
Abstract
Among studies conceptualizing quality of life (QoL) as the subjective measure of one’s well-being, evidence suggests a link between cognitive impairment and diminished quality of life. However, the direction of the association is not clear, and most studies have employed a global measure of cognition, which can mask subtle domain-specific declines. In this study, we aim at examining the longitudinal associations between memory and QoL in a representative sample of adults and older adults in Europe and Israel, employing data from the Survey of Health, Ageing and Retirement in Europe (SHARE). The sample was composed by 56,616 respondents aged 50 or older at the beginning of the study period. A Parallel-Process Latent Growth Model (PP LGM) of memory and QoL conditioned on the effects of age, gender, educational level, physical inactivity, depressive symptomatology and social activity participation, was tested. Results displayed a trajectory of decline for both memory and QoL, with higher initial levels of memory associated with higher initial levels of QoL, and steeper decline in memory associated with steeper decline in QoL. Moreover, a positive effect of initial memory onto QoL trend over time was found, indicating that better memory is associated to better QoL in the future, but the opposite did not occur. Results also provide evidence of gender differences. All in all, this work found evidence supporting the longitudinal effect of memory on QoL, which may have consequences for intervention implementation, given that actions for alleviating age-related memory impairment could also have a positive impact onto older adults’ QoL.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Aging of the population is the result of higher life expectancies and lower birth rates (Tavares, 2022; Weber & Loichinger 2022). Increments in life expectancy are partially due to improvements in treatment of communicable diseases and, consequently, chronic diseases have become the main cause of death among developed countries (McCracken & Phillips, 2017). Dementia in particular is among the top 10 causes of death globally (WHO, 2022), which highlights the importance of the study of cognition in old age.
Some studies (Bárrios et al., 2013; Hoe et al., 2009; Lawson et al., 2014, 2016; Maki et al., 2014) point towards a link between cognitive impairment and quality of life (QoL). However, the lack of consensus on the definition of QoL (Noll, 2021) has given rise to different operationalizations of the construct, which hinders the comparison of results across different studies. Namely, the World Health Organization (WHO) offered a definition of QoL as “individuals’ perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns” (WHOQOL Group, 1995, p. 1405). Nonetheless, as argued by Karimi and Brazier (2016), some studies have operationalized QoL as “health-related quality of life” (HRQoL), which corresponds to an operationalization of self-perceived health and therefore interferes with the understanding of QoL as the subjective measure of one’s well-being comprising the physical, psychological, social and spiritual dimensions defined by the WHO.
The assessment of QoL among individuals with advanced cognitive impairment poses a problem in its own (Bárrios et al., 2013; Bowling et al., 2015). Nevertheless, studies have generally found diminished levels of QoL among individuals with Mild Cognitive Impairment (MCI; Bárrios et al., 2013; Lawson et al., 2014; Lawson et al., 2016; Maki et al., 2014), and individuals with dementia (Ernecoff et al., 2019; Hoe et al., 2009; Marventano et al., 2015; Van der Zon et al., 2018), either using a self-report measure of QoL or a proxy measure.
Across studies examining cognition and QoL in healthy older adults, results also support a positive relationship between both (Godin et al., 2019; Wilson et al., 2013). Namely, Godin et al. (2019) showed that increases in cognitive impairment were associated to lower QoL at follow-up, after controlling for baseline cognition and QoL, as well as for sociodemographic characteristics. In its part, Wilson et al. (2013) tested the longitudinal effects of cognition onto the sense of purpose in life and found bidirectional effects both using a measure of global cognition and other domain-specific measures of memory and executive function. Other studies have consistently found greater subjective cognitive impairment (SCI) to be related to lower QoL (Hill et al., 2017; Stites et al., 2018).
Be that as it may, previous studies generally employed a global measure of cognition or different measures combined. According to Steinerman et al. (2010), using a global measure of cognition may mask normative age-related declines of cognition. Therefore, a domain-specific decline in cognition and its effect onto QoL may be already evident in healthy individuals with normative cognitive aging. In the same line, Wilson et al. (2013) argued that the specific cognitive domains of memory and executive function are critical to cognitive-demanding evaluations of one’s life and could underlie declines in QoL. The problem of QoL self-assessment when cognitive ability is compromised has also been raised by Bárrios et al. (2013) and Bowling et al. (2015), among others.
Among the different cognitive functions, impairment in the memory domain becomes especially relevant, as it can be considered an early manifestation of dementia (Ding et al., 2019; Mowrey et al., 2016). In addition, several studies (Bertola et al., 2019; Fernández et al., 2024; Johnson et al., 2012; Liampas et al., 2022; Yam et al., 2014) have documented normative age-related declines in memory among healthy older adults. Given that declines in memory are normative of the aging process, analysing the longitudinal associations of this cognitive domain and QoL among healthy adults and older adults can help untangle the nature of the association. Namely, results from studies using clinical samples (Bárrios et al., 2013; Ernecoff et al., 2019; Hoe et al., 2009; Lawson et al., 2014; Lawson et al., 2016; Maki et al., 2014; Marventano et al., 2015; Van der Zon et al., 2018) may be distorted because individuals’ ability to make assessments of their own life is compromised. Previous studies using samples of healthy older adults did not consider domain-specific measures of cognition (Godin et al., 2019) or did not employ a culturally and socioeconomically diverse sample (Wilson et al., 2013).
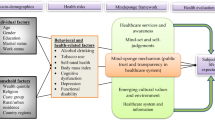
In this study, we aim at examining the longitudinal associations between memory and both general and domain-specific QoL in a representative sample of adults and older adults in Europe. Moreover, we will test the effects of several covariates known to be related to memory, QoL, or both. The considered covariates are age, gender, education, physical activity, depressive symptomatology, and social activity participation. Education will be employed as a marker of cognitive reserve (Stern, 2002), physical activity will be used to control for physical functioning (Wilson et al., 2013), depressive symptomatology will be used to control for affective functioning (Wilson et al., 2013), and social activity participation will be used to control for cognitive enrichment potential (Scarmeas & Stern, 2003).
Method
Sample and Procedure
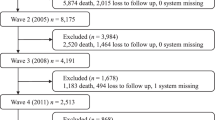
Data from the Survey of Health, Aging and Retirement in Europe (SHARE; Börsch-Supan et al., 2013) was employed in this study. SHARE is a longitudinal panel study that currently has eight waves of data since the beginning of the project in 2004. The study is targeted at individuals aged 50 and over and their partners, regardless of their age. At each bi-annual wave, the baseline sample and the refreshment sample are interviewed about a variety of topics on health, retirement, income, healthcare and social networks. Wave 3 is an exception, in which a retrospective interview, instead of the usual one, was done (Schröder, 2011), and therefore was not included in this study. In this study, data from SHARE waves 4 (Börsch-Supan, 2022a), 5 (Börsch-Supan, 2022b), 6 (Börsch-Supan, 2022c), 7 (Börsch-Supan, 2022d) and 8 (Börsch-Supan, 2022e), collected during years 2011/12, 2013, 2015, 2017 and 2019/20, respectively, were used.
The final sample was composed by all individuals that participated in the fourth wave of SHARE and that were aged 50 or older at that moment. We used data from these participants at each wave considered in the study. This yielded a sample size of 56,616 respondents. From these, 56.0% were women and 44.0% were men. At wave 4, their age ranged between 50 and 103 years, with an average of 65.93 years (SD = 10.01). There were 16 European countries represented in the data: Austria (8.8%), Germany (2.8%), Sweden (3.5%), Netherlands (4.9%), Spain (6.4%), Italy (6.2%), France (10.0%), Denmark (3.9%), Switzerland (6.5%), Belgium (9.1%), Czech Republic (9.5%), Poland (3.0%), Hungary (5.3%), Portugal (3.4%), Slovenia (4.8%) and Estonia (11.9%).
Instruments
Memory was measured using the 10-Word Recall Test, in which respondents were asked to remember a list of 10 words immediately (immediate recall) and 10 min after having them read (delayed recall). They were instructed to say, in any order, as many words as they could recall. The number of correctly evoked words in the immediate trial was employed as a marker of memory.
QoL measurement was done with a modified version of the CASP-19 (Hyde et al., 2003), the CASP-12. This scale has 12 items that cover four dimensions (control, autonomy, self-realization and pleasure), three tapping each. Items are answered on a 4-point Likert scale, ranging from 1 “never” to 4 “often”. The study by Oliver et al. (2021) provided evidence of adequate psychometric properties of the shortened 12-item version of CASP using SHARE data.
Other measures included as covariates in the model were age, gender, educational attainment, physical inactivity, depressive symptomatology and social activity participation.
Educational attainment was recorded using the International Standard Classification of Education-1997 (ISCED-1997; Schneider, 2008), according to which seven levels of education are considered: level 0 “Pre-primary education”, level 1 “First stage of basic education”, level 2 “Second stage of basic education”, level 3 “Upper secondary education”, level 4 “Post-secondary non-tertiary education”, level 5 “First stage of tertiary education”, and level 6 “Second level of tertiary education”.
Physical inactivity was considered as a binary indicator assessed as 1 when the individual reported less than weekly engagement in moderate physical activity, and considered 0 otherwise.
Depressive symptomatology was assessed employing the EURO-D (Prince et al., 1999). This scale covers 12 different symptoms of depression within the last month: depressed mood, pessimism, suicidality, guilt, sleep, lack of interest, irritability, loss of appetite, fatigue, lack of concentration, lack of enjoyment and tearfulness. One point is given for each symptom reported by the individual. Adequacy of the psychometric properties of this scale in the SHARE context was recently reported by Tomás et al. (2022).
Finally, social activity participation was assessed as the sum of participation in four different social activities within the last year. These activities were voluntary/charity work, educational/training courses, sport/social/other clubs, and political/community-related organization. Information regarding evidence of the psychometric properties of instruments employed to obtain composite scores in the study are available in the Appendix.
Statistical Analyses
First, descriptive statistics were computed for memory and QoL at each time point, as well as for the covariates, measured at the first time point. After that, Latent Growth Modelling (LGM) was used to study the relationships among memory and QoL over time. More concretely, a Parallel-Process Latent Growth Model (PP-LGM) with linear trends was specified and tested using Robust Maximum Likelihood (MLR). Once the unconditional (no covariates) model was fitted, a conditional model controlling for the effects of age, gender, educational level, physical inactivity, depressive symptomatology and social activity participation was further specified. This was done for the general factor of QoL as well as for the QoL domains contemplated in the CASP-12 (control, autonomy, self-realization and pleasure).
Model fit was assessed using the recommended fit indexes (Kline, 2016): the chi-square statistic, the Comparative Fit Index (CFI), the Root Mean Squared Error of Approximation (RMSEA), the Standardized Root Mean Square Residual (SRMR), as measures of absolute fit, and the Akaike’s Information Criterion (AIC) and the Bayesian Information Criterion (BIC), as measures of relative fit. In general, model fit is considered adequate with CFI values of at least 0.90 and RMSEA/SRMR values of 0.08 or less (Hu & Bentler, 1999). AIC and BIC are used for model comparisons, with lower values of these indexes indicating better relative fit of this model against another alternative model. Regarding missing data handling, Full Information Maximum Likelihood (FIML) was employed, given that this method outperforms traditional techniques for missing mechanisms that are Missing at Random (MAR) or Missing Completely at Random (MCAR). FIML produces parameter estimates using the value that maximizes the likelihood function based on available data only, rather than imputing data values for missing data-points (Enders, 2010). Analyses were performed using MPlus 8.9 (Muthén & Muthén, 1998–2017).
Results
Memory and General QoL
Descriptive statistics are available in Table 1. The PP-LGM of memory and QoL with no covariates yielded the following results of fit: χ2 (42) = 1227.94, p < .001, CFI = 0.989, RMSEA = 0.023 [0.022 – 0.024], SRMR = 0.032, AIC = 1674025.33, BIC = 1674239.73. As this model displayed optimal fit to the data, a second model considering the aforementioned covariates was tested. This model is graphically represented in Fig. 1. Fit of the conditional PP-LGM was also deemed adequate: χ2 (77) = 1856.38, p < .001, CFI = 0.989, RMSEA = 0.021 [0.020 – 0.022], SRMR = 0.020, AIC = 1553792.74, BIC = 1554219.06.

Parallel-Process Latent Growth Model of memory and quality of life with covariates. Note I= Intercept; S= Slope; M= Memory; QoL= Quality of life; W = Wave
This model presented an intercept of memory with an average value of 5.23 (p < .001) and a variance of 1.85 (p < .001). The results indicated a decline in memory over time, with a statistically significant and negative mean slope (M= -0.08, p < .001) and statistically significant variance of 0.05 (p < .001). Statistically significant variances of the intercept and the slope of memory indicate that there is inter-individual variability in terms of the initial memory level and the rate of change.
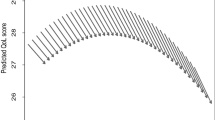
In the case of QoL, the average value of the intercept was 37.08 (p < .001) with a variance of 29.12 (p < .001). For the slope, this was also statistically significant and negative, with a mean value of -0.09 (p < .001) and a variance of 0.94 (p < .001). Therefore, inter-individual variability is also observed in initial levels of QoL as well as on the rate of decline of QoL over time.
Turning to the standardized effects of the covariates onto memory and QoL, these are displayed in Table 2. All covariates presented statistically significant effects onto the intercepts of memory and QoL in the expected direction. In addition, age, gender and depression also exerted an effect on the slopes of memory and QoL. For memory specifically, education further affected its slope. For the slope of QoL, education did not present statistically significant effects but physical inactivity did. Finally, social participation did not present statistically significant effects in any of the latent slopes.
Regarding the associations among the latent intercepts and slopes of memory and QoL, both intercepts present a statistically significant and positive correlation (r = .190, p < .001), indicating that higher initial levels of memory co-occur with higher initial levels of QoL. This positive relationship is also observed between the latent slopes of memory and QoL (r = .345, p < .001), which entails that steeper decline in memory is accompanied by steeper decline in QoL. The correlation between memory’s intercept and slope has an estimated value of r = − .179 (p < .001). Therefore, higher initial levels of memory are associated to a lower degree of memory decline over time. This is also the case for QoL, whose intercept and slope correlate r = − .145 (p < .001).
Finally, the model displays a statistically significant and positive effect of memory’s intercept onto QoL’s slope (β = 0.061, p < .05). However, no statistically significant effects of the initial level of QoL onto memory decline over time is found (β = − 0.017, p = .395). Therefore, it seems that initial memory affects QoL over time but not the inverse. From these results, a causal relationship of memory onto QoL can be potentially inferred. Results of the PP-LGM between delayed recall and QoL are very similar to those just presented and are available for interested readers in the Appendix.
Memory and QoL Domains
Descriptive statistics of the QoL domains at each time point are available in Table 1. First, we tested the unconditional PP-LGM between each QoL domain and memory (models 1a to 4a). Model fit results from these unconditional models are displayed in Table 3. In all cases, models adequately fitted the data. Next, the conditional PP-LGM were specified for memory and each QoL domain (models 1b to 4b). Model fit was also adequate in all cases. The fit statistic and indices from models 1b to 4b can be consulted in Table 3.
All models displayed excellent fit to the data. Regarding the characteristics of the latent trajectories of immediate memory and every of the four domains of QoL (control, autonomy, self-realization and pleasure), these are displayed in Table 4. In general, immediate memory displays decline over time, with statistically significant variances, which indicate variability of initial memory levels and rate of decline across individuals. Regarding QoL domains, we can observe differences among domains. While control and self-realization both display trajectories of decline over time, this is neither the case for autonomy nor pleasure, which display positive trajectories over time. In all cases, statistically significant variances of domains’ intercepts and slopes indicate inter-individual variations from this general trend.
Standardized effects of the covariates onto memory and QoL domains are available in Table 5. All covariates have statistically significant effects onto memory’s intercept in the expected direction. For QoL domains, all covariates display statistically significant effects onto the intercepts of control, autonomy, self-realization and pleasure, with the exception of gender onto the initial level of autonomy and age onto the initial level of pleasure. Regarding the slopes, age and depression were statistically significant predictors of memory and all QoL domains. Gender and educational attainment further exerted statistically significant effects onto memory’s slope. For QoL domains, there were inter-domain differences in the effects of the rest of covariates. For control, only social participation, in addition to age and depression, presented statistically significant effects onto its slopes, while for the slopes of the other QoL domains gender was a statistically significant predictor. Educational attainment, physical inactivity and social participation further exhibited statistically significant effects onto the slope of autonomy.
Turning to the relationships between the latent intercepts and latent slopes of memory and QoL domains within each model, these are represented in Fig. 2. In all cases, the intercept and slope of memory and QoL domains were negatively correlated. Moreover, memory’s intercept positively correlated with the intercept of each QoL domain, entailing that higher initial levels of memory are associated with higher initial levels of control, autonomy, self-realization and pleasure. In the case of the slopes of memory and QoL domains, these also exhibited a positive correlation, which indicates that steeper decline in memory is accompanied by steeper decline in control and self-realization, and that steeper decline in memory is associated with a steeper increase in autonomy and pleasure.

Standardized estimates of the relationships between latent immediate memory and latent quality of life domains from models 1b to 4b. Observable variables not shown for clarity. Note I= Intercept; S= Slope; M= Memory; C = Control; A = Autonomy; SR = Self-realization; P = Pleasure; W = Wave; ns = not statistically significant; * p < .05
Finally, as shown in Fig. 2, memory’s intercept exhibited positive and statistically significant effects onto the slopes of control and autonomy, but not onto the slopes of pleasure and self-relation. In turn, the intercepts of control and self-realization presented negative statistically significant effects on the slope of memory, while autonomy and pleasure’s intercepts did not affect the slope of memory.
Discussion
The present study examined the longitudinal association of memory with general and specific-domain QoL in a sample of the general population of European adults and older adults, while also controlling the effects of several covariates. A positive effect of initial memory onto general QoL’s trend over time was found, indicating that better memory is associated to better QoL in the future, but the opposite did not occur. Within QoL domains, results differed; while a positive effect of initial memory onto control and autonomy’s trends over time, this did not occur for self-realization and pleasure. In turn, initial levels of control and self-realization exhibited negative effects onto memory’s trend over time.
At the general QoL level, the result contrasts with the study of Wilson et al. (2013). In this study, the authors report a bidirectional and positive relationship between working memory and well-being. The research by Wilson et al. (2013) employed intentional sampling, only considered older adults and used a measure of purpose in life, a dimension of QoL, as a marker of well-being. On the one hand, it is possible that the relationship between memory and purpose in life becomes more blurred with advancing age, as having a sense of purpose in life could become cognitively challenging per se. On the other hand, the intrinsic difficulty of self-assessing one’s purpose in life when cognitive ability is compromised may be interfering in the directionality of the results (Bárrios et al., 2013; Bowling et al., 2015).
In fact, results at the QoL domain-level provide different information. In the case of control, higher initial levels of memory are associated to lower decline of feelings of control in the future, but higher initial feelings of control are associated to steeper decline of memory over time. These results imply a bidirectional relationship between control and memory but in contrast to the results by Wilson et al. (2013), this relationship is negative. In the case of autonomy, the results resemble those found for the general QoL factor. For self-realization, initial levels of memory do not affect the trend of self-realization’s feelings over time but initial levels of self-realization predict a steeper decline of memory over time. Lastly, results show that there are not longitudinal relationships between pleasure and self-realization in any direction. The heterogeneity of domain-specific results provides evidence of the multidimensionality of QoL, as stated by the definition of QoL offered by the WHO (WHOQOL Group, 1995). These results add to the reasons for which QoL should not be equated to HRQoL (Karimi & Brazier, 2016). However, we ought to keep acknowledging the theoretical conception of QoL as a whole, which defies the concept of HRQoL, and has been supported by both theory and psychometric evidence regarding the factor structure of QoL measures (for example Oliver et al., 2021).
Turning to the effects of covariates, all effects of covariates onto the latent intercepts and slopes of memory and both general and domain-specific QoL were in the expected direction according to previous literature examining memory (Ding et al., 2019; Liampas et al., 2022; McFall et al., 2019; Wu et al., 2021) and QoL (Roberts & Adams, 2018; Ward et al., 2019; Zaninotto et al., 2009) trajectories over time. One exception was the aforementioned positive effect of depression onto the latent slopes. A plausible explanation of this positive effect accompanied by the negative effect of depression onto the latent intercepts is that individuals who present high depressive symptomatology at the beginning also present diminished immediate memory and QoL, and may not have as much room for variation over time as less depressed individuals. Therefore, this would not be a beneficial effect of depression over time but the manifestation of a floor effect. Another exception was the positive effect of physical inactivity, as well as the negative effect of social participation, onto the latent slope of autonomy. These results could also be due to the negative effect of physical inactivity and the positive effect of social participation onto autonomy’s latent intercept and hence represent a floor effect rather than a substantive effect.
Moreover, gender displayed statistically significant effects onto the latent intercepts and slopes of general QoL, pleasure and self-reallization. In all three cases, women displayed higher initial levels, as noted by the negative effects of gender onto the latent intercepts, and steeper decline in general QoL and self-realization and lower increases in pleasure, as noted by the positive effects of gender onto the latent slopes. This finding is in line with findings from Cao et al. (2020) that women’s gains in healthy life expectancy are not proportional to men’s, and therefore the gap between life expectancy and healthy life expectancy is greater for women, which implies that women live more years than men in a disabled state. Nonetheless, the male advantage on QoL over time could also be a manifestation of a floor effect. As men’s initial QoL is diminished, a possible explanation is that their QoL cannot decline much over time and therefore, in comparison to women, their QoL deteriorates less severely. However, for autonomy, gender did not significantly affected the latent intercept but there was a positive effect of gender onto autonomy’s latent slope, indicating a steeper decline for women. In addition, gender did present a statistically significant effect onto the latent intercept of control in favour of women, but it did not exert significant effects onto control’s latent intercept. Overall, results seem to suggest a substantive finding rather than a methodological artefact. Previous studies have also reported this female advantage in initial levels of QoL (Roberts & Adams, 2018; Ward et al., 2019; Zaninotto et al., 2009), but none of them found evidence of gender having an effect on the latent slope of QoL.
All in all, this work found evidence supporting the longitudinal effect of memory on general QoL. In addition, this study examined longitudinal relationships of memory and domain-specific QoL and provided evidence of the heterogeneity of the relationships between memory and the specific domains of QoL. Data employed from this work came from waves 4 to 8 of the Survey of Health, Ageing and Retirement in Europe (SHARE). Some of the previously examined research used data form the English Longitudinal Study of Ageing (ELSA; Zaninotto et al., 2009) and The Irish Longitudinal Study of Ageing (TILDA; Ward et al., 2019). These constitute the three main panel studies targeted at older adults in Europe. Previous studies, however, only focused on QoL trajectories and did not test parallel latent trajectories of other important phenomena for QoL, such as cognitive ability. Moreover, most previous studies examining the relationship of cognition and QoL employed measures of HRQoL (for example: Ezzati et al., 2019; Li et al., 2020; Li et al., 2021; Xue et al., 2022). Therefore, this research extends previous research on QoL trajectories. In addition, this work highlights the multidimensional essence of QoL and has showed that considering split dimensions of QoL does not lead to the same findings as considering QoL as a whole. Finally, these results can be transferred to intervention implementation, given that evidence from this work suggests that actions directed towards alleviating age-related memory impairment could also have a positive impact onto older adults’ QoL, in line with previous research (Hudes et al., 2019).
The main shortfall in this work concerns the selection of covariates as well as the lack of fine-grained information that is characteristic of the large-scale panel surveys such as SHARE. On the one hand, the complexity of data modelling employing growth modelling methods complicated the inclusion of an elevated number of covariates. Apart from demographics and education, which are time-invariant covariates whose effects are well-documented, physical inactivity, depressive symptomatology and social activity participation were selected as indicators of the individuals’ bio-psycho-social status. Although these covariates are clearly time-variant, they were introduced onto the models as time-invariant. This was done because introducing the covariates as time-variant would have yielded an estimation of the latent trajectories of memory and QoL corrected by the effect of the covariates. However, the aim of this work was to estimate the effect these covariates have on future performance. Finally, a good compromise between QoL predictors and memory predictors had to be determined. In this sense, previous studies examining QoL trajectories employed measures of functional limitations instead of physical inactivity, which was introduced here for its strong association to cognitive ability.
References
Bárrios, H., Narciso, S., Guerreiro, M., Maroco, J., Logsdon, R., & De Mendonça, A. (2013). Quality of life in patients with mild cognitive impairment. Aging and Mental Health, 17(3), 287–292. https://doi.org/10.1080/13607863.2012.747083.
Bertola, L., Wei-Ming Watson, C., Avila, J. F., Zahodne, L. B., Angevaare, M., Schupf, N., & Manly, J. J. (2019). Predictors of episodic memory performance across Educational Strata: Multiple-group comparisons. Journal of the International Neuropsychological Society, 25(9), 901–909. https://doi.org/10.1017/S1355617719000717.
Börsch-Supan, A. (2022a). Survey of Health, Ageing and Retirement in Europe (SHARE) Wave 4. Release version: 8.0.0. SHARE-ERIC. Data set. https://doi.org/10.6103/SHARE.w4.800.
Börsch-Supan, A. (2022b). Survey of Health, Ageing and Retirement in Europe (SHARE) Wave 5. Release version: 8.0.0. SHARE-ERIC. Data set. https://doi.org/10.6103/SHARE.w5.800.
Börsch-Supan, A. (2022c). Survey of Health, Ageing and Retirement in Europe (SHARE) Wave 6. Release version: 8.0.0. SHARE-ERIC. Data set. https://doi.org/10.6103/SHARE.w6.800.
Börsch-Supan, A. (2022d). Survey of Health, Ageing and Retirement in Europe (SHARE) Wave 7. Release version: 8.0.0. SHARE-ERIC. Data set. https://doi.org/10.6103/SHARE.w7.800.
Börsch-Supan, A. (2022e). Survey of Health, Ageing and Retirement in Europe (SHARE) Wave 8. Release version: 8.0.0. SHARE-ERIC. Data set. https://doi.org/10.6103/SHARE.w8.800.
Börsch-Supan, A., Brandt, M., Hunkler, C., Kneip, T., Korbmacher, J., Malter, F., Schaan, B., Stuck, S., & Zuber, S. (2013). Data resource profile: The survey of health, ageing and retirement in europe (SHARE). International Journal of Epidemiology, 42(4), 992–1001. https://doi.org/10.1093/ije/dyt088.
Bowling, A., Rowe, G., Adams, S., Sands, P., Samsi, K., Crane, M., Joly, L., & Manthorpe, J. (2015). Quality of life in dementia: A systematically conducted narrative review of dementia-specific measurement scales. Aging and Mental Health, 19(1), 13–31. https://doi.org/10.1080/13607863.2014.915923.
Cao, X., Hou, Y., Zhang, X., Xu, C., Jia, P., Sun, X., Sun, L., Gao, Y., Yang, H., Cui, Z., Wang, Y., & Wang, Y. (2020). A comparative, correlate analysis and projection of Global and Regional Life Expectancy, Healthy Life Expectancy, and their GAP: 1995–2025. Journal of Global Health, 10(2). https://doi.org/10.7189/jogh.10.020407.
Ding, X., Charnigo, R. J., Schmitt, F. A., Kryscio, R. J., & Abner, E. L. (2019). Evaluating trajectories of episodic memory in normal cognition and mild cognitive impairment: Results from ADNI. Plos One, 14(2), 1–16. https://doi.org/10.1371/journal.pone.0212435.
Enders, C. K. (2010). Applied missing data analysis. Guilford Press.
Ernecoff, N. C., Lin, F. C., Wessell, K. L., & Hanson, L. C. (2019). Quality of life with late-stage dementia: Exploring opportunities to intervene. Journal of the American Geriatrics Society, 67(6), 1189–1196. https://doi.org/10.1111/jgs.15794.
Ezzati, A., Zammit, A. R., Katz, M. J., Derby, C. A., Zimmerman, M. E., & Lipton, R. B. (2019). Health-related quality of life, cognitive performance, and Incident Dementia in a community-based Elderly Cohort. Alzheimer Disease and Associated Disorders, 33(3), 240–245. https://doi.org/10.1097/WAD.0000000000000324.
Fernández, I., Tomás, J. M., & Bethmann, A. (2024). Latent trajectories of recent and delayed memory and their predictors: Evidence from SHARE. International Psychogeriatrics, 36(3), 210–220. https://doi.org/10.1017/S1041610222001016
Godin, J., Armstrong, J. J., Wallace, L., Rockwood, K., & Andrew, M. K. (2019). The impact of frailty and cognitive impairment on quality of life: Employment and social context matter. International Psychogeriatrics, 31(6), 789–797. https://doi.org/10.1017/S1041610218001710.
Hill, N. L., McDermott, C., Mogle, J., Munoz, E., Depasquale, N., Wion, R., & Whitaker, E. (2017). Subjective cognitive impairment and quality of life: A systematic review. International Psychogeriatrics, 29(12), 1965–1977. https://doi.org/10.1017/S1041610217001636.
Hoe, J., Hancock, G., Livingston, G., Woods, B., Challis, D., & Orrell, M. (2009). Changes in the quality of life of people with dementia living in care homes. Alzheimer Disease and Associated Disorders, 23(3), 285–290. https://doi.org/10.1097/WAD.0b013e318194fc1e.
Hu, L. T., & Bentler, P. M. (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling, 6(1), 1–55. https://doi.org/10.1080/10705519909540118.
Hudes, R., Rich, J. B., Troyer, A. K., Yusupov, I., & Vandermorris, S. (2019). The impact of memory-strategy training interventions on participant- reported outcomes in healthy older adults: A systematic review and meta-analysis. Psychology and Aging, 34(4), 587–597. https://doi.org/10.1037/pag0000340.
Hyde, M., Wiggins, R. D., Higgs, P., & Blane, D. B. (2003). A measure of quality of life in early old age: The theory, development and properties of a needs satisfaction model (CASP-19). Aging and Mental Health, 7(3), 186–194. https://doi.org/10.1080/1360786031000101157.
Johnson, J. K., Gross, A. L., Pa, J., McLaren, D. G., Park, L. Q., & Manly, J. J. (2012). Longitudinal change in neuropsychological performance using latent growth models: A study of mild cognitive impairment. Brain Imaging and Behavior, 6(4), 540–550. https://doi.org/10.1007/s11682-012-9161-8.
Karimi, M., & Brazier, J. (2016). Health, health-related quality of life, and quality of life: What is the difference? Pharmacoeconomics 34 7 645–649 https://doi.org/10.1007/s40273-016-0389-9.
Kline, R. B. (2016). Principles and practice of structural equation modeling (4th ed.).). Guildford.
Lawson, R. A., Yarnall, A. J., Duncan, G. W., Khoo, T. K., Breen, D. P., Barker, R. A., Collerton, D., Taylor, J. P., & Burn, D. J. (2014). Severity of mild cognitive impairment in early Parkinson’s disease contributes to poorer quality of life. Parkinsonism and Related Disorders, 20(10), 1071–1075. https://doi.org/10.1016/j.parkreldis.2014.07.004.
Lawson, R. A., Yarnall, A. J., Duncan, G. W., Breen, D. P., Khoo, T. K., Williams-Gray, C. H., Barker, R. A., Collerton, D., Taylor, J. P., & Burn, D. J. (2016). Cognitive decline and quality of life in incident Parkinson’s disease: The role of attention. Parkinsonism and Related Disorders, 27, 47–53. https://doi.org/10.1016/j.parkreldis.2016.04.009.
Li, C. L., Chang, H. Y., & Stanaway, F. F. (2020). Combined effects of frailty status and cognitive impairment on health-related quality of life among community dwelling older adults. Archives of Gerontology and Geriatrics, 87, 103999. https://doi.org/10.1016/j.archger.2019.103999.
Li, H. W., Lee, W. J., Lin, M. H., Peng, L. N., Loh, C. H., Chen, L. K., & Lu, C. C. (2021). Quality of life among community-dwelling middle-aged and older adults: Function matters more than multimorbidity. Archives of Gerontology and Geriatrics, 95(115), 104423. https://doi.org/10.1016/j.archger.2021.104423.
Liampas, I., Folia, V., Ntanasi, E., Yannakoulia, M., Sakka, P., Hadjigeorgiou, G., Scarmeas, N., Dardiotis, E., & Kosmidis, M. H. (2022). Longitudinal episodic memory trajectories in older adults with normal cognition. The Clinical Neuropsychologist. https://doi.org/10.1080/13854046.2022.2059011.
Maki, Y., Yamaguchi, T., Yamagami, T., Murai, T., Hachisuka, K., Miyamae, F., Ito, K., Awata, S., Ura, C., Takahashi, R., & Yamaguchi, H. (2014). The impact of subjective memory complaints on quality of life in community-dwelling older adults. Psychogeriatrics, 14(3), 175–181. https://doi.org/10.1111/psyg.12056.
Marventano, S., Prieto-Flores, M. E., Sanz-Barbero, B., Martín-García, S., Fernandez-Mayoralas, G., Rojo-Perez, F., Martinez-Martin, P., Forjaz, M. J., Rodríguez-Blázquez, C., Ayala, A., Frades-Payo, B., León-Salas, B., Ávila, M., & Martínez-Lopez, I. (2015). Quality of life in older people with dementia: A multilevel study of individual attributes and residential care center characteristics. Geriatrics and Gerontology International, 15(1), 104–110. https://doi.org/10.1111/ggi.12238.
McCracken, K., & Phillips, D. R. (2017). Demographic and epidemiological transition. In D. Richardson, N. Castree, M. F. Goodchild, et al. (Eds.), The International Encyclopedia of Geography. Wiley.
McFall, G. P., McDermott, K. L., & Dixon, R. A. (2019). Modifiable risk factors discriminate memory trajectories in non-demented aging: Precision factors and targets for promoting healthier brain aging and preventing dementia. Journal of Alzheimer’s Disease, 70(s1), S101–S118. https://doi.org/10.3233/JAD-180571.
Mowrey, W. B., Lipton, R. B., Katz, M. J., Ramratan, W. S., Loewenstein, D. A., Zimmerman, M. E., & Buschke, H. (2016). Memory binding test predicts Incident Amnestic mild cognitive impairment. Journal of Alzheimer’s Disease, 53(4), 1585–1595. https://doi.org/10.3233/JAD-160291.
Muthén, L. K., & Muthén, B. O. (1998–2017). Mplus User’s Guide, 8th ed. Muthén & Muthén.
Noll, H. H. (2021). The good life under attack: Reflections on the future of the quality of life concept. In A. C. Michalos (Ed.), The Pope of happiness: A festschrift for Ruut Veenhoven (pp. 195–201). Springer Nature.
Oliver, A., Sentandreu-Mañó, T., Tomás, J. M., Fernández, I., & Sancho, P. (2021). Quality of life in European older adults of SHARE wave 7: Comparing the old and the oldest-old. Journal of Clinical Medicine, 10(13). https://doi.org/10.3390/jcm10132850.
Prince, M. J., Reischies, F., Beekman, A. T. F., Fuhrer, R., Jonker, C., Kivela, S. L., Lawlor, B. A., Lobo, A., Magnusson, H., Fichter, M., Van Oyen, H., Roelands, M., Skoog, I., Turrina, C., & Copeland, J. R. M. (1999). Development of the EURO-D scale - A European Union initiative to compare symptoms of depression in 14 European centres. British Journal of Psychiatry, 174(4), 330–338. https://doi.org/10.1192/bjp.174.4.330.
Roberts, A. R., & Adams, K. B. (2018). Quality of Life trajectories of older adults living in Senior Housing. Research on Aging, 40(6), 511–534. https://doi.org/10.1177/0164027517713313.
Scarmeas, N., & Stern, Y. (2003). Cognitive reserve and lifestyle. Journal of Clinical and Experimental Neuropsychology, 25(5), 625–633. https://doi.org/10.1076/jcen.25.5.625.14576.
Schneider, S. L. (2008). The International Standard Classification of Education (ISCED-97). An evaluation of content and criterion validity for 15 European countries. MZES.
Schröder, M. (2011). Retrospective Data Collection in the Survey of Health, Ageing and Retirement in Europe. SHARELIFE Methodology. MEA.
Steinerman, J. R., Hall, C. B., Sliwinski, M. J., & Lipton, R. B. (2010). Modeling cognitive trajectories within longitudinal studies: A focus on older adults. Journal of the American Geriatrics Society, 58(2), 313–318. https://doi.org/10.1111/j.1532-5415.2010.02982.x.
Stern, Y. (2002). What is cognitive reserve? Theory and research application of the reserve concept. Journal of the International Neuropsychological Society, 8(3), 448–460. https://doi.org/10.1017/S1355617702813248.
Stites, S. D., Harkins, K., Rubright, J. D., & Karlawish, J. (2018). Relationships between cognitive complaints and quality of life in older adults with mild cognitive impairment, mild Alzheimer’s Disease dementia, and normal cognition. Alzheimer Disease and Associated Disorders, 32(4), 276–283. https://doi.org/10.1097/WAD.0000000000000262.
Tavares, A. I. (2022). Life expectancy at 65, associated factors for women and men in Europe. European Journal of Ageing. https://doi.org/10.1007/s10433-022-00695-1.
Tomás, J. M., Torres, Z., Oliver, A., Enrique, S., & Fernández, I. (2022). Psychometric properties of the EURO-D scale of depressive symptomatology: Evidence from SHARE wave 8. Journal of Affective Disorders, 313(15), 49–55. https://doi.org/10.1016/j.jad.2022.06.079.
Van der Zon, A., Wetzels, R. B., Bor, H., Zuidema, S. U., Koopmans, R. T. C. M., & Gerritsen, D. L. (2018). Two-year course of quality of life in nursing home residents with dementia. American Journal of Geriatric Psychiatry, 26(7), 754–764. https://doi.org/10.1016/j.jagp.2018.01.202.
Ward, M., McGarrigle, C. A., & Kenny, R. A. (2019). More than health: Quality of life trajectories among older adults—findings from the Irish longitudinal study of Ageing (TILDA). Quality of Life Research, 28(2), 429–439. https://doi.org/10.1007/s11136-018-1997-y.
Weber, D., & Loichinger, E. (2022). Live longer, retire later? Developments of healthy life expectancies and working life expectancies between age 50–59 and age 60–69 in Europe. European Journal of Ageing, 19(1), 75–93. https://doi.org/10.1007/s10433-020-00592-5.
WHOQOL Group. (1995). The World Health Organization Quality of Life assessment (WHOQOL): Position paper from the World Health Organization. Social Science & Medicine, 41(10), 1403–1409. https://doi.org/10.1016/0277-9536(95)00112-k.
Wilson, R. S., Boyle, P. A., Segawa, E., Yu, L., Begeny, C. T., Anagnos, S. E., & Bennett, D. A. (2013). The influence of cognitive decline on well-being in old age. Psychology and Aging, 28(2), 304–313. https://doi.org/10.1037/a0031196.
World Health Organization (2022). The top 10 causes of death World Health Organization. https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death.
Wu, Z., Woods, R. L., Wolfe, R., Storey, E., Chong, T. T. J., Shah, R. C., Orchard, S. G., McNeil, J. J., Murray, A. M., & Ryan, J. (2021). Trajectories of cognitive function in community-dwelling older adults: A longitudinal study of population heterogeneity. Alzheimer’s and Dementia: Diagnosis Assessment and Disease Monitoring, 13(1), 1–12. https://doi.org/10.1002/dad2.12180.
Xue, H., Huang, C., Zhu, Q., Zhou, S., Ji, Y., Ding, X., Zhang, D., & Gu, D. (2022). Relationships among cognitive function, frailty, and health outcome in community-dwelling older adults. Frontiers in Aging Neuroscience. https://doi.org/10.3389/fnagi.2021.790251.
Yam, A., Gross, A. L., Prindle, J. J., & Marsiske, M. (2014). Ten-year longitudinal trajectories of older adults’ basic and everyday cognitive abilities. Neuropsychology, 28(6), 819–828. https://doi.org/10.1037/neu0000096.
Zaninotto, P., Falaschetti, E., & Sacker, A. (2009). Age trajectories of quality of life among older adults: Results from the English longitudinal study of Ageing. Quality of Life Research, 18(10), 1301–1309. https://doi.org/10.1007/s11136-009-9543-6.
Acknowledgements
This study is part of the first author’s doctoral thesis. The SHARE data collection has been funded by the European Commission, DG RTD through FP5 (QLK6-CT-2001-00360), FP6 (SHARE-I3: RII-CT-2006-062193, COMPARE: CIT5-CT-2005-028857, SHARELIFE: CIT4-CT-2006-028812), FP7 (SHARE-PREP: GA N°211909, SHARE-LEAP: GA N°227822, SHARE M4: GA N°261982, DASISH: GA N°283646) and Horizon 2020 (SHARE-DEV3: GA N°676536, SHARE-COHESION: GA N°870628, SERISS: GA N°654221, SSHOC: GA N°823782, SHARE-COVID19: GA N°101015924) and by DG Employment, Social Affairs & Inclusion through VS 2015/0195, VS 2016/0135, VS 2018/0285, VS 2019/0332, and VS 2020/0313. Additional funding from the German Ministry of Education and Research, the Max Planck Society for the Advancement of Science, the U.S. National Institute on Aging (U01_AG09740-13S2, P01_AG005842, P01_AG08291, P30_AG12815, R21_AG025169, Y1-AG-4553-01, IAG_BSR06-11, OGHA_04–064, HHSN271201300071C, RAG052527A) and from various national funding sources is gratefully acknowledged (see www.share-project.org).
Funding
Open Access funding provided thanks to the CRUE-CSIC agreement with Springer Nature. This research is supported by project PID2021-124418OB-I00 funded by MCIN/AEI/https://doi.org/10.13039/501100011033 and by “ERDF A way of making Europe”.
Open Access funding provided thanks to the CRUE-CSIC agreement with Springer Nature.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethical Approval
Data for this study was reviewed and approved by the Ethics Council of the Max Planck Society. For an overview and summary of the ethics approvals, please see: https://share-eric.eu/fileadmin/user_upload/Ethics_Documentation/SHARE_ethics_approvals.pdf.
Competing Interests
The authors declare no conflict of interest.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic Supplementary Material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Fernández, I., Sansó, N. & Tomás, J.M. A Longitudinal Study of the Effect of Memory on the Quality of life of European Adults and Older Adults. Applied Research Quality Life (2024). https://doi.org/10.1007/s11482-024-10310-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11482-024-10310-3