
Abstract
Introduction
The long-term recurrence rate of ventral hernia repair is 20–50 %, with a higher rate of recurrence in cases that do not use mesh. Previous teachings have cautioned against the use of mesh in contaminated wounds. Therefore, emergent ventral hernia repair is often performed without the use of mesh. Our aim is to determine if mesh is used in these cases and its effect on 30-day wound-related morbidity using the American College of Surgeons National Surgery Quality Improvement Program database.
Methods
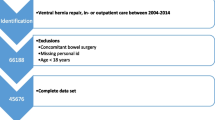
All emergency ventral hernia repairs performed from 2005 to 2013 were identified. The effect of mesh on postoperative morbidity and mortality was investigated. Significance was defined as p < 0.05.
Results
A total of 2449 patients met inclusion criteria. The use of mesh was associated with a significantly longer operative time for all wound classes and increased risk of return to the operating room in contaminated cases. Patients who returned to the operating room did not return to the OR for mesh or hernia-related complications.
Conclusions
Emergency ventral hernia repair with mesh can be safely performed without an increase in wound-related or additional 30-day patient morbidity or mortality. Additional studies are needed to determine the long-term outcomes of mesh utilization in this cohort.
Similar content being viewed by others


References
Choi JJ, Palaniappa NC, Dallas KB, et al. Use of Mesh During Ventral Hernia Repair in Clean-Contaminated and Contaminated Cases: Outcomes of 33,832 Cases. Ann Surg. 2012; 255.1: 176–180.
Viela PM, Thaina J, Ribeiro GG, et al. Laparoscopy Versus Laparotomy in the Repair of Ventral Hernias: Systematic Review and Meta-Analysis. Arq Gastroeneterol. 2014; 51.3: 205–211.
Altom LK, Synder CW, Gray SH, et al. Outcomes of Emergent Incisional Hernia Repair. Am Surg. 2011; 77: 971–976.
Carbonell AM, Criss CC, Cobb WS. Outcomes of Synthetic Mesh in Contaminated Ventral Hernia Repairs. J Am Coll Surg. 2013; 217.6: 991–998.
Zafar H, Zaidi M, Qadir I, et al. Emergency Incisional Hernia Repair: A Difficult Problem Waiting for a Solution. Ann Surg Innov Res. 2012; 6.1:1. doi: 10.1186/1750-1164-6-1.
Kelly ME and Behrman SW. The Safety and Efficacy of Prosthetic Hernia Repair in Clean-Contaminated and Contaminated Wounds. Ann Surg. 2002; 68.6: 524–528; Discussion 528–529.
Finan KR, Vick CC, Kiefe CI, et al. Predictors of Wound Infection in Ventral Hernia Repair. Am J Surg. 2005; 190: 676–681.
Breuing K, Butler CE, Ferzoco S, et al. Incisional Ventral Hernias: Review of the Literature and Recommendations Regarding the Grading and Technique of Repair. Surgery. 2010; 148.3: 544–558.
Rosen MJ, Audogdu K, Grafmiller K, et al. A Multidisciplinary Approach to Medical Weight Loss Prior to Complex Abdominal Wall Reconstruction: Is It Feasible? J Gastrointest Surg. 2015; 19: 1399–1406.
Dunne JR, Malone DL, Tracy JK, et al. Abdominal Wall Hernias: Risk Factors for Infection and Resource Utilization. J Surg Res. 2003; 111.1: 78–84.
Krpata DM, Blatnik JA, Novitsky YW, et al. Evaluation of High-Risk, Comorbid Patients Undergoing Open Ventral Hernia Repair with Synthetic Mesh. Surgery. 2013; 153.1: 120–125.
Pauli EM, Wang J, Petro CC, et al. Posterior Component Separation with Transversus Abdominis Release Successfully Addresses Recurrent Ventral Hernias following Anterior Component Separation. Hernia. 2015; 19.2: 285–291.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
None
Rights and permissions
About this article

Cite this article
Haskins, I.N., Amdur, R.L., Lin, P.P. et al. The Use of Mesh in Emergent Ventral Hernia Repair: Effects on Early Patient Morbidity and Mortality. J Gastrointest Surg 20, 1899–1903 (2016). https://doi.org/10.1007/s11605-016-3207-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11605-016-3207-y