
ABSTRACT
Background
Hepatitis B virus (HBV) DNA and alanine aminotransferase (ALT) levels predict future complications in chronic hepatitis B (CHB) patients. To determine when to initiate antiviral therapy, treatment guidelines recommend monitoring of HBV DNA and ALT levels at least annually. This study aimed to assess adherence to treatment guideline-recommended monitoring of CHB patients not receiving antiviral treatment and to identify predictors of laboratory monitoring and subsequent initiation of antiviral therapy.
Methods
This retrospective cohort study used data from a large US health care claims database over a 5-year period (January 1, 2003 to December 31, 2007). The study population included patients 18–65 years of age with at least two paid medical claims with an ICD-9 code for CHB, at least one positive hepatitis B surface antigen test, and at least 12 months of continuous health plan enrollment after initial diagnosis. Descriptive statistics assessed the proportion of patients with claims for ALT and/or HBV DNA monitoring. Multivariate logistic regression models were used to determine predictors of monitoring and subsequent antiviral therapy.
Results
The study included 1,168 CHB patients, with a mean follow-up of 728 days (median = 696 days). The proportion monitored at least every 12 months was 53.3% for ALT, 39.0% for HBV DNA, and 35.1% for both. Significant predictors of monitoring were a higher Deyo-Charlson Comorbidity Index (DCCI) score for ALT (OR 1.90, p < 0.001), male gender for HBV DNA (OR 1.49, p < 0.01), and a higher DCCI score (OR 1.10, p < 0.05) and male gender (1.46, p < 0.01) for both. Significant predictors of subsequent initiation of antiviral treatment were HBV DNA monitoring (OR 2.08, p < 0.001), a higher DCCI score (OR 1.24, p < 0.001), and male gender (OR 1.53, p < 0.01).
Conclusions
Laboratory monitoring of CHB patients not receiving antiviral treatment is below guideline recommendations, suggesting that initiation of antiviral therapy may also be delayed, leaving patients at risk for disease progression.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
INTRODUCTION
An estimated 400 million people are believed to be chronically infected with hepatitis B virus (HBV) worldwide. Over 1 million US residents have chronic hepatitis B (CHB) infection, with an estimated prevalence of 0.3%–0.5%1,2. In spite of the availability of an effective vaccine, the number of US residents with CHB infection remains high, primarily due to the slow progression of CHB and the influx of immigrants from countries with a high prevalence of chronic infection2.
Approximately 15%–40% of untreated CHB patients will develop serious hepatic sequelae during their lifetime, including cirrhosis, hepatic decompensation, and hepatocellular carcinoma (HCC)1,3–5. CHB is currently estimated to contribute to between 2,000 and 4,000 deaths annually in the US2. As a major cause of cirrhosis and HCC, CHB is a substantial public health burden, not only in terms of human suffering, but also in terms of social and economic costs, with over $1 billion spent each year on hepatitis B-related hospitalizations in the US2.
A recent report from the Institute of Medicine (IOM) highlighted that HBV infection is a serious health problem in the USA6. Thus, it strongly recommended the implementation of a national strategy for the prevention and control of HBV infection6. The American Association for the Study of Liver Diseases (AASLD) has responded by joining forces with Trust for America’s Health (TFAH) to implement a plan of action, including increased knowledge and awareness about chronic viral hepatitis among health care providers, social service providers, and the public; improved surveillance for hepatitis B and hepatitis C; and better integration of viral hepatitis services7. The findings of this study emphasize the importance of CHB and the need for careful screening and monitoring practices.
Evidence suggests that effective antiviral treatment could slow the progression of CHB8. Currently approved drugs for the treatment of CHB include interferons (interferon-α2b and peginterferon-α2a) and oral nucleoside or nucleotide analogs (lamivudine, adefovir dipivoxil, entecavir, telbivudine, and tenofovir disoproxil fumarate)5,9. The main goal of CHB therapy is to prevent the progression of liver disease. Although over 1 million US residents have CHB1,2, it is believed that only a small percentage is being actively treated with antiviral therapy. While there is little published research on the topic, a US study found that 93% of CHB patients receiving care at an urban hospital outpatient clinic were not undergoing antiviral treatment10, and, in a European study, 84% of CHB patients who were candidates for antiviral treatment were not receiving antiviral treatment11. Prescription drug sales data indicate that the majority of patients (>60%) currently receiving antiviral treatment for CHB in the US are commercially insured12.
Persistently elevated serum HBV DNA and alanine aminotransferase (ALT) levels have been found to be the most important predictors of future complications in CHB patients, including cirrhosis, hepatic decompensation, HCC, and death2,13–19. The decision to treat CHB with antivirals is primarily based upon the results of two laboratory tests: high levels of serum HBV DNA, indicative of active viral replication, and elevated serum ALT levels, indicative of ongoing liver injury9,20. While the ALT level is an important criterion for assessing the requirement for therapy in most treatment guidelines5,21,22, it can be affected by non-HBV-related factors (e.g., body mass index, gender, exercise, abnormal lipid and carbohydrate metabolism, and co-morbidities)23,24. Therefore, ALT results should not be used as the sole criterion for initiating treatment and should instead be assessed in conjunction with HBV DNA levels23.
Optimal management of CHB requires routine monitoring, even when patients are asymptomatic, in order to determine the extent of liver disease progression and the timing of treatment initiation. Two major CHB treatment guidelines are widely used in the US: AASLD guidelines and the US Treatment Algorithm5,23. The AASLD guidelines currently recommend both serum ALT and serum HBV DNA monitoring in untreated CHB patients, with treatment initiated in those with HBV DNA levels of at least 20,000 IU/ml and ALT more than twice the upper limit of normal5. Patients for whom immediate therapy is not routinely indicated include patients with CHB in the immune-tolerant phase (high HBV DNA but normal ALT, or minimal activity on liver biopsy) and patients in the inactive-carrier or low-replicative phase (low or undetectable HBV DNA and normal ALT)2. Similarly, the US Treatment Algorithm currently recommends monitoring serum ALT and serum HBV DNA in patients who do not require treatment23.
While there are likely to be multiple barriers to appropriate initiation of treatment, one major factor may be that physicians are not appropriately monitoring the laboratory values necessary to determine the correct point for treatment initiation. AASLD guidelines recommend monitoring of both HBV DNA and ALT levels at least annually5, although the recommended frequency of laboratory monitoring may be higher if laboratory results warrant it. In contrast, the US Treatment Algorithm currently recommends laboratory monitoring every 3–6 months23. The intent of this study is to examine the quality of care of CHB patients by assessing adherence to AASLD guideline recommendations in routine laboratory monitoring of CHB patients not currently receiving antiviral treatment. For this study, we chose the AASLD guideline recommendations rather than the US Treatment Algorithm since they are more conservative in terms of recommended frequency of CHB laboratory monitoring.
OBJECTIVES
The main objective of this study was to assess the level of adherence to AASLD CHB treatment guideline recommendations for laboratory monitoring in CHB patients not receiving antiviral treatment. The study also aimed to identify predictors of laboratory monitoring and to identify predictors of subsequent initiation of antiviral treatment (oral nucleoside/nucleotide analogs, or interferon/peginterferon).
METHODS
Data Source
Administrative databases are increasingly being used for studying the outcomes of medical care25,26. This retrospective cohort study used health care claims data from the Ingenix LabRx dataset over a 5-year period (January 1, 2003 to December 31, 2007). The Ingenix LabRx database contains health care claims for over 15 million commercially insured outpatients and inpatients across the USA (http://www.ispor.org/DigestOfIntDB/Default.aspx?rcd=393). Each medical claim contains primary and secondary diagnosis codes, which are assigned according to the International Classification of Diseases, ninth revision (ICD-9)27. The Ingenix LabRx database includes a very large and diverse set of patients across the country; however, since claims data are administrative data and not collected for a specific scientific purpose, these data cannot be assumed to be nationally representative.
Study Population
The study population included any patient 18–65 years of age who had at least one positive hepatitis B surface antigen (HBsAg) test and at least 12 months of continuous enrollment after initial diagnosis. In addition, in order to ensure that no patients with acute hepatitis B were included in the study, the inclusion criteria stated that patients had to have at least two paid medical claims (inpatient or outpatient) with an ICD-9 code for CHB (070.3×), in line with the AASLD definition of CHB, which includes HBsAg-positivity for at least 6 months.
Patients were excluded from the study if they had received a prescription for any antiviral medication (including lamivudine, adefovir, telbivudine, entecavir, tenofovir, emtricitabine, or interferon/peginterferon) prior to the monitoring period. Patients who eventually received antiviral medication during the monitoring period were only included in the study up to this event.
A diagnosis of HCC was also an exclusion criterion of the study.
Outcomes of Interest
The primary outcome of interest was frequency of serum laboratory testing, specifically testing for ALT and HBV DNA. Secondary outcomes of interest included predictors for serum laboratory monitoring (i.e., ALT and HBV DNA) and predictors for subsequent initiation of antiviral therapy.
Explanatory Variables
Demographic data were collected by the health care provider and reported on the patient’s medical claim. Clinical variables, defined using ICD-9 coding, were also reported on the patient’s medical claim. Note that, while laboratory results for the presence of HBsAg (dichotomous variable) formed part of the inclusion criteria for defining the analytic sample, ALT and HBV DNA test results were not assessed as that would have required taking continuous variables and turning them into dichotomous variables (taking test values and classifying patient results as “normal” and “abnormal”). The Deyo-Charlson Comorbidity Index, a clinical comorbidity index for use with ICD-9 administrative databases, was included as a variable in the study. The Deyo-Charlson Comorbidity Index score is calculated based on the number of comorbidities the patient has and the severity of those comorbidities; the higher the score, the greater is the disease burden28.
Statistical Analysis
Descriptive statistics assessed the characteristics of the study sample, including age, sex, geographical region, and Deyo-Charlson Comorbidity Index. Data captured included the proportion of patients with claims for ALT and/or HBV DNA laboratory testing at any time during follow-up, and the proportion with claims for ALT and HBV DNA laboratory tests at least once during the first 12 months of follow-up (±60 days; equivalent to patients meeting guideline criteria). Descriptive statistics compared unadjusted levels of monitoring and subsequent treatment in aggregate and by patient characteristic.
Multivariate logistic regression was used to determine predictors of monitoring using ALT testing, HBV DNA testing, and both ALT and HBV DNA testing as dichotomous outcome variables. Variables examined included age, sex, region, and Deyo-Charlson Comorbidity Index. Multivariate logistic regression was also used to determine predictors of subsequent initiation of antiviral therapy using the same variables, as well as ALT or HBV DNA monitoring as additional predictors.
RESULTS
Study Sample
Of 16,120 patients with two claims with a diagnosis of CHB, 1,168 met the full inclusion criteria (Fig. 1). Table 1 summarizes the characteristics of the study population, which had a mean age of 40.6 (SD, 10.5) years, was 58.3% male, and had a mean follow-up time of 728 (SD, 510.9) days (median = 696 days).

Patient flow. CHB, chronic hepatitis B; HCC, hepatocellular carcinoma; HBV, hepatitis B virus; HBsAg, hepatitis B surface antigen.
Adherence to Guideline-Recommended Monitoring
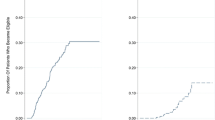
The proportion of patients who received monitoring at least every 12 months was 53.3% for ALT, 39.0% for HBV DNA, and 35.1% for both ALT and HBV DNA (Table 2). During this period, the mean number of tests per patient was 1.7 for ALT (median = 1.0) and 1.1 for HBV DNA (median = 1.0). The proportion of patients who received laboratory monitoring at any time point during follow-up was 93.7% for ALT, 79.6% for HBV DNA, and 76.4% for both ALT and HBV DNA (Table 2). During this period, the mean number of tests per patient was 5.0 for ALT (median = 3.0) and 3.4 for HBV DNA (median = 2.0). Approximately 32% of patients were eventually treated with an antiviral medication during the follow-up period (n = 375; Table 2).
Predictors of Laboratory Monitoring
Table 3 summarizes the unadjusted estimates of outcomes by predictors of laboratory monitoring for CHB, while Table 4 summarizes results of the logistic regression analyses, including predictors of laboratory monitoring. The only significant predictor of ALT monitoring was a higher Deyo-Charlson Comorbidity Index score (OR 1.90, p < 0.001, Table 4). Significant differences in monitoring of HBV DNA were observed for gender and region. Males were more likely to be monitored than females (OR 1.49, p < 0.01), while patients in the Midwest were less likely to be monitored than patients in the Northeast (OR 0.29, p < 0.001, Table 4).
The significant predictors of monitoring for combined ALT and HBV DNA were the same as the predictors for the individual assays, with a higher Deyo-Charlson Comorbidity Index score (OR 1.10, p < 0.05) and male sex (1.46, p < 0.01) both positively associated with dual monitoring (Table 4).
Predictors of Initiation of Antiviral Treatment
Unadjusted estimates of outcomes by predictors of subsequent antiviral treatment for CHB are summarized in Table 3. Table 4 summarizes results of the logistic regression analyses, including predictors of subsequent initiation of antiviral treatment. Initiation of antiviral treatment was found to be more likely among those who received HBV DNA monitoring (OR 2.08, p < 0.001), males (OR 1.53, p < 0.01), and patients with higher Deyo-Charlson Comorbidity Index scores (OR 1.24, p < 0.001; Table 4). Conversely, antiviral treatment initiation was less likely among patients receiving ALT monitoring only (OR 0.26, p < 0.001; Table 4).
DISCUSSION
The results of this study suggest that rates of guideline-recommended laboratory monitoring of ALT and HBV DNA in untreated patients with CHB are low, with high variability according to the specific test. Only about one-third of patients received both ALT and HBV DNA tests on an annual basis. Although ALT assessment is the more frequently applied of the two tests, only slightly more than half of all patients receive annual ALT testing. ALT testing also appears to be applied in a non-specific manner, as the only predictor of monitoring was comorbidity burden (Table 4). This is probably because ALT testing may be obtained for reasons other than for monitoring liver damage caused by HBV, for example, liver damage caused by disorders of the gall bladder or pancreas, or caused by drugs or alcohol; thus not everyone with elevated ALT would have received antiviral treatment.
The study shows that HBV DNA monitoring rates are lower than rates of ALT monitoring, and HBV DNA monitoring appears to be more specifically applied than ALT monitoring, as it is not influenced by comorbidities. This is perhaps unsurprising as liver function tests represent a relatively quick and inexpensive way of monitoring the need to treat, so it is possible that physicians are using these tests as an initial screen for active CHB. This is potentially a rational approach, as therapy is only indicated for patients with both elevated ALT and HBV DNA5,19,20. However, liver function tests have limitations because patients with advanced liver disease (for example, fibrosis) may have normal liver function and therefore may not receive appropriate treatment if HBV DNA levels are not monitored in addition to ALT.
Treatment in the Midwest was shown to be a negative predictor of HBV DNA monitoring. However, rates of monitoring for both ALT and HBV DNA were found to be similar in this patient population, suggesting that the rate of HBV DNA monitoring is more limited than ALT monitoring (as most patients who receive HBV DNA monitoring also receive ALT monitoring). Low rates of monitoring in the Midwest may reflect the distribution of CHB screening programs in the US; a recent survey of community-based hepatitis screening programs in the US identified few or no programs in the Midwest, the American Southeast and the Southwest outside of California and the Houston area29.
The study results demonstrate a poor level of adherence to guideline-recommended laboratory monitoring of CHB in commercially insured patients, particularly monitoring of HBV DNA. Since HBV DNA testing is a strong predictor of treatment initiation, it is likely that the low rates of monitoring may lead to delays in appropriate medical treatment of CHB. Results of delaying treatment may include cirrhosis, liver failure, and HCC, all of which may not become apparent until late in the course of the disease1,3,4.
Although this study provides interesting data, there are a number of limitations that should be considered. Firstly, this is a retrospective study using health insurance claims data. No information was available regarding the ethnic, socioeconomic, or educational distribution of the population and reasons for monitoring or not monitoring. Secondly, the results of this study may not be generally applicable to populations that are not commercially insured; CHB patients covered under public programs, such as Medicaid and Medicare, are not represented in this dataset, nor are CHB patients who are undocumented resident immigrants. It will be beneficial to include these populations in future CHB monitoring studies in order to gain a fuller picture of monitoring prevalence across different patient groups.
This study demonstrated that, in a commercially insured population of CHB patients, rates of guideline-recommended laboratory monitoring were low and varied according to the specific test. Improving monitoring rates may increase the rates of medically appropriate treatment of CHB, preventing delays in treatment initiation and, therefore, complications of the disease.
References
McMahon BJ. Epidemiology and natural history of hepatitis B. Semin Liver Dis. 2005;25(Suppl 1):3–8.
Sorrell MF, Belongia EA, Costa J, et al. National Institutes of Health Consensus Development Conference Statement: management of hepatitis B. Ann Intern. Med. 2009;150:104–10.
Hadziyannis SJ, Tassopoulos NC, Heathcote EJ, et al. Long-term therapy with adefovir dipivoxil for HBeAg-negative chronic hepatitis B for up to 5 years. Gastroenterology. 2006;131:1743–51.
Yim HJ, Lok AS. Natural history of chronic hepatitis B virus infection: what we knew in 1981 and what we know in 2005. Hepatology. 2006;43:S173–81.
Lok AS, McMahon BJ. Chronic hepatitis B: update 2009. Hepatology. 2009;50:661–2.
Institute of Medicine. Hepatitis and Liver Cancer. A National Strategy for Prevention and Control of Hepatitis B and C. Available at: http://books.nap.edu/openbook.php?record_id=12793&page=R1 (accessed September 2010).
American Association for the Study of Liver Diseases. The Route from the IOM to Public Health Passes through AASLD. AASLD News; May 6, 2010. Available at: http://www.aasld.org/journals/archive/050610/Pages/default.aspx (accessed September 2010).
Liaw YF, Sung JJ, Chow WC, et al. Lamivudine for patients with chronic hepatitis B and advanced liver disease. N Engl J Med. 2004;351:1521–31.
Gish RG. Hepatitis B treatment: Current best practices, avoiding resistance. Cleve. Clin J Med. 2009;76 Suppl 3:S14–9.
Widjaja D, Yarlagadda S, Singu BS, et al. Characteristics of patients with chronic hepatitis-B virus infection in an urban hospital. J Natl. Med Assoc. 2007;99:384–8.
Giannini EG, Torre F, Basso M, et al. A significant proportion of patients with chronic hepatitis B who are candidates for antiviral treatment are untreated: A region-wide survey in Italy. J Clin Gastroenterol. 2009;43:1001–7.
Wolters Kluwer Pharma Solutions, Inc. Chronic Hepatitis B, Total Prescription Sales Data, Sep 2009–Feb 2010. Philadelphia, PA, March 2010.
Chen CJ, Yang HI, Su J, et al. Risk of hepatocellular carcinoma across a biological gradient of serum hepatitis B virus DNA level. JAMA. 2006;295:65–73.
Iloeje UH, Yang HI, Su J, Jen CL, You SL, Chen CJ. Predicting cirrhosis risk based on the level of circulating hepatitis B viral load. Gastroenterology. 2006;130:678–86.
Iloeje UH, Yang HI, Jen CL, et al. Risk and predictors of mortality associated with chronic hepatitis B infection. Clin Gastroenterol Hepatol. 2007;5:921–31.
Chen G, Lin W, Shen F, Iloeje UH, London WT, Evans AA. Past HBV viral load as predictor of mortality and morbidity from HCC and chronic liver disease in a prospective study. Am J Gastroenterol. 2006;101:1797–803.
Liu CJ, Chen BF, Chen PJ, et al. Role of hepatitis B viral load and basal core promoter mutation in hepatocellular carcinoma in hepatitis B carriers. J Infect Dis. 2006;193:1258–65.
Ohata K, Hamasaki K, Toriyama K, Ishikawa H, Nakao K, Eguchi K. High viral load is a risk factor for hepatocellular carcinoma in patients with chronic hepatitis B virus infection. J Gastroenterol Hepatol. 2004;19:670–5.
Yu MW, Yeh SH, Chen PJ, et al. Hepatitis B virus genotype and DNA level and hepatocellular carcinoma: a prospective study in men. J Natl. Cancer Inst. 2005;97:265–72.
Chevaliez S, Pawlotsky JM. Virological techniques for the diagnosis and monitoring of hepatitis B and C. Ann Hepatol. 2009;8:7–12.
European Association For The Study Of The Liver. EASL Clinical Practice Guidelines. Management of chronic hepatitis B. J Hepatol. 2009;50:227–42.
Liaw YF, Leung N, Kao JH, et al. Asian-Pacific consensus statement on the management of chronic hepatitis B: a 2008 update. Hepatol Int. 2008;2:263–83.
Keeffe EB, Dieterich DT, Han SH, et al. A treatment algorithm for the management of chronic hepatitis B virus infection in the United States: 2008 update. Clin Gastroenterol Hepatol. 2008;6:1315–41.
Prati D, Taioli E, Zanella A, et al. Updated definitions of healthy ranges for serum alanine aminotransferase levels. Ann Intern. Med. 2002;137:1–10.
Mitra D, Davis KL, Beam C, Medjedovic J, Rustgi V. Treatment patterns and adherence among patients with chronic hepatitis C virus in a US managed care population. Value Health. 2010;13:479–86.
Berger ML, Mamdani M, Atkins D, Johnson ML. Good research practices for comparative effectiveness research: defining, reporting and interpreting nonrandomized studies of treatment effects using secondary data sources: the ISPOR Good Research Practices for Retrospective Database Analysis Task Force report-part I. Value Health. 2009;12:1044–52.
International Classification of Diseases, 9th Revision, Clinical Modification. 5th edition Medicode Publications, Salt Lake City UT, 1997.
Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol. 1992;45:613–9.
Rein DB, Lesesne SB, Leese PJ, Weinbaum CM. Community-based hepatitis B screening programs in the United States in 2008. J Viral Hepat. 2010;17:28–33.
Acknowledgements and Conflict of Interest
We would like to acknowledge Miriam Banner and Andrew Street for editorial support given in the preparation of the manuscript; this assistance was funded by Bristol-Myers Squibb Co. The study was sponsored by Bristol-Myers Squibb Co.
Timothy Juday, Hong Tang, and Melissa Harris are employees of Bristol-Myers Squibb Co. George Hanna is an employee of Bristol-Myers Squibb Co. and a stockholder in the company. Annette Powers and Edward Kim are former employees of Bristol-Myers Squibb Co. and are currently employees of Eisai Inc.
This paper was presented as a poster at the 60th annual meeting of the American Association for the Study of Liver Diseases, November 1, 2009.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Juday, T., Tang, H., Harris, M. et al. Adherence to Chronic Hepatitis B Treatment Guideline Recommendations for Laboratory Monitoring of Patients Who Are Not Receiving Antiviral Treatment. J GEN INTERN MED 26, 239–244 (2011). https://doi.org/10.1007/s11606-010-1549-9
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-010-1549-9