
Abstract
BACKGROUND
In response to dramatic increases in obesity prevalence, clinical guidelines urge health care providers to prevent and treat obesity more aggressively.
OBJECTIVE
To describe the proportion of obese primary care patients receiving obesity care over a 5-year period and identify factors predicting receipt of care.
DESIGN
Retrospective cohort study utilizing VHA administrative data from 6 of 21 VA administrative regions.
PATIENTS
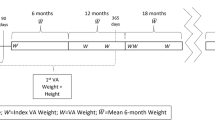
Veterans seen in primary care in FY2002 with a body mass index (BMI) ≥30 kg/m2 based on heights and weights recorded in the electronic medical record (EMR), survival through FY2006, and active care (1 or more visits in at least 3 follow-up years FY2003–2006).
MAIN MEASURES
Receipt of outpatient visits for individual or group education or instruction in nutrition, exercise, or weight management; receipt of prescriptions for any FDA-approved medications for weight reduction; and receipt of bariatric surgery.
KEY RESULTS
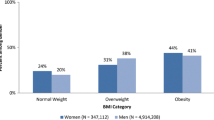
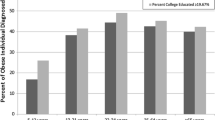
Of 933,084 (88.6%) of 1,053,228 primary care patients who had recorded heights and weights allowing calculation of BMI, 330,802 (35.5%) met criteria for obesity. Among obese patients who survived and received active care (N = 264,667), 53.5% had a recorded obesity diagnosis, 34.1% received at least one outpatient visit for obesity-related education or counseling, 0.4% received weight-loss medications, and 0.2% had bariatric surgery between FY2002–FY2006. In multivariable analysis, patients older than 65 years (OR = 0.62; 95% CI: 0.60–0.64) were less likely to receive obesity-related education, whereas those prescribed 5–7 or 8 or more medication classes (OR = 1.41; 1.38–1.45; OR = 1.94; 1.88–2.00, respectively) or diagnosed with obesity (OR = 4.0; 3.92–4.08) or diabetes (OR = 2.23; 2.18–2.27) were more likely to receive obesity-related education.
CONCLUSIONS
Substantial numbers of VHA primary care patients did not have sufficient height or weight data recorded to calculate BMI or have recorded obesity diagnoses when warranted. Receipt of obesity education varied by sociodemographic and clinical factors; providers may need to be cognizant of these when engaging patients in treatment.


Similar content being viewed by others
References
NHLBI Obesity Education Initiative. Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults: the evidence report. Washington: National Institutes of Health; 1998.
National Task Force on the Prevention and Treatment of Obesity. Overweight, obesity, and health risk. Arch Intern Med. 2000;160:898–904.
Nawaz H, Katz DL. American College of Preventive Medicine Practice policy statement. Weight management counseling of overweight adults. Am J Prev Med. 2001;21:73–8.
Lyznicki JM, Young DC, Riggs JA, Davis RM. Council on Scientific Affairs American Medical Association. Obesity: assessment and management in primary care. Am Fam Physician. 2001;63:2185–96.
National Task Force on the Prevention and Treatment of Obesity. Medical care for obese patients: advice for health care professionals. Am Fam Physician. 2002;65:81–8.
McTigue KM, Harris R, Hemphill B, et al. Screening and interventions for obesity in adults: summary of the evidence for the US Preventive Services Task Force. Ann Intern Med. 2003;139:933–49.
Mehrotra C, Serdula M, Naimi TS, Khan LK, Miller J, Dietz W. Population-based study of trends, costs, and complications of weight loss surgeries from 1990–2002. Obes Res. 2005;13(11):2029–34.
Davis MM, Slish K, Chao C, Cabana MD. National trends in bariatric surgery, 1996–2002. Arch Surg. 2006;141(1):71–4.
Stafford RS, Radley DC. National trends in antiobesity medication use. Arch Intern Med. 2003;169(9):1046–50.
Stafford RS, Farhat JH, Misra B, Schoenfeld DA. National patterns of physician activities related to obesity management. Arch Fam Med. 2000;9:631–8.
McAlpine DD, Wilson AR. Trends in obesity-related counseling in primary care: 1995–2004. Med Care. 2007;45:322–9.
United States. Department of Health and Human Services. HSS announces revised Medicare obesity coverage policy. News Release. Available from: URL: http://www.hhs.gov/news/press/2004pres/20040715.html. Accessed January 20, 2010.
National Committee for Quality Assurance. Proposed new measures for HEDIS 2009: Body Mass Index (BMI) Assessment (BAA) BMI Percentile Assessment and Counseling for Nutrition and Physical Activity (BCA). 2008; NCQA.
Das SR, Kinsinger LS, Yancy WS Jr, Wang A, Ciesco E, Burdick M, et al. Obesity prevalence among veterans at Veterans Affairs medical facilities. Am J Prev Med. 2005;28:291–4.
Kinsinger LK, Jones KR, Kahwati LK, Harvey R, Burdick M, Zele V, Yevich SJ. Design and dissemination of the MOVE! weight management program for veterans. Prev Chron Dis. 2009;6(3):1–6.
Perrin R, Bates J, Noel PH, Copeland LA, Lancaster B. National Clinical Data for VA Research: the VA Corporate Data Warehouse. Workshop. February, 2008 National HSR&D Meeting, Baltimore, MD.
Sohn MW, Zhang H, Arnold N, Stroupe K, Taylor BC, Wilt TJ, Hynes DM. Transition to the new race/ethnicity data collection standards in the Department of Veterans Affairs. Popul Health Metr. 2006;4:7.
Long JA, Bamba MI, Linq B, Shea JA. Missing race/ethnicity data in Veterans Health Administration based disparities research: a systematic review. J Health Care Poor Underserved. 2006;17(1):128–40.
Gao J, Wang Y, Engelhardt J. Logistic analysis of veterans’ eligibility-status changes. Health Serv Manag Res. 2005;18:175–85.
U.S. Census Bureau. (2000). Population and housing profile, US census STF1. Generated from http://factfinder.census.gov/servlet/DTGeoSearchByListServlet?ds_name=DEC_2000_SF1_U&_lang=en&_ts=272882185413. Accessed October 6, 2009.
SAS Insitute Inc., SAS 9.2, Cary, NC: SAS Institute Inc., 2008.
World Health Organization. International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM). American Medical Association Press, 2006}.
Kerr EA, Hofer TP, Hayward RA, Adams JL, Hogan MM, McGlynn EA, Asch SM. Quality by any other name?: A comparison of three profiling systems for assessing health care quality. Health Serv Res. 2007;42(5):2070–87.
Cornell J, Pugh JA, Williams JW Jr, Kazis L, Lee A, Parchman M, Zeber J, Pederson T, Montgomery KA, Noël PH. Multimorbidity clusters: clustering binary data from a large administrative medical database. Applied Multivariate Research. 2008;12(3):163–82.
Zeber JE, Copeland LA, Amuan M, Cramer JA, Pugh MJV. The role of comorbid psychiatric conditions in health status in epilepsy. Epilepsy & Behavior. 2007;10:539–46.
Schneeweiss S, Seeger JD, Maclure M, Wang PS, Avorn J, Glynn RJ. Performance of comorbidity scores to control for confounding in epidemiologic studies using claims data. Am J Epidemiol. 2001;154(9):854–64.
Buck CJ. Saunders 2008 ICD-9-CM, Volumes 1, 2, and 3, HCPCS Level II and CPT Professional Edition Package. 2007. St. Louis, Mo. Saunders.
Ma J, Xiao L, Stafford RS. Underdiagnosis of obesity in adults in US outpatient settings. Arch Intern Med. 2009;169(3):313–4.
Ma J, Xiao L, Stafford RS. Adult obesty and office-based quality of care in the United States. Obesity (Silver Spring) 2009 Feb 5. [Epub ahead of print].
Ruelaz AR, Diefenbach P, Simon B, Lanto A, Arterburn D, Shekelle PG. Perceived barriers to weight management in primary care-perspectives of patients and providers. JGIM. 2007;22:518–22.
Personal Communication. Leila C. Kahwati, MD MPH, VHA Deputy Chief Consultant for Preventive Medicine, summarizing findings from the MOVE! Weight Management Program for Veterans, Special Evaluation Report: Clinical Effectiveness, 2009.
National Committee for Quality Assurance. Proposed new measures for HEDIS 2009: Body Mass Index (BMI) Assessment (BAA) BMI Percentile Assessment and Counseling for Nutrition and Physical Activity (BCA). 2008; NCQA.
Acknowledgements
The research reported here was supported by the Department of Veteran Affairs, Veterans Health Administration, Health Services Research and Development Service (project no. IIR 05–121). Dr. Noël is a Research Psychologist at the South Texas Veterans Health Care System. The views expressed in this article are those of the author(s) and do not necessarily represent the views of the Department of Veterans Affairs.
Conflict of Interest
The research reported here was supported by the Department of Veterans Affairs, Veterans Health Administration, Health Services Research and Development Service (project no. IIR 05–121). The funding agency provided support to conduct this study, including collection, management, analysis, and interpretation of the data, and preparation of the manuscript, but has not participated in manuscript development, and has not reviewed or approved this manuscript.
The authors have no conflict of interests to declare. Sources of support for the authors for the past 3 years are listed below:
Dept. of Veterans Affairs: Noël, Copeland, Pugh, Kahwati, Tsevat, Nelson, Wang, Bollinger
UT Health Science Center: Noël, Copeland, Pugh, Hazuda, Wang
University of Cincinnati: Tsevat
University of Washington: Nelson
NIH: Noël, Copeland, Pugh, Wang, Nelson, Tsevat
CDC: Pugh
Epilepsy Foundation: Pugh
Abbott Laboratories: Pugh
Author information
Authors and Affiliations
Corresponding author
Additional information
The research reported here was supported by the Department of Veteran Affairs, Veterans Health Administration, Health Services Research and Development Service (project no. IIR 05–121). Dr. Noël is a Research Psychologist at the South Texas Veterans Health Care System. The views expressed in this article are those of the author(s) and do not necessarily represent the views of the Department of Veterans Affairs.
Rights and permissions
About this article
Cite this article
Noël, P.H., Copeland, L.A., Pugh, M.J. et al. Obesity Diagnosis and Care Practices in the Veterans Health Administration. J GEN INTERN MED 25, 510–516 (2010). https://doi.org/10.1007/s11606-010-1279-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-010-1279-z