
Abstract
Communities marginalized because of racism, heterosexism, and other systems of oppression have a history of being aggressively policed, and in those contexts, researchers have observed associations between a range of negative experiences with police and poor physical, mental, and behavioral health outcomes. However, past studies have been limited in that experiences of police contacts were aggregated at the neighborhood level and, if police contacts were self-reported, the sample was not representative. To address these limitations, we employed NYC Department of Health and Mental Hygiene 2017 Social Determinants of Health Survey (n = 2335) data to examine the associations of self-reported police contacts and discrimination by police and the courts with measures of physical (poor physical health), mental (poor mental health, serious psychological distress), and behavioral health (binge drinking). Residents marginalized because of racial, ethnic, and sexual minority status were more likely to be stopped, searched, or questioned by the police; threatened or abused by the police; and discriminated against by the police or in the courts; those experiences were associated with poor physical, mental, and behavioral health outcomes. The associations between experiences with police and poor health outcomes were strongest among Black residents and residents aged 25–44. Our findings suggest that the health of NYC residents who have had exposure to police and experienced discrimination by the police and courts is poorer than those who have not, and build on a growing body of evidence that aggressive policing practices have implications for public health.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Communities marginalized because of racism, heterosexism, and other systems of oppression in New York City (NYC), and other large urban areas in the United States (US), have experienced a long history of aggressive policing [1,2,3]. Aggressive policing is a practice in which pedestrians are stopped for low-level offenses or suspicion of an offense with the intention of preventing more serious crime [3]. The conceptual origin of aggressive policing practices is the Broken Windows Theory developed by social scientists George Kelling and James Wilson and introduced in The Atlantic magazine in 1982 [4]. The untested yet widely accepted theory hypothesized that signs of the disorder, such as a broken window, are a signal of limited neighborhood collective efficacy and social cohesion and control, and consequently, there is no formal or informal punishment in the neighborhood for acts of disorder. Thus, reducing serious crime starts with the prevention of minor offenses that create the appearance of disorder. When applied in practice, this theory shifts policing focus to low-level crimes [4]. Quality-of-life (QOL) policing, introduced in NYC in 1994, was an early iteration of an aggressive policing policy. QOL policing targeted low-level, nonviolent offenses for which a person could be arrested or issued a summons [5], both requiring adjudication in the court. Another aggressive policing practice is stop, question and frisk (SQF). Introduced in 2003, SQF permitted police officers to stop and question a person based on probable cause, then frisk the person for weapons or other contraband [1]. In 2013, this practice in NYC was found by a federal judge to be unconstitutional and racially discriminatory [6].
Aggressive policing practices operate at multiple levels to compound marginalization of communities already marginalized because of racism [7] and heterosexism [8]. At the institutional level, aggressive policing practices such as SQF are concentrated among socially disadvantaged communities [9]. For example, Black and Latino New Yorkers are disproportionately stopped and ordered to appear in court, with nearly 12,000 Black and Latino New Yorkers stopped by the police in 2019, compared to just over 1000 White New Yorkers [10]. The disparity at the intersection of age, race, and gender is more stark. For example, the average yearly rate of stops between 2004 and 2012 was highest among 18-year-old Black male New Yorkers at 976 per 1000 Black males. The rate of stops for 18-year-old White male New Yorkers was well below 250 per 1000 White males [11]. At the interpersonal level, Black, Latino, and sexual minority individuals have been found across a number of studies to be more likely to report experiencing discrimination—differential treatment based on social identity—when interacting with the police than individuals not occupying those identities [12,13,14,15,16,17]. Another study found that among individuals with recent court experiences, Black individuals were more likely than White individuals to report having negative experiences, including perceiving court procedures and outcomes as unfair and low levels of concern and respect displayed by the court [18].
As a consequence of differential practices by the criminal legal system based on race, ethnicity, and sexual identity, socially marginalized communities might bear a disproportionate burden of poor health from aggressive policing. The ecosocial theory posits that it is the embodiment of socially structured—patterns of human relationships by social position—conditions that contribute to the distribution of disease in a population [19]. Populations positioned lower on the social structure, or socially marginalized populations, because of racism, heterosexism, or other systems of oppression are differentially exposed—contemporarily and historically—to negative conditions that render them vulnerable to disease via diverse, concurrent, and interacting pathways that accumulate over the life course [19]. Aggressive policing practices are socially structured exposures [7, 8] that can increase vulnerability to disease via stress pathways [20] linked to mental [20] and physical [21] health outcomes. In addition, these practices can also increase the risk of poor behavioral health outcomes such as excessive alcohol use to cope with the stress of a police-initiated contact [22, 23]. Past analyses indicate that police stops and abuse are associated with poor mental, physical, and behavioral health outcomes [24]. Studies have also found discrimination by the police is associated with health; if an individual experienced a police encounter as discriminatory, the association with poor mental health was stronger [25].
Previous studies on police encounters and health outcomes, however, have had several limitations. Prior studies that used representative samples either did not take into account factors known to be associated with health outcomes (e.g., education and income) [24] or solely employed an aggregated neighborhood-level police exposure [26]. To address these gaps, we examine the associations of self-reported police stops and abuse and discrimination by the police and courts, with poor physical, mental, and behavioral health outcomes in a representative sample of adult residents in NYC. Our hypotheses are informed by the ecosocial theory. We hypothesize that there will be a positive association between police stops, abuse by the police, and discrimination by the police and courts and poor health outcomes. Considering the embodiment of socially structured conditions [19], we also examine whether these associations vary by race and ethnicity. Moreover, the embodiment of socially structured conditions [19] accumulates over the life course [19]; therefore, we also examine whether these associations vary by age. We hypothesize that the associations will be stronger among individuals who experience racism, such as Black and Latino populations, and among those who are older.
Methods
Data
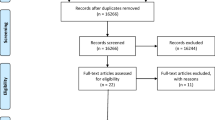
We analyzed data from the 2017 Social Determinants of Health (SDH) Survey, a cross-sectional survey of 2335 adults aged 18 and older conducted by the NYC Department of Health and Mental Hygiene to assess health and wellness. The SDH survey sample was drawn using both random digit dialing and address-based sampling, with surveys completed via landline telephone or cell phone interviews (n = 1433), web (n = 247), or pencil-and-paper (n = 655). With the purpose of having data be representative of the NYC adult population, data collected from telephone interviews were adjusted for initial probability of selection, dual cell phone and landline use, and non-response. Data collected from landline interviews were additionally adjusted for the probability of respondent selection in a household with multiple adults and for respondents in a household with two or more landlines. The survey had an overall response rate of 11.6% and cooperation rate of 80.4%, using modified versions of the American Association for Public Opinion Research’s (AAPOR) Response and Cooperation Rates #3 [27].
Estimates presented here are based on self-reported data, which were weighted to represent the 2015 NYC adult residential population (n = 6,585,635) using American Community Survey demographic data. The weighting approach reduced differences in health measures across survey modes [28]. Data were age adjusted to the United States 2000 standard population. Phone interviews were conducted in English, Spanish, Russian, Mandarin, and Cantonese; surveys completed online and by pencil-and-paper were in English.
Measures
We focused on three exposures of interest: self-reported lifetime experience of being stopped by police, assessed with the question “Have you ever been stopped, searched, or questioned by the police?;” self-reported lifetime experience of threats or abuse by the police, assessed with the question “Have you ever been physically threatened or abused by the police?;” and lifetime experience of racial discrimination by the police or court system, assessed with the question “Have you ever experienced discrimination, been prevented from doing something or been hassled or made to feel inferior because of your race, ethnicity, or color from the police or in the courts?” Below we refer to each of these constructs as being stopped by the police, experiencing police abuse, and experiencing discrimination by police or in courts, respectively.
We examined four physical, mental, and behavioral health outcomes. In alignment with the measures used by the Behavioral Risk Factor Surveillance System (BRFSS), poor physical health and mental health were defined by the reported number of days that each was not good in the last 30 days, dichotomized as poor (14 days or more) versus not poor (13 days or less) for both physical and mental health [29, 30]. Also in line with BRFSS measurements [29], serious psychological distress in the last 30 days was defined by a score of 13 or greater on the Kessler Psychological Distress Scale (K6), based on analyses to determine the optimal cut point for classification accuracy [31]. We used the definition of the National Institute of Alcohol Abuse and Alcoholism to examine binge drinking, defined as having 5 or more drinks for men and 4 or more drinks for women on a single occasion in the last 30 days [32].
Analysis
We calculated age-adjusted prevalence estimates of being stopped by the police, abused by the police, or experiencing discrimination by police or in courts by sociodemographic characteristics and health outcomes and behaviors (PROC DESCRIPT [33]; we used CONTRAST [33] statements to perform 2-tailed tests of significance (α = 0.05)).
We first evaluated the association between each of the exposures of interest and the selected health outcomes using multivariable logistic regression models (PROC RLOGIST and PRED_EFF [33] for pairwise comparisons). As most outcomes were relatively common (prevalence > 10%), we used the ADJRR [33] statement to obtain model-adjusted risk ratios (RRs) and 95% confidence intervals (CIs); this approach computes the ratio of predicted marginal proportions for logistic regression models. Multivariable models were adjusted for potential confounders of the relationship between our exposures and outcomes of interest, based on our review of extant literature [24,25,26]: nativity status (born in the US or elsewhere), household income (< 200% versus ≥ 200% of the Federal Poverty Level, FPL), and education (less than high school, high school graduate, some college, and college graduate). We investigated the potential collinearity of variables in the models and found variation inflation factors did not exceed 2.22, indicating low collinearity.
Based on our interest in examining differences across socially structured groups and the accumulation of negative conditions experienced by populations low on the social structure, we then explored effect measure modification to determine whether the strength of the association varied by race and ethnicity (Black, Latino, White, Asian/Pacific Islander, Other/Multi-race), by age (18–24, 25–44, 45–64, 65 +), and by sex (male/female) by testing 2-way interaction terms (α = 0.1). Statistical analyses were performed using SAS Enterprise Guide 7.15 software (Cary, NC) and SAS-callable SUDAAN 11.01 software (Research Triangle Institute, Research Triangle Park, NC) to account for the complex survey design. Statistical significance was determined at two-sided p-values < 0.05.
Results
Overall, 29.3% of NYC adult residents reported having ever been stopped by police (weighted N = 1,941,000), 8.7% reported having ever experienced police abuse (weighted N = 577,000), and 14.6% reported having ever experienced discrimination by police or in courts (weighted N = 950,000). Those who reported having ever been stopped by police were more likely to be male; be gay, lesbian or bisexual; be born in the US; have a household income equal to or greater than 200% of the Federal Poverty Level (FPL); and not be in the labor force (Table 1). They were less likely to be Asian/Pacific Islander and to be aged 65 years and older. People who reported having ever experienced police abuse were more likely to be male; be Black or Other/Multi-race; be born in the US; have a household income less than 200% of FPL; and have completed some college, completed high school, or have education less than a high school degree. They were less likely to be older than 65 years of age. People having experienced discrimination by police or in courts were more likely to be male; be Black or Latino or Other/Multi-race; be born in the US; have a household income less than 200% of FPL; and have a high school degree or less than a high school education. NYC residents who reported having ever been stopped by police or having ever been abused by police were more likely to report poor physical health in the past 30 days (17.5% and 29.4%, respectively), as compared to those who had not had these experiences (11.0% and 11.8%, respectively) (Table 2). People reporting having ever been stopped by police, having ever been abused by police, or having ever experienced discrimination by police or in courts were approximately twice as likely to report poor mental health in the last 30 days (20.4%, 26.7%, and 21.3%, respectively) compared to those who had not had these experiences (11.9%, 13.5%, and 13.3%, respectively). Similarly, people who had ever experienced police abuse were over twice as likely (13.8%) as those who had not (5.8%) to report serious psychological distress, and over one-quarter of people ever stopped by police reported binge drinking (27.4%), compared to 17.9% of those never stopped by police.
After adjusting for education, household income and US nativity, ever having been stopped by police (RR: 1.68; 95% CI 1.23, 2.30), ever having been abused by police (RR: 1.67; 95% CI 1.07, 2.60), and ever having experienced discrimination by police or in courts (RR: 1.52; 95% CI 1.02, 2.27) were all positively associated with poor mental health (Table 3). Having been stopped by police and having experienced police abuse was positively associated with poor physical health (RR: 1.74; 95%CI 1.27, 2.38 and RR: 2.27; 95% CI 1.51, 3.40 respectively), and police abuse was positively associated with serious psychological distress (RR: 2.27; 95% CI 1.31, 3.92). Having ever been stopped by police and having ever experienced discrimination by police or in courts was positively associated with binge drinking (RR: 1.47; 95% CI 1.16, 1.86 and RR: 1.39; 95% CI 1.05, 1.85, respectively).
The associations between having ever been stopped by police, abused by police, or having experienced discrimination by police or in courts and health outcomes varied by race and ethnicity (Table 4). Associations were more often observed among Black NYC residents, with the likelihood of reporting adverse physical, mental, or behavioral health outcomes up to three and a half times greater among people having ever been stopped by police, or having ever experienced police abuse or discrimination by police or in courts. Fewer associations were observed among White, Latino, and Asian/Pacific Islander residents as well as among those of other or multiple races. While some point estimates in these strata were of larger magnitude, their wide confidence intervals suggest they are possibly unreliable owing to smaller cell sizes.
Variation was also observed across age groups (Table 5). Associations were most often observed among NYC adults aged 25–44 years, with people having ever been stopped by police, or having ever experienced police abuse or discrimination by police or in courts up to four times as likely to report adverse physical, mental, and behavioral health outcomes. Fewer associations were observed among the youngest (18–24 years), middle-aged (45–64 years), and oldest (65 + years) NYC residents, though the magnitude of some point estimates was similar to those of New Yorkers aged 25–44 years.
Discussion
The criminal legal system is one of multiple systems of oppression that disproportionately impacts and marginalizes Black, Latino, and sexual minority individuals by exposing them to adverse conditions such as aggressive policing practices [7, 8, 22, 34, 35]. We examined the associations of policing practices and discrimination with health among a representative sample of adult NYC residents, as well as whether those associations varied by race and ethnicity and age. We found that approximately one-third (29%) had ever been stopped by the police, close to 10% had ever been physically abused by police and almost 15% had ever experienced racial discrimination from the police or in the courts. We also found that gay, lesbian, and bisexual New Yorkers were more likely to report being stopped by police than heterosexual New Yorkers and Black New Yorkers were more likely to report being abused by police and experience racial discrimination by the police or in courts than White New Yorkers. Our findings on rates of stops and abuse contribute to a growing body of literature on the quantity and character of police contacts in large urban areas. Analyses by Geller and colleagues focusing on young adult men in NYC [25] found a much higher rate of stops (85%), while Hirschtick and colleagues found that 21% of residents of select Chicago neighborhoods experienced at least three police stops and 4% experienced stops characterized as aggressive [36]. Notably, we did not find differences across race and ethnicity in stops, although Black and Latino New Yorkers were disproportionately stopped based on stop, question, and frisk data [10]. However, our assessment of police stops had a lifetime timeframe and was not specific to street stops, a focus of aggressive policing practices. We did find, however, that Black New Yorkers were more likely to report having ever been abused by the police and that Black and Latino New Yorkers were more likely to report having ever experienced racial discrimination by police or in courts than White New Yorkers. These latter findings reflect racial and ethnic differences in interpersonal experiences with the police.
We also found that NYC residents with the lived experiences of police contact and discrimination were more likely to report several poor health outcomes relative to those who had not had those experiences with police. Having been stopped by the police was associated with poor physical and mental health and with binge drinking; having been abused by the police was associated with poor physical and mental health and with psychological distress; and having experienced racial discrimination by police and the courts were associated with poor mental health and binge drinking. Informed by the ecosocial theory of disease distribution, we also examined whether associations between police contacts and discrimination by the police or in court and health outcomes varied by race and ethnicity and age. We hypothesized that the associations between police contact and racial discrimination by the police and courts and health outcomes would be stronger among individuals socially marginalized because of race and ethnicity and older age groups. We found that the associations were more common and most consistently stronger among Black New Yorkers than for other racial and ethnic groups. Our findings on older New Yorkers were not consistent with our study hypothesis, as the association between having ever been stopped or abused by police or having ever faced discrimination by police or in courts with poor health outcomes was most often observed among New Yorkers aged 25 to 44 years as compared to their younger and older counterparts. While all New Yorkers have resided in a city with aggressive policing practices, the 25- to 44-year-old cohort would have been exposed on an ongoing basis to these practices which initiated during their young adult years, which may explain our findings among this age group.
Our finding that NYC residents who had ever had contact with the police were more likely to experience poor health outcomes is generally consistent with previous research [24, 26]. Similar to Geller et al. (2014), who found police contact associated with poor mental health among young adult men [25], we observed an association for serious psychological distress among younger adult New Yorkers who had ever been abused by police, but did not identify further associations between mental health measures and other experiences of police contact. Geller et al. (2014) examined associations between recent police contacts and health during the peak years of SQF (2012–2013), whereas our study asked about lifetime police contact [10]. We did not find the 2-way interaction term for sex significant in our analyses, and therefore, we did not stratify by sex, which may have obscured the experience of younger men in our analyses.
Our findings on Black New Yorkers are consistent with previous research indicating that police contacts may be harmful to the physical and mental health of Black individuals throughout the US [26, 34, 35, 37,38,39]. A systematic literature review identified, across studies, a nearly twofold higher prevalence of poor mental health among Black Americans who report any prior police interaction compared to those who did not [34]. In their study on multiple lifetime police interactions and mental health, Hirschtick et al. (2020) found that those who reported a higher number of lifetime police stops had three times greater odds of experiencing post-traumatic stress disorder (PTSD) symptoms compared to those who reported fewer stops [36]. These findings echo those of Geller et al. (2014) and Jackson et al. (2019), whose research indicated that more intrusive police contacts were associated with current and lifetime trauma, anxiety symptoms, and/or emotional distress [25, 38]. Additionally, Black residents in our study were more likely than their racial and ethnic counterparts to be subjected to abusive police behavior [40]. Together, these findings may indicate the particular salience for the health of any racialized exposures for Black Americans because they are reminders of other, past, and historical racial traumas [41] and that the effects of these exposures are unique and extend beyond the typical effects of other violence exposures on mental health [20].
A major strength of our study is the use of 2017 SDH Survey data, which included information on lifetime exposure of police contact and discrimination by police and the courts as well as several sociodemographic characteristics and health outcomes. This dataset allowed the opportunity to examine the relationship between these variables in a weighted sample that is representative of the adult NYC population.
Study limitations included the cross-sectional nature of the survey data which restricted our ability to establish the temporal relation of police contact and discrimination with poor health outcomes, as well as our ability to establish causality. As suggested by the increase in reports of anxiety and symptoms of depression among Black people observed in the wake of George Floyd’s murder [42, 43], the increasingly publicized nature of police violence experienced via the media may contribute to poor mental health [44]; this was not accounted for in our analysis. Despite a high cooperation rate among participants contacted, the low response rate among eligible participants may potentially hamper generalizability. Furthermore, the data did not include information on the timing and frequency of police contact or court experiences during the life course or on the geographic location of said experiences. While we acknowledge the concentration of policing in particular neighborhoods, as well as the role of the built environment in shaping health, the dataset did not contain elements that permit us to control for or explore geographic variability. Underreporting of police contact is possible given the sensitive nature of the topic and could be differential across racial and ethnic and age groups. Potential recall bias, especially among older adults, could have also resulted in underreporting of police contact, though the higher likelihood of recalling negative police contacts than positive ones may mean that our findings on the associations between police contacts and health may be biased towards contacts assessed as negative [45]. Past research [46, 47] has highlighted the disproportionate police contact and interaction with the carceral system experienced by people with darker complexions, and as such, the absence of data on colorism in our analysis is an important limitation. Our measures were self-reported with inherent limitations related to what respondents were willing to share and social desirability bias [48]. We did not adjust for multiple comparisons in our analysis; had we done so, it is possible that fewer findings would be statistically significant. Finally, we did not test measurement nonequivalence for the outcomes of interest, though past research has highlighted some estimation differences for Kessler-6 across racial/ethnic groups [49]. Notwithstanding limitations, our findings are relevant to aggressive policing practices employed in cities throughout the US and their association with adverse health outcomes.
Conclusion
Public policies related to the criminal legal system in the US inequitably impact the health of socially marginalized communities. Policing policies are no exception. Many police departments in large urban areas have embraced aggressive policing practices such as SQF and quality-of-life policing with the goal of preventing disorder and deterring crime. Black and Latino New Yorkers have been inequitably subjected to decades of these aggressive policing practices, which we have found to be associated with a range of poor health outcomes. Our findings, in combination with the growing body of literature on the relationship between criminal legal exposures and health, can inform municipalities and states in the US that are increasingly considering changes to policing and criminal legal approaches [50,51,52], in particular community-based and health-centered approaches to community safety. These include efforts to shift more resources towards community services such as substance use disorder treatment and housing [53]; increasing transparency and accountability for police misconduct [54]; decriminalizing or de-prioritizing arrest for low-level crimes associated with substance use or poverty [55]; and programs to dispatch health professionals for mental health emergencies, rather than police [56]. Finally, as noted by the American Public Health Association [51], the epidemic of police violence is a public health crisis. It is urgent that public health surveillance systems include data on the impact of exposure to police contact and discrimination and to the carceral system on health outcomes. This would allow researchers to highlight the critical evidence to inform and reform policies that disproportionately impact individuals and communities of color.
References
Jones-Brown D. Stop, question & frisk policing practices in New York City: a primer. Center on Race, Crime and Justice John J College of Criminal Justice; 34.
Stoudt BG, Fine M, Fox M. Growing up policed in the age of aggressive policing policies. N Y Law Sch Law Rev. Published online 2012 2011:1332–1370.
Zero Tolerance and Aggressive Policing (And Why To Avoid It) Quick Guide. Accessed March 2, 2021. https://www.rand.org/pubs/tools/TL261/better-policing-toolkit/all-strategies/zero-tolerance.html.
Wilson JQ, Kelling GG. Broken Windows. Atl Mon. 1982;249(3):29–38.
Vitale AS. Innovation and institutionalization: factors in the development of “quality of life” policing in New York City. Polic Soc. 2005;15(2):99–124. https://doi.org/10.1080/10439460500071754.
Fangman JL. Stop the stop and frisk: how Floyd v. City of New York will limit the power of law enforcement across the nation. Public Interest Law Rep. 2013;19:50.
National Academies of Sciences, Engineering, and Medicine. The criminal justice system and Social exclusion: race, ethnicity, and gender: proceedings of a workshop—in brief. National Academies of Sciences, Engineering, and Medicine; 2018. https://doi.org/10.17226/25247.
United States of America Stonewalled : Police Abuse and Misconduct against Lesbian, Gay, Bisexual and Transgender People in the U.S. Amnesty International, New York, NY; 2005.
Nolan T. Perilous policing: criminal justice in marginalized communities. Routledge, New York, NY; 2019.
Stop-and-Frisk Data. New York Civil Liberties Union. Accessed February 24, 2021. https://www.nyclu.org/en/stop-and-frisk-data.
Figu KD, Legewie J. Visualizing police exposure by race, gender, and age in New York City. Socius. 2019;5:2378023119828913. https://doi.org/10.1177/2378023119828913.
Bleich SN, Findling MG, Casey LS, et al. Discrimination in the United States: experiences of Black Americans. Health Serv Res. 2019;54(S2):1399–408. https://doi.org/10.1111/1475-6773.13220.
Findling MG, Bleich SN, Casey LS, et al. Discrimination in the United States: experiences of Latinos. Health Serv Res. 2019;54(S2):1409–18. https://doi.org/10.1111/1475-6773.13216.
Casey LS, Reisner SL, Findling MG, et al. Discrimination in the United States: experiences of lesbian, gay, bisexual, transgender, and queer Americans. Health Serv Res. 2019;54(S2):1454–66. https://doi.org/10.1111/1475-6773.13229.
Bowleg L, Maria del Río-González A, Mbaba M, Boone CA, Holt SL. Negative police encounters and police avoidance as pathways to depressive symptoms among US Black Men, 2015–2016. Am J Public Health. 2020;110(S1):S160–6. https://doi.org/10.2105/AJPH.2019.305460.
Remch M, Duncan DT, Geller A, et al. Police harassment and psychosocial vulnerability, distress, and depressive symptoms among black men who have sex with men in the U.S.: longitudinal analysis of HPTN 061. SSM - Popul Health. 2021;13:100753. https://doi.org/10.1016/j.ssmph.2021.100753.
Feelemyer J, Duncan DT, Dyer TV, et al. Longitudinal associations between police harassment and experiences of violence among Black men who have sex with men in six US cities: the HPTN 061 study. J Urban Health. 2021;98(2):172–82. https://doi.org/10.1007/s11524-021-00526-1.
Sun IY, Wu Y. Citizens’ perceptions of the courts: the impact of race, gender, and recent experience. J Crim Justice. 2006;34(5):457–67. https://doi.org/10.1016/j.jcrimjus.2006.09.001.
Krieger N. Methods for the scientific study of discrimination and health: an ecosocial approach. Am J Public Health. 2012;102(5):936–44. https://doi.org/10.2105/AJPH.2011.300544.
DeVylder J, Fedina L, Link B. Impact of police violence on mental health: a theoretical framework. Am J Public Health. 2020;110(11):1704–10. https://doi.org/10.2105/AJPH.2020.305874.
Geronimus AT, Hicken M, Keene D, Bound J. “Weathering” and age patterns of allostatic load scores among Blacks and Whites in the United States. Am J Public Health. 2006;96(5):826–33. https://doi.org/10.2105/ajph.2004.060749.
Duarte CD, Salas-Hernandez L, Griffin JS. Policy determinants of inequitable exposure to the criminal legal system and their health consequences among young people. Am J Public Health. 2020;110(S1):S43–9.
Verplaetse TL, Peltier MR, Roberts W, Pittman B, McKee SA. Gender and past year serious psychological distress are associated with past year AUD: time-varying results from the National Survey on Drug Use and Health (NSDUH; 2008–2017). Addict Behav. 2021;116: 106815. https://doi.org/10.1016/j.addbeh.2020.106815.
Zweig K, Baquero M, Meropol S, Vasan A. Criminal justice system involvement and measures of health among New York City residents 2017. New York City Department of Health and Mental Hygiene, New York, NY; 2019.
Geller A, Fagan J, Tyler T, Link BG. Aggressive policing and the mental health of young urban men. Am J Public Health. 2014;104(12):2321–7.
Sewell AA, Jefferson KA, Lee H. Living under surveillance: gender, psychological distress, and stop-question-and-frisk policing in New York City. Soc Sci Med. 1982;2016(159):1–13.
The American Association for Public Opinion Research (AAPOR). Standard definitions: final dispositions of case codes and outcome rates for surveys. 9th ed., Washington, DC; 2016.
Immerwahr S, Lim S, Brassell T, ZuWallck RS, Levanon Seligson A. Is ABS more respresentative than RDD for public health surveillance surveys? Presented at the: 73rd annual AAPOR Conference; May 17, 2018.
Centers for Disease Control and Prevention. Calculated variables in the 2019 data file of the behavioral risk factor surveillance system (Version #11-Revised). Centers for Disease Control and Prevention, Atlanta, GA; 2020.
Healthy Days Core Module: HRQOL-14 Measure | HRQOL | CDC. Published November 5, 2018. Accessed February 23, 2021. https://www.cdc.gov/hrqol/hrqol14_measure.htm.
Kessler RC, Barker PR, Colpe LJ, et al. Screening for serious mental illness in the general population. Arch Gen Psychiatry. 2003;60(2):184–9. https://doi.org/10.1001/archpsyc.60.2.184.
NIAAA council approves definition of binge drinking. NIAAA Newsl. 2004;3(3).
Bieler G. SUDAAN Language Manual, Release 10.0. RTI International; 2008.
McLeod MN, Heller D, Manze MG, Echeverria SE. Police interactions and the mental health of Black Americans: a systematic review. J Racial Ethn Health Disparities. 2020;7(1):10–27. https://doi.org/10.1007/s40615-019-00629-1.
Alang S, McAlpine D, McCreedy E, Hardeman R. Police brutality and Black health: setting the agenda for public health scholars. Am J Public Health. 2017;107(5):662–5. https://doi.org/10.2105/AJPH.2017.303691.
Hirschtick JL, Homan SM, Rauscher G, et al. Persistent and aggressive interactions with the police: potential mental health implications. Epidemiol Psychiatr Sci. 2020;29. https://doi.org/10.1017/S2045796019000015.
DeVylder JE, Cogburn C, Oh HY, et al. Psychotic experiences in the context of police victimization: data from the survey of police–public encounters. Schizophr Bull. 2017;43(5):993–1001. https://doi.org/10.1093/schbul/sbx038.
Jackson DB, Fahmy C, Vaughn MG, Testa A. Police stops among at-risk youth: repercussions for mental health. J Adolesc Health. 2019;65(5):627–32. https://doi.org/10.1016/j.jadohealth.2019.05.027.
DeVylder JE, Jun H-J, Fedina L, et al. Association of exposure to police violence with prevalence of mental health symptoms among urban residents in the United States. JAMA Netw Open. 2018;1(7):e184945–e184945. https://doi.org/10.1001/jamanetworkopen.2018.4945.
Kramer R, Remster B. Stop, frisk, and assault? Racial disparities in police use of force during investigatory stops. Law Soc Rev. 2018;52(4):960–93. https://doi.org/10.1111/lasr.12366.
Mohatt NV, Thompson AB, Thai ND, Tebes JK. Historical trauma as public narrative: a conceptual review of how history impacts present-day health. Soc Sci Med. 2014;106:128–36. https://doi.org/10.1016/j.socscimed.2014.01.043.
Eichstaedt JC, Sherman GT, Giorgi S, et al. The emotional and mental health impact of the murder of George Floyd on the US population. Proc Natl Acad Sci. 2021;118(39): e2109139118. https://doi.org/10.1073/pnas.2109139118.
Depression and anxiety spike among Black Americans after George Floyd’s death - the Washington Post. Accessed October 15, 2021. https://www.washingtonpost.com/health/2020/06/12/mental-health-george-floyd-census/.
Bor J, Venkataramani AS, Williams DR, Tsai AC. Police killings and their spillover effects on the mental health of Black Americans: a population-based, quasi-experimental study. Lancet. 2018;392(10144):302–10. https://doi.org/10.1016/S0140-6736(18)31130-9.
Skogan WG. Asymmetry in the impact of encounters with police. Polic Soc. 2006;16(2):99–126. https://doi.org/10.1080/10439460600662098.
Alcalá HE, Montoya MFL. Association of skin color and generation on arrests among Mexican-Origin Latinos. Race Justice. 2018;8(2):178–93. https://doi.org/10.1177/2153368716670998.
Geller A, Monk E. Race, Skin Tone, and Police Contact Among Contemporary Teens. Princeton University, School of Public and International Affairs, Center for Research on Child Wellbeing.; 2019. Accessed October 7, 2021. https://ideas.repec.org/p/pri/crcwel/wp19-07-ff.html.
Krieger N. Measures of racism, sexism, heterosexism, and gender binarism for health equity research: from structural injustice to embodied harm—an ecosocial analysis. Annu Rev Public Health. 2020;41(1):37–62. https://doi.org/10.1146/annurev-publhealth-040119-094017.
Kim G, DeCoster J, Bryant AN, Ford KL. Measurement equivalence of the K6 scale: the effects of race/ethnicity and language. Assessment. 2016;23(6):758–68. https://doi.org/10.1177/1073191115599639.
Lo K. Assessing the state of police reform. Center for American Progress. American Public Health Association (APHA), Washington, DC. Published July 16, 2020. Accessed March 1, 2021. https://www.americanprogress.org/issues/criminal-justice/news/2020/07/16/487721/assessing-state-police-reform/.
APHA. Policy statement: addressing law enforcement violence as a public health issue; National Association of County and City Health Officials (NACCHO), Washington, DC; 2018.
NACCHO. Policy statement: public health, racism, and police violence; 2015.
Closing Rikers Island: a roadmap for reducing jail in New York City. Center for Court Innovation. George Floyd Justice in Policing Act of 2021. HR. 1280. 117th Congress (2021‐2022)\. Accessed October 15, 2021. https://www.courtinnovation.org/publications/reducing_jail_Rikers/.
Bass K. George Floyd Justice in Policing Act of 2021; NY State Assembly Bill A2212. N.Y. Legis. Assemb, A2212 2021‐2022. 2021‐2022 Legislative Session. Section 160.50 of the criminal procedure la; 2021.
Aubry J. AN ACT to Amend the Criminal Procedure Law; 2019.
B-HEARD Transforming NYC’s Response to Mental Health Crises: First Month of Operations. Mayors Office of Community Mental Health; 2021. https://mentalhealth.cityofnewyork.us/wp-content/uploads/2021/07/B-HEARD-First-Month-Data.pdf. Accessed 10/16/21.
Acknowledgements
We would like to thank the generous guidance and support provided by Marivel Davila and Nneka Lundy De La Cruz (NYC DOHMH), Francesca Gany (Memorial Sloan Kettering Cancer Center), and the From Punishment to Public Health (P2PH) initiative at John Jay College of Criminal Justice.
Funding
This study was conducted through the Marginalized Populations Health Data for New York City (HD4NYC) Working Group. HD4NYC, funded by the Robert Wood Johnson Foundation and led by the New York Academy of Medicine and the New York City Department of Health and Mental Hygiene, is a multi-institutional research platform that seeks to advance health equity by producing actionable, policy-relevant research, and promoting the careers of academic and applied public health researchers.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Azure Thompson and María Baquero contributed equally to this work.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Thompson, A., Baquero, M., English, D. et al. Associations between Experiences of Police Contact and Discrimination by the Police and Courts and Health Outcomes in a Representative Sample of Adults in New York City. J Urban Health 98, 727–741 (2021). https://doi.org/10.1007/s11524-021-00583-6
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11524-021-00583-6