
Abstract
OBJECTIVE
To evaluate the association between chronic illness with complexity (CIC) and optimal glycemic control.
PARTICIPANTS
Cross-sectional and longitudinal analyses of Diabetes Epidemiologic Cohort database of Veterans Health Administration (VHA) users with diabetes, less than 75 years old, with HbA1c tests in fiscal year (FY) 1999 and 2000, alive at FY2000 end (N = 95,423).
DESIGN/MEASUREMENTS
Outcomes were HbA1c < 7% in each FY. CIC included three domains: nondiabetes physical illness, diabetes-related, and mental illness/substance abuse conditions. Other independent variables included age, gender, race, marital status, VHA priority status, and diabetes severity. Longitudinal analyses were restricted to patients with HbA1c ≥ 7% in FY1999 and included hospitalizations between final HbA1c’s in FY1999 and FY2000. Multiple logistic regressions examined associations between CIC categories and HbA1c.
RESULTS
In FY1999, 33% had HbA1c <7%. In multivariate analyses, patients with nondiabetes physical illness and mental illness/substance abuse were more likely to have HbA1c <7% in FY1999 [adjusted odds ratios for cancer (AOR), 1.31; 95% CI (1.25–1.37); mental illness only, 1.18; 95% CI (1.14–1.22)]. Those with diabetes-related complications were less likely to have HbA1c <7% in FY1999. Associations generally held in FY2000. However, conditions in the mental illness/substance abuse complexity domain were less strongly associated with HbA1c <7%. Macrovascular-related hospitalizations were positively associated with HbA1c <7% [AOR, 1.41; 95% CI (1.34–1.49)].
CONCLUSIONS
The association between CIC and HbA1c <7% is heterogeneous and depends on the domain of complexity. The varying associations of CIC categories with optimal glycemic control suggest the need for appropriate risk adjustment when using HbA1c <7% as a valid performance measure for diabetes quality of care.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
INTRODUCTION
Controlling glycemia is critical to reducing the risk of costly and disabling complications associated with both type 1 and type 2 diabetes.1,2 A measure of “poor glycemic control,” defined as glycosylated hemoglobin A1c (HbA1c) level greater than 9.0%, is recommended as a performance measure because it represents “poor control” for all patients, including those with chronic illnesses with complexity (CIC).3–6 “Optimal glycemic control,” HbA1c target values of less than 7%, has been used to guide quality improvement efforts only within plans and practices because differences in patient case mix, including prevalence of CIC among plans, cannot be adequately addressed by current case mix adjustment methods. Recently, however, HbA1c <7% for all persons 18–75 years old, without any appropriate risk adjustment or exclusion criteria, was adopted for public reporting of health plans.4
Studies have examined the association between chronic comorbid conditions and glycemic control. The most common adjustment for physical comorbidity has been the Charlson Comorbidity Index.7–11 Other measures include presence of diabetes-related complications11–13 and simple count of comorbid conditions.14 However, these measures may not adequately control for CIC that may influence glycemic control. Summary scores like the Charlson Comorbidity Index do not provide insight into comorbidities that may have varying associations with glycemic control. Therefore, the current paper uses an alternative and comprehensive classification of CIC based on theory and prior empirical research.
In the absence of a widely accepted conceptual framework for CIC, we used the recent conceptual model of comorbid chronic illness complexity in diabetes care by Piette and Kerr15 as a starting point and operationalized CIC in the context of glycemic control. Our categories of CIC were designed to reflect overall similarity in pathophysiologic profiles, treatment plans, and self-management strategies in achieving glycemic control and the need to develop a reasonable summarization of CIC. We categorized CIC into three domains of complexity: (1) nondiabetes-related physical illness, (2) diabetes-related, and (3) mental illness and substance abuse conditions. Our primary objective in this manuscript is to evaluate associations between CIC categories and HbA1c < 7% in Veterans Health Administration (VHA) clinic users with diabetes.
Macrovascular, microvascular complications, and metabolic decompensation formed the domain diabetes-related complexity because these tend to co-occur in patients with diabetes, increase cardiovascular morbidity, and treatment strategies are synergistic with contemporary standards of diabetes management. For example, macrovascular complications consisted of angina, myocardial infarction, congestive heart failure, arrhythmia, peripheral vascular disease, stroke, transient ischemic attack, and hypertension. For an individual with diabetes and a macrovascular complication, the treatment plans would continue to focus on intensive glycemic control in addition to reducing the elevated risk of cardiovascular complications.
Non-diabetes physical illness complexity domain included categories of cancer, musculoskeletal, gastrointestinal, pulmonary, and other diseases because of a lower degree of synergism in treatment plans and self-management strategies compared to the categories in the domain of diabetes-related complexity. For example, if an individual has diabetes and a musculoskeletal condition, the self-management of diabetes (e.g., exercise) may be compromised. In addition, we developed a hierarchy within this domain to reflect increasing complexity with diabetes management. In the presence of clinically dominant conditions (e.g., cancer), in the short-term, the focus may revolve around managing and treating cancer rather than diabetes. Similarly, if a person with diabetes had at least one disease in all three categories (musculoskeletal, gastrointestinal, pulmonary), addressing diabetes management becomes highly complex. Because of empirical evidence that mental illness and substance abuse conditions exert their own unique influence on diabetes outcomes and care, we considered mental illness and substance abuse in a separate domain of complexity.16
In summary, our classification provides an alternative specification for CIC based on overall similarities in pathophysiologic profiles, treatment plans, and self-management strategies that may influence glycemic control. The primary objective of this paper is to analyze the association between various categories of CIC based on our conceptualization and optimal glycemic control in VHA users with diabetes.
METHODS
Data
Our data are from the Diabetes Epidemiologic Cohort (DepiC), a dataset of merged nationwide VHA inpatient and outpatient administrative files, pharmaceutical utilization, and laboratory data (the VA Healthcare Analysis and Information Group: VA-HAIG) and Medicare paid claims on nationwide veteran clinic users identified with diabetes.17 For the current paper, we used the cohort identified with diabetes in fiscal year (FY) 1999 (prevalent and incident cases) and followed through FY2000. Medicare claims are used because prior research has demonstrated that using only VHA administrative data can underestimate the prevalence of chronic illness.18 Thus, to determine prevalence of CIC categories among veterans, we utilized a merged dataset that included both VHA administrative and Medicare claims data. Because Medicare claims data are not available for Medicare Health Maintenance Organization enrollees, they were excluded from the analytic dataset. The laboratory values and pharmaceutical utilization (VA-HAIG) data were based only on VHA files because Medicare claims data have no laboratory values and Medicare did not cover prescription drugs during the period of our study. We used FY1999/2000 data because of their extensive validation10,19 and nonavailability of DepiC dataset with merged Medicare data beyond FY2000.
Study Population
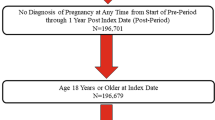
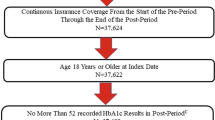
The study population (N = 95,423) consisted of VHA users diagnosed with diabetes during FY1999, aged less than 75 years as per standard practice,4 and alive at the end of FY2000. We also required that individuals have HbA1c values in both FY1999 and FY2000 with at least 90 days interval between the final HbA1c in FY1999 and FY2000.8
Measures
Dependent Variable: Glycemic Control
The dependent variable of our analyses was glycemic control measured by the last measurement of HbA1c in the FY. For our primary analyses, we used HbA1c <7%. For our secondary analyses, we used HbA1c <8%. Both these thresholds were used because the definition of optimal glycemic control (HbA1c <7% or HbA1c <8%) remains a controversial policy issue.20
For our primary longitudinal analysis, we included only those individuals with HbA1c ≥7% in FY1999 (N = 64,156) because of our focus on the association between CIC categories and achieving optimal glycemic control given lack of optimal glycemic control during the baseline year.
Key Independent Variables—Chronic Illness with Complexity
Nondiabetes physical illness complexity
Nondiabetes physical illness complexity was hierarchically evaluated using five categories of chronic illness based on International Classification of Diseases, 9th revision, Clinical Modification (ICD-9-CM) codes21 (see Table 5 in Appendix A). The presence of cancer was given priority, and we categorized gastrointestinal, musculoskeletal, pulmonary, and other diagnoses only among those without cancer. Thus, our final classification of nondiabetes physical illness complexity consisted of seven groups: (1) any cancer; (2) all three (gastrointestinal, musculoskeletal, pulmonary diagnoses); (3) any two; (4) only gastrointestinal; (5) only musculoskeletal; (6) only pulmonary; and (7) none of these nondiabetes physical illness categories.
Diabetes-related complexity
This was measured by the presence of microvascular (diabetic retinopathy, renal disease, ulcers, and lower extremity amputations), macrovascular (coronary artery disease, congestive heart failure, arrhythmia, cerebrovascular disease, and peripheral vascular disease),22,23 and metabolic decompensation (uncontrolled and short-term complications of diabetes) derived from ICD-9-CM codes.24
Mental illness/substance abuse complexity
We used ICD-9-CM codes of 295–314 (other than substance abuse codes) to represent mental illness. Substance abuse consisted of drug use, alcohol use, and tobacco use. Individuals were grouped into four categories: (1) no substance abuse and no mental illness; (2) substance abuse only; (3) mental illness only; and (4) both mental illness and substance abuse.
Other Independent Variables
Other independent variables included age, gender, race/ethnicity, marital status, VHA priority group status, dual VHA/Medicare use, endocrinology care, and baseline severity of diabetes. Severity of diabetes was based on the patient’s pharmaceutical treatment regimen (oral agents only, insulin only, insulin and oral agents, no agents) because the use of multiple oral agents or insulin is associated with increasing duration of the disease 25. Diabetes medications, endocrinology care, and dual VHA/Medicare use were all assessed in the 120 days before the HbA1c tests in FY1999.
Longitudinal analysis included the presence of hospitalization during the period between the two HbA1c tests because hospitalization may interrupt normal management of diabetes and may have an impact on HbA1c control. We followed a similar taxonomy to our CIC categories, and based on significant findings, we finally grouped them into three categories: (1) no hospitalization; (2) macrovascular-related hospitalization; and (3) other.
In our study population, individuals were tested for HbA1c at different time points, which caused variation in time interval between the last test in FY1999 and the last test in FY2000. We adjusted for this varying number of months between the two HbA1c tests by including it as a covariate in our regressions.
Statistical Techniques
Chi-square tests were used to assess unadjusted associations between CIC categories and HbA1c <7%. Among all VHA users with diabetes (N = 95,423), we used logistic regressions to investigate the effect of CIC on HbA1c in FY1999, controlling for other independent variables. Parameter estimates from logistic regressions were converted to odds ratios, and we also report the 95% confidence intervals (CI). To understand how CIC may influence longitudinal HbA1c outcomes, we evaluated the association between CIC and HbA1c <7% in FY2000 among only those who had HbA1c ≥7% in FY1999 (N = 64,156).
Sensitivity analysis
To ensure that the relationship was robust across different HbA1c values, we tested the relationship between CIC and HbA1c < 8%, and these findings are summarized in Table 4.
FINDINGS
The study population (N = 95,423) was predominantly male (98%), white (68%), married (61%), enrolled in Medicare (60%), and younger than 65 years of age (59%; Table 1). A majority were enrolled in the VHA through a priority status that reflected having both no service connected disability and low income (52%). Nearly one third (29%) had severe diabetes based on the use of insulin in the 120 days before the HbA1c test in FY1999. Only 3.3% saw an endocrinologist during that period. In FY1999, 33% of patients had an HbA1c <7%, with mean HbA1c value of 7.9 and standard deviation (SD) 1.8. In FY2000, 37% of patients had HbA1c <7% with mean value of 7.8 (SD = 1.8). Average time between HbA1c tests was approximately 12 months.
Chronic Illness with Complexity
Nondiabetes Physical Illness Complexity
We found that 13% had cancer, 0.8% had all three diagnoses (gastrointestinal, pulmonary, and musculoskeletal), 8.5% had any two of gastrointestinal, pulmonary, and musculoskeletal diagnoses, 3% had gastrointestinal diagnoses only, 6.6% had pulmonary diagnoses only, and 23% had musculoskeletal diagnoses only. Forty-five percent of the study population did not have any cancer, gastrointestinal, musculoskeletal, or pulmonary diagnoses.
Diabetes-Related Complexity
Forty-four percent had diagnoses of macrovascular complications, 35% had microvascular complications, and 31% were diagnosed with metabolic decompensations. Twenty-nine percent had no microvascular complications, macrovascular complications, or metabolic decompensation.
Mental Illness/Substance Abuse Complexity
Mental illness was diagnosed in 25% of the study population, either alone (19%) or in combination with substance abuse (6%). Seven percent of the study population had a substance abuse diagnosis without mental illness.
Baseline Glycemic Control and Chronic Illness with Complexity
In FY1999 (Table 2), overall, one third (N = 31,267) had optimal glycemic control (HbA1c <7%). Patients with nondiabetes physical illness were more likely to have HbA1c <7% at baseline than those without nondiabetes physical illness. The percentages of VHA users with optimal control ranged from 29% among those without nondiabetes physical illness to 37% among patients with cancer and 39% among those with all three gastrointestinal, musculoskeletal, and pulmonary diagnoses. A similar pattern was seen in the mental illness/substance abuse domain. Slightly more patients with mental illness alone (35%) and both mental illness and substance abuse (34%) had optimal glycemic control compared to those without any mental illness or substance abuse (32%).
On the other hand, we found that a lower proportion of patients with diabetes-related conditions [macrovascular complications (32%), microvascular complications (28%), and metabolic decompensation (26%)] had HbA1c <7% compared to those without these complications (33, 35, and 36%, respectively).
Logistic regression on optimal glycemic control in FY1999 confirmed the bivariate findings (Table 2). Patients with any cancer were more likely to have optimal glycemic control than patients without nondiabetes physical illness [adjusted odds ratio (AOR), 1.31; 95% CI (1.25–1.37)]. Similarly, individuals who had gastrointestinal, pulmonary, or musculoskeletal diagnoses, either individually or in combination, were more likely to have optimal glycemic control than those without nondiabetes physical illness. The AORs ranged from 1.12 to 1.56.
Those with mental illness only or both mental illness and substance abuse were more likely to have optimal glycemic control than their counterparts without any mental illness and substance abuse. The AOR for mental illness only was 1.18 [95% CI (1.14–1.22)].
Those with diabetes-related complications were less likely to have HbA1c <7% than patients without diabetes-related complications. The AORs ranged from 0.70 for metabolic decompensation to 0.91 for macrovascular complications.
Longitudinal Optimal Glycemic Control and Chronic Illness with Complexity
We also analyzed the relationship between CIC and optimal glycemic control in FY2000 among those who did not have optimal control in FY1999 (Table 3). Among those who did not have optimal control in FY1999 (N = 64,156), only 20% (N = 13,056) achieved HbA1c <7% in FY2000. In multivariate analysis, except for pulmonary diagnoses, those with nondiabetes physical illness (range of AOR, 1.17–1.34) were more likely to achieve optimal control than those without (P < 0.01 for all comparisons). Individuals with only mental illness were slightly more likely to achieve optimal glycemic control (P < 0.01).
Patients hospitalized for macrovascular complications were more likely to achieve optimal glycemic control [AOR, 1.41; 95% CI (1.34–1.49)] compared to patients who were not hospitalized. On the other hand, hospitalization for all other conditions was not associated with achieving optimal glycemic control.
Sensitivity Analysis
Using HbA1c <8%, we found generally similar direction and strength of associations between CIC and glycemic control in FY1999 (Table 4). However, in the longitudinal analyses, the associations between CIC and HbA1c <8% were attenuated; only cancer and musculoskeletal diagnoses were significantly associated with HbA1c <8% (P < 0.001). Within diabetes-related complexity, macrovascular and microvascular conditions remained significantly and negatively associated with HbA1c < 8% (P < 0.01). There was no significant association between mental illness/substance abuse complexity and HbA1c <8%.
DISCUSSION
Our findings demonstrate that the association between CIC and optimal glycemic control varied by type of complexity. In general, patients with nondiabetes physical or mental illness/substance abuse complexities were more likely to have and achieve HbA1c <7%. Patients with diabetes-related complications were less likely to have or achieve optimal glycemic control.
There are many plausible explanations for the association between nondiabetes physical illness complexity and achieving HbA1c <7%. For example, nondiabetes physical illnesses may result in improved HbA1c control due to pathophysiologic mechanisms beyond the influence of the healthcare provider, such as involuntary weight loss and anorexia that could result in increased sensitivity to antiglycemic agents. In addition, individuals with chronic diseases may have more contact with the health care system and may be more likely to achieve optimal glycemic control because of closer monitoring and better care coordination. However, in our preliminary and published research on diabetes quality of care measures, controlling for frequency of visits did not alter the findings regarding quality of care.16, 26 Further research is necessary to understand the clinically relevant associations between nondiabetes illness and glycemic control, their underlying mechanisms, and implications for performance measurement.
VHA users with diabetes-related complexity were less likely to be in control either at baseline or at follow-up. In other studies, microvascular complications were associated with both longer duration and poorer control of diabetes,1, 2 both of which may increase the difficulty of achieving HbA1c <7% even with newer insulin preparations.27
We found that those with mental illness/substance abuse complexity were more likely to have optimal glycemic control. These findings are consistent with studies that suggest that the association is dependent on the selection of the threshold for glycemic control.16 For example, Frayne et al.16 reported that when glycemic control was measured at HbA1c > 7%, the AOR for mental health conditions fell below 1.0, suggesting better control.
A noteworthy finding of our study is that the associations between CIC and glycemic control vary by HbA1c threshold. In FY2000, both nondiabetes physical illness and mental illness/substance abuse complexity were more strongly associated with HbA1c <7% than HbA1c <8%. As noted in the concluding paragraph, these findings have policy implications for performance measurement of optimal glycemic control.
Hospitalization for macrovascular complications between the baseline and follow-up HbA1c value was associated with a greater likelihood of achieving HbA1c control relative to no hospitalization, whereas hospitalization for all other conditions was not associated with glycemic control. This finding may reflect the clinically plausible overlap in treatments for acute cardiovascular conditions and diabetes.28
Strengths of the study include a nationwide population, longitudinal study design, inclusion of ambulatory and inpatient data, and incorporation of multiple disease categories to define CIC. We also acknowledge some limitations of our study. We were unable to explicitly measure the severity of diabetes or other illnesses within disease categories. Because our study population was relatively homogeneous, validation in other populations using clinical data would enhance the generalizability of our findings. In addition, individuals with CIC may have more interactions with the healthcare system and receive better care. We could not test this hypothesis because our CIC categories were defined using the ICD-9-CM codes recorded in administrative data. It is likely that those with more visits have more unique diseases coded and, therefore, are more likely to be classified in CIC categories. Thus, the number of visits may have had an influence on our CIC categorization itself. Although our data are 6–7 years old and there has been a decline in mean HbA1c levels during FY2000 through FY2003, the proportion of individuals with HbA1c <7% did not change (Pogach, personal communication). Thus, we believe that use of more recent data may not lead to substantially different conclusions.
The varying associations of CIC categories with optimal glycemic control have implications for the validity of using HbA1c <7% threshold as a performance measure for diabetes quality of care. When using HbA1c <7% as a performance measure, appropriate risk adjustment based on CIC may be necessary. In the absence of validated and widely accepted risk adjustment models,20 our findings highlight the need for developing appropriate risk adjustment models for optimal glycemic control. An alternative approach may be to use HbA1c <8% to measure optimal glycemic control, which is less influenced by CIC categories. In addition, for performance measurement, excluding individuals with clinically dominant conditions such as cancer or who are in their last years of life could be considered.29 These approaches have been used in performance measurement of other conditions,30 are consistent with guidelines,31–33 and acknowledge the importance of accounting for complexities in diabetes management in patients with CIC rather than considering all patients equivalent for the purpose of performance measurement. Further research is needed to elucidate the mechanisms of these associations to improve performance measurement of optimal glycemic control.
References
Diabetes Control and Complications Trial Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med. 1993;329:977–86.
UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet. 1998;352:837–53.
National Quality Forum. Available at: http://www.qualityforum.org. Accessed April 29, 2007.
National Committee for Quality Assurance. HEDIS 2007 Volume 2, Technical Manual. Washington DC, 2006.
Ambulatory Care Quality Alliance. Recommended starter set: clinical performance measures for ambulatory care. Available at: http://www.ahrq.gov/qual/aqastart.htm. Accessed April 29, 2007.
National Diabetes Quality Improvement Alliance. Available at: http://www.nationaldiabetesalliance.org/organizations.html. Accessed April 29, 2007.
Berlowitz DR, Ash AS, Hickey EC, Kader B, Friedman R, Moskowitz MA. Profiling outcomes of ambulatory care: casemix affects perceived performance. Med Care. 1998;36:928–33.
Zhang Q, Safford M, Ottenweller J, et al. Performance status of health care facilities changes with risk adjustment of HbA1c. Diabetes Care. 2000;23:919–27.
Weiner M, Long J. Cross-sectional versus longitudinal performance assessments in the management of diabetes. Med Care. 2004;42:II34–9.
Thompson W, Wang H, Xie M, et al. Assessing quality of diabetes care by measuring longitudinal changes in hemoglobin A1c in the Veterans Health Administration. Health Serv Res. 2005;40:1818–35.
Sundaram M, Kavookjian J, Patrick JH, Miller LA, Madhavan SS, Scott VG. Quality of life, health status and clinical outcomes in Type 2 diabetes patients. Qual Life Res. 2007;16:165–77.
De Rekeneire N, Resnick HE, Schwartz AV, et al. Diabetes is associated with subclinical functional limitation in nondisabled older individuals: the Health, Aging, and Body Composition study. Diabetes Care. 2003;26:3257–63.
Wendel CS, Shah JH, Duckworth WC, Hoffman RM, Mohler MJ, Murata GH. Racial and ethnic disparities in the control of cardiovascular disease risk factors in Southwest American veterans with type 2 diabetes: the Diabetes Outcomes in Veterans Study. BMC Health Serv Res. 2006;6:58.
Joish VN, Malone DC, Wendel C, Mohler MJ. Profiling quality of diabetes care in a Veterans Affairs Healthcare System. Am J Med Qual. 2004;19:112–20.
Piette JD, Kerr EA. The impact of comorbid chronic conditions on diabetes care. Diabetes Care. 2006;29:725–31.
Frayne SM, Halanych JH, Miller DR, et al. Disparities in diabetes care: impact of mental illness. Arch Intern Med. 2005;165:2631–8.
Miller DR, Safford MM, Pogach LM. Who has diabetes? Best estimates of diabetes prevalence in the Veterans Health Administration based on computerized patient data. Diabetes Care. 2004;27:B10–21.
Byrne MM, Kuebeler M, Pietz K, Petersen LA. Effect of using information from only one system for dually eligible health care users. Med Care. 2006;44:768–73.
Kerr EA, Smith DM, Hogan MH, et al. Comparing clinical automated, medical record, and hybrid data sources for diabetes quality measures. Jt Comm J Qual Improv. 2002;28:555–65.
Pogach L, Engelgau M, Aron D. Measuring progress toward achieving hemoglobin A1c goals in diabetes care: pass/fail or partial credit. JAMA. 2007;297:520–3.
Selim AJ, Fincke G, Ren XS, et al. Comorbidity assessments based on patient report: results from the Veterans Health Study. J Ambul Care Manage. 2004;27:281–95.
Selby JV, Karter AJ, Ackerson LM, Ferrara A, Liu J. Developing a prediction rule from automated clinical databases to identify high-risk patients in a large population with diabetes. Diabetes Care. 2001;24:1547–55.
Reker DM, Rosen AK, Hoenig H, et al. The hazards of stroke case selection using administrative data. Med Care. 2002;40:96–104.
Helmer DA, Tseng CL, Brimacombe M, Rajan M, Stiptzarov N, Pogach L. Applying diabetes-related prevention quality indicators to a national cohort of veterans with diabetes. Diabetes Care. 2003;26:3017–23.
Turner RC, Cull CA, Frighi V, Holman RR. Glycemic control with diet, sulfonylurea, metformin, or insulin in patients with type 2 diabetes mellitus: progressive requirement for multiple therapies (UKPDS 49). UK Prospective Diabetes Study (UKPDS) Group. JAMA. 1999;281:2005–12.
Helmer D, Sambamoorthi U, Rajan M, Tiwari A, Pogach LM. A comparison of care quality between patients who rely on an integrated healthcare delivery system and those who obtain care outside the system. Annual meeting of the Society of General Internal Medicine, New Orleans, LA, May 2005.
Rosenstock J, Dailey G, Massi-Benedetti M, Fritsche A, Lin Z, Salzman A. Reduced hypoglycemia risk with insulin glargine: a meta-analysis comparing insulin glargine with human NPH insulin in type 2 diabetes. Diabetes Care. 2005;28:950–5.
Selvin E, Marinopoulos S, Berkenblit G, et al. Meta-analysis: glycosylated hemoglobin and cardiovascular disease in diabetes mellitus. Ann Intern Med. 2004;141:421–31.
Pogach LM, Tiwari A, Maney M, Rajan M, Miller DR, Aron D. Should mitigating comorbidities be considered in assessing healthcare plan performance in achieving optimal glycemic control? Am J Manag Care. 2007;13:133–40.
Rathore SS, Wang Y, Radford MJ, Ordin DL, Krumholz HM. Quality of care of Medicare beneficiaries with acute myocardial infarction: who is included in quality improvement measurement? J Am Geriatr Soc. 2003;51:466–75.
American Diabetes Association. Standards of medical care for patients with diabetes mellitus. Diabetes Care. 2006;29:S4–S42.
Veterans Health Administration. VHA/DoD Clinical Practice Guidelines for Management of Diabetes Mellitus. Available at: http://www.oqp.med.va.gov/cpg/DM/DM_base.htm. Accessed April 29, 2007.
Brown AF, Mangione CM, Saliba D, Sarkisian CA. California Healthcare Foundation/American Geriatrics Society Panel on Improving Care for Elders with Diabetes. Guidelines for improving the care of the older person with diabetes mellitus. J Am Geriatr Soc. 2003;51:S265–80.
Acknowledgment
This research was supported by VHA Clinical Services Research and Development grants and Health Services Research and Development grants REA-03-021 and IIR 00-072-1 (Dr. Pogach), IEA-05-255 and IIR 05-016 (Dr. Sambamoorthi), and a Research Career Development Award RC002-041-2 (Dr. Helmer). Dr. Meduru is supported by a War-Related Illness and Injury Study Center Post-Doctoral Fellowship funded through the VHA Office of Academic Affiliations. The authors would like to thank Dr. Anjali Tiwari for her assistance in this research. The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the VHA or any other organizations.
Conflicts of interest
Authors Pramod Meduru, Drew Helmer, Chin-Lin Tseng, Leonard Pogach, and Usha Sambamoorthi report no potential conflicts of interest. Author Mangala Rajan reports involvement in a consultancy with Sanofi-Aventis within the last 3 years.
Author information
Authors and Affiliations
Corresponding author
APPENDIX A
APPENDIX A
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License ( https://creativecommons.org/licenses/by-nc/2.0 ), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Meduru, P., Helmer, D., Rajan, M. et al. Chronic Illness with Complexity: Implications for Performance Measurement of Optimal Glycemic Control. J GEN INTERN MED 22 (Suppl 3), 408–418 (2007). https://doi.org/10.1007/s11606-007-0310-5
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11606-007-0310-5