
Abstract
Electrochemotherapy is an effective antitumor treatment currently applied to cutaneous and subcutaneous tumors. Electrochemotherapy of tumors located close to the heart could lead to adverse effects, especially if electroporation pulses were delivered within the vulnerable period of the heart or if they coincided with arrhythmias of some types. We examined the influence of electroporation pulses on functioning of the heart of human patients by analyzing the electrocardiogram. We found no pathological morphological changes in the electrocardiogram; however, we demonstrated a transient RR interval decrease after application of electroporation pulses. Although no adverse effects due to electroporation have been reported so far, the probability for complications could increase in treatment of internal tumors, in tumor ablation by irreversible electroporation, and when using pulses of longer durations. We evaluated the performance of our algorithm for synchronization of electroporation pulse delivery with electrocardiogram. The application of this algorithm in clinical electroporation would increase the level of safety for the patient and suitability of electroporation for use in anatomical locations presently not accessible to existing electroporation devices and electrodes.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
The combined treatment in which delivery of chemotherapeutic drug is followed by application of high-voltage electric pulses locally to the tumor has been termed electrochemotherapy. The effect of local electropermeabilization of the cell membrane (the disruption of the lipid matrix and creation of aqueous pathways [10, 38]), also termed electroporation, transiently enables the entry of anticancer drugs, such as bleomycin or cisplatin, into the cells and hence greater effectiveness of tumor treatment. Electrochemotherapy has been successfully used for treatment of cutaneous and subcutaneous tumors irrespective of their histological origin in different animal tumor models and in humans [19, 36, 51, 52]. In these studies, a typical electrochemotherapy protocol involved eight electroporation pulses (EP pulses) with amplitude of about 1,000 V, duration 100 μs, repetition frequency 1 Hz, and inter-electrode distance 8 mm. However, the protocol involving eight EP pulses at repetition frequency of 5 kHz has been suggested and is currently replacing the 1-Hz protocol due to a lesser discomfort and pain inflicted to patients [31, 57]. Electrodes of three different configurations can be used for EP pulse delivery during electrochemotherapy. EP pulses applied by plate electrodes are used in case of superficial tumor nodules whereas EP pulses to deeper-seated tumors (subcutaneous nodules) are applied using needle row array electrodes (eight needle electrodes arranged in two rows) or needle hexagonal array electrodes (six hexagonally arranged electrodes with the seventh electrode in the centre) [31]. The number of applied EP pulses and pulse repetition frequency depend on the electrode type and define the duration of electroporation, which is 1.6 ms for plate and needle row array electrodes [31] and approximately 200 ms for needle hexagonal array electrodes [31, 45]. New protocols for delivery of EP pulses are either already in use or are being developed. For gene electrotransfer three different EP pulse protocols are in use: short high-voltage EP pulses, EP pulses of a much longer duration (in the order of milliseconds), or combination of short high-voltage EP pulses with very long low-voltage electrophoretic pulses (amplitude 50–100 V, duration 100 ms) [8, 18, 20, 40, 48]. Tumor ablation by irreversible electroporation is another recently developed application, where EP pulses with larger amplitudes (up to 3,000 V) and longer durations (up to 24 ms) are delivered [3, 14, 28, 35]. New applications using endoscopic or surgical means to access internal tumors are also being developed [21].
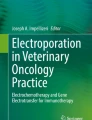
Electrochemotherapy is reported as an efficient and safe method. No adverse effects have been reported so far. Electrochemotherapy causes only minor side effects in the patients such as the transient lesions in areas in direct contact with the electrodes [37] and acute localized pain due to contraction of muscles in vicinity of the electrodes [36, 57]. The induced contraction could present a problem if provoked in the heart muscle [46]. There is very little chance that currently used electroporation protocols could interfere with functioning of the heart since there is no such practical evidence. However, this issue has not been systematically investigated yet. Given the increasing need for palliative treatment of internal tumors, the possibility of EP pulses interfering with functioning of the heart is emerging for tumors located close to the heart muscle. Among possible irregularities of functioning of the heart that the application of EP pulses could induce (e.g., atrial and ventricular flutter and fibrillation, premature heartbeats), the most dangerous is ventricular fibrillation [46]. Fibrillation can be induced if electrical stimulus is delivered during late atrial or ventricular systole, during the so-called vulnerable period of the heart [25, 46, 55] (Fig. 1). For ventricular myocardium, the vulnerable period coincides with the middle and terminal phases of the T wave [46], but higher shock strengths cause the vulnerable period to occur several milliseconds earlier in the heartbeat [27]; therefore, the whole T wave can be considered to be within the vulnerable period of the ventricles. For the atria, the vulnerable period is somewhere in the S wave [46]. Externally applied electric pulses delivered outside the vulnerable period have extremely low probability of inducing ventricular fibrillation [46]. According to this fact the synchronization of EP pulse delivery with electrocardiogram (ECG) would increase safety of the patient. The likelihood of electroporation to influence functioning of the heart depends also on applied pulse voltage, duration, number and repetition frequency of EP pulses, and electric current pathway [46].

The vulnerable period and characteristics of a typical heartbeat
Although fibrillation can occur in normal and healthy hearts, it is more likely in hearts with structural or functional abnormalities [11]. Abnormalities of the heart rhythm (arrhythmias) are indicated by significant deviation of RR interval from its normal value [12, 46]. During some arrhythmias the heart becomes more susceptible to external stimuli due to a decreased threshold level for fibrillation. Therefore EP pulses coinciding with some arrhythmias could elicit fibrillation. This potential danger is most significant after premature heartbeat, the extrasystole [46].
The main purpose of this study was therefore to investigate the possible effects of EP pulses on functioning of the heart and to address the relevance of synchronization of EP pulse delivery with ECG. In this context we also evaluated the performance of our previously developed algorithm for QRS detection and synchronization of EP pulse delivery with ECG [30].
2 Methods and materials
2.1 Patients and electrochemotherapy
Fourteen human patients were included in this study. Before electrochemotherapy treatment a signed consent was obtained from each patient. Patients were treated according to the electrochemotherapy protocols as described by Marty et al. [31] with the addition of ECG monitoring. Electrochemotherapy drugs (cisplatin or bleomycin) were administered locally to tumors. EP pulses were generated by the electric pulse generator Cliniporator™ (IGEA S.R.L., Carpi, Italy). Altogether 93 applications of EP pulses were performed. Main characteristics of the patients, tumors and electrochemotherapy are presented in Table 1.
We recorded 16 ECG signals on 14 patients during electrochemotherapy at the Institute of Oncology in Ljubljana. Two patients were treated twice. Thus ECG signals number 1 and 2 belong to the same person as well as signals number 5 and 6 (Table 1). ECG signals were acquired at sampling frequency of 250 Hz using a BIOPAC data acquisition and measurement system (BIOPAC Systems, Inc., USA). To enable early detection of QRS complex we required an ECG lead, which results in a distinctive ascendant QR junction, high R wave amplitude and high dynamics within the QRS complex in comparison to other parts of the ECG signal. Typical standard ECG leads fulfilling these requirements include the chest lead V4 and standard limb leads I, II and III. We recorded ECG signals from leads I and III by placing the electrodes (disposable soft cloth ECG electrodes, diameter 6 cm, 3M™ Red Dot™) on wrists and ankles and computed the third limb lead II by summing the leads I and III. The lead with best dynamic characteristics was selected for the analysis individually for each patient (see Table 5).
2.2 Analysis of electrocardiograms
The primary analysis of ECG signals recorded during electrochemotherapy was made by using QRS detection algorithm based on the analysis of a single lead ECG, which enables EP pulse delivery prior to the vulnerable period of the heart [30]. This algorithm for synchronization of EP pulse delivery with ECG was developed and evaluated using records of the Long-term ST database (LTST DB database) [23] and was written in ANSI C programming language. The algorithm is described in detail elsewhere [30]. Briefly, it consists of two major components (the detection phase and the decision-making phase), which are preceded by the learning phase during which architecture parameters are estimated from the ECG signal. The detection phase is based on consideration of several ECG signal features: the QR interval, the R wave amplitude and the RR interval (see Fig. 1), in order to achieve a reliable QRS detector performance and to assure clear distinction between normal and abnormal individual heartbeats. For implementation of such a detector the peaks of Q and R waves and the isoelectric level are extracted from the ECG signal. During the decision-making phase, a decision is made whether the EP pulse can be delivered or not based on evaluating deviations of R wave amplitude and RR interval of individual heartbeat from moving average values of these two parameters.
Further analysis of ECG signals recorded during electrochemotherapy was performed to estimate the effect of EP pulse delivery on ECG. For this purpose the peaks of S waves and ends of QRS complexes were determined using program routines written in Matlab. Since the longest normal duration of the QRS complex is 120 ms [22] and the R peak is located approximately at the centre of the QRS complex, it is reasonable to expect the S peak within an interval of 60-ms after the R peak. The algorithm calculates the first derivative of the ECG signal in this 60 ms interval and looks for the first occurrence of three successive samples with negative first derivative followed by a sample with nonnegative derivative. The S peak is assigned to the third of these four samples. Next, the algorithm searches for the flattest part of the ST segment in order to determine the end of the QRS complex. For this purpose an interval of 40 ms after the S peak is analyzed. The average value of five successive samples from this interval having the minimal total deviation from their average value is taken as the flattest part of the ST segment and the middle sample is considered as the end of QRS complex, i.e., the end of QRS interval. After this, the area under the QRS complex is estimated. A similar routine is used for localization of the end of T wave except that an interval of 130 ms after the T peak is analyzed; the flattest part is searched for and the middle sample of this flattest part is considered as the end of T wave. The corrected QT interval (QTc interval) is calculated as the QT interval divided by the square root of the corresponding RR interval.
For evaluation of the effects of EP pulse delivery on functioning of the heart we calculated the average values of RR interval, QRS interval, QTc interval, QRS area and R wave amplitude before and after the application of EP pulses. The length of the averaging interval (8.5 s) was chosen based on the minimum interval between two successive applications of EP pulses, which was 8.5 s.
Testing and evaluation of this newly developed part of the algorithm was performed by manual verification of automatically defined locations of S peak, T peak, the end of T wave, and duration of QRS interval on randomly selected sequences of ECG signals included in our study. In addition, since this was the first application of the newly developed part algorithm, we also manually verified the results of the algorithm on 8.5 s-long segments of ECG signals before and after all 93 applications of EP pulses.
All ECG signals were manually examined by two medical doctors (including a cardiologist), who classified all abnormal heartbeats present in the signals. Other heartbeats were considered as normal. They found no evidence of significant long-lasting heart arrhythmias (e.g., bradycardia, tachycardia). For evaluation of QRS complex detection, we calculated the following scores for each record: N d , TP, FN and FP (for definitions see Table 5). Based on these scores obtained with a beat-by-beat comparison of the results of our algorithm [30] with the medical expert-defined annotations of the heartbeats, we calculated standard performance measures of the algorithm: the sensitivity (Se), the positive predictivity (+P) and the detection error rate (DER) for QRS detection (Eqs. 1–3, respectively). The performance measures for an ideal QRS detector would be Se = 100%, +P = 100% and DER = 0%.
For evaluation of EP pulse delivery we calculated the following scores for each record: N p , TP p , FN p and FP p (for definitions see Table 5). Based on these scores and in the absence of any standard performance metrics for EP pulse delivery, we calculated the performance measures analogous to QRS detection metrics: the sensitivity (Se p ), the positive predictivity (+P p ) and the delivery error rate (DER p ) for EP pulses. The performance measures for an ideal algorithm for EP pulse delivery would be Se p = 100%, +P p = 100% and DER p = 0%.
The performance of our algorithm for QRS detection and EP pulse delivery has previously been evaluated on ECG signals from a standard LTST DB database [30]. The results were: Se = 99.4%, +P = 100.0%, DER = 0.6%, Se p = 91.8%, +P p = 100.0% and DER p = 8.3% (median values).
2.3 Numerical modeling
We performed numerical calculations of electric field and current distribution for tissue models. The geometry of models and electrode configurations are shown in Fig. 2. The modeled conditions (needle row array, needle hexagonal array and plate electrode configurations and voltages applied) were the same as actually used in clinical electrochemotherapy (see Tables 3 and 4 for details). The modeled tissues (the target tumor tissue and the surrounding healthy tissue) are treated as isotropic materials with ohmic behavior (only conductivity of the tissues was taken into account). The assigned conductivity values were set to be 0.4 S/m for the tumor and 0.2 S/m for the healthy tissue according to previous measurements of tumor and tissue conductivity [34], models of subcutaneous tumor and skin electropermeabilization [43], a 3D finite element model of thorax, where the sensitivity of defibrillation parameters to the variations in model inhomogeneity and approximation of skeletal muscle anisotropy was examined for different paddle placements [9], and average conductivity of tissues composing the thorax [26]. The conductivity of cardiac muscle was reported to be in the range between 0.17 and 0.25 S/m [9, 26]. The assigned conductivity values for target tumor tissue (0.4 S/m) and the surrounding healthy tissue (0.2 S/m) describe the conductivity at the end of the electropermeabilization process, thus incorporating the changes to tissue conductivity due to exposure to external electric pulses.

The geometry of tissue models with tumor for: a plate electrodes (length 7 mm, thickness 0.7 mm, distance between the electrodes d is 4, 6 or 8 mm, tumor diameter is 1 mm larger than distance between the electrodes); b needle row array electrodes (diameter 0.7 mm for each needle, distance between two rows of electrodes d = 4 mm, tumor radius r = 4 mm, tumor location 0.5 mm under the skin surface); c needle hexagonal array electrodes (diameter 0.7 mm for each needle, distance between two electrodes 8 mm, tumor radius r = 15 mm)
The critical depth for electric field of 200 and 450 V/cm (value for reversible and irreversible electroporation of the muscle, respectively [43]), by solving the Laplace equation, and the critical depth for current of 100 mA (threshold for ventricular fibrillation for 500 μs-long electrical stimulus [46]), were estimated by means of finite element method using COMSOL Multiphysics 3.3 software package (COMSOL AB, Sweden). Of the total electric current flowing through the tissue during the EP pulse delivery, no more than 100 mA (the threshold value for fibrillation) is allowed to flow through the heart. Therefore we defined the critical depth as a distance from the surface of the body (at the site of EP delivery) below which the total electric current flowing is equal to this threshold value. This is a very conservative approach in which it is assumed that the entire current flowing below the critical depth actually passes through the heart. The validity of the model is further discussed in the Sect. 4.1.
2.4 Statistical analysis
The performance of the algorithm and average values of heartbeat parameters were compared using either the Mann–Whitney Rank Sum or Wilcoxon Signed Rank test. In all tests, a p value of less than 0.05 was considered as indication of statistically significant difference. The statistical analysis was performed using SigmaStat 3.1 software package. Since the data were not normally distributed, we give statistical summary of the results using both the mean/standard deviation and the median/quartile values. However, when we say “on average” in the text we are referring to median values, which are more representative of the middle of the sample and population than the mean values.
3 Results
3.1 The effect of electroporation pulse delivery on electrocardiogram
Our program-based analysis of heartbeat characteristics (RR interval, QRS interval, QTc interval, R wave and QRS area) revealed no pathological morphological changes caused by EP pulses in patients subjected to electrochemotherapy. This finding was confirmed independently by two medical doctors. The significant change, however, was detected in RR and QRS interval duration after each application of EP pulses (see Table 2).
The medical doctors involved in the study confirmed that EP pulses induced no heart arrhythmias. Moreover, additional premature heartbeats were not triggered by EP pulses in the cases where premature heartbeats were present in ECG signal before the application of EP pulses.
The results of modeling the distribution of electric field and current in tissue models are presented in Tables 3 and 4. It can be seen that in the worst-case scenario (needle hexagonal array electrodes, 10 mm depth of insertion) the critical depth for current of 100 mA is 4.10 cm. The largest critical depths for reversible and irreversible electroporation are 1.30 and 1.07 cm, respectively, for needle row array electrodes at insertion depth 10 mm.
3.2 The algorithm for synchronization of electroporation pulse delivery with electrocardiogram
The performance of the algorithm for QRS detection and synchronization of EP pulse delivery with ECG is summarized in Table 5. On average, the algorithm correctly detected 99.2% of all QRS complexes. The total number of erroneously detected QRS complexes was 15. On average, the algorithm would correctly deliver EP pulses in 94.6% of normal QRS complexes. The average positive predictivity for EP pulses (+P p ) was 100.0% and thus ideal.
A comparison of performance between 16 ECG signals recorded during electrochemotherapy and 42 ECG signals from the LTST DB database [30] was performed. The results showed that there is not a statistically significant difference in the median values between all compared performance measures (Se, +P, DER, Se p , DER p ) (0.142 < p < 0.924) except for the positive predictivity for EP pulse delivery (+P p ) (p = 0.026, Mann–Whitney Rank Sum test). This performance measure was significantly better for ECG signals recorded during electrochemotherapy than for ECG signals from LTST DB database.
4 Discussion
4.1 The effect of electroporation pulse delivery on electrocardiograms
We found no heart arrhythmias or other pathological morphological changes of heartbeat as a consequence of applied EP pulses. No additional premature heartbeats were triggered even in cases when these were present in ECG signal before the first application of EP pulses (signals number 11, 12 and 16). This is in agreement with the results of the work by Al-Khadra et al. [2] that showed no arrhythmias in association with electroporation applied directly on the heart. According to the heart strength-duration curve a very large current would be required to cause a single premature heartbeat [7, 15, 46] for very short EP pulse duration (the microsecond range). Since no additional premature heartbeats were detected, it is highly improbable that EP pulses alone could create the inhomogeneity (altered states of depolarization–repolarization), which is a requisite for onset of fibrillation.
The computer-based analysis demonstrated no significant statistical change in the QTc interval but a significant statistical decrease in the RR and QRS interval after each application of EP pulses (Table 2). This transient effect disappeared within 10 s after each application of EP pulses. The RR and QRS intervals are tightly correlated because they are both dependent on the heartbeat frequency [46]. A significant change in QT interval is one of the most important indicators of arrhythmias [4]. However, its value is also dependent on the heart rate (the faster the heart rate, the shorter the QT interval) and has to be adjusted to aid interpretation. For this reason the QTc interval is used in practice. A significant change in the QTc interval would indicate a clinically relevant effect of electrochemotherapy. However, no such effect was observed in our study (1.89 ms median change of QTc interval after application of EP pulses, see Table 2).
Several studies suggested that there is a link between negative emotions (e.g., anxiety) and the oscillations of RR interval [1, 16, 24, 32, 53, 56]. The most frequently reported symptoms in panic attacks, which are characterized by episodes of intense anxiety, are heart pounding and tachycardia [16, 32]. Another possible reason for RR interval decrease is intrinsic sympathetic activation of the nervous system, occurring in response to stress, exercise, or heart disease [1, 53]. The applications of electrochemotherapy to internal tumors could also directly affect the cardiac tissue if tumors were located close to the heart muscle. However, this effect is highly unlikely for current applications of electrochemotherapy because of relatively large distance between treated tumors and the heart (at least several centimeters) and due to small inter-electrode distances (8 mm or less). This assumption is further supported by the calculated critical depths for electric current threshold values discussed later in the text. Therefore, we suggest that the observed changes in RR interval can be largely if not completely attributed to anxiety and stress of the patient undergoing electrochemotherapy.
In our study almost one third (30.5%) of the 93 non-synchronized EP applications were delivered within the vulnerable period, which is in accordance with the fact that the duration of the vulnerable period is around one third of the duration of heart cycle [46]. The study of occurrence of ventricular fibrillation after atrial cardioversion performed with transthoracic electrodes pointed out that delivery of electric pulse, which was not synchronized with the R wave consistently resulted in ventricular fibrillation if the pulse was delivered within the T wave, the vulnerable period of the ventricles [5]. The probability for ventricular fibrillation was decreased but not eliminated with the arrival of synchronized defibrillators for cardioversion [5]. A high percentage of EP pulses delivered during the vulnerable period in our study, when EP application is not synchronized with ECG, underlines the importance of synchronization.
The values of electric field and current in the heart muscle during electroporation are important for evaluation of the danger for inducing ventricular fibrillation. For tissue models (Fig. 2) we estimated critical depths by calculating threshold value of electric field for reversible and irreversible electroporation of the muscle (200 and 450 V/cm, respectively [43]), and threshold value of current for ventricular fibrillation (100 mA for 500 μs-long stimulus [46]) (see Tables 3 and 4). In the study by Galvão et al. [17] they showed that the threshold current that stimulates the heart strongly depends on the age of the animal (i.e., old animals have lower threshold levels). Due to the relatively old patients included in our study (median value 70.8 years) we can therefore assume that the current threshold value is lowered. On the other hand, the EP pulses used in electrochemotherapy are much shorter (100 μs) and therefore the threshold value should in theory be approximately five times greater than for the 500 μs-long stimulus [15, 46]. Furthermore, amplitude threshold for fibrillation for pulsed direct currents is considerably higher than for alternating currents [46]. Currently we have no conclusive information regarding the influence of the repetition frequency of pulsed direct currents on the threshold for fibrillation. Therefore we adopted the threshold value of 100 mA as an estimate of true threshold value. For the needle row array and needle hexagonal array electrodes the critical depth depends on the depth of insertion. The results showed that for the plate electrodes with 8 mm distance between the electrodes the critical depth for threshold current was 2.38 cm (see Table 3). For needle row array and needle hexagonal array electrodes at depth of insertion of 10 mm, the critical depths for threshold current were 3.79 and 4.10 cm, respectively (see Table 4). The critical depth for threshold current for plate electrodes is smaller in comparison to the needle row array or needle hexagonal array electrodes because most of the voltage drop occurs on the skin [33].
With electrodes positioned distantly from the heart (e.g., on a single limb), as in the majority of EP pulse delivery cases (see Table 1), the current traversing the heart is negligible and therefore a smaller risk of accidental cardiac stimulation exists [44]. EP pulses frequently provoke strong and painful muscle contractions [57]. In contrast to the heart muscle, the motor neurons innervating the skeletal muscles, which are located in relative proximity to the electrodes, are always stimulated by EP pulses.
In electrochemotherapy applications included in our study, plate electrodes with distances between the electrodes of 6 and 8 mm and needle hexagonal array electrodes with small depths of insertion (2 or 3 mm) were used (see Table 1). The majority of the EP pulses were delivered on extremities and even when delivered on the trunk they were delivered distantly from the heart. However, two applications of EP pulses were delivered on the chest relatively close to the heart (distance approximately 5 cm) with plate electrodes. Since the heart lies at least 3 cm beneath the skin surface [54], for the applications involved in our study the results of modeling indicated that it is highly unlikely that EP pulses even when applied on the trunk directly above the heart could affect functioning of the heart (critical depths 2.23 and 2.38 cm for needle hexagonal array and plate electrodes, respectively). Furthermore, the most vulnerable part of the heart, the apex, lies behind the breast and is thus additionally protected from the external stimulation by breast tissue. Additionally, if the electrodes were located above sternum or above a rib, the risk of affecting the heart would be further reduced due to low conductivity of bones (range from 0.01 to 0.06 S/m) [34] and larger dimension of sternum and ribs in comparison to the distance between the electrodes. However, if the electrodes were not located directly above the sternum or a rib, the critical depths would be larger due to higher conductivity of the underlying tissues. In this case according to the results of modeling there exists a theoretical chance to affect the functioning of the heart in case of deep insertion of either needle hexagonal or row array electrodes (approximately 4 cm for both types of electrodes at insertion depth of 10 mm). This should be considered in future applications of electrochemotherapy.
For the modeled tissues only the conductivity was taken into account. The capacitive behavior of the tissues was neglected since the transient effects are present only during the charging time of the cell membrane, which lasts around 1 μs [39]. The membrane charging time is much shorter compared to the EP pulse duration used in electrochemotherapy. It was also shown in several studies that static analysis of the electric field distribution during electroporation without taking into account the transient effects are adequate [43, 49, 50], since after the transient effect the tissue exhibits only ohmic behavior [13]. Using current-voltage measurements on cells in vitro [42] or tissues in vivo [13] it was shown that electroporation occurs after the transient time and that the dynamic behavior at the start of the pulses (that includes capacitive behavior of the tissue) is not crucial for the process of electroporation. On the other hand, this transient effect induces a rapid initial current increase followed by an exponential decrease and a constant level. The applied current during electrochemotherapy is limited to 16 A. Since the transient effect lasts only 1 μs and according to the heart strength-duration curve it is very unlikely that the transient part of an EP pulse could induce ventricular fibrillation [7, 15, 46].
Since the electrode dimensions (electrode–tissue contact surface area) and distance between electrodes used in electrochemotherapy for tumors analyzed in our study are significantly smaller compared to the electrode dimensions and positions used for cardiac defibrillation, we can assume that the differences in thorax tissues conductivities should not change the electric field and current distribution calculated with our numerical models. Therefore, based on the previous studies [9, 26, 34, 43] we can conclude that our numerical models with chosen electrical properties can be used for the evaluation (rough estimate) of critical electric field and current for protruding cutaneous tumors or subcutaneous tumors, which are located immediately under the skin surface (0.5 mm under the skin surface in our study). However, for more deeply located tumors the exact conductivities of all tissues should be incorporated in the numerical model of the thorax.
Recently a new method of local and drug-free tissue ablation called irreversible electroporation has been developed for clinical use as a promising approach to solid tumor therapy [3, 14, 35], prostate ablation [41] and cardiac tissue ablation [28]. In these studies EP pulses with larger amplitudes (up to 3,000 V [11]) and longer durations (range from 100 to 24 ms) are used. The application of EP pulses during irreversible electroporation is therefore more likely to influence functioning of the heart than EP pulses usually applied in electrochemotherapy. However, the results of a recent study by Lavee et al. [28] using irreversible electroporation for epicardial atrial ablation for the treatment of atrial fibrillation showed that ablation pulses (amplitudes of 1,500–2,000 V, duration 100 μs, frequency 5 Hz) caused no permanent arrhythmia or any other rhythm disturbance apart from the rapid atrial pacing during the pulse sequence application. The immediate resumption of sinus rhythm following the ablation was recorded. Similarly, the results of study by Al-Khadra et al. [2] demonstrated lack of any evidence of spontaneous arrhythmias (reentrant or focal) associated with electroporation of the endocardium or the papillary muscles. In their study they presented experimental evidence suggesting that electroporation might even transiently reduce myocardial vulnerability to arrhythmias. But on the other hand, they pointed out that electric pulses of high energy are known to produce a permanent damage, perhaps associated with electroporation. This effect of electroporation may provide a substrate for arrhythmogenesis [2]. Our results of modeling showed that the critical depths for irreversible electroporation of the muscle/heart (450 V/cm) are 1.07 and 0.93 cm for needle row array and needle hexagonal array electrodes, respectively, at insertion depth 10 mm (Table 3). The critical depth for the plate electrodes is smaller (0.30 cm for 8 mm distance between the electrodes). Since the heart lies at least 3 cm beneath the skin surface [54], for the applications involved in our study the results of modeling indicated that it is impossible to affect functioning of the heart by irreversible electroporation even when EP pulses were applied on the trunk directly above the heart. That would not be the case for electrochemotherapy treatment of internal tumors located close to the heart muscle.
Considering these facts, it is nevertheless advisable to incorporate synchronization of EP pulse delivery with ECG in medical equipment for electroporation in order to maximize safety of the patients especially in future clinical applications. Synchronization of EP pulse delivery with the refractory period of the cardiac cycle is always advisable whenever there is a possibility of EP pulses influencing the functioning of the heart.
4.2 The algorithm for synchronization of electroporation pulse delivery with electrocardiogram
The algorithm for QRS detection and EP pulse delivery reliably detected QRS complexes in all signals recorded during electrochemotherapy (see Table 5). The algorithm would allow for EP pulse delivery only for correctly identified heartbeats with no abnormalities. The performance of our algorithm for QRS detection is similar to that of some other detectors with comparably simple algorithms [6, 47]. The algorithm performed poorly (large DER, marked with # in Table 5) for ECG signals with either very unstable R wave amplitudes or RR intervals, or heavy contamination with high-frequency noise with amplitudes similar to R wave, or presence of premature heartbeats not satisfying the dynamic requirements within the QRS complex [12, 29]. In total we found 15 false positive detections (FP), which were caused by the occurrence of transient noise having the morphology and the time of appearance so similar to a normal QRS complex that the algorithm could not distinguish them. Many of the false negative detections (FN) were due to our self-imposed strict requirements for as few as possible false positive detections (FP).
The most appropriate time for EP pulse delivery is before the onset of the vulnerable period since the vulnerable period can sometimes be prolonged (e.g., after premature heartbeat) [46]. Thus delivery of EP pulses immediately after the R wave detection but within the QRS complex is the most reasonable. The delivery of EP pulses during the vulnerable period of the atria does not present a serious threat for the patient’s life. The hemodynamic effects of atrial flutter and fibrillation, which could be potentially caused by EP pulses during the vulnerable period of the atria, are slim and patients are frequently unaware of them [46]. The time reserve for safe EP pulse delivery after the R wave detection and before the onset of the vulnerable period of the ventricles is approximately 60 ms. This time reserve is long enough for safe EP pulse delivery by plate or needle row electrodes and even avoids the vulnerable period of the atria. The requirement for avoiding the delivery of EP pulses at the moments of potential danger for the patient would be fulfilled excellently as indicated by the ideal +P p values for all ECG signals (see Table 5). However, when using hexagonal electrodes the synchronization becomes irrelevant due to 200 ms-long EP pulse sequence which extends into the vulnerable period of the atria and ventricles. Therefore, a modification of the existing EP pulse delivery protocol for hexagonal electrodes would be needed for safer application in the immediate vicinity of the heart. The suggested solution is to delay the delivery of EP pulses by approximately one half of the current RR interval, which would result in EP pulses being delivered after the vulnerable period provided that the following heartbeat was normal. However, delayed EP pulses would be delivered exactly within the vulnerable period in case of the appearance of premature heartbeat. The other possibility is to synchronize the switching between the electrodes and partial pulse delivery with ECG.
The statistical comparison of performance of the algorithm between ECG signals recorded during electrochemotherapy and ECG signals from the LTST DB database [30] generally showed no statistically significant differences except for positive predictivity for EP pulse delivery (+P p ). This performance measure was significantly better for ECG signals recorded during electrochemotherapy than for ECG signals from LTST DB database thus showing that the algorithm was developed for worser conditions than encountered during clinical application of electroporation. In spite of numerous arrhythmias in some ECG signals from the LTST DB database the algorithm performed excellently [30]. The clinical electrochemotherapy was so far indicated only for patients without clinically significant or severe heart disease, which reflects in ideal value +P p = 100% in all ECG signals recorded during electrochemotherapy. However, mostly old patients are included in electrochemotherapy treatment nowadays because of the emerging need for palliative treatment of tumors with electrochemotherapy. With the increasing age of the patients, the probability for encountering pathological ECG is also increasing, therefore, the synchronization of EP pulse delivery with ECG would maximize safety of the patient.
5 Conclusions
Currently used electroporation protocols could interfere with functioning of the heart although no such practical evidence exists till now. Because no systematic study regarding this topic has been done yet, we examined in our study the effects of EP pulses on functioning of the heart. We measured ECG signals during electrochemotherapy and analyzed their characteristics. We found no arrhythmias or other pathological morphological changes due to application of EP pulses. The only demonstrated effect of EP pulses on ECG is a transient RR interval decrease. The facts contributing to a belief that EP pulse delivery during electrochemotherapy cannot affect functioning of the heart are: short EP pulse duration, use of direct current, application mainly on locations relatively distant from the heart (i.e., on extremities), and small inter-electrode distance. On the other hand, there are some open issues regarding electrochemotherapy that need to be considered, for example: EP pulses delivered by plate or needle row electrodes that are not synchronized with ECG could be delivered within the vulnerable period, EP pulses delivered by hexagonal electrodes mainly coincide within the vulnerable period, the threshold levels of the heart for elderly patients are lowered, possible use of electrochemotherapy on patients with clinically significant heart disease, new applications with longer durations and/or higher amplitudes of EP pulses as well as applications involving endoscopic or surgical means to access internal tumors are being developed. Even though no practical evidence for electroporation having an effect on functioning of the heart has been observed so far, we can still maximize safety of the patients by incorporating the algorithm for synchronization of EP pulse delivery with ECG in medical equipment for EP pulse delivery. The usual application of eight EP pulses with duration 100 μs each can benefit from synchronizing delivery of EP pulses with electrocardiogram but this is not the case for hexagonal electrodes or combination of high- and low-voltage EP pulses and pulses with higher amplitudes as used in tumor tissue ablation by irreversible electroporation.
References
Acharya UR, Joseph KP, Kannathal N, Lim CM, Suri JS (2006) Heart rate variability: a review. Med Biol Eng Comput 44:1031–1051
Al-Khadra A, Nikolski V, Efimov IR (2000) The role of electroporation in the fibrillation. Circ Res 87:797–804
Al-Sakere B, Bernat C, André F, Connault E, Opolon P, Davalos RV, Mir LM (2007) A study of the immunological response to tumor ablation with irreversible electroporation. Technol Cancer Res Treat 6:301–305
Anderson ME (2006) QT interval prolongation and arrhythmia: an unbreakable connection? J Intern Med 259:81–90
Ayers GM, Alferness CA, Ilina M, Wagner DO, Sirokman WA, Adams JM, Griffin JC (1994) Ventricular proarrhythmic effects of ventricular cycle length and shock strength in a sheep model of transvenous atrial defibrillation. Circulation 89:413–422
Benitez DS, Gaydecki PA, Zaidi A, Fitzpatrick AP, Laguna P (2000) A new QRS detection algorithm based on the Hilbert transform. IEEE Comput Cardiol 27:379–382
Bruner JMR, Leonard PF (1989) Electricity, safety, and the patient. Year Book Medical Publishers, Inc., Chicago
Bureau MF, Gehl J, Deleuze V, Mir LM, Scherman D (2000) Importance of association between permeabilization and electrophoretic forces for intramuscular DNA electrotransfer. Biochim Biophys Acta 1474:353–359
Camacho MA, Lehr JL, Eisenberg SR (1995) A three-dimensional finite element model of human transthoracic defibrillation: paddle placement and size. IEEE Trans Biomed Eng 42:572–578
Chen C, Smye SW, Robinson MP, Evans JA (2006) Membrane electroporation theories: a review. Med Biol Eng Comput 44:5–14
Clayton RH, Holden AV (2000) Re-entry in computational models of heterogenous and abnormal myocardium. Int J Bioelectromagn, available online: http://www.rgi.tut.fi/ijbem/volume2/number2/clayton/paper_ijbem.htm
Cuesta-Frau D, Biagetti MO, Quinteiro RA, Micó-Tormos P, Aboy M (2007) Unsupervised classification of ventricular extrasystoles using bounded clustering algorithms and morphology matching. Med Biol Eng Comput 45:229–239
Cukjati D, Batiuskaite D, André F, Miklavcic D, Mir LM (2007) Real time electroporation control for accurate and safe in vivo non-viral gene therapy. Bioelectrochemistry 70:501–507
Davalos RV, Mir LM, Rubinsky B (2005) Tissue ablation with irreversible electroporation. Ann Biomed Eng 33:223–231
Fish RM, Geddes LA, Babbs CF (2003) Medical and bioengineering aspects of electrical injuries. Lawyers and Judges Publishing Company, Arizona
Friedman BH, Thayer JF (1998) Autonomic balance revisited: panic anxiety and heart rate variability. J Psychosom Res 44:133–151
Galvão KM, Mateus EF, Gomes PAP (2001) Electric stimulation of isolated hearts: age dependance of the threshold electric field. Memorias II Congreso Latinoamericano de Ingeniería Biomédica 950-7132-57-5 (c)
Heller R, Jaroszeski M, Atkin A, Moradpour D, Gilbert R, Wands J, Nicolau C (1996) In vivo gene electroinjection and expression in rat liver. FEBS Lett 389:225–228
Heller R, Jaroszeski MJ, Reintgen DS, Puleo CA, DeConti RC, Gilbert RA, Glass LF (1998) Treatment of cutaneous and subcutaneous tumors with electrochemotherapy using intralesional bleomycin. Cancer 83:148–157
Heller LC, Heller R (2006) In vivo electroporation for gene therapy: review. Hum Gene Ther 17:890–897
Hofmann GA (2000) Instrumentation and electrodes for in vivo electroporation. In: Jaroszeski MJ, Heller R, Gilbert R (eds) Electrochemotherapy, electrogenetherapy, and transdermal drug delivery: electrically mediated delivery of molecules to cells. Humana, Totowa
Houghton AR, Gray D (1997) Making sense of the ECG: a hands-on guide. Arnold, London
Jager F, Taddei A, Moody GB, Emdin M, Antolic G, Dorn R, Smrdel A, Marchesi C, Mark RG (2003) Long-term ST database: a reference for the development and evaluation of automated ischaemia detectors and for the study of the dynamics of myocardial ischaemia. Med Biol Eng Comput 41:172–182
Johnsen BH, Thayer JF, Laberg JC, Wormnes B, Raadal M, Skaret E, Kvale G, Berg E (2003) Attentional and physiological characteristics of patients with dental anxiety. J Anxiety Disord 17:75–87
Jones M, Geddes LA (1977) Strength-duration curves for cardiac pacemaking and ventricular fibrillation. Cardiovasc Res Cent Bull 15:101–112
Karlon WJ, Lehr JL, Eisenberg SR (1994) Finite element models of thoracic conductive anatomy: sensitivity to changes in inhomogeneity and anisotropy. IEEE Trans Biomed Eng 41:1010–1017
Kirchhof PF, Fabritz CL, Zabel M, Franz MR (1996) The vulnerable period for low and high energy T-wave shocks: role of dispersion of repolarization and effect of d-sotalol. Cardiovasc Res 31:953–962
Lavee J, Onik G, Mikus P, Rubinsky B (2007) A novel nonthermal energy source for surgical epicardial atrial ablation: irreversible electroporation. Heart Surg Forum 10:96–101
Lin CH (2006) Classification enhancible grey relational analysis for cardiac arrhythmias discrimination. Med Biol Eng Comput 44:311–320
Mali B, Jarm T, Jager F, Miklavcic D (2005) An algorithm for synchronization of in vivo electroporation with ECG. J Med Eng Technol 29:288–296
Marty M, Sersa G, Garbay JR, Gehl J, Collins CG, Snoj M, Billard V, Geertsen PF, Larkin JO, Miklavcic D, Pavlovic I, Paulin-Kosir SM, Cemazar M, Morsli N, Soden DM, Rudolf Z, Robert C, O’Sullivan GC, Mir LM (2006) Electrochemotherapy—an easy, highly effective and safe treatment of cutaneous and subcutaneous metastases: results of ESOPE (European Standard Operating Procedures of Electrochemotherapy) study. Eur J Cancer Suppl 4:3–13
McCraty R, Atkinson M, Tomasino D, Stuppy WP (2001) Analysis of twenty-four hour heart rate variability in patients with panic disorder. Biol Psychol 56:131–150
Miklavcic D, Corovic S, Pucihar G, Pavselj N (2006) Importance of tumour coverage by sufficiently high local electric field for effective electrochemotherapy. Eur J Cancer Suppl 4:45–51
Miklavcic D, Pavselj N, Hart FX (2006) Electric properties of tissues. In: Wiley encyclopedia of biomedical engineering. Wiley, New York
Miller L, Leor J, Rubinsky B (2005) Cancer cells ablation with irreversible electroporation. Technol Cancer Res Treat 4:1–7
Mir LM, Glass LF, Sersa G, Teissie J, Domenge C, Miklavcic D, Jaroszeski MJ, Orlowski S, Reintgen DS, Rudolf Z, Belehradek M, Gilbert R, Rols MP, Belehradek J Jr, Bachaud JM, DeConti R, Stabuc B, Cemazar M, Coninx P, Heller R (1998) Effective treatment of cutaneous and subcutaneous malignant tumors by electrochemotherapy. Br J Cancer 77:2336–2342
Mir LM, Orlowski S (1999) Mechanisms of electrochemotherapy. Adv Drug Deliv Rev 35:107–118
Neumann E, Schaefer-Ridder M, Wang Y, Hofschneider PH (1982) Gene transfer into mouse lyoma cells by electroporation in high electric fields. EMBO J 1:841–845
Neumann E, Sowers AE, Jordan CA (1989) Electroporation and electrofusion in cell biology. Plenum Press, New York
Niu G, Heller R, Catlett-Falcone R, Coppola D, Jaroszeski M, Dalton W, Jove R, Yu H (1999) Gene therapy with dominant-negative Stat3 suppresses growth of the murine melanoma B16 tumor in vivo. Cancer Res 59:5059–5063
Onik G, Mikus P, Rubinsky B (2007) Irreversible electroporation: implications for prostate ablation. Technol Cancer Res Treat 6:295–300
Pavlin M, Kanduser M, Rebersek M, Pucihar G, Hart FX, Magjarevic R, Miklavcic D (2005) Effect of cell electroporation on the conductivity of a cell suspension. Biophys J 88:4378–4390
Pavselj N, Bregar Z, Cukjati D, Batiuskaite D, Mir LM, Miklavcic D (2005) The course of tissue permeabilization studied on a mathematical model of a subcutaneous tumour in small animals. IEEE Trans Biomed Eng 52:1373–1381
Prausnitz MR (1996) The effects of electric current applied to skin: a review for transdermal drug delivery. Adv Drug Deliv Rev 18:395–425
Rebersek M, Faurie C, Kanduser M, Corovic S, Teissié J, Rols MP, Miklavcic D (2007) Electroporator with automatic change of electric field direction improves gene electrotransfer in vitro. Biomed Eng Online 6:25
Reilly JP (1998) Applied bioelectricity: from electrical stimulation to electropathology. Springer, New York
Ruha A, Sallinen S, Nissilä S (1997) A real-time microprocessor QRS detector system with a 1-ms timing accuracy for the measurement of ambulatory HRV. IEEE Trans Biomed Eng 44:159–167
Satkauskas S, Bureau MF, Puc M, Mahfoudi A, Scherman D, Miklavcic D, Mir LM (2002) Mechanisms of in vivo DNA electrotransfer: respective contributions of cell electropermeabilization and DNA electrophoresis. Mol Ther 5:133–140
Sel D, Macek Lebar A, Miklavcic D (2007) Feasibility of employing model-based optimization of pulse amplitude and electrode distance for effective tumor electropermeabilization. IEEE Trans Biomed Eng 54:773–781
Sel D, Cukjati D, Batiuskaite D, Slivnik T, Mir LM, Miklavcic D (2005) Sequential finite element model of tissue electropermeabilization. IEEE Trans Biomed Eng 52:816–827
Sersa G, Cufer T, Cemazar M, Miklavcic D, Rebersek M, Rudolf Z (2000) Electrochemotherapy with bleomycin in the treatment of hypernephroma metastasis: case report and literature review. Tumori 86:163–165
Sersa G (2006) The state-of-the-art of electrochemotherapy before the ESOPE study; advantages and clinical uses. Eur J Cancer Suppl 4:52–59
Task Force of the European Society of Cardiology, the North American Society of Pacing and Electrophysiology (1996) Heart rate variability: standards of measurement, physiological interpretation, and clinical use. Eur Heart J 17:354–381
The visible human project. National Library of Medicine, United States, online: http://www.nlm.nih.gov/research/visible/visible_human.html
Wiggers CJ, Wégria R (1940) Ventricular fibrillation due to single, localized induction and condenser shocks applied during the vulnerable phase of ventricular systole. Am J Physiol 128:500–505
Yeragani VK, Balon R, Pohl R, Ramesh C, Glitz D, Weinberg P, Merlos B (1990) Decreased R-R variance in panic disorder patients. Acta Psychiatr Scand 81:554–559
Zupanic A, Ribaric S, Miklavcic D (2007) Increasing the repetition frequency of electric pulse delivery reduces unpleasant sensations that occur in electrochemotherapy. Neoplasma 54:246–250
Acknowledgments
The research was supported by fifth EU Framework Programme projects (CLINIPORATOR QLK3-CT-1999-00484 and ESOPE QLK3-2002-02003) and by various grants from the Research Agency of the Republic of Slovenia.
Open Access
This article is distributed under the terms of the Creative Commons Attribution Noncommercial License which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License (https://creativecommons.org/licenses/by-nc/2.0), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Mali, B., Jarm, T., Corovic, S. et al. The effect of electroporation pulses on functioning of the heart. Med Biol Eng Comput 46, 745–757 (2008). https://doi.org/10.1007/s11517-008-0346-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11517-008-0346-7