
Abstract
Background
Previous studies have shown that curative resection (R0 resection) was among the most crucial factors for the long-term survival of patients with PHCC. To achieve R0 resection, we performed the transhepatic direct approach and resection on the limits of division of the hepatic ducts. Although a recent report showed that the resection margin (RM) status impacted PHCC patients’ survival, it is still unclear whether RM is an important clinical factor.
Objective
To describe a technique of transhepatic direct approach and resection on the limit of division of hepatic ducts, investigate its short-term surgical outcome, and validate whether the radial margin (RM) would have a clinical impact on long-term survival of perihilar cholangiocarcinoma (PHCC) patients.
Methods
Consecutive PHCC patients (n = 211) who had undergone major hepatectomy with extrahepatic bile duct resection, without pancreaticoduodenectomy, in our department were retrospectively evaluated.
Results
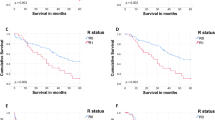
R0 resection rate was 92% and 86% for invasive cancer-free and both invasive cancer-free and high-grade dysplasia-free resection, respectively. Overall 5-year survival rate was 46.9%. Univariate analysis showed that preoperative serum carcinoembryonic antigen level (> 7.0 mg/dl), pathological lymph node metastasis, and portal vein invasion were independent risk factors, but R status on both resection margin and bile duct margin was not an independent risk factor for survival.
Conclusion
The transhepatic direct approach to the limits of division of the bile ducts leads to the highest R0 resection rate in the horizontal margin of PHCC. Further examination will be needed to determine the adjuvant therapy for PHCC to improve patient survival.




Similar content being viewed by others


References
Kondo S, Hirano S, Ambo Y, Tanaka E, Okushiba S, Morikawa T et al. Forty consecutive resections of hilar cholangiocarcinoma with no postoperative mortality and no positive ductal margins: results of a prospective study. Ann Surg. 2004;240(1):95-101.
Shinohara K, Ebata T, Shimoyama Y, Mizuno T, Yokoyama Y, Yamaguchi J et al. A Study on Radial Margin Status in Resected Perihilar Cholangiocarcinoma. Ann Surg. 2019. doi:https://doi.org/10.1097/SLA.0000000000003305.
Lee SG, Song GW, Hwang S, Ha TY, Moon DB, Jung DH et al. Surgical treatment of hilar cholangiocarcinoma in the new era: the Asan experience. J Hepatobiliary Pancreat Sci. 2010;17(4):476-89. doi:https://doi.org/10.1007/s00534-009-0204-5.
Shimizu H, Kimura F, Yoshidome H, Ohtsuka M, Kato A, Yoshitomi H et al. Aggressive surgical resection for hilar cholangiocarcinoma of the left-side predominance: radicality and safety of left-sided hepatectomy. Ann Surg. 2010;251(2):281-6. doi:https://doi.org/10.1097/SLA.0b013e3181be0085.
Matsuo K, Rocha FG, Ito K, D'Angelica MI, Allen PJ, Fong Y et al. The Blumgart preoperative staging system for hilar cholangiocarcinoma: analysis of resectability and outcomes in 380 patients. J Am Coll Surg. 2012;215(3):343-55. doi:https://doi.org/10.1016/j.jamcollsurg.2012.05.025.
Cheng QB, Yi B, Wang JH, Jiang XQ, Luo XJ, Liu C et al. Resection with total caudate lobectomy confers survival benefit in hilar cholangiocarcinoma of Bismuth type III and IV. Eur J Surg Oncol. 2012;38(12):1197-203. doi:https://doi.org/10.1016/j.ejso.2012.08.009.
Song SC, Choi DW, Kow AW, Choi SH, Heo JS, Kim WS et al. Surgical outcomes of 230 resected hilar cholangiocarcinoma in a single centre. ANZ J Surg. 2013;83(4):268-74. doi:https://doi.org/10.1111/j.1445-2197.2012.06195.x.
Furusawa N, Kobayashi A, Yokoyama T, Shimizu A, Motoyama H, Miyagawa S. Surgical treatment of 144 cases of hilar cholangiocarcinoma without liver-related mortality. World J Surg. 2014;38(5):1164-76. doi:https://doi.org/10.1007/s00268-013-2394-x.
Higuchi R, Yazawa T, Uemura S, Izumo W, Ota T, Kiyohara K et al. Surgical Outcomes for Perihilar Cholangiocarcinoma with Vascular Invasion. J Gastrointest Surg. 2019;23(7):1443-53. doi:https://doi.org/10.1007/s11605-018-3948-x.
Matsuyama R, Morioka D, Mori R, Yabushita Y, Hiratani S, Ota Y et al. Our Rationale of Initiating Neoadjuvant Chemotherapy for Hilar Cholangiocarcinoma: A Proposal of Criteria for "Borderline Resectable" in the Field of Surgery for Hilar Cholangiocarcinoma. World J Surg. 2019;43(4):1094-104. doi:https://doi.org/10.1007/s00268-018-04883-y.
Olthof PB, Miyasaka M, Koerkamp BG, Wiggers JK, Jarnagin WR, Noji T et al. A comparison of treatment and outcomes of perihilar cholangiocarcinoma between Eastern and Western centers. HPB (Oxford). 2019;21(3):345-51. doi:https://doi.org/10.1016/j.hpb.2018.07.014.
Tran TB, Ethun CG, Pawlik TM, Schmidt C, Beal EW, Fields RC et al. Actual 5-Year Survivors After Surgical Resection of Hilar Cholangiocarcinoma. Ann Surg Oncol. 2019;26(2):611-8. doi:https://doi.org/10.1245/s10434-018-7075-4.
Hirano S, Tanaka E, Shichinohe T, Suzuki O, Hazama K, Kitagami H et al. Treatment strategy for hilar cholangiocarcinoma, with special reference to the limits of ductal resection in right-sided hepatectomies. J Hepatobiliary Pancreat Surg. 2007;14(5):429-33. doi:https://doi.org/10.1007/s00534-006-1190-5.
De Lu C, Huang J, Wu SD, Hua YF, Javed AA, Fang JZ et al. Total Hilar En Bloc Resection with Left Hemihepatectomy and Caudate Lobectomy: a Novel Approach for Treatment of Left-Sided Perihilar Cholangiocarcinoma (with Video). J Gastrointest Surg. 2017;21(11):1906-14. doi:https://doi.org/10.1007/s11605-017-3561-4.
Kamachi H, Kamiyama T, Tsuruga Y, Orimo T, Wakayama K, Shimada S et al. Transparenchymal glissonean approach: a novel surgical technique for advanced perihilar bile duct cancer. Langenbecks Arch Surg. 2018;403(3):387-94. doi:https://doi.org/10.1007/s00423-017-1633-2.
Kuriyama N, Isaji S, Tanemura A, Iizawa Y, Kato H, Murata Y et al. Transhepatic Hilar Approach for Perihilar Cholangiocarcinoma: Significance of Early Judgment of Resectability and Safe Vascular Reconstruction. J Gastrointest Surg. 2017;21(3):590-9. doi:https://doi.org/10.1007/s11605-016-3332-7.
Nagino M, Kamiya J, Arai T, Nishio H, Ebata T, Nimura Y. "Anatomic" right hepatic trisectionectomy (extended right hepatectomy) with caudate lobectomy for hilar cholangiocarcinoma. Ann Surg. 2006;243(1):28-32. doi:https://doi.org/10.1097/01.sla.0000193604.72436.63.
Uesaka K. Left hepatectomy or left trisectionectomy with resection of the caudate lobe and extrahepatic bile duct for hilar cholangiocarcinoma (with video). J Hepatobiliary Pancreat Sci. 2012;19(3):195-202. doi:https://doi.org/10.1007/s00534-011-0474-6.
Govil S, Reddy MS, Rela M. Surgical resection techniques for locally advanced hilar cholangiocarcinoma. Langenbecks Arch Surg. 2014;399(6):707-16. doi:https://doi.org/10.1007/s00423-014-1216-4.
Noji T, Okamura K, Tanaka K, Nakanishi Y, Asano T, Nakamura T et al. Surgical technique and results of intrapancreatic bile duct resection for hilar malignancy (with video). HPB (Oxford). 2018;20(12):1145-9. doi:https://doi.org/10.1016/j.hpb.2018.05.010.
Nakanishi Y, Tsuchikawa T, Okamura K, Nakamura T, Tamoto E, Murakami S et al. Prognostic impact of the site of portal vein invasion in patients with surgically resected perihilar cholangiocarcinoma. Surgery. 2016;159(6):1511-9. doi:https://doi.org/10.1016/j.surg.2016.01.012.
Noji T, Tsuchikawa T, Okamura K, Tanaka K, Nakanishi Y, Asano T et al. Concomitant hepatic artery resection for advanced perihilar cholangiocarcinoma: a case-control study with propensity score matching. J Hepatobiliary Pancreat Sci. 2016;23(7):442-8. doi:https://doi.org/10.1002/jhbp.363.
Kawamura T, Noji T, Okamura K, Tanaka K, Nakanishi Y, Asano T et al. Postoperative Liver Failure Criteria for Predicting Mortality after Major Hepatectomy with Extrahepatic Bile Duct Resection. Dig Surg. 2019;36(2):158-65. doi:https://doi.org/10.1159/000486906.
Hirano S, Kondo S, Tanaka E, Shichinohe T, Tsuchikawa T, Kato K et al. Outcome of surgical treatment of hilar cholangiocarcinoma: a special reference to postoperative morbidity and mortality. J Hepatobiliary Pancreat Sci. 2010;17(4):455-62. doi:https://doi.org/10.1007/s00534-009-0208-1.
Kawakami H, Kuwatani M, Onodera M, Haba S, Eto K, Ehira N et al. Endoscopic nasobiliary drainage is the most suitable preoperative biliary drainage method in the management of patients with hilar cholangiocarcinoma. J Gastroenterol. 2011;46(2):242-8. doi:https://doi.org/10.1007/s00535-010-0298-1.
Yokoyama Y, Nishio H, Ebata T, Igami T, Sugawara G, Nagino M. Value of indocyanine green clearance of the future liver remnant in predicting outcome after resection for biliary cancer. Br J Surg. 2010;97(8):1260-8. doi:https://doi.org/10.1002/bjs.7084.
Ikeyama T, Nagino M, Oda K, Ebata T, Nishio H, Nimura Y. Surgical approach to bismuth Type I and II hilar cholangiocarcinomas: audit of 54 consecutive cases. Ann Surg. 2007;246(6):1052-7. doi:https://doi.org/10.1097/SLA.0b013e318142d97e.
Ebata T, Mizuno T, Yokoyama Y, Igami T, Sugawara G, Nagino M. Surgical resection for Bismuth type IV perihilar cholangiocarcinoma. Br J Surg. 2017. doi:https://doi.org/10.1002/bjs.10556.
Noji T, Hirano S. Surgical indication and procedure for perihilar cholangiocarcinoma with Bismuth type III or IV. Geka. 2017;79(8):714-9.
Natsume S, Ebata T, Yokoyama Y, Igami T, Sugawara G, Shimoyama Y et al. Clinical significance of left trisectionectomy for perihilar cholangiocarcinoma: an appraisal and comparison with left hepatectomy. Ann Surg. 2012;255(4):754-62. doi:https://doi.org/10.1097/SLA.0b013e31824a8d82.
Clavien PA, Strasberg SM. Severity grading of surgical complications. Ann Surg. 2009;250(2):197-8. doi:https://doi.org/10.1097/SLA.0b013e3181b6dcab.
Primrose JN, Fox RP, Palmer DH, Malik HZ, Prasad R, Mirza D et al. Capecitabine compared with observation in resected biliary tract cancer (BILCAP): a randomised, controlled, multicentre, phase 3 study. Lancet Oncol. 2019;20(5):663-73. doi:https://doi.org/10.1016/s1470-2045(18)30915-x.
Ebata T, Hirano S, Konishi M, Uesaka K, Tsuchiya Y, Ohtsuka M et al. Randomized clinical trial of adjuvant gemcitabine chemotherapy versus observation in resected bile duct cancer. Br J Surg. 2018;105(3):192-202. doi:https://doi.org/10.1002/bjs.10776.
Saito H, Noji T, Okamura K, Tsuchikawa T, Shichinohe T, Hirano S. A new prognostic scoring system using factors available preoperatively to predict survival after operative resection of perihilar cholangiocarcinoma. Surgery. 2016;159(3):842-51. doi:https://doi.org/10.1016/j.surg.2015.10.027.
Ferrone CR, Marchegiani G, Hong TS, Ryan DP, Deshpande V, McDonnell EI et al. Radiological and surgical implications of neoadjuvant treatment with FOLFIRINOX for locally advanced and borderline resectable pancreatic cancer. Ann Surg. 2015;261(1):12-7. doi:https://doi.org/10.1097/SLA.0000000000000867.
Khushman M, Dempsey N, Maldonado JC, Loaiza-Bonilla A, Velez M, Carcas L et al. Full dose neoadjuvant FOLFIRINOX is associated with prolonged survival in patients with locally advanced pancreatic adenocarcinoma. Pancreatology. 2015;15(6):667-73. doi:https://doi.org/10.1016/j.pan.2015.08.010.
Noji T, Kondo S, Hirano S, Tanaka E, Ambo Y, Kawarada Y et al. CT evaluation of paraaortic lymph node metastasis in patients with biliary cancer. J Gastroenterol. 2005;40(7):739-43. doi:https://doi.org/10.1007/s00535-005-1618-8.
Noji T, Kondo S, Hirano S, Tanaka E, Suzuki O, Shichinohe T. Computed tomography evaluation of regional lymph node metastases in patients with biliary cancer. Br J Surg. 2008;95(1):92-6. doi:https://doi.org/10.1002/bjs.5920.
Kobayashi S, Nagano H, Hoshino H, Wada H, Marubashi S, Eguchi H et al. Diagnostic value of FDG-PET for lymph node metastasis and outcome of surgery for biliary cancer. J Surg Oncol. 2011;103(3):223-9. doi:https://doi.org/10.1002/jso.21811.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Rights and permissions
About this article

Cite this article
Noji, T., Tanaka, K., Matsui, A. et al. Transhepatic Direct Approach to the “Limit of the Division of the Hepatic Ducts” Leads to a High R0 Resection Rate in Perihilar Cholangiocarcinoma. J Gastrointest Surg 25, 2358–2367 (2021). https://doi.org/10.1007/s11605-020-04891-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-020-04891-1