
Abstract
Ethnic–racial discrimination, the differential treatment of individuals based on ethnic or racial group membership, predicts poor mental health outcomes such as anxiety. This is supported by long-standing theories on the social determinants of health and minority stress. However, these theories are rarely expanded to neurobiological sciences, limiting our understanding of mechanisms underlying observed associations. One potential neurobiological pathway between ethnic–racial discrimination exposure and anxiety is that ongoing exposure to racially charged encounters presents imminent threats that may modify stress-sensitive neurocircuitry, like the amygdala.
The current study evaluated whether amygdala volume mediated associations between ethnic–racial discrimination exposure and anxiety symptoms in Latina girls, a group exhibiting heightened levels of untreated anxiety and disproportionately subjected to ethnic–racial discrimination.
Thirty predominantly Mexican-identifying Latina girls residing in Southern California (MAge = 9.76, SD = 1.11 years) completed a T1-weighted structural MRI scan. Using the Perceptions of Racism in Children and Youth, participants self-reported the prevalence and severity of various discriminatory experiences. Participants also self-reported their anxiety symptoms via the Screen for Child Anxiety and Related Emotional Disorders. Controlling for total intracranial volume and annual household income, an indirect effect of ethnic–racial discrimination on anxiety symptoms via left amygdala volume was observed, β = −0.28, SE = 0.17, BC 95% CI [−0.690, −0.017]. The current findings suggest that the left amygdala is sensitive to racialized threats in childhood and that stress-related alterations may, in part, contribute to elevated anxiety in Latina girls. Our data elucidate a potential mechanism by which this form of sociocultural stress can adversely impact mental health, particularly in the transition from middle childhood to early adolescence, a period marked by a host of interlinked neurophysiological and social changes.
Zusammenfassung
Ethnische oder rassistische Diskriminierung, d. h. die unterschiedliche Behandlung von Menschen aufgrund rassistischer oder ethnisch-diskriminierender Zuschreibungen von Gruppenzugehörigkeiten, ist mit schädlichen Folgen für die psychische Gesundheit assoziiert. Langjährige Theorien zu den sozialen Determinanten der Gesundheit und Minderheitenstress unterstützen solche Beobachtungen. Diese Theorien werden jedoch selten in die neurobiologischen Wissenschaften erweitert, was unser Verständnis von Mechanismen einschränkt. Ein möglicher neurobiologischer Pfad zwischen Diskriminierungserfahrungen und Angststörungen ist, dass die ständige Bedrohung rassistisch motivierter Begegnungen stressempfindliche neuronale Schaltkreise des Gehirns, wie zum Beispiel die Amygdala, verändern kann.
In dieser Studie wurde untersucht, ob das Amygdala-Volumen eine vermittelnde Rolle zwischen ethnisch-rassistischen Diskriminierungserfahrungen und Angstsymptomen von Latina-Mädchen spielt. Latina-Mädchen haben oft erhöhte Angststörungen und sind in den Vereinigten Staaten von Amerika häufig ethnischer und rassistischer Diskriminierung ausgesetzt.
Dreißig überwiegend mexikanisch identifizierte Latina-Mädchen aus Südkalifornien (M = 9,76, SD = 1,11 Jahre) nahmen an einem T1-gewichteten strukturellen MRI-Scan teil. Teilnehmerinnen berichteten über die Prävalenz und Schwierigkeit verschiedener diskriminierender Erfahrungen. Sie berichteten auch über ihre Angstsymptome. Beobachtet wurde eine indirekte Auswirkung ethnisch-rassistischer Diskriminierung auf Angstsymptome über das Volumen der linken Amygdala (β = −0,28, SE = 0,17, BC 95 % KI [−0,690, −0,017]), nach Kontrolle des gesamten intrakraniellen Volumens und des jährlichen Haushaltseinkommens. Diese Erkenntnisse deuten darauf hin, dass die linke Amygdala empfindlich auf rassistische Bedrohungen reagiert und dass stressbedingte Veränderungen bei Latina-Mädchen teilweise zu erhöhter Angst beitragen können. Unsere Daten verdeutlichen einen möglichen Mechanismus, durch den diese Form von soziokulturellem Stress sich negativ auf die psychische Gesundheit auswirkt, insbesondere während der mittleren Kindheit bis zur frühen Adoleszenz, einer Zeitspanne, die von einer Vielzahl miteinander verbundener neurophysiologischer und sozialer Veränderungen geprägt ist.
Similar content being viewed by others

1 Introduction
Ethnic–racial discrimination, the differential treatment of individuals based on ethnic or racial group membership (Carter and Forsyth 2010), is a chronic, potent stressor with adverse effects on mental health outcomes such as anxiety (Berger and Sarnyai 2015; Priest et al. 2013). However, the neurobiological mechanisms underlying these observed associations are inconclusive, particularly during the transition from middle childhood to early adolescence when emotion regulatory networks are developing and social networks are expanding (Scherf et al. 2013). The current study is aimed at addressing this gap by testing whether volumetric alterations of the amygdala, a highly stress-sensitive neural region, account for associations between ethnic–racial discrimination exposure and anxiety symptoms. This study was conducted in preadolescent Latina girls, a group exhibiting heightened levels of untreated anxiety (Ginsburg and Silverman 1996) that is also disproportionately subjected to ethnic–racial discrimination (Vargas et al. 2021). If replicated, identifying how this form of sociocultural stress influences threat-relevant brain networks and escalates the risk for anxiety represents a promising potential step toward developing culturally informed treatment programs to reduce the burden of ethnic- and racial-based mental health disparities in minoritized youth.
1.1 Discrimination and Anxiety in Latinx Youth
Antagonistic political views and growing animosity toward immigrants and people of color have recently brought ethnic–racial discrimination into the limelight of the United States’ political, economic, and social landscape. Ethnic–racial discrimination is more prevalent among people from disadvantaged backgrounds (i.e., individuals with limited access to social and financial resources), including immigrant populations (Carter and Forsyth 2010), than those from privileged backgrounds. For instance, approximately half of Latinx people have experienced ethnic–racial discrimination, with immigration status as a primary reason for unfair treatment (Lopez et al. 2020). Latinx youth, in particular, report experiencing both overt and subtle forms of ethnic–racial discrimination from multiple sources (e.g., peers, teachers, strangers) and across multiple contexts (e.g., at school, in stores, on public transportation) (Pasco et al. 2022).
Latinx people are the largest and second fastest-growing ethnically minoritized group in the USA (United States Census Bureau 2020). Despite this trend, there is substantially less research on the mental health costs of ethnic–racial discrimination in Latinx populations than in African American and Asian populations (Araújo and Borrell 2006). Even though discriminatory treatment is an experience shared across ethnic and racial groups, different groups are embedded within unique sociohistorical contexts, and their experiences of mistreatment may thus possess unique sociocultural underpinnings. Examining these processes in Latinx individuals could illuminate the generalizability of currently understood sociocultural risk and protective processes. Doing so is consequential because exposure to discrimination from birth through adolescence predicts various physical and mental health outcomes, including anxiety (Priest et al. 2013). Latina girls, vulnerable to multiple or intersectional forms of discrimination based on race, ethnicity, and gender, may be at heightened risk. For instance, a study of internalizing symptomatology and suicidality in Latinx youth observed a pronounced effect of discrimination on suicide risk for Latina girls relative to Latino boys (Vargas et al. 2021).
An estimated one-third of adolescent girls are affected by internalizing symptoms, including anxiety, and rates among Latina adolescents, in particular, have significantly increased in recent years (Anderson and Mayes 2010; Ginsburg and Silverman 1996; Kessler et al. 1994; Varela et al. 2004). In both community-based and clinically referred samples, Latinx youth demonstrate higher rates of anxiety than their European American peers (Glover et al. 1999; Pina and Silverman 2004; Roberts et al. 2006). Further, Latina girls report more anxiety symptoms than European American, African American, and Latino youth (McLaughlin et al. 2007). Because sex differences in the incidence of anxiety begin in childhood and increase in magnitude during adolescence (Lewinsohn et al. 1998; Roza et al. 2003), characterizing mechanisms by which sociocultural stressors, like ethnic–racial discrimination, may escalate anxiety risk at the transition to adolescence is crucial. This work has significant implications for culturally informed intervention and prevention efforts to reduce the disproportionately high rates of anxiety observed in Latina youth.
1.2 Minority Stress Processes
One potential neurobiological pathway between ethnic–racial discrimination experiences and anxiety is that ongoing exposure to racially charged stressors presents imminent threats that may perturb stress-sensitive neural networks (Bale and Jovanovic 2021). Exposure to stress triggers an adaptive response that helps the body to prepare for danger, injury, or infection (Boyce and Ellis 2005). However, when this stress becomes chronic, our capacity to efficiently process it declines, and takes its toll on our health. Importantly, these processes are shaped by physical risk factors, individual behaviors, and social conditions. Social determinants of health—defined as the circumstances in which people are born, grow up, live, work, and age—are as influential on health as access to health care (Lucyk and McLaren 2017). Theories of social stress suggest that adverse conditions in the social environment can overwhelm our stress response systems and induce physical or mental illness (Dohrenwend 2000). Minority stress theory, in particular, posits that social stress can significantly and adversely impact the lives of people belonging to stigmatized social groups, including categories related to ethnicity or race (Meyer 1995; Meyer and Dean 1998). One such chronic, potent social stressor experienced by minoritized individuals is ethnic–racial discrimination. Repeated exposure to cumulative experiences associated with discrimination and victimization overtaxes individuals’ stress response systems, contributing to health deterioration (Geronimus et al. 2006) and escalating their vulnerability to stress-related health problems over the life course. Empirically, experiencing ethnic–racial discrimination has been observed to predict greater cardiovascular reactivity, including higher systolic and diastolic blood pressure throughout the day (Steffen et al. 2003). However, the link between experienced discrimination and anxiety-relevant neurobiological stress-response systems is relatively unexplored, particularly among youth.
1.2.1 Neurobiological Pathways
Ethnic–racial discrimination predicts wide-ranging physical and mental health outcomes (Gaylord-Harden and Cunningham 2009; Pachter et al. 2018; Steffen et al. 2003; Stein et al. 2019), including elevating stress and anxiety among children and adolescents (Priest et al. 2013). The mechanisms underlying these observed associations are complex and not yet fully understood. However, neuroscience, particularly when situated in a sociological framework, provides a valuable tool for measuring and characterizing how experiences of ethnic–racial discrimination contribute to anxiety symptoms (Firat 2019, 2021). Several brain regions are responsible for processing different aspects of fear, threat, and pain. Specifically, the amygdala is essential to monitoring the social environment for basic threats, including threats of discriminatory treatment (Krill and Platek 2009), and coordinating with other brain regions to mediate stress response systems (Calder et al. 2001; Fanselow and LeDoux 1999). When chronic stressors like ethnic–racial discrimination perturb communication within and among these systems, this can engender anxious hypervigilance or an excessive anticipatory response to potential social threats (Goosby et al. 2018; van Marle et al. 2009), a core feature of pathological anxiety. Among the most consistent findings in individuals with an anxiety disorder is exaggerated amygdala activation (see Etkin and Wager 2007, for a review). Individuals with subthreshold anxiety exhibit elevated amygdala responses to social anxiety-inducing cues (Beaton et al. 2008); Díaz et al. 2024), suggesting that anxiety might fall on a continuum (Jayakar et al. 2020).
Because the amygdala aids centrally in threat vigilance, it is conceivable that it would be similarly active in response to discriminatory treatment. Indeed, emerging functional and structural neuroimaging evidence in adults documents the detrimental and compounding effects of ethnic–racial discrimination on the neural architecture of the amygdala (Hobson et al. 2022). For example, the amygdala is highly responsive to social exclusion (Eisenberger 2013) and these processes relate to increased sympathetic nervous system activity (Critchley et al. 2003; McEwen and Gianaros 2010), a known biomarker of heightened anxiety (Wenner 2018). Individuals who report higher levels of ethnic–racial discrimination also exhibit heightened spontaneous amygdala activity (Krill and Platek 2009) and greater functional connectivity with regions involved in threat processing and emotion regulation during resting state functional magnetic resonance imaging (Clark et al. 2018; Webb et al. 2022). A related study finds that greater amygdala functional connectivity to threat-relevant brain regions among Hispanic and Black participants relative to white participants is, in part, driven by race-related differences in structural inequities (Harnett et al. 2023).
Fewer studies have examined the effect of ethnic–racial discrimination on brain anatomy, with one recent study documenting larger amygdala volumes in adults exposed to higher levels of ethnic–racial discrimination (Rosario et al. 2020). Importantly, no studies of ethnic–racial discrimination, to date, have investigated functional or structural alterations of the amygdala in youth. This is consequential, as anxiety disorders that affect adults typically begin in late childhood (Glenn et al. 2012). Further, the transition from childhood to adolescence is marked by a host of connected neurophysiological (Glenn et al. 2022) and social changes, including a heightened sensitivity to social exclusion (Masten et al. 2009) and an increasing awareness of social status and positions in social hierarchies (Goosby et al. 2013). Therefore, examining these processes in preadolescence could be informative for developing culturally informed intervention and prevention efforts to reduce the burden of ethnicity- and race-based health disparities in minoritized youth (Michalska and Davis 2019).
1.3 Study Overview
The current study utilized structural brain imaging to evaluate whether altered amygdala volume is one mechanism underlying vulnerability to anxiety in preadolescent Latina girls experiencing ethnic–racial discrimination. We expected that youth with greater ethnic–racial discrimination exposure would report higher anxiety levels. We also tested a mediation model that evaluated an indirect effect of ethnic–racial discrimination exposure on anxiety symptoms through amygdala volume. We complement and extend prior work in several ways. First, emerging empirical work (see Fani et al. 2021, 2022) examining neural mechanisms underlying the association between ethnic–racial discrimination and mental health is still in its infancy. Here, we add to a growing body of literature probing these mechanisms. Second, to our knowledge, this is the first neurobiological study of ethnic–racial discrimination and anxiety in preadolescent youth, enabling examination of these processes during an earlier developmental period marked by significant neurophysiological and social transitions. Third, we study a sample consisting exclusively of Latina girls, a group exhibiting heightened levels of untreated anxiety (Ginsburg and Silverman 1996; McLaughlin et al. 2007; Varela et al. 2004) that is disproportionately subjected to experiences of discrimination (Vargas et al. 2021) and has been underrepresented in research focused on the mental health costs of ethnic–racial discrimination (Araújo and Borrell 2006; La Scala et al. 2023).
2 Methods
2.1 Participants
Participants included 30 Latina girls (MAge = 9.76, SD = 1.11, range = 8–12 years, 66.67% Mexican, 10.00% Cuban, and 23.33% of mixed or unspecified Latina heritage) residing in the Inland Empire Region of Southern California. Participants were recruited via fliers in outpatient mental health clinics and local hospitals, and the University of California, Riverside Psychology Department shared database of child participants. Participant eligibility was determined by phone screening with a parent. Children were eligible for participation if they were fluent in English, aged 8–13 years, self-identified as Latina, were pre-menstrual, had no contraindications for neuroimaging, and did not meet any exclusionary criteria. We note that although menstruation was initially included as an exclusion criterion, it was later dropped to increase sample size and two post-menstrual participants were recruited. Exclusion criteria for children were a current psychiatric diagnosis of Tourette’s syndrome or obsessive-compulsive disorder, suicidal ideation, active medical problems, or any lifetime history of mania, psychosis, or pervasive developmental disorder. On average, families had household incomes ($ 25,000–$ 39,999) below the median annual household income in the USA ($ 70,784; United States Census Bureau 2022). The income distribution of the current sample appears in Fig. 1.

Pie chart depicting the distribution of annual household incomes
2.2 Procedures
Data for the present analyses were collected at participants’ first of several laboratory assessments as part of an ongoing longitudinal study of socioemotional development (Díaz et al. 2024; Glenn et al. 2022; Mullins et al. 2021). Upon participant arrival, written parent consent and child assent were obtained. During the laboratory session, children completed a structural magnetic resonance imaging (MRI) scan and a battery of self-report questionnaires assessing demographics, discrimination exposure, and anxiety symptoms. At the end of the laboratory session, participants were compensated with a gift card and a small prize. The university Institutional Review Board approved all study procedures.
2.3 Measures
2.3.1 Brain Imaging, Data Processing, and Analysis
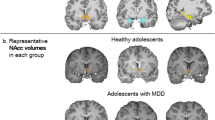
Magnetic resonance imaging scans were acquired on a 3-Tesla Siemens Magnetom Prisma scanner (Siemens, Malvern, PA, USA) with a 32-channel receive-only head coil at the University of California, Riverside Center for Advanced Neuroimaging. Participants completed a T1-weighted magnetization-prepared rapid conditioning gradient-echo scan with the following parameters: 208 sagittally acquired 0.80-mm slices, 320 × 300 matrix, 0.8 mm3 isotropic voxels, flip angle = 8°, field of view = 256 × 240 mm, repetition time = 2400 ms, echo time = 2.72 ms, inversion time = 1060 ms. Using Freesurfer Version 6.0.0 (https://surfer.nmr.mgh.harvard.edu), T1 images were processed, cortical surface reconstruction was performed, and the left and right amygdala volume measurements were extracted using standard processing pipelines (Fig. 2).

Using Freesurfer Version 6.0.0 (https://surfer.nmr.mgh.harvard.edu/), volume measurements for the left and right amygdala were extracted. For visualization in FMRIB Software Library (https://fsl.fmrib.ox.ac.uk/fsl/fslwiki/), the sample subject Freesurfer amygdala labels were converted to volumetric masks and overlaid on a coronal view of the Freesurfer-provided brain mask as the underlay
2.3.2 Experiences of Discrimination
To assess experiences of ethnic–racial discrimination, participants completed the Perceptions of Racism in Children and Youth (PRaCY; Pachter et al. 2010). Prior to questionnaire administration, children were told, “When people are racially discriminated against, they are treated badly, not given respect, or are considered inferior because of the color of their skin, because they speak a different language or have an accent, or because they come from a different country or culture. For each of the following situations, think whether you have ever in your life felt discriminated against because of your color, language or accent, or because of your culture or country of origin.” Children were then provided a list of 23 discriminatory experiences (e.g., “someone called you an insulting name,” “teachers assume you’re not smart or intelligent,” etc.) and were asked to indicate which of them they had experienced. For each endorsed item, children used a five-point Likert scale to indicate how often this had happened to them (1 = Once to 5 = Weekly) and how much this experience upset them (0 = Not at all to 4 = Extremely). Responses to these scales were summed to index the prevalence and severity of discriminatory experiences respectively—children who did not endorse any experiences of ethnic–racial discrimination received prevalence and severity scores of 0. The PRaCY has been utilized as a valid measure of perceived discriminatory experiences in studies of both children (Marcelo and Yates 2019) and adolescents (Park et al. 2017).
2.3.3 Anxiety Symptoms
Participants completed the 41-item Screen for Child Anxiety-Related Emotional Disorders (SCARED; Birmaher et al. 1999) to provide continuous measures of anxiety symptoms across five domains: panic/somatic, generalized anxiety, separation anxiety, social phobia, and school phobia. For each item, children indicated on a three-point Likert scale (0 = Not true or hardly ever true to 2 = Very true or often true) the extent to which each was true for them. Responses were summed across all items, as well as within each subdomain. The SCARED demonstrated strong internal consistency in the current sample with a Cronbach’s α of 0.93. Of note, 80.0% of the sample met clinical thresholds for anxiety disorder (≥ 25).
2.4 Data Analysis
Linear regression analysis implemented in SPSS Version 28.0.0 (IBM, Armonk, NY: https://www.ibm.com/spss), together with the PROCESS macro (Hayes 2013), was used to evaluate the associations of ethnic–racial discrimination and anxiety symptoms and mediating effects of amygdala volume on any observed associations. To do this, we first evaluated whether ethnic–racial discrimination exposure was associated with amygdala volume (a path). Next, we examined whether amygdala volume was associated with anxiety symptoms, controlling for ethnic–racial discrimination exposure (b path). Finally, we assessed whether amygdala volume indirectly mediated the association between ethnic–racial discrimination and anxiety symptoms. Separate regression models were conducted for each predictor (i.e., ethnic–racial discrimination prevalence, ethnic–racial discrimination severity) and mediator (i.e., left amygdala volume, right amygdala volume) of interest. As such, four regression models were conducted, each controlling for total intracranial volume and annual household income, which has been linked with alterations in brain structure (Merz et al. 2018).
All variables were continuous and mean centered prior to analysis, and the estimated effects are reported as standardized regression coefficients. To address any non-normality in the distribution of the outcomes, the models were estimated using bootstrapped samples (bootstrap N = 5000) to produce 95% bias-corrected confidence intervals (BC 95% CI) around the parameter estimates. Effects were determined to be significant at p < 0.05 if the upper and lower limits of the CIs did not contain zero. To account for multiple tests, Bonferroni corrections were applied.
3 Results
3.1 Descriptive Statistics
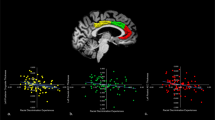
Descriptive statistics appear in Table 1, and bivariate correlations appear in Table 2. Of note, a significant positive association between ethnic–racial discrimination severity and anxiety symptoms emerged (r = 0.38, p = 0.040). Scatter plots depicting the association of amygdala volume with ethnic–racial discrimination prevalence, ethnic–racial discrimination severity, and anxiety symptoms appear in Fig. 3.

Scatter plots depicting the association of amygdala volume with a ethnic–racial discrimination prevalence, b ethnic–racial discrimination severity, and c anxiety symptoms. (ERD Ethnic–Racial Discrimination)
3.2 Ethnic–Racial Discrimination and Anxiety Symptoms
Controlling for total intracranial volume and annual household income, regression analysis revealed that the effect of children’s concurrent ethnic–racial discrimination experiences on anxiety symptoms was positive but not statistically significant for both ethnic–racial discrimination prevalence (β = 0.20, SE = 0.25, BC 95% CI [−0.259, 0.766], p = 0.318) and ethnic–racial discrimination severity (β = 0.31, SE = 0.24, BC 95% CI [−0.101, 0.885], p = 0.114). Because it is appropriate to examine a mediation analysis even when the total effect does not reach conventional thresholds of statistical significance, as such a requirement reduces the statistical power to detect mediation (Hayes 2009; MacKinnon et al. 2007; Muele 2019; Zhao et al. 2010), we conducted analyses to test whether ethnic–racial discrimination indirectly contributed to greater anxiety symptoms through alterations in amygdala volume. As a reminder, we evaluated: first, whether ethnic–racial discrimination exposure was associated with amygdala volume (a path); second, whether amygdala volume was associated with anxiety symptoms, controlling for ethnic–racial discrimination exposure (b path); and third, whether amygdala volume indirectly mediated the association between ethnic–racial discrimination and anxiety symptoms.
3.3 Ethnic–Racial Discrimination and Brain Structure (a Path)
Participants who reported more severe ethnic–racial discrimination exposure had a significantly smaller left amygdala volume than participants who reported less severe ethnic–racial discrimination exposure (β = −0.37, SE = 2.13, BC 95% CI [−9.680, −0.902], p = 0.020), controlling for total intracranial volume and annual household income. This association was not significant for the right amygdala or the prevalence of ethnic–racial discrimination exposure, all ps > 0.066.
3.4 Brain Structure and Anxiety (b Path)
Participants with a larger left amygdala volume reported more anxiety symptoms than participants with a smaller left amygdala volume (β = 0.76, SE = 0.02, BC 95% CI [0.030, 0.106], p = 0.001), controlling for total intracranial volume, annual household income, and the severity of ethnic–racial discrimination exposure. This association was not significant for the right amygdala, p = 0.774. Participants with a larger left amygdala volume reported more anxiety symptoms than participants with a smaller left amygdala volume (β = 0.57, SE = 0.02, BC 95% CI [0.011, 0.092], p = 0.015), controlling for total intracranial volume, annual household income, and the prevalence of ethnic–racial discrimination exposure. This association was not significant for the right amygdala, p = 0.990.
3.5 Mediation Analyses
Mediation analyses revealed indirect effects of ethnic–racial discrimination on anxiety symptoms via amygdala volume (Table 3). The first analysis tested whether left amygdala volume mediated the association between ethnic–racial discrimination prevalence and anxiety symptoms. Controlling for total intracranial volume and annual household income, no significant mediating effect emerged, BC 95% CI [−0.483, 0.065], p = 0.093. The second linear regression analysis tested whether left amygdala volume mediated the association between ethnic–racial discrimination severity and anxiety symptoms, controlling for total intracranial volume and annual household income. The BC 95% CI of the standardized index of mediation for the model with left amygdala volume (β = −0.28, SE = 0.17, BC 95% CI [−0.690, −0.017], p = 0.014) did not include zero, suggesting a significant indirect effect for this model (Fig. 4). The third linear regression analysis tested whether right amygdala volume mediated the association between ethnic–racial discrimination prevalence and anxiety symptoms. Controlling for total intracranial volume and annual household income, no significant mediating effect emerged, BC 95% CI [−0.241, 0.185], p = 0.982. The fourth linear regression analysis tested whether right amygdala volume mediated the association between ethnic–racial discrimination severity and anxiety symptoms. Controlling for total intracranial volume and annual household income, no significant mediating effect emerged, BC 95% CI [−0.299, 0.155], p = 0.712. We note that because of the direction of our paths (see Fig. 4), our results do not explicitly support a mediation effect but rather two indirect paths linking (a) ethnic–racial discrimination severity with left amygdala volume and (b) left amygdala volume with child anxiety symptoms.

Controlling for age and total intracranial volume, two indirect paths were observed: a negative association between ethnic–racial discrimination severity and left amygdala volume and a positive association between left amygdala volume and anxiety symptoms. Although the mediation model was significant, (β = −0.28, SE = 0.17, BC 95% CI [−0.690, −0.017], p = 0.014), we interpret these data as two indirect paths rather than partial or full mediation as c’ was not smaller than c. (Effects are reported as standardized regression coefficients. ERD Ethnic–Racial Discrimination. *p < 0.05, **p < 0.01, ***p < 0.001)
3.5.1 Bonferroni Corrections
The current analyses separately tested the indirect effects of left and right amygdala volume on the association between ethnic–racial discrimination exposure and anxiety symptoms. As such, Bonferroni corrections were applied to correct for multiple tests of laterality. With an adjusted p value of 0.05/2 = 0.025, the observed indirect effect of left amygdala volume on the association between ethnic–racial discrimination severity and anxiety symptoms remained significant, p = 0.014.
4 Discussion
We provide preliminary evidence that racialized threats in childhood may contribute to smaller left amygdala volume among Latina girls and that alterations in amygdala volume may indirectly contribute to increased vulnerability to anxiety symptoms. Our data elucidate a potential mechanism by which experiences of ethnic–racial discrimination can adversely impact mental health, particularly in the transition from middle childhood to early adolescence, a period marked by a host of interlinked neurophysiological and social changes. Prior work has consistently shown that youth who have experienced adversity, including abuse, neglect, and violence exposure, are at an elevated risk for mental health problems (King 2021). However, scholars have only recently begun investigating the neurobiological mechanisms underlying these patterns, including their extension to stressors unique to underrepresented and marginalized groups. Such efforts are consequential because chronic sociocultural stress may compound the effects of more widely experienced social stressors, suggesting that the health of individuals of color might be at a heightened risk (Meyer 1995; Meyer and Dean 1998).
In partial support of our first hypothesis, ethnic–racial discrimination severity correlated positively with anxiety symptoms. This result parallels previous findings that discrimination is related to detriments in mental health, including elevated anxiety (Priest et al. 2013). Even though we did not specify distinct effects of ethnic–racial discrimination severity and prevalence on anxiety symptoms, it is worth noting that only the severity of discriminatory experiences, not their prevalence, was associated with higher anxiety levels in our sample. This observed association is consistent with work on more conventionally studied forms of adversity (e.g., abuse, neglect), which suggests that the subjective experience of adversity might be a more potent predictor of child psychopathology than the objective occurrence (Baldwin and Degli Esposti 2021; Danese and Widom 2020). Under this notion, the degree to which children are upset by ethnic–racial discrimination experiences (i.e., severity) may be a unique indicator of anxiety risk relative to the frequency of ethnic–racial discrimination experiences accumulated (i.e., prevalence). As such, continued research on ethnic–racial discrimination must carefully examine these distinctions to characterize the potential differential effects of distinct facets of ethnic–racial discrimination on mental health.
In partial support of our second hypothesis, we observed evidence of racialized stress sensitization operating indirectly on anxiety symptoms via reduced left amygdala volume. Ethnic–racial discrimination severity was associated with reduced volume in the left amygdala. This finding is consistent with prior studies examining the association between trauma exposure and amygdala volume in children and adolescents, finding smaller amygdala volumes among children exposed to maltreatment (McLaughlin et al. 2016, 2019; Saxbe et al. 2018; Weissman et al. 2020). Importantly, our work suggests that sociocultural adversity might similarly implicate the structure of this stress-sensitive neural region. Left amygdala volume, in turn, was associated with elevated anxiety symptoms. This result parallels previous structural and functional work identifying larger amygdala volumes in anxious relative to non-anxious youth (De Bellis et al. 2000) and a compounding effect of adverse life experiences on linkages between amygdala reactivity and anxiety (Silvers et al. 2017). We note that subcortical structure does not consistently map onto function and subsequent psychopathology. Whereas increased amygdala volume may index heightened sensitivity to threat and create a vulnerability to anxiety, it is simultaneously plausible that increased amygdala volume might be the result of increased anxiety during development. Thus, we contend that in addition to identifying structural alterations in threat-relevant brain regions, we must also identify functional perturbations within and among these neural networks. Doing so would more completely clarify the role of amygdala volume and reactivity in anxiety risk.
Whereas ethnic–racial discrimination severity did not significantly predict anxiety symptoms, a significant indirect effect of ethnic–racial discrimination on anxiety symptoms via left amygdala volume emerged, identifying a potential neurobiological pathway by which ethnic–racial discrimination may contribute to elevated anxiety. Finally, these associations were not observed for the prevalence of ethnic–racial discrimination or right amygdala volume. The absence of an effect of the prevalence of ethnic–racial discrimination on left amygdala volume was surprising, given its high correlation with the severity of ethnic–racial discrimination. We note that the associative patterns of these discrimination indices with amygdala volume are qualitatively similar (see Fig. 3) and attribute the lack of similar quantitative effects to our modest sample size. However, future work in larger samples would be informative. Relatedly, we expect the observed lateral differences in amygdala volume to be a function of sample size too and argue that continued research is needed to determine the role the amygdala plays in mediating sociocultural stress and mental health changes depending on laterality.
The current findings should be considered in the context of several limitations. First, our sample size was modest, potentially reducing statistical power. Although analyses utilized bootstrapping techniques to assist with this, future work in larger samples would be informative. Of note, our mediation analysis included negative (i.e., effect of ethnic–racial discrimination severity on left amygdala volume) and positive (i.e., effect of left amygdala volume on anxiety symptoms) effects, suggesting that an untested variable might be moderating one or both paths linking racialized stress, amygdala volume, and anxiety symptoms. Larger samples may provide opportunities to parse out interactive effects of more proximal environmental factors through tests of moderated paths. For instance, structural inequities such as income detrimentally affect brain structure and function (Harnett et al. 2023; Merz et al. 2018), although household income was not significantly related to any variables of interest in the current study. Future work should continue probing the effects of income and other forms of structural inequity on the links among discrimination, neurobiology, and mental health. Second, this was a cross-sectional design. Longitudinal studies testing whether the effects of ethnic–racial discrimination on anxiety via alterations in amygdala volume prospectively sensitize Latina girls’ threat systems and exacerbate anxiety symptoms are necessary to more completely understand the toll of discrimination on stress-sensitive neurocircuitry and mental health over time. Third, this was a structural MRI investigation, limiting our ability to make inferences about the role of amygdala reactivity in the link between ethnic–racial discrimination and anxiety. Functional neuroimaging studies would elucidate whether ethnic–racial discrimination disrupts activity within and surrounding this stress-sensitive region, consequently elevating anxiety. Fourth, considering that the sample was primarily community-based (La Scala et al. 2023), participants exhibited unexpectedly high levels of anxiety, which may limit generalizability. Although these trends are consistent with a growing body of research showing heightened levels of untreated anxiety in Latina youth (Anderson and Mayes 2010; McLaughlin et al. 2007; Pina and Silverman 2004; Polo et al. 2024) and may further support our hypothesis that discriminatory experiences elevate anxiety, future work in samples with more varied levels of anxiety is warranted.
Several strengths mitigate these limitations and offer data about the amygdala’s role in linking ethnic–racial discrimination exposure and anxiety symptoms in Latina youth. First, emerging empirical work (see Fani et al. 2021, 2022) examining neurobiological mechanisms by which ethnic–racial discrimination shapes mental health is still in its infancy. Here, we add to a growing body of literature probing these pathways and to broader investigations of the influence of sociocultural processes on the psychobiology of emotional development (Michalska and Davis 2019). Second, to our knowledge, this is the first neurobiological study of ethnic–racial discrimination and anxiety in preadolescents, enabling examination of these processes during an earlier developmental period marked by significant neurophysiological and social transitions. Third, we study a sample consisting exclusively of Latina girls, a group exhibiting heightened levels of untreated anxiety (Ginsburg and Silverman 1996; McLaughlin et al. 2007; Varela et al. 2004) that is disproportionately subjected to experiences of discrimination (Vargas et al. 2021), and has been underrepresented in research focused on the mental health costs of ethnic–racial discrimination (Araújo and Borrell 2006).
In sum, the current study elucidates a potential neurobiological pathway by which negative social experiences detrimentally impact mental health. Specifically, we add to existing literature identifying ethnic–racial discrimination as a threat-relevant social stressor related to altered threat neurocircuitry and elevated anxiety. This work highlights the utility of neuroscience in measuring and understanding how adverse social conditions shape health trajectories and likely perpetuate ethnicity- and race-based health disparities. Together with other efforts, our investigation lays the initial groundwork for developing culturally-informed intervention and prevention efforts targeting long-term mental health outcomes in minoritized youth.
References
Anderson, Emily R., and Linda C. Mayes. 2010. Race/ethnicity and internalizing disorders in youth: A review. Clinical Psychology Review 30:338–348.
Araújo, Beverly Y., and Luisa N. Borrell. 2006. Understanding the link between discrimination, mental health outcomes, and life chances among Latinos. Hispanic Journal of Behavioral Sciences 28:245–266.
Baldwin, Jessie R., and Michelle Degli Esposti. 2021. Triangulating evidence on the role of perceived versus objective experiences of childhood adversity in psychopathology. JCPP Advances 1:e12010.
Bale, Tracy L., and Tanja Jovanovic. 2021. The critical importance in identifying the biological mechanisms underlying the effects of racism on mental health. Neuropsychopharmacology 46:233.
Beaton, Elliott A., Louis A. Schmidt, Jay Schulkin, Martin M. Antony, Richard P. Swinson and Geoffrey B. Hall. 2008. Different neural responses to stranger and personally familiar faces in shy and bold adults. Behavioral Neuroscience 122:704.
Berger, Maximus, and Zoltán Sarnyai. 2015. “More than skin deep”: stress neurobiology and mental health consequences of racial discrimination. Stress 18:1–10.
Birmaher, Boris, David A. Brent, Laurel Chicapetta, Jeffrery Bridge, Suneeta Monga and Marianne Baugher. 1999. Psychometric properties of the Screen for Child Anxiety Related Emotional Disorders (SCARED): a replication study. Journal of the American Academy of Child & Adolescent Psychiatry 38:1230–1236.
Boyce, W. Thomas, and Bruce J. Ellis. 2005. Biological sensitivity to context: I. An evolutionary—developmental theory of the origins and functions of stress reactivity. Development and Psychopathology 17:271–301.
Calder, Andrew J., Andrew D. Lawrence and Andrew W. Young. 2001. Neuropsychology of fear and loathing. Nature Reviews Neuroscience 2:352–363.
Carter, Robert T., and Jessica Forsyth. 2010. Reactions to racial discrimination: Emotional stress and help-seeking behaviors. Psychological Trauma: Theory, Research, Practice, and Policy 2:183.
Clark, Uraina S., Evan R. Miller and Rachal R. Hegde. 2018. Experiences of discrimination are associated with greater resting amygdala activity and functional connectivity. Biological Psychiatry 3:367–378.
Critchley, Hugo D., Christopher J. Mathias, Oliver Josephs, John O’Doherty, Sergio Zanini, Bonnie-Kate Dewar, Lisa Cipolotti, Tim Shallice and Raymond J. Dolan. 2003. Human cingulate cortex and autonomic control: converging neuroimaging and clinical evidence. Brain 126:2139–2152.
Danese, Andrea, and Cathy Spatz Widom. 2020. Objective and subjective experiences of child maltreatment and their relationships with psychopathology. Nature Human Behaviour 4:811–818.
De Bellis, Michael D., B.J. Casey, Ronald E. Dahl, Boris Birmaher, Douglas E. Williamson, Kathleen M. Thomas, David A. Axelson, Karin Frustaci, Amy M. Boring, Julie Hall and Neal D. Ryan. 2000. A pilot study of amygdala volumes in pediatric generalized anxiety disorder. Biological Psychiatry 48:51–57.
Díaz, Dana E., Wan-Ling Tseng and Kalina J. Michalska. 2024. Pre-scan state anxiety is associated with greater right amygdala-hippocampal response to fearful versus happy faces among trait-anxious Latina girls. BMC psychiatry 24(1):1.
Dohrenwend, Bruce P. 2000. The role of adversity and stress in psychopathology: Some evidence and its implications for theory and research. Journal of Health and Social Behavior 41:1–19.
Eisenberger, Naomi I. 2013. Social ties and health: a social neuroscience perspective. Current Opinion in Neurobiology 23:407–413.
Etkin, Amit, and Tor D. Wager. 2007. Functional neuroimaging of anxiety: a meta-analysis of emotional processing in PTSD, social anxiety disorder, and specific phobia. American Journal of Psychiatry 164:1476–1488.
Fani, Negar, Sierra E. Carter, Nathaniel G. Harnett, Kerry J. Ressler and Bekh Bradley. 2021. Association of racial discrimination with neural response to threat in Black women in the US exposed to trauma. JAMA psychiatry 78:1005–1012.
Fani, Negar, Nathaniel G. Harnett, Bekh Bradley, Yara Mekawi, Abigail Powers, Jennifer S. Stevens, Kerry J. Ressler and Sierra Carter. 2022. Racial discrimination and white matter microstructure in trauma-exposed Black women. Biological Psychiatry 91:254–261.
Fanselow, Michael S., and Joseph E. LeDoux. 1999. Why we think plasticity underlying Pavlovian fear conditioning occurs in the basolateral amygdala. Neuron 23:229–232.
Firat, Rengin B. 2019. Opening the “Black Box”: Functions of the frontal lobes and their implications for sociology. Frontiers in Sociology 4:3.
Firat, Rengin B. 2021. A neurosociological theory of culturally and structurally situated cognition and ethno-racial stress. Frontiers in Sociology 6:695042.
Gaylord-Harden, Noni K., and Jamila A. Cunningham. 2009. The impact of racial discrimination and coping strategies on internalizing symptoms in African American youth. Journal of Youth and Adolescence 38:532–543.
Geronimus, Arline T., Margaret Hicken, Danya Keene and John Bound. 2006. “Weathering” and age patterns of allostatic load scores among blacks and whites in the United States. American Journal of Public Health 96:826–833.
Ginsburg, Golda S., and Wendy K. Silverman. 1996. Phobic and anxiety disorders in Hispanic and Caucasian youth. Journal of Anxiety Disorders 10:517–528.
Glenn, Catherine R., Daniel N. Klein, Shmuel Lissek, Jennifer C. Britton, Daniel S. Pine and Greg Hajcak. 2012. The development of fear learning and generalization in 8–13 year-olds. Developmental Psychobiology 54:675–684.
Glenn, Dana E., Jenna L. Merenstein, Ilana J. Bennett and Kalina J. Michalska. 2022. Anxiety symptoms and puberty interactively predict lower cingulum microstructure in preadolescent Latina girls. Scientific Reports 12:20755.
Glover, Saundra H., Andres J. Pumariega, Charles E. Holzer III, Brian K. Wise and Moises Rodriguez. 1999. Anxiety symptomatology in Mexican-American adolescents. Journal of Child and Family Studies 8:47–57.
Goosby, Bridget J., Anna Bellatorre, Katrina M. Walsemann and Jacob E. Cheadle. 2013. Adolescent loneliness and health in early adulthood. Sociological Inquiry 83:505–536.
Goosby, Bridget J., Jacob E. Cheadle and Colter Mitchell. 2018. Stress-related biosocial mechanisms of discrimination and African American health inequities. Annual Review of Sociology 44:319–340.
Harnett, Nathaniel G., Negar Fani, Sierra Carter, Leon D. Sanchez, Grace E. Rowland, William M. Davie, Camilo Guzman, Lauren A. M. Lebois, Timothy D. Ely, Sanne J. H. van Rooij, Antonia V. Seligowski, Sterling Winters, Lana R. Grasser, Paul I. Musey Jr., Mark J. Seamon, Stacey L. House, Francesca L. Beaudoin, Xinming An, Donglin Zeng, Thomas C. Neylan, Gari D. Clifford, Sarah D. Linnstaedt, Laura T. Germine, Kenneth A. Bollen, Scott L. Rauch, John P. Haran, Alan B. Storrow, Christopher Lewandowski, Phyllis L. Hendry, Sophia Sheikh, Christopher W. Jones, Brittany E. Punches, Robert A. Swor, Lauren A. Hudak, Jose L. Pascual, Erica Harris, Anna M. Chang, Claire Pearson, David A. Peak, Roland C. Merchant, Robert M. Domeier, Niels K. Rathlev, Steven E. Bruce, Mark W. Miller, Robert H. Pietrzak, Jutta Joormann, Deanna M. Barch, Diego A. Pizzagalli, Steven E. Harte, James M. Elliott, Ronald C. Kessler, Karestan C. Koenen, Samuel A. McLean, Tanja Jovanovic, Jennifer S. Stevens and Kerry J. Ressler. 2023. Structural inequities contribute to racial/ethnic differences in neurophysiological tone, but not threat reactivity, after trauma exposure. Molecular Psychiatry 28:2975–2984.
Hayes, Andrew F. 2009. Beyond Baron and Kenny: Statistical mediation analysis in the new millennium. Communication monographs 76:408–420.
Hayes, Andrew F. 2013. Introduction to mediation, moderation, and conditional process analysis. A regression-based approach. New York, NY: Guilford Press.
Hobson, Joanna M., Myles de Moody, Robert E. Sorge and Burel R. Goodin. 2022. The neurobiology of social stress resulting from Racism: Implications for pain disparities among racialized minorities. Neurobiology of Pain 12:100101.
Jayakar, Reema, Erin B. Tone, Bruce Crosson, Jessica A. Turner, Page L. Anderson, K. Luan Phan and Heide Klumpp. 2020. Amygdala volume and social anxiety symptom severity: Does segmentation technique matter? Psychiatry Research 295:111006.
Kessler, Ronald C., Katherine A. McGonagle, Shanyang Zhao, Christopher B. Nelson, Michael Hughes, Suzann Eshleman, Hans-Ulrich Wittchen, Kenneth S. Kendler. 1994. Lifetime and 12-month prevalence of DSM-III‑R psychiatric disorders in the United States: results from the National Comorbidity Survey. Archives of General Psychiatry 51:8–19.
King, Alan R. 2021. Childhood adversity links to self-reported mood, anxiety, and stress-related disorders. Journal of Affective Disorders 292:623–632.
Krill, Austen, and Steven M. Platek. 2009. In-group and out-group membership mediates anterior cingulate activation to social exclusion. Frontiers in Evolutionary Neuroscience 1:438.
La Scala, Shayna, Jordan L. Mullins, Rengin B. Firat, Emotional Learning Research Community Advisory Board and Kalina J. Michalska. 2023. Equity, diversity, and inclusion in developmental neuroscience: Practical lessons from community-based participatory research. Frontiers in Integrative Neuroscience 16:1007249.
Lewinsohn, Peer M., Ian H. Gotlib, Mark Lewinsohn, John R. Seeley and Nicholas B. Allen. 1998. Gender differences in anxiety disorders and anxiety symptoms in adolescents. Journal of Abnormal Psychology 107(1):109-117.
Lopez, Mark H., Ana Gonzalez-Barrera and Jens M. Krogstad. 2020. Latinos’ experiences with discrimination. Retrieved from https://www.pewresearch.org/hispanic/2018/10/25/more-latinos-have-serious-concerns-about-their-place-in-america-under-trump/
Lucyk, Kelsey, and Lindsay McLaren. 2017. Taking stock of the social determinants of health: A scoping review. PloS one 12:e0177306.
MacKinnon, David P., Amanda J. Fairchild and Matthew S. Fritz. 2007. Mediation analysis. Annual Review of Psychology 58:593–614.
Marcelo, Ana K., and Tuppett M. Yates. 2019. Young children’s ethnic–racial identity moderates the impact of early discrimination experiences on child behavior problems. Cultural Diversity and Ethnic Minority Psychology 25:253.
Masten, Carrie L., Naomi I. Eisenberger, Larissa A. Borofsky, Jennifer H. Pfeifer, Kristin McNealy, John C. Mazziotta and Mirella Dapretto. 2009. Neural correlates of social exclusion during adolescence: understanding the distress of peer rejection. Social Cognitive and Affective Neuroscience 4:143–157.
McEwen, Bruce S., and Peter J. Gianaros. 2010. Central role of the brain in stress and adaptation: links to socioeconomic status, health, and disease. Annals of the New York Academy of Sciences 1186:190–222.
McLaughlin, Katie A., Lori M. Hilt and Susan Nolen-Hoeksema. 2007. Racial/ethnic differences in internalizing and externalizing symptoms in adolescents. Journal of Abnormal Child Psychology 35:801–816.
McLaughlin, Katie A., Margaret A. Sheridan, Andrea L. Gold, Andrea Duys, Hilary K. Lambert, Matthew Peverill, Charlotte Heleniak, Tomer Shechner, Zuzanna Wojcieszak and Daniel S. Pine. 2016. Maltreatment exposure, brain structure, and fear conditioning in children and adolescents. Neuropsychopharmacology 41:1956–1964.
McLaughlin, Katie A., David Weissman and Debbie Bitrán. 2019. Childhood adversity and neural development: A systematic review. Annual Review of Developmental Psychology 1:277–312.
Merz, Emily C., Nim Tottenham and Kimberly G. Noble. 2018. Socioeconomic status, amygdala volume, and internalizing symptoms in children and adolescents. Journal of Clinical Child & Adolescent Psychology 47:312–323.
Meyer, Ilan H. 1995. Minority stress and mental health in gay men. Journal of Health and Social Behavior 36:38–56.
Meyer, Ilan H., and Laura Dean. 1998. Internalized homophobia, intimacy, and sexual behavior among gay and bisexual men. In Stigma and sexual orientation: Understanding prejudice against lesbians, gay men, ed. Gregory M. Herek, 160–186. Thousand Oaks, CA: Sage.
Michalska, Kalina J., and Elizabeth L. Davis. 2019. The psychobiology of emotional development: The case for examining sociocultural processes. Developmental Psychobiology 61:416–429.
Muele, Adrian. 2019. Contemporary Understanding of Mediation Testing. Meta-Psychology 3:1–7.
Mullins, Jordan L., Elayne Zhou, Dana E. Glenn, Elizabeth Moroney, Steve S. Lee and Kalina J. Michalska. 2021. Paternal expressed emotion influences psychobiological indicators of threat and safety learning in daughters: A preliminary study. Developmental Psychobiology 63:e22205.
Pachter, Lee M., Laura A. Szalacha, Bruce A. Bernstein and Cynthia García Coll. 2010. Perceptions of Racism in Children and Youth (PRaCY): Properties of a self-report instrument for research on children’s health and development. Ethnicity & Health 15:33–46.
Pachter, Lee M., Cleopatra H. Caldwell, James S. Jackson and Bruce A. Bernstein. 2018. Discrimination and mental health in a representative sample of African-American and Afro-Caribbean youth. Journal of Racial and Ethnic Health Disparities 5(4):831–837.
Park, Irene J. K., Lijuan Wang, David R. Williams and Margarita Alegría. 2017. Does anger regulation mediate the discrimination–mental health link among Mexican-origin adolescents? A longitudinal mediation analysis using multilevel modeling. Developmental Psychology 53:340.
Pasco, Michelle C., Nilda Flores-González and Annabelle Lin Atkin. 2022. A retrospective analysis of racial discrimination experiences for latinx adolescents and young adults. Journal of Research on Adolescence 32:636–649.
Pina, Armando A., and Wendy K. Silverman. 2004. Clinical phenomenology, somatic symptoms, and distress in Hispanic/Latino and European American youths with anxiety disorders. Journal of Clinical Child and Adolescent Psychology 33:227–236.
Polo, Antonio J., Jesus E. Solano-Martinez, Laura Saldana, Amber D. Ramos, Miguel Herrera, Taylor Ullrich and Milena DeMario. 2024. The epidemic of internalizing problems among Latinx adolescents before and during the coronavirus 2019 pandemic. Journal of Clinical Child & Adolescent Psychology 53(1):66–82.
Priest, Naomi, Yin Paradies, Brigid Trenerry, Mandy Truong, Saffran Karlsen and Yvonne Kelly. 2013. A systematic review of studies examining the relationship between reported racism and health and wellbeing for children and young people. Social Science & Medicine 95:115–127.
Roberts, Robert E., Catherine Ramsay Roberts and Yun Xing. 2006. Prevalence of youth-reported DSM-IV psychiatric disorders among African, European, and Mexican American adolescents. Journal of the American Academy of Child & Adolescent Psychiatry 45:1329–1337.
Rosario, Michael A., Amara Ayoub, Razan Alotaibi, Uraina S. Clark and Karin Schon. 2020. Perceived control attenuates the relationship between experiences of discrimination and left amygdala volume in older adults: Neuroimaging/Normal brain aging. Alzheimer’s & Dementia 16:e045394.
Roza, Sabine J., Marijke B. Hofstra, Jan van der Ende and Frank C. Verhulst. 2003. Stable prediction of mood and anxiety disorders based on behavioral and emotional problems in childhood: a 14-year follow-up during childhood, adolescence, and young adulthood. American Journal of Psychiatry 160:2116–2121.
Saxbe, Darby, Hannah Khoddam, Larissa Del Piero, Sarah A. Stoycos, Sarah I. Gimbel, Gayla Margolin and Jonas T. Kaplan. 2018. Community violence exposure in early adolescence: Longitudinal associations with hippocampal and amygdala volume and resting state connectivity. Developmental Science 21:e12686.
Scherf, K. Suzanne, Joshua M. Smyth and Mauricio R. Delgado. 2013. The amygdala: an agent of change in adolescent neural networks. Hormones and Behavior 64:298–313.
Silvers, Jennifer A., Bonnie Goff, Laurel J. Gabard-Durnam, Dylan G. Gee, Dominic S. Fareri, Christina Caldera and Nim Tottenham. 2017. Vigilance, the amygdala, and anxiety in youths with a history of institutional care. Biological Psychiatry: Cognitive Neuroscience and Neuroimaging 2(6):493–501.
Steffen, Patrick R., Maya McNeilly, Norman Anderson and Andrew Sherwood. 2003. Effects of perceived racism and anger inhibition on ambulatory blood pressure in African Americans. Psychosomatic Medicine 65:746–750.
Stein, Gabriela Livas, Laura Castro-Schilo, Alyson M. Cavanaugh, Yesenia Mejia, N. Keita Christophe and Richard Robins. 2019. When discrimination hurts: The longitudinal impact of increases in peer discrimination on anxiety and depressive symptoms in Mexican-origin youth. Journal of Youth and Adolescence 48:864–875.
United States Census Bureau. 2020. ACS Demographic and Housing Estimate. Retrieved from https://data.census.gov/cedsci/table?q=United%20States&tid=ACSDP1Y2019.DP05
United States Census Bureau. 2022. Income in the United States: 2021. Retrieved from https://www.census.gov/library/publications/2022/demo/p60-276.html
Van Marle, Hein J.F., Erno J. Hermans, Shaozheng Qin and Guillén Fernández. 2009. From specificity to sensitivity: how acute stress affects amygdala processing of biologically salient stimuli. Biological Psychiatry 66:649–655.
Varela, R. Enrique, Eric M. Vernberg, Juan Jose Sanchez-Sosa, Angelica Riveros, Montserrat Mitchell and Joanna Mashunkashey. 2004. Anxiety reporting and culturally associated interpretation biases and cognitive schemas: A comparison of Mexican, Mexican American, and European American families. Journal of Clinical Child and Adolescent Psychology 33:237–247.
Vargas, Sylvanna M., Vanessa Calderon, Christopher R. Beam, Yolanda Cespedes-Knadle and Stanley J. Huey Jr. 2021. Worse for girls? Gender differences in discrimination as a predictor of suicidality among Latinx youth. Journal of Adolescence 88:162–171.
Webb, E. Kate, Claire M. Bird, Terri A. deRoon-Cassini, Carissa N. Weis, Ashley A. Huggins, Jacklynn M. Fitzgerald, Tara Miskovich, Kenneth Bennett, Jessica Krukowski, Lucas Torres and Christine L. Larson. 2022. Racial discrimination and resting-state functional connectivity of salience network nodes in trauma-exposed black adults in the United States. JAMA network open 5:e2144759–e2144759.
Weissman, David G., Hilary K. Lambert, Alexandra M. Rodman, Matthew Peverill, Margaret A. Sheridan and Katie A. McLaughlin. 2020. Reduced hippocampal and amygdala volume as a mechanism underlying stress sensitization to depression following childhood trauma. Depression and anxiety 37:916–925.
Wenner, Megan M. 2018. Sympathetic activation in chronic anxiety: not just at the “height” of stress. Editorial Focus on “Relative burst amplitude of muscle sympathetic nerve activity is an indicator of altered sympathetic outflow in chronic anxiety”. Journal of Neurophysiology 120:7–8.
Zhao, Xinshu, John G. Lynch Jr. and Qimei Chen. 2010. Reconsidering Baron and Kenny: Myths and truths about mediation analysis. Journal of Consumer Research 37:197–206.
Funding
Support for this study was provided by a grant from the Hellman Fellows Program and a National Science Foundation CAREER award (NSF 2239067) to Dr. Kalina J. Michalska, and by a National Institute of Health subaward (U54MD013368) from the UCR Center for Health Disparities Research to Jordan Mullins.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
J.L. Mullins, D.E. Díaz, R.B. Firat, and K.J. Michalska declare that they have no competing interests.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Mullins, J.L., Díaz, D.E., Firat, R.B. et al. Ethnic–Racial Discrimination Exposure and Anxiety in Latina Girls: Amygdala Volume as an Indirect Neurobiological Pathway. Köln Z Soziol (2024). https://doi.org/10.1007/s11577-024-00946-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11577-024-00946-2
Keywords
- Developmental psychopathology
- Internalizing symptoms
- Structural magnetic resonance imaging (sMRI)
- Health disparities
- Racism