
Abstract
Background
Multivisceral resection for T4b colon cancer constitutes a heterogeneous group of surgical procedures. The purpose of this study was to explore clinically distinct categories of multivisceral resection, with subsequent correlation to postoperative complications and oncological outcomes.
Methods
In this multicenter cohort study, all consecutive patients without metastases who underwent multivisceral resection for pT4bN0-2M0 colon cancer between 2000 and 2014 were included. Multivisceral resection was divided into four categories: (i) gastrointestinal (including the stomach), (ii) urologic ((partial) bladder and ureter), (iii) solid organ (spleen, kidney, liver, pancreas, and uterus), and (iv) abdominal wall/omentum/ovaries. The primary outcome was surgical complications and secondary outcomes were 5-year intra-abdominal recurrence, disease-free survival, and overall survival.
Results
In total, 130 patients who underwent curative intent resection of pT4 colon cancer were included. Patients who underwent multivisceral resection within multiple categories were assigned to one of the categories based on hierarchy of clinical impact after exploratory analysis. For the primary endpoint, 55 patients were assigned to gastrointestinal, 14 to urologic, 14 to solid organ, and 47 to abdominal wall/omentum/ovaries multivisceral resection. Gastrointestinal multivisceral resection was independently associated with surgical complications (HR 3.9, 95% CI 1.4–10.6). Abdominal wall/omentum/ovaries multivisceral resection was significantly related with intra-abdominal recurrence (HR 7.8, 95% CI 1.0–57.8). The 5-year disease-free survival and overall survival showed no significant differences per multivisceral resection category.
Conclusions
Multivisceral resections for T4b colon cancer are heterogeneous procedures considering risk profiles. The proposed multivisceral resection subclassification needs validation, but might improve comparability between studies and hospitals (auditing).
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Approximately 5% of patients with colon cancer already have invasion of adjacent organs or structures (stage T4b) at time of presentation.1 For these patients, a multivisceral resection (MVR) is required to achieve curative intent surgery (R0-resection). Reported postoperative complication rates after MVR are relatively high (> 30%), with local recurrence rates around 10% and 5-year overall survival around 50%.2
MVR for colon cancer constitutes a heterogeneous group of surgical procedures, varying from an en bloc resection of adherent peritoneum to cystectomy with Bricker deviation. Despite the assumption that these different procedures have a different risk profile, no attempt to further categorize MVRs has yet been made. Recognizing different risks of surgery is relevant for informing patients preoperatively and could endorse tailored operative risk management or follow-up strategies. Furthermore, in the era of centralization of low-volume care with high complexity, it is important to specifically define high-risk surgical procedures. Subsequent benchmarking requires adequate case mix correction in the context of clinical auditing. So far, data on MVR for locally advanced colorectal cancer are mainly based on relatively small cohorts with restricted details on the different surgical procedures that were performed, and predominantly including rectal cancer patients.3,4,5,6,7
The aim of this international multicenter trial was to explore subcategories of MVR for T4b colon cancer and to evaluate the association of these subcategories with postoperative surgical complications as primary outcome, with oncological outcomes as secondary outcome parameters.
Materials and Methods
Patients and Databases
Four prospectively maintained T4 colon cancer databases of the University Hospital Leuven in Belgium, the Dutch teaching hospital St. Antonius, and two Dutch university medical centers (Radboud UMC and Amsterdam UMC) were combined. All consecutive patients undergoing curative intent MVR (R0/R1) for primary T4bN0-2M0 colon cancer between January 2004 and July 2013 (UH Leuven), January 2000 and December 2007 (St. Antonius), January 2000 and December 2013 (Radboud UMC), and January 2004 and December 2014 (Amsterdam UMC) were included. Patients were excluded when they were known with distant metastatic disease at time of diagnosis (M1), and when pathological or surgical report was missing. According to the national guidelines, adjuvant chemotherapy was recommended in high-risk stage II and stage III colon cancer for a total duration of 6 months. In the first years of the study period, adjuvant chemotherapy consisted of fluoropyrimidine monotherapy (5-flourouracil or capecitabine); since 2005, oxaliplatin (FOLFOX or CAPOX) was preferably added. Oncological follow-up lasted 5 years, including colonoscopy, abdominal ultrasound or CT, chest radiography, and tumor markers during regular outpatient clinic visits. Survival status was updated on October 2018. This study was waived from review of the medical ethics boards. Reporting of the data adheres to the STROBE Statement.
MVR Classification
MVRs were subdivided based on the involved structures and clustered based on both belonging to a certain tract and generally considered similarity regarding impact on surgical complications and/or peritoneal recurrence. MVR categories were defined before any analysis of the data: (i) gastrointestinal, defined as additional bowel resection with or without extra anastomosis and/or partial gastric resection; (ii) urologic, containing additional resection of (partial) bladder and/or ureter; (iii) (parts of) solid organs, such as the pancreas, spleen, kidney, liver, or uterus; and (iv) abdominal wall/omentum/ovaries. When (parts of) solid organs were resected, it was because of invasion from the primary tumor, and not because of distant metastases. Although the ovary can be considered a solid organ, it was decided to categorize this together with the abdominal wall and omentum based on the considered low impact on surgical complications, and all being target organs for peritoneal metastases. In exploratory analyses, the outcome measure was assessed when only one category was involved and also when structures from other categories were resected besides the category of interest. A hierarchy was made in MVR categories based on clinical impact, from highest to lowest using the derived HRs with 95% confidence intervals. Patients who underwent MVR within multiple categories were subsequently assigned to the MVR category of highest impact first, and then to the second, third, and fourth category with decreasing clinical impact. For example, if a patient underwent both resection of small bowel and abdominal wall, the patient was categorized to gastrointestinal MVR based on exploratory analysis that showed a higher risk of complications related to the additional bowel resection if compared to excision of part of the abdominal wall.
Removal of organs not adjacent to the tumor, such as cholecystectomy for symptomatic gallstone disease or splenic resection for iatrogenic injury, was not considered MVR for the purpose of this study.
Variables and Outcomes
The primary outcome was surgical complications within 30 days or during hospitalization, including postoperative surgical site infection (SSI), containing deep incisional and organ/space SSIs (i.e., anastomotic leakage and abdominal abscess), ileus in the absence of a SSI, and postoperative bleeding.8 The patient files were retrospectively reviewed to extract particulars of these complications. Surgical complications were categorized in accordance with the Clavien-Dindo (CD) score. Only CD scores of ≥ 2 were extracted for analysis, as retrospective data collection was considered not accurate enough to identify CD 1.9 Secondary outcomes were intra-abdominal recurrence rate, 5-year disease-free survival (DFS), and overall survival (OS). Intra-abdominal recurrence was defined as any potential site of outgrowth of free intraperitoneal cancer cells including incisional, local recurrence, ovarian, omental, and peritoneal metastases. Pathology reports were reviewed for pathological staging and MVR classification. T4b colon cancer was defined according to TNM7.10 Completeness of resection was classified as R0 (radical) and R1 (microscopic irradical) resection.
Statistical Analysis
Differences in baseline characteristics between the MVR groups were assessed using a chi-square test, or a Fisher’s exact test, as appropriate. Continuous variables were reported as mean and standard deviation (SD). The primary outcome (surgical complications) was analyzed using logistic regressing. Variables were included in the model based on a directed acyclic graph (DAG),11 in which identified (potential) confounders from previous series were incorporated.12,13,14 Additionally, Bonferroni correction was used to correct for multiple testing. Potential confounders associated with oncological outcomes (intra-abdominal recurrence, OS, and DFS) were also based on literature and were identified using cox regression.15,16 Variables were included in the multivariable model when the p value was < 0.10 in the univariable analyses. Multicollinearity was assessed for all multivariable analyses. Due to multicollinearity between MVR category and type of segmental colectomy, the latter was not included in any model. Concerning oncological outcomes, Kaplan-Meier analyses with log-rank test were used. Statistical significance was defined as a p value of < 0.05. PASW Statistics, version 24 (SPSS inc., Chicago, IL) was used.
Results
Patients
A total of 707 patients with primary pT4 colon cancer underwent a macroscopic complete (R0/R1) resection (Supplementary Figure 1). Of these, 321 patients and 256 patients were excluded because of T4a stage and M1 disease at diagnosis respectively, resulting in the inclusion of 130 patients with a mean age 68 years and 53% of males. The number of MVRs for T4b colon cancer per hospital was 39 in the St. Antonius Hospital, 36 in the Radboud UMC, 34 in the UH Leuven, and 21 in the Amsterdam UMC. Laparoscopic surgery was performed in 25 patients (19%) with a conversion rate of 32%.
Out of 130 included patients, 86 patients underwent MVR restricted to a single category, whereas 44 had a MVR procedure belonging to multiple subcategories. Out of the 86 MVRs restricted to a single category, 47 were MVR including abdominal wall/omentum/ovaries, 22 gastrointestinal MVR, 8 urologic MVR, and 9 MVRs included (parts of) a solid organ. When including combined MVR categories, 70 patients underwent abdominal wall/omentum/ovaries MVR, 55 patients gastrointestinal MVR, 32 patients urologic MVR, and 30 patients MVR including (parts of) solid organs. All the different subcategories of MVR and combinations are specified in Supplementary Table 1.
In 97% of patients, the baseline data were complete, and the lost to follow-up rate was 14%, of which half completed 3-year follow-up.
MVR Subcategories Based on Surgical Complications
Explorative analyses using surgical complications as outcome parameter revealed that gastrointestinal MVRs had the strongest association with surgical complications, followed by urologic MVRs, MVRs including (parts of) solid organs, and abdominal wall/omentum/ovaries MVRs (Table 1). Using this hierarchy, 55 patients (42%) were assigned to the gastrointestinal MVR group, 14 (11%) to the urologic MVR group, 14 (11%) to the group with MVRs including (parts of) solid organs, and 47 (36%) to the abdominal wall/omentum/ovaries MVR group.
The baseline characteristics of the included patients are shown in Table 2 (Supplementary Table 2 shows baseline characteristics without assignment to one specific category). Tumor location, surgical procedure, and N-stage significantly differed between the four MVR categories. Patients in the gastrointestinal MVR category most often had stage II disease (75%). Patients undergoing urologic MVR had a left-sided tumor in 93% and N2-stage in 31%. In the abdominal wall/omentum/ovaries MVR group, right-sided tumors (66%) were overrepresented.
The overall surgical complication rate was 35%. This was 49% after gastrointestinal MVR, 29% after urologic MVR, 36% after MVR including (parts of) solid organs, and 19% after abdominal wall/omentum/ovaries MVR (Supplementary Table 3a). Emergency surgery, higher ASA, and open surgery were included in the regressions analysis (Supplementary Figure 2). Gastrointestinal MVR was independently associated with surgical complications (HR 3.89; 95% CI 1.42–10.64, corrected p = 0.048) as shown in Table 3. Furthermore, gastrointestinal MVR (HR 3.45; 95% CI 1.15–10.77, corrected p = 0.198) seemed associated with severe complications (CD ≥ 3) (Supplementary Table 3b). Performing a subanalysis for gastrointestinal MVR patients with and without surgical complications showed that, especially for patients with a combined gastrointestinal/urologic MVR, the complication rate was high (Supplementary Table 3c).
MVR Subcategories Based on Oncological Outcomes
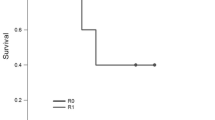
The overall median follow-up was 56 months (IQR 22–60). After exploratory analyses to assess intra-abdominal recurrence in the total patient group (Table 1) and in the patients with MVR belonging to a single category, MVRs were assigned to the four categories in the following order based on clinical impact: 1. Abdominal wall/omentum/ovaries MVRs; 2. MVRs including (parts of) solid organs; 3. urologic MVR; and 4. gastrointestinal MVRs. Overall 5-year intra-abdominal recurrence was 26%. Intra-abdominal recurrence rates for the different categories of MVRs were 36.6% after abdominal wall/omentum/ovaries MVRs; 18.7% after MVRs including (parts of) solid organs; 12.5% after urologic MVRs; and 5.9% after gastrointestinal MVR (log rank, p = 0.041). After multivariable analysis, including age, radicality, and surgical site infections in the model, a high association between MVR abdominal wall/omentum/ovaries and intra-abdominal recurrence was seen (HR 7.8; 95% CI 1.0–57.8, p = 0.046, Table 4). No significant association was found of MVR type and 5-year DFS and 5-year OS after multivariable analyses (Supplementary Table 4a and b).
Discussion and Conclusion
In this multicenter cohort study including 130 MVRs for T4b colon cancer, a classification with four categories was defined prior to any analysis of the data, based on expected differences in clinical impact. Gastrointestinal MVR combined with or without other categories, was independently associated with postoperative surgical complications if compared to other MVR categories. Almost half of these patients had at least one surgical complication. Regarding oncological outcomes, MVR of the abdominal wall, omentum, or ovaries was independently associated with intra-abdominal recurrence. No significant impact between MVR category and DFS or OS was observed.
So far, no classifications of MVRs have been described in the literature. Published data on MVR for T4b colon cancer are scarce, as most reports include rectal cancer.17 As most of rectal cancers are located extraperitoneally, the surgical implications and pathophysiology of metastatic invasion seem to be different if compared to the intraperitoneal location of colon cancers. Therefore, also from the perspective of MVR for locally advanced disease, colon and rectal cancer are two distinct clinical entities that require a different surgical approach and might have different risk profiles. Only small case series on MVR for colon cancer have been published, with overall complication rates varying between 28 and 48%, recurrence rates between 48 and 86%, and OS between 42 and 74%.13,18,19,20 These results are consistent with the overall outcomes of the present study.
MVR subclassification can potentially be used to define high-risk MVRs. Consequently, it could guide the discussion of centralized care and be used for benchmarking between centers or between countries. The high association of gastrointestinal MVR with surgical complications could be due to more left-sided resections that are more prone for complications and more often involve the urologic tract. In contrast, abdominal wall/omentum/ovaries MVR was more often associated with right-sided tumors and less often combined with the more high-risk gastrointestinal and urologic MVR categories.
It could be argued that high-risk MVRs should be referred to a limited number of centers, to increase volumes and expertise, which might subsequently improve outcomes. In addition, the risk stratification following the MVR subclassification is of great importance for preoperative patient consultation, especially in the era of shared decision-making. For example, patients with known comorbidities who are planned to undergo gastrointestinal MVRs should probably receive a more tailored and intensified perioperative care.
Interestingly, gastrointestinal MVR tended to have most favorable oncological outcomes, whereas abdominal wall/omentum/ovaries MVR showed the highest association with intra-abdominal recurrence. This group predominantly included abdominal wall resections. This is an interesting hypothesis generating finding. One might suggest that a process of adhesion to adjacent bowel might be part of an inflammatory reaction around the tumor that precedes subsequent tumor infiltration. This could play a protective role, as it is assumed that a shield of adjacent bowel loops around the colon cancer might protect against intraperitoneal seeding of cancer cells.21 In other words, covering of a serosal site with peritumoral infiltration or minimal tumor penetration by bowel loops or stomach might prevent intraperitoneal dissemination at the time of transition from a T3 to T4 stage. In contrast, adequate coverage of a serosal site by adjacent abdominal wall is probably more difficult considering the restricted mobility in comparison to bowel loops, with more chance of intra-abdominal seeding of exfoliated tumor cells.
To our knowledge, this is the first study exploring associations of categories of MVR with surgical complications and oncological outcomes. The present findings therefore need validation in other cohorts, and one might even explore other subclassifications to look for clinically relevant discrimination of colon cancer patients that need complex surgery for a locally advanced disease. More specifically, we decided to separate the two gynecological organs within the proposed MVR classification, as hysterectomy results in a suture line with potential fistula formation to a bowel anastomosis, while resection of the ovaries is only associated with a minimal risk of surgical complications. However, these theoretical considerations warrant future studies to test the validity of separating the uterus and ovaries. The study is limited by the retrospective data collection, which might have caused an underestimation of postoperative complications due to restricted consistency of variable scoring. Furthermore, complications might have occurred after discharge or beyond the 30-day time frame, and not being captured due to incomplete registration of complications at the outpatient clinic or due to readmission at the local referring hospital. To optimize registration, the first two authors collected all the data and discussed complicated cases. All the pathology (both TNM staging and MVR) was reviewed and Clavien-Dindo grade 1 complications were not taken into account. Furthermore, there was no gold standard to assess intra-abdominal recurrence. Detection of peritoneal metastases can be problematic due to restricted sensitivity of current imaging modalities.
In conclusion, a subclassification of MVRs is a useful way to identify high-risk patients. Patients that underwent a gastrointestinal MVR were identified as having a higher risk of postoperative surgical complications, whereas those with MVRs including abdominal wall/omentum/ovaries were at a higher risk of intra-abdominal recurrences. Validation of this classification and subsequent implementation could be a step forward in facilitating cross-study comparisons, optimizing benchmarking of clinical performance and tailored perioperative care.
References
Govindarajan A, Coburn NG, Kiss A, Rabeneck L, Smith AJ, Law CHL. Population-based assessment of the surgical management of locally advanced colorectal cancer. J Natl Cancer Inst. 2006;98(20):1474-1481. https://doi.org/10.1093/jnci/djj396
Lehnert T, Methner M, Pollok A, Schaible A, Hinz U, Herfarth C. Multivisceral resection for locally advanced primary colon and rectal cancer: an analysis of prognostic factors in 201 patients. Ann Surg. 2002;235(2):217-225. https://doi.org/10.1097/00000658-200202000-00009
Mohan HM, Evans MD, Larkin JO, Beynon J, Winter DC. Multivisceral resection in colorectal cancer: a systematic review. Ann Surg Oncol. 2013;20(9):2929-2936. https://doi.org/10.1245/s10434-013-2967-9
Bartoş A, Bartoş D, Dunca F, et al. Multi-organ resections for colorectal cancer: analysis of potential factors with role in the occurrence of postoperative complications and deaths. Chirurgia (Bucur). 107(4):476-482. http://www.ncbi.nlm.nih.gov/pubmed/23025114. Accessed June 19, 2017.
Gezen C, Kement M, Altuntas YE, et al. Results after multivisceral resections of locally advanced colorectal cancers: an analysis on clinical and pathological t4 tumors. World J Surg Oncol. 2012;10(1):39. https://doi.org/10.1186/1477-7819-10-39
Park S, Lee YS. Analysis of the prognostic effectiveness of a multivisceral resection for locally advanced colorectal cancer. J Korean Soc Coloproctol. 2011;27(1):21-26. https://doi.org/10.3393/jksc.2011.27.1.21
Nakafusa Y, Tanaka T, Tanaka M, Kitajima Y, Sato S, Miyazaki K. Comparison of multivisceral resection and standard operation for locally advanced colorectal cancer: analysis of prognostic factors for short-term and long-term outcome. Dis Colon Rectum. 2004;47(12):2055-2063. https://doi.org/10.1007/s10350-004-0716-7
Ban KA, Minei JP, Laronga C, et al. American College of Surgeons and Surgical Infection Society: Surgical Site Infection Guidelines, 2016 Update. J Am Coll Surg. 2016;224(1):59-74. https://doi.org/10.1016/j.jamcollsurg.2016.10.029
Clavien PA, Barkun J, de Oliveira ML, et al. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg. 2009;250(2):187-196. https://doi.org/10.1097/SLA.0b013e3181b13ca2
Sobin L, Gospodarowicz M, Wittekind C. TNM Classification of Malignant Tumours, 7th Edition. Wiley. http://eu.wiley.com/WileyCDA/WileyTitle/productCd-1444332414.html. Published 2009.
Williams TC, Bach CC, Matthiesen NB, Henriksen TB, Gagliardi L. Directed acyclic graphs: a tool for causal studies in paediatrics. Pediatr Res. 2018;84(4):487-493. https://doi.org/10.1038/s41390-018-0071-3
Klaver CEL, Wasmann KATGM, Verstegen M, et al. Postoperative abdominal infections after resection of T4 colon cancer increase the risk of intra-abdominal recurrence. Eur J Surg Oncol. 2018;44(12):1880-1888. https://doi.org/10.1016/j.ejso.2018.09.016
Croner RS, Merkel S, Papadopoulos T, Schellerer V, Hohenberger W, Goehl J. Multivisceral resection for colon carcinoma. Dis Colon Rectum. 2009;52(8):1381-1386. https://doi.org/10.1007/DCR.0b013e3181ab580b
Mirnezami A, Mirnezami R, Chandrakumaran K, Sasapu K, Sagar P, Finan P. Increased Local Recurrence and Reduced Survival From Colorectal Cancer Following Anastomotic Leak. Ann Surg. 2011;253(5):890-899. https://doi.org/10.1097/SLA.0b013e3182128929
Segelman J, Granath F, Holm T, Machado M, Mahteme H, Martling A. Incidence, prevalence and risk factors for peritoneal carcinomatosis from colorectal cancer. Br J Surg. 2012;99(5):699-705. https://doi.org/10.1002/bjs.8679
Leijssen LGJ, Dinaux AM, Amri R, Kunitake H, Bordeianou LG, Berger DL. The Impact of a Multivisceral Resection and Adjuvant Therapy in Locally Advanced Colon Cancer. J Gastrointest Surg. October 2018. https://doi.org/10.1007/s11605-018-3962-z
Laurence G, Ahuja V, Bell T, Grim R, Ahuja N. Locally advanced primary recto-sigmoid cancers: Improved survival with multivisceral resection. Am J Surg. December 2016. https://doi.org/10.1016/j.amjsurg.2016.12.018
Cukier M, Smith AJ, Milot L, et al. Neoadjuvant chemoradiotherapy and multivisceral resection for primary locally advanced adherent colon cancer: a single institution experience. Eur J Surg Oncol. 2012;38(8):677-682. https://doi.org/10.1016/j.ejso.2012.05.001
Luna-Pérez P, Rodríguez-Ramírez SE, De La Barrera MG, Zeferino M, Labastida S. Multivisceral resection for colon cancer. J Surg Oncol. 2002;80(2):100-104. https://doi.org/10.1002/jso.10105
Lopez-Cano M, Manas MJ, Hermosilla E, Espin E. Multivisceral resection for colon cancer: analysis of prognostic factors. Dig Surg. 2010;27(3):238-245. https://doi.org/10.1159/000276974
De Sousa E Melo F, Wang X, Jansen M, et al. Poor-prognosis colon cancer is defined by a molecularly distinct subtype and develops from serrated precursor lesions. Nat Med. 2013;19(5):614-618. https://doi.org/10.1038/nm.3174
Author information
Authors and Affiliations
Contributions
JvdB, BvR, and IN take responsibility for integrity of prospectively maintaining the database. KW and CK had full access to all of the data in the study and take responsibility for the integrity of the data. PT was responsible for the study concept and design. KW, CK, and PT were responsible for the analysis and interpretation of data and drafting the manuscript. JvdB, IN, BvR, PT, AW, HvS, AD, and JdW were responsible for critical revision of the manuscript for important intellectual content.
Corresponding authors
Ethics declarations
Conflicts of Interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
The data were presented as a poster presentation at the European Society of Coloproctology, Berlin, Germany, 20–22 September 2017 and as a podium presentation at the Dutch Digestive Days, Veldhoven, The Netherlands, 5–6 October 2017.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

{kind=link}
Cite this article
Wasmann, K.A.T.G.M., Klaver, C.E.L., van der Bilt, J.D.W. et al. Subclassification of Multivisceral Resections for T4b Colon Cancer with Relevance for Postoperative Complications and Oncological Risks. J Gastrointest Surg 24, 2113–2120 (2020). https://doi.org/10.1007/s11605-019-04426-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-019-04426-3