
ABSTRACT
BACKGROUND
Readmissions cause significant distress to patients and considerable financial costs. Identifying hospitalized patients at high risk for readmission is an important strategy in reducing readmissions. We aimed to evaluate how well physicians, case managers, and nurses can predict whether their older patients will be readmitted and to compare their predictions to a standardized risk tool (Probability of Repeat Admission, or Pra).
METHODS
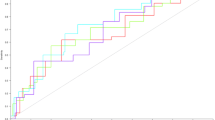
Patients aged ≥65 discharged from the general medical service at University of California, San Francisco Medical Center, a 550-bed tertiary care academic medical center, were eligible for enrollment over a 5-week period. At the time of discharge, the inpatient team members caring for each patient estimated the chance of unscheduled readmission within 30 days and predicted the reason for potential readmission. We also calculated the Pra for each patient. We identified readmissions through electronic medical record (EMR) review and phone calls with patients/caregivers. Discrimination was determined by creating ROC curves for each provider group and the Pra.
RESULTS
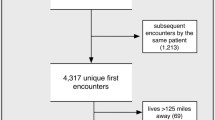
One hundred sixty-four patients were eligible for enrollment. Of these patients, five died during the 30-day period post-discharge. Of the remaining 159 patients, 52 patients (32.7%) were readmitted. Mean readmission predictions for the physician providers were closest to the actual readmission rate, while case managers, nurses, and the Pra all overestimated readmissions. The ability to discriminate between readmissions and non-readmissions was poor for all provider groups and the Pra (AUC from 0.50 for case managers to 0.59 for interns, 0.56 for Pra). None of the provider groups predicted the reason for readmission with accuracy.
CONCLUSIONS
This study found (1) overall readmission rates were higher than previously reported, possibly because we employed a more thorough follow-up methodology, and (2) neither providers nor a published algorithm were able to accurately predict which patients were at highest risk of readmission. Amid increasing pressure to reduce readmission rates, hospitals do not have accurate predictive tools to guide their efforts.


Similar content being viewed by others

References
A New Era of Responsibility: Renewing America’s Promise. http://www.whitehouse.gov/omb/assets/fy2010_new_era/A_New_Era_of_Responsibility2.pdf. Accessed February 2, 2011.
U.S. Department of Health & Human Services. http://www.hospitalcompare.hhs.gov. Accessed February 2, 2011.
University HealthSystem Consortium. https://www.uhc.edu/. Accessed February 2, 2011.
A path to bundled payment around a rehospitalization.: Medicare payment Advisory Commission; June 2005.
Copeland-Fields L, Griffin T, Jenkins T, Buckley M, Wise LC. Comparison of outcome predictions made by physicians, by nurses, and by using the Mortality Prediction Model. Am J Crit Care. 2001;10(5):313–319.
Ebell MH, Bergus GR, Warbasse L, Bloomer R. The inability of physicians to predict the outcome of in-hospital resuscitation. J Gen Intern Med. 1996;11(1):16–22.
Eriksen BO, Kristiansen IS, Pape JF. Prediction of five-year survival for patients admitted to a department of internal medicine. J Intern Med. 2001;250(5):435–440.
Gusmao Vicente F, Polito Lomar F, Melot C, Vincent JL. Can the experienced ICU physician predict ICU length of stay and outcome better than less experienced colleagues? Intensive Care Med. 2004;30(4):655–659.
Pierpont GL, Parenti CM. Physician risk assessment and APACHE scores in cardiac care units. Clin Cardiol. 1999;22(5):366–368.
Poses RM, Smith WR, McClish DK, et al. Physicians’ survival predictions for patients with acute congestive heart failure. Arch Intern Med. 199;157(9):1001–1007.
Boult C, Dowd B, McCaffrey D, Boult L, Hernandez R, Krulewitch H. Screening elders for risk of hospital admission. J Am Geriatr Soc. 1993;41(8):811–817.
Novotny NL, Anderson MA. Prediction of early readmission in medical inpatients using the Probability of Repeated Admission instrument. Nurs Res. 2008;57(6):406–415.
Centor RM, Schwartz JS. An evaluation of methods for estimating the area under the receiver operating characteristic (ROC) curve. Med Decis Making Summer. 1985;5(2):149–156.
Hosmer DW, Lemeshow S.Applied Logistic Regression. 2nd ed. NY: John Wiley & Sons Inc.; 2000.
Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360(14):1418–1428.
Yamokoski LM, Hasselblad V, Moser DK, et al. Prediction of rehospitalization and death in severe heart failure by physicians and nurses of the ESCAPE trial. J Card Fail. 2007;13(1):8–13.
Dobrzanska L, Newell R. Readmissions: a primary care examination of reasons for readmission of older people and possible readmission risk factors. J Clin Nurs. 2006;15(5):599–606.
Laniece I, Couturier P, Drame M, et al. Incidence and main factors associated with early unplanned hospital readmission among French medical inpatients aged 75 and over admitted through emergency units. Age Ageing. 2008;37(4):416–422.
Grant RW, Charlebois ED, Wachter RM. Risk factors for early hospital readmission in patients with AIDS and pneumonia. J Gen Intern Med. 1999;14(9):531–536.
Murphy BM, Elliott PC, Le Grande MR, et al. Living alone predicts 30-day hospital readmission after coronary artery bypass graft surgery. Eur J Cardiovasc Prev Rehabil. 2008;15(2):210–215.
Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW. The incidence and severity of adverse events affecting patients after discharge from the hospital. Ann Intern Med. 2003;138(3):161–167.
Forster AJ, Murff HJ, Peterson JF, Gandhi TK, Bates DW. Adverse drug events occurring following hospital discharge. J Gen Intern Med. 2005;20(4):317–323.
Pippins JR, Gandhi TK, Hamann C, et al. Classifying and predicting errors of inpatient medication reconciliation. J Gen Intern Med. 2008;23(9):1414–1422.
Polanczyk CA, Newton C, Dec GW, Di Salvo TG. Quality of care and hospital readmission in congestive heart failure: an explicit review process. J Card Fail. 2001;7(4):289–298.
Coleman EA, Parry C, Chalmers S, Min SJ. The care transitions intervention: results of a randomized controlled trial. Arch Intern Med. 2006;166(17):1822–1828.
Koehler BE, Richter KM, Youngblood L, et al. Reduction of 30-day postdischarge hospital readmission or emergency department (ED) visit rates in high-risk elderly medical patients through delivery of a targeted care bundle. J Hosp Med. 2009;4(4):211–218.
Woodend AK, Sherrard H, Fraser M, Stuewe L, Cheung T, Struthers C. Telehome monitoring in patients with cardiac disease who are at high risk of readmission. Heart Lung. 2008;37(1):36–45.
Tibaldi V, Isaia G, Scarafiotti C, et al. Hospital at home for elderly patients with acute decompensation of chronic heart failure: a prospective randomized controlled trial. Arch Intern Med. 2009;169(17):1569–1575.
Hasan O, Meltzer DO, Shaykevich SA, et al. Hospital readmission in general medicine patients: a prediction model. J Gen Intern Med. Mar; 25(3):211–219
Acknowledgements
None.
Conflict of interest
None disclosed.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Allaudeen, N., Schnipper, J.L., Orav, E.J. et al. Inability of Providers to Predict Unplanned Readmissions. J GEN INTERN MED 26, 771–776 (2011). https://doi.org/10.1007/s11606-011-1663-3
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-011-1663-3