing requests by patients for nonbeneficial interventions. JAMA. 2012;307(2):149–50.
Kupfer JM, Bond EU. Patient satisfaction and patient-centered care: necessary but not equal. JAMA. 2012;308(2):139–40.
Gliwa C, Pearson SD. Evidentiary rationales for the choosing wisely top 5 lists. JAMA. 2014;311(14):1443–4.
Rosenberg A, Agiro A, Gottlieb M, et al. Early trends among seven recommendations from the choosing wisely campaign. JAMA Intern Med. 2015;175(12):1913–20.
Hershey JC, Asch DA, Thumasathit T, Meszaros J, Waters VV. The roles of altruism, free riding, and bandwagoning in vaccination decisions. Organ Behav Hum Decis Process. 1994;59(2):177–87.
Jasper JD, Nickerson CA, Ubel PA, Asch DA. Altruism, incentives, and organ donation: attitudes of the transplant community. Med Care. 2004;42(4):378–86.
Jansen LA. The ethics of altruism in clinical research. Hast Cent Rep. 2009;39(4):26–36.
Wolfson D, Santa J, Slass L. Engaging physicians and consumers in conversations about treatment overuse and waste: a short history of the choosing wisely campaign. Acad Med. 2014;89(7):990–5.
American Board of Internal Medicine Foundation, American College of Physicians – American Society of Internal Medicine Foundation, European Federation of Internal Medicine. Medical professionalism in the new millennium: a physician charter. Ann Intern Med. 2002;136(3):243–6.
Doukas DJ, Hardwig J. Patient informed choice for altruism. Camb Q Healthc Ethics. 2014;23(4):397–402.
Reuben DB, Cassel CK. Physician stewardship of health care in an era of finite resources. JAMA. 2011;306(4):430–1.
Cho MK, Magnus D, Constantine M, et al. Attitudes toward risk and informed consent for research on medical practices: a cross-sectional survey. Ann Intern Med. 2015;162(10):690–6.
Khare S, Hajat S, Kovats S, et al. Heat protection behaviour in the UK: results of an online survey after the 2013 heatwave. BMC Public Health. 2015;15(1):1–12.
Potosky AL, Malin JL, Kim B, et al. Use of colony-stimulating factors with chemotherapy: opportunities for cost savings and improved outcomes. J Natl Cancer Inst. 2011;103(12):979–82.
Agency for Healthcare Research and Quality. CAHPS: Surveys and Tools to Advance Patient-Centered Care. http://www.ahrq.gov/cahps/index.html. Accessed August 18, 2016.
Smith TW. Altruism and Empathy in America: Trends and Correlates. Chicago, IL: National Opinion Research Center; 2006.
Kaji AH, Lewis RJ. Noninferiority trials: is a new treatment almost as effective as another? JAMA. 2015;313(23):2371–2.
Sullivan GM, Feinn R. Using effect size-or why the P value is not enough. J Grad Med Educ. 2012;4(3):279–82.
Weinick RM, Elliott MN, Volandes AE, Lopez L, Burkhart Q, Schlesinger M. Using standardized encounters to understand reported racial/ethnic disparities in patient experiences with care. Health Serv Res. 2011;46(2):491–509.
Vietri JT, Li M, Galvani AP, Chapman GB. Vaccinating to help ourselves and others. Med Dec Making. 2012;32(3):447–58.
Paulhus DL, Shaffer DR, Downing LL. Effects of making blood donor motives salient upon donor retention: a field experiment. Personal Soc Psychol Bull. 1976;3(1):99–102.
Batson CD, Powell AA. Altruism and prosocial behavior. In: Handbook of Psychology. Hoboken, NJ: Wiley; 2003:463–84.
Emanuel EJ, Ubel PA, Kessler JB, et al. Using behavioral economics to design physician incentives that deliver high-value care. Ann Intern Med. 2016;164(2):114–9.
Reiter SM, Samuel W. Littering as a function of prior litter and the presence or absence of prohibitive signs. J Appl Soc Psychol. 1980;10(1):45–55.
Sommers R, Goold SD, McGlynn EA, Pearson SD, Danis M. Focus groups highlight that many patients object to clinicians’ focusing on costs. Health Aff (Millwood). 2013;32(2):338–46.
Casarett D. The science of choosing wisely—overcoming the therapeutic illusion. N Engl J Med. 2016;374(13):1203–5.
Goroll AH. Toward trusting therapeutic relationships—in favor of the annual physical. N Engl J Med. 2015;373(16):1487–9.
Mehrotra A, Prochazka A. Improving value in health care—against the annual physical. N Engl J Med. 2015;373(16):1485–7.
Bass EB. Controversy about choosing wisely and creating value for patients. SGIM Forum. 2014;37(3):1–2.
Schwartz B. Preventing the spread of antimicrobial resistance among bacterial respiratory pathogens in industrialized countries: the case for judicious antimicrobial use. Clin Infect Dis. 1999;28(2):211–3.
Contributors
We would like to acknowledge assistance with the statistical analysis that was supported by the National Center for Research Resources and the National Center for Advancing Translational Sciences (NCATS) of the National Institutes of Health through grant number 1UL1TR001079.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they do not have a conflict of interest.
Funders
Dr. Riggs’s work on this manuscript was funded by NIH grant T32 HL007180 and the Society of General Internal Medicine Founders Grant.
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM 1
(DOCX 56 kb)
Rights and permissions
About this article

Cite this article
Riggs, K.R., Ubel, P.A. & Saloner, B. Can Appealing to Patient Altruism Reduce Overuse of Health Care Services? An Experimental Survey. J GEN INTERN MED 32, 732–738 (2017). https://doi.org/10.1007/s11606-017-4002-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-017-4002-5