
ABSTRACT
Background
The Affordable Care Act is designed to decrease the numbers of uninsured patients in U.S. However, even with insurance, patients who have financial hardships may have difficulty obtaining their medications because of cost issues.
Objective
Among patients with type 2 diabetes, to examine the association between patients’ self-reported financial pressures on cost-related medication non-adherence and glucose control. Additionally, to examine whether having insurance decrease the financial pressures of diabetes care.
Design and Participants
Racially/ethnically diverse patients (N = 1,361; 249 non-Hispanic whites, 194 Vietnamese, and 533 Mexican American) with type 2 diabetes were recruited from seven outpatient clinics for a cross-sectional, observational study.
Key Results
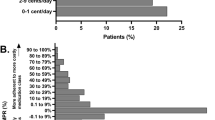
Although both Vietnamese and Mexican-American patients reported having low annual incomes, more Mexican Americans reported the presence of financial barriers to getting medical care and perceived financial burden due to their diabetes, compared to whites and Vietnamese (p < 0.001). Over half (53.2%) of Mexican Americans reported cost-related non-adherence compared to 27.2% of white and 27.6% of Vietnamese patients (p < 0.001). Perceived financial burden was found to be associated with poor glucose control (HbA1c ≥8%), after adjusting for sociodemographic and health characteristics (aOR = 1.70, 95%CI 1.09-2.63), but not when adjusting for non-adherence. Similarly, a significant association between presence of financial barriers and HbA1c (aOR = 1.69, 95%CI 1.23-2.32) was attenuated with the inclusion of insurance status in the model. Being uninsured (aOR = 1.90, 95%CI 1.13-3.21) and non-adherent (aOR = 1.49, 95%CI 1.06-2.08) were each independently associated with HbA1c.
Conclusions
While having health insurance coverage eliminated some of the financial barriers associated with having diabetes, low-income patients still faced significant financial burdens. Thus, providing health insurance to more individuals is only the first step towards eliminating health disparities. It is important to address medication cost in order to improve medication adherence and glucose control.
Similar content being viewed by others


References
DeNavas-Walt C, Proctor BD, Smith JC. Income, Poverty, and Health Insurance Coverage in the United States: 2009, in Current Population Reports, P60-238, U.S. Census Bureau, Editor. Washington, DC; 2010.
Kirby J, Taliaferro G, Zuvekas SH. Explaining racial and ethnic disparities in health care. Medical care. 2006;44(5):I-64–72.
Hargraves JL, Hadley J. The contribution of insurance coverage and community resources to reducing racial/ethnic disparities in access to care. Health Serv Res. 2003;38(3):809–829.
Heisler M, et al. Mechanisms for racial and ethnic disparities in glycemic control in middle-aged and older Americans in the health and retirement study. Arch Intern Med. 2007;167(17):1853–1860.
Harris MI. Racial and ethnic differences in health care access and health outcomes for adults with type 2 diabetes. Diabetes Care. 2001;24(3):454–9.
Piette JD, Heisler M, Wagner TH. Problems paying out-of-pocket medication costs among older adults with diabetes. Diabetes Care. 2004;27(2):384–391.
National Committee for Quality Assurance. Changes to the Diabetes Recognition Program. 2009; Available from: http://www.ncqa.org/tabid/1023/Default.aspx.
Agency for Healthcare Research and Quality (AHRQ). Medical Expenditure Panel Survey (MEPS) [cited 2010 December 15]; Available from: http://www.meps.ahrq.gov/mepsweb/.
Greenfield S, et al. The uses of outcomes research for medical effectiveness, quality of care, and reimbursement in type II diabetes. Diabetes Care. 1994;17(Suppl 1):32–9.
Soumerai SB. Cost-related medication nonadherence among elderly and disabled Medicare beneficiaries: a national survey 1 year before the Medicare drug benefit. Arch Intern Med. 2006;166(17):1829–35.
Safran DG, et al. Prescription drug coverage and seniors: findings from a 2003 national survey. Health Aff (Millwood). 2005, Suppl Web Exclusives, p. W5-152-W5-166.
Wilson IB, et al. Cost-related skipping of medications and other treatments among Medicare beneficiaries between 1998 and 2000. Results of a national study. J Gen Intern Med. 2005;20(8):715–20.
Radloff LS. The CES-D Scale: A self-report depression scale for research in the general population. Appl Psychol Meas. 1977;1(3):385–401.
Greenfield S. Development and testing of a new measure of case mix for use in office practice. Med Care. 1995;33(4):AS47–55.
Thom DH, et al. Further validation and reliability testing of the Trust in Physician Scale. The Stanford Trust Study Physicians. Med Care. 1999;37(5):510–7.
Bullinger M, et al. Translating health status questionnaires and evaluating their quality: the IQOLA Project approach. International quality of life assessment. J Clin Epidemiol. 1998;51(11):913–23.
Fowler FJ. Improving Survey Questions: Design and Evaluation. Newbury Park: Sage Publications; 1995.
Briesacher BA, Gurwitz JH, Soumerai SB. Patients at-risk for cost-related medication nonadherence: a review of the literature. J Gen Intern Med. 2007;22(6):864–71.
Piette JD, et al. The role of patient–physician trust in moderating medication nonadherence due to cost pressures. Arch Intern Med. 2005;165(15):1749–1755.
Kurlander JE, et al. Cost-related nonadherence to medications among patients with diabetes and chronic pain: factors beyond finances. Diabetes Care. 2009;32(12):2143–8.
Tseng CW, et al. Race/ethnicity and economic differences in cost-related medication underuse among insured adults with diabetes: the translating research into action for diabetes study. Diabetes Care. 2008;31(2):261–6.
Piette JD, Heisler M, Wagner TH. Medication characteristics beyond cost alone influence decisions to underuse pharmacotherapy in response to financial pressures. J Clin Epidemiol. 2006;59(7):739–46.
Wagner TH, Heisler M, Piette JD. Prescription drug co-payments and cost-related medication underuse. Health Econ Policy Law. 2008;3(Pt 1):51–67.
Piette JD, et al. Beliefs about prescription medications among patients with diabetes: variation across racial groups and influences on cost-related medication underuse. J Health Care Poor Underserved. 2010;21(1):349–61.
Acknowledgments
This work was supported by the Robert Wood Johnson Foundation (Generalist Physician Faculty Award #1051084 and Finding Answers: Disparities Research for Change #59758), the NovoNordisk Foundation, and the National Institute of Diabetes, Digestive and Kidney Diseases (R18DK69846 and K01DK078939). All authors have no relevant conflict of interest to disclose. Dr. Ngo-Metzger completed this work as an Associate Professor at the University of California, Irvine. The views expressed in this publication are solely the opinions of the authors and do not necessarily reflect the official policies of the U.S. Department of Health and Human Services (HHS) or the Health Resources and Services Administration (HRSA), nor does mention of the department or agency names imply endorsement by the U.S. Government.
Conflict of interest
None disclosed.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ngo-Metzger, Q., Sorkin, D.H., Billimek, J. et al. The Effects of Financial Pressures on Adherence and Glucose Control Among Racial/Ethnically Diverse Patients with Diabetes. J GEN INTERN MED 27, 432–437 (2012). https://doi.org/10.1007/s11606-011-1910-7
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-011-1910-7