
Abstract
To a large extent health-related quality of life (HRQoL) is a product of life-course experiences. Therefore, we examined employment, marital, and reproductive life-course typologies as predictors of HRQoL in women and men. To determine life course clusters, sequence and cluster analysis were performed on the annual (waves 1990–2019) employment, marital, and children in household states of the German Socio-Economic Panel data (N = 8,998; age = 53.57, 52.52% female); separately for men and women. Using hierarchical linear regression analyses, and Tukey HSD post-hoc tests, associations between clusters and change in life satisfaction, subjective mental, and physical health were examined. Five life-course clusters were identified in the female and six in the male sample. Life courses differed greatly across gender regarding employment aspects (e.g., men generally work full-time vs. women underwent frequent transitions). The family aspects appeared similar – e.g., ‘starting a family’ or ‘marital separation’ clusters – but still differed in the particulars. Life course typologies were related to distinct patterns of HRQoL. For instance, both for men and women the ‘separated’ clusters, as well as the male ‘entering non-employment’ cluster were associated with a steeper decline in HRQoL. However, change in subjective mental health showed few associations. Distinct types of life courses and differential associations with sociodemographic background and HRQoL emerged for women and men. The analyses reveal a burden on individuals who experienced marital separation, and non-employment and thus present important target groups for health prevention, e.g., for physical health problems.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
A ‘healthy lifestyle’ is a phrase often used by health services. This generally addresses health behaviours like a balanced diet or physical activity (Kekäläinen et al., 2020), but to what extent does a healthy lifestyle – and its relation to health-related quality of life (HRQoL) – also refer to how life is shaped by family and employment? And further, do certain lifestyles relate to HRQoL differently in men and women?
The concept of work-family-balance – i.e., the homemakers versus the breadwinners – has been connected to HRQoL and shown to differ in men and women. For instance, a focus on family integration over career success corresponds to social expectations of women but can lead to disengagement at work and would thus foster the work-family conflict (Lyu & Fan, 2020).
In general, better health status is associated with full-time compared to part-time or non-employment (Tomczyk et al., 2021; Gander et al., 2021), but men tend to assign greater importance to work and to report worse effects following unemployment (McKee‐Ryan et al., 2005). Yet, female participation in the labour market is rising in most European countries and attitudes towards gender roles are increasingly liberal as well (Stavrova et al., 2012). While men gain most of their status from their job, women attain their status from numerous sources (van der Meer, 2014). Forret et al. (2010) found that men with children who lost their paid work were more likely to see it as a defeat while women were more likely to see it as an opportunity.
In the past decades, an increase in father’s – and mother’s – contribution to childcare is seen Boll and Leppin (2011). Still, more time spent with childcare, household chores, and errands is related to lower HRQoL in women, but unrelated in men (Tomczyk et al., 2021). While the having a child is considered generally a joyous event, this increase in HRQoL is short-lived for fathers (Krämer & Rodgers, 2020), and mothers report lower happiness, more stress, and greater fatigue with increased time spent on childcare (Musick et al., 2016).
Being in a partnership and cohabiting is related to better HRQoL (Brazil & Clark, 2017), but again gender differences are evident; for instance, previous as opposed to present marriage is related to better life satisfaction in men (Frijters et al., 2004).
Most commonly previous studies examine life events or characteristics at a specific time point in relation to health, this approach however neglects the dynamic processes of life experiences especially in relation to health (e.g., Plagnol & Scott, 2011). In the last decade, studies have examined health outcomes in relation to life courses in the domains of employment (Giudici & Morselli, 2019), relationships and reproductivity (Mariani et al., 2017), and housing (Lim et al., 2020). Consistent across these studies is that some life course typologies are related to better HRQoL than others.
As we wanted to examine the holistic picture of the impact of work and family on HRQoL, we examined employment, marital, and reproductive trajectories together. To the best of our knowledge only two previous studies examined employment and family trajectories simultaneously: McKetta et al. (2018) studied mortality rates in women and found five types of trajectories: “nonworking, married, later-mothers; working divorced mothers; working and non-working, never-married mothers; working, never-married non-mothers; and nonworking, married earlier-mothers” (p. 301). The typologies never-married mothers as well as working, never married, childless women in comparison to non-working, married, later-mothers were linked to an elevated mortality risk.
van Hedel et al. (2016) examined cardiovascular risk in women and identified the following five life course typologies: working single childless women, non-working married mothers, working single mothers, married mothers who returned to work after some non-employment, and working married mothers. While some life courses were associated with worse health, overall, they could not determine a consistent pattern linking specific life course types to an elevated health risk.
It is noteworthy, that these two studies employed female only samples. However, both family and employment life courses are highly gendered (Helske et al., 2015; Wahrendorf et al., 2018): For example, typologies such as entering a first partnership in later life and later multiple partners are reported by men more than women (Helske et al., 2015) and full-time employment ending in later retirement is a more male dominated while predominantly part-time employment and domestic work are more female dominated life course typologies (Wahrendorf et al., 2018).
Giudici and Morselli (2019) examined the interaction of employment life course typologies and gender on health outcomes. Compared to men, women were more likely to report depressed mood in most employment versus vocationally inactive life courses, especially in full-time and double job trajectories. Women also reported worse self-rated health with frequent employment changes. Their findings stand in contrast to methodologies that examine single measurements of employment status, where men generally assign greater importance to employment and in turn report greater health detriments when non-traditional, instable employment is experienced (McKee-Ryan et al., 2005). This discrepancy stresses the importance of taking a life course – and so a holistic – approach. Therefore, we aim to:
-
1.
Determine clusters of employment, marital, and reproductive life-course trajectories by means of sequence and cluster analysis.
-
2.
Examine the associations of life course clusters with change in HRQoL.
Methodology
Data and Ethics
Data from the Core-Study of the German Socio-Economic Panel (GSOEP) was used. This is an annual representative longitudinal study of private households (Goebel et al., 2019). In the GSOEP some constructs, and indicators are measured annually (e.g., household structure, employment history, income), while others are measured once or at less frequent intervals (e.g., subjective mental and physical health).
Data collection began in West Germany in 1984 and directly after reunification in 1990 a sample of East German participants joined the panel. To reflect German society in the period since the reunification, we used data from 1990 to the most recent wave (i.e., 2019). As our focus lay on employment and family aspects, we concentrated on middle-aged persons and only included participants who were between 18 and 65 years old in each respective wave (n = 24,836). Furthermore, to be able to determine sequences and not merely include individual states, participants with less than 50% complete data with respect to employment, partnership, and children in household were excluded (n = 28,888).
This study is a secondary analysis of the GSOEP data; therefore, no additional ethical approval was needed. In the primary studies, all human studies were approved by the appropriate ethics committee and have therefore been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards and written informed consent was obtained from each subject (Goebel et al., 2019; Liebig et al., 2019). The data that support the findings of this study are available from German Institute for Economic Research (DIW). The current study protocols were approved by the (DIW). Data can be accessed following an application to the DIW: https://www.diw.de/en/diw_01.c.618953.en/the_institute.html.
Variables and Measures
Life Courses
Employment, marital, and reproductive states were examined as longitudinal sequences in annual intervals (1990–2019).
Employment Life Course
The item “Are you currently employed? Which one of the following applies best to your status?” was used to measure employment status. The following four categories were formed: full-time employment, regular part-time employment, non-employment, and other employment (including: vocational training, marginally employed, near retirement, zero working hours, voluntary military service, voluntary services, sheltered workshop, internship, & completing compulsory military service / community service).
Marital Life Course
Marital status was measured with the item “What is your marital status?”. The following categories were used: married, separated (response options: “married, separated”, “divorced, registered partnership dissolved”), and single.Footnote 1
Reproductive Life Course
Three categories, using the item children currently living in the household, were formed: no children, 1 child, and 2 or more children.
Change in Health-Related Quality of Life
The present study focuses on the concept of health-related quality of life, in the analyses the following three components of HRQoL are examined separately: general life satisfaction, subjective mental, and physical health.
General life satisfaction was measured using the items. How satisfied are you with your life overall?” (Schimmack et al., 2008). An 11-point scale of 0 (completely dissatisfied) to 10 (completely satisfied) was used, where higher values reflected greater satisfaction.
Subjective mental and physical health were measure using the SOEP-SF-12 (Nübling et al., 2006). The mental health subscale includes six items that measure mental health, emotional role functioning, social functioning, and vitality, while the physical health subscale contains six items that measure general health, physical fitness, bodily pain, and physical role functioning. General health is assessed on a 5-point Likert scale ([1] very good to [5] bad), the physical fitness items are assessed on a 3-point Likert scale ([1] greatly to [3] not at all), and the other items are measured on a 5-point Likert scale ([1] always to [5] never). Example items include: “Please think about the last four weeks. How often did it occur within this period of time, that due to mental or emotional problems you carried out your work or everyday tasks less thoroughly than usual?” (subjective mental health) and “…that you had strong physical pains?” (subjective physical health). Each subscale was scaled onto a value between 0–100, where higher scores represent better subjective health.
Change in HRQoL components (i.e., general life satisfaction, subjective mental, and physical health) were computed by subtracting each participant's baseline value from their last value in the time period 1990–2019.
Sociodemographic Variables
The last value in the time period 1990–2019 was used for gender (0 = male, 1 = female), age (years), household income (Euros ÷ 1000), education (ISCED-11 dummy coded: low [1–3], moderate [4–5] (reference), high [6–8]), and region of residence (0 = West Germany, 1 = East Germany).
Statistical Analysis
Sequence and Cluster Analysis
Sequence analysis (SA) (Gauthier et al., 2010; Pollock, 2007) in women and men separately was used to establish the typical employment, marital, and reproductive life courses (see supplementary information 1 for an example of this statistical approach). This method allows life histories to be quantified by examining ‘states’ (e.g., employed full-time, employed part-time, not employed) and their respective changes from one state to another (e.g., not employed in 1992 to employed full-time in 1993). Missing data for employment, marital, or reproductive states were coded as separate states (i.e., ‘Missing’).
By means of SA all sequences are compared pairwise to determine how similar they are to one another (Abbott, 1995). Optimal matching analysis is one of the most popular methods of SA, where the number of modifications that need to be made from one sequence to another (i.e., altering a state in each wave) determines sequence similarity. It also provides flexibility in setting the substitution costs. That is to say, individual sequences are considered similar if they are made up of similar states occurring at similar time points. Optimal matching produces a pairwise distance matrix, which shows the ‘distance’ between all possible pairs of individual sequences.
As we are examining employment, marital, and reproductive sequences simultaneously, we used multi-channel SA. The main difference between SA and multi-channel SA is that the latter takes into account the interaction between two or more domains by examining similarities between sequences in more than one domain (Gauthier et al., 2010; Ward, 1963). That means that two individual sequences are only considered similar if the states in all domains are similar and experienced at similar time points. The three channels were weighted equally.
Once sequence similarity was established, we clustered sequences that were more similar to one another and determined typologies. For this we employed Ward cluster analysis (Ward, 1963). The Ward method is a hierarchical clustering algorithm that joins the two least distant groups at each step. It is the preferred clustering method as it aims to minimize within cluster discrepancies (Gauthier et al., 2010). We examined the two- to 15-cluster options. To determine the most appropriate number of clusters we examined the dendrograms, and the cluster cut-off criteria (Average Silhouette Width [ASW] & Point Biserial Correlation [PBC]; higher values indicate higher quality partitions; (Hennig & Liao, 2010; Studer, 2013)). We conducted sensitivity analyses with different waves of the data, to ensure robustness of the clusters.
Descriptive Statistics
Data was examined across gender (male, female), and life course clusters using t-tests, ANOVA, Tukey HSD post-hoc-tests, and chi-square tests. To describe the life course clusters we also used Shannon’s entropy (“the ‘uncertainty’ of predicting the states in a given sequence”; (Gabadinho et al., 2011a, p. 78)), and Elzinga’s turbulence (the amount of states and state changes; (Elzinga & Liefbroer, 2007)).
Hierarchical Linear Regression Analyses (HLR)
To examine the associations between life course clusters and change in HRQoL, HLR models were run separately for gender (i.e., male, female) and HRQoL outcomes (i.e., life satisfaction, subjective mental, and physical health). Life course cluster was entered as the predictor variable, the respective HRQoL baseline variable was entered as the control variable, and change in HRQoL was considered the outcome variable. In a next step Tukey HSD post-hoc-tests, which corrects p-values for multiple testing, were performed to examine all potential cluster contrasts.
All analyses were conducted with the statistical software R version 3.6.2 (R Core Team, 2019), along with the libraries car (Fox & Weisberg, 2019) to relevel the categorical variables, TraMineR (Gabadinho et al., 2011b) for the multichannel SA and visualisation of the life course clusters, cluster (Maechler et al., 2019) for cluster analysis, lm to run the HLRs, multcomp (Hothorn et al., 2008) to run the Tukey HSD post-hoc tests, broom (Robinson et al., 2020) and DescTools (Signorell et al., 2021) to summarise the output, emmeans (Searle et al., 1980) to extract the predicted values, and ggplot2 (Wickham & Chang, 2015) to visualise the predicted values and results from the post-hoc-tests.
Results
The sample comprised 8,998 persons (52.52% female), with a mean age of 53.57 years (SD = 9.60; see Table 1). Compared to women, men were older and reported higher education. Men also reported better subjective mental and physical subjective health, but lower life satisfaction.
Life-Course Clusters
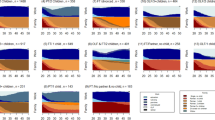
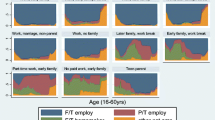
See supplementary information 2 for the substitution cost matrices, the ten most frequent sequences for the employment, marital, and reproductive sequences, entropy and turbulence values, dendrograms, and cluster cut-off criteria. See Fig. 1 for individual employment, marital, and reproductive sequences.

Employment-family life course clusters separate by female (n = 4,726) and male (n = 4,272) sample Note. Female typologies: C1=‘getting employed, married, & 2+ children’, C2=‘single & no children’, C3=‘employed, married & 1 child’, C4=‘separated’, C5=‘starting a family’. Male typologies: C1=‘entering employment, single & no children’, C2=‘leaving employment & married’, C3=‘separated’, C4=‘married & children moving out by 2005’, C5=‘starting a family’, C6=‘married & children moving out by 2010’.
For the female sample, the dendrogram favoured the four- to six cluster options. Of the cluster cut off criteria, the highest ASW-values were seen for the two-, three-, and five-cluster options, while the highest PBC-value was seen for the five-cluster option. The sensitivity analyses confirmed the robustness of the five-cluster option.
The first female life course cluster ‘getting employed, married, & 2 + children’ (n = 885, 18.73%) was characterised mainly by transitions from non- or other to part-time employment around 2002. Most individuals in this cluster had two or more children. The second female cluster ‘single & no children’ (n = 928, 19.64%) was characterised by singledom and having no children living in the household. It also showed numerous changes in employment states. The third cluster ‘employed, married & 1 child’ (n = 1894, 40.08%) was the largest cluster, making up 40% of the female sample. Most women in this cluster were either in part- or full-time employment, were married, and had one child living with them. The fourth female cluster ‘separated’ (n = 474, 10.03%) was the smallest cluster and was characterised by marital separation. Women in this cluster showed numerous employment transitions and generally had two or more children living with them. The fifth cluster ‘starting a family’ (n = 545, 11.53%) was the second smallest cluster and was characterised by women who got married and had children around 2000. Also, around this time they were not employed and mainly re-entered part-time employment around 2010. The female life-course clusters generally show high turbulence for employment compared to marriage, and some extent children, sequences. Cluster 1 ‘getting employed, married, & 2 + children’, and C3 ‘employed, married & 1 child’ showed the lowest turbulence and entropy, while the highest values were seen for C5 ‘starting a family’.
For the male sample, the dendrogram favoured the three- to six-cluster options. Of the cluster cut off criteria, the highest ASW-values were seen for the two- to six-cluster options, while the highest PBC-values were seen for the four- to seven-cluster options. The six-cluster option proved most robust following the sensitivity analyses.
The first male life course cluster ‘entering employment, single & no children’ (n = 891, 20.86%) is mainly characterised by singledom and not having children throughout. Men in this cluster also transition from other or non-employment to full-time employment around 2010. The second male cluster ‘leaving employment & married’ (n = 1066, 24.95%) is characterised by becoming not employed by around 2003. These men were also mainly married and had no children living in the household. The third male cluster ‘separated’ (n = 372, 8.71%) was the smallest and was characterised by marital separation and children moving out by around 2000. These men were mainly in full-time employment, although some also showed sequences of non-employment. The fourth male cluster ‘married & children moving out by 2005’ (n = 834, 19.52%) showed men who were mainly in full-time employment, married, and their children moved out by around 2005. The fifth male cluster ‘starting a family’ (n = 400, 9.36%) was characterised by getting married and having children by around 2000. These men were mainly in full-time employment, while some were in other or non-employment before 2000. The sixth cluster ‘married & children moving out by 2010’ (n = 709, 16.60%) showed similar trajectories to cluster 4, except that the children moved out later, namely by around 2010. Cluster 4 ‘married & children moving out by 2005’, and C6 ‘married & children moving out by 2010’ showed the lowest turbulence in employment and marital states. Also, turbulence values for the children sequences increased from cluster 1 to 6.
Associations with Sociodemographic Background
Both the female and male life course clusters differed significantly regarding sociodemographic background (Table 2). In both the male and female samples, the ‘single’, and ‘starting a family’ clusters were youngest, while the ‘separated’ clusters were oldest. In the female sample, C1 ‘getting employed, married, & 2 + children’, and C5 ‘starting a family’ showed the highest, while in the male sample C2 ‘leaving employment & married’, and C3 ‘separated’ the lowest household income. The female C1 ‘getting employed, married, & 2 + children’ consisted of the highest proportion of East German residents, while the male C6 ‘married & children moving out by 2010’ of the lowest proportion. The female C3 ‘employed, married & 1 child’ comprised the highest proportion of individuals with higher education, while the male C3 ‘separated’ comprised the lowest proportion of individuals with moderate education as well as the highest proportion of individuals with low education.
Associations with Change in Health-Related Quality of Life
Below we highlight some of the findings from the HLR analyses and Tukey HSD post-hoc tests (see Figs. 2 & 3).

Predicted values from the hierarchical linear regression analyses and results from the Tukey HSD post-hoc-tests in the female sample (n = 4,726). Note. C1 = ‘getting employed, married, & 2 + children’, C2 = ‘single & no children’, C3 = ‘employed, married & 1 child’, C4 = ‘separated’, C5 = ‘starting a family’. Significant Tukey HSD post-hoc contrasts are coloured black (p < .05). Analyses are controlling for baseline values of health-related quality of life

Predicted values from the hierarchical linear regression analyses and results from the Tukey HSD post-hoc-tests in the male sample (n = 4,272). Note. C1 = ‘entering employment, single & no children’, C2 = ‘leaving employment & married’, C3 = ‘separated’, C4 = ‘married & children moving out by 2005’, C5 = ‘starting a family’, C6 = ‘married & children moving out by 2010’. Significant Tukey HSD post-hoc contrasts are coloured black (p < .05). Analyses are controlling for baseline values of health-related quality of life
First we examined the results for the female sample: The HLM with life satisfaction (F(5, 4565) = 497.2, p < 0.001, R2 = 0.35) showed significant associations with the baseline values (b = -0.60, p < 0.001). Compared to C3 ‘employed, married & 1 child’, which showed a deterioration in life satisfaction, C1 ‘getting employed, married, & 2 + children’ (b = 0.10, p = 0.002), C2 ‘single & no children’ (b = 0.12, p < 0.001), and C5 ‘starting a family’ (b = 0.17, p < 0.001) showed stability. The post-hoc test confirmed, for instance, that C3 ‘employed, married & 1 child’ showed a greater deterioration in life satisfaction as compared to C1 ‘getting employed, married, & 2 + children’. Also C4 ‘separated’ showed a greater deterioration in life satisfaction compared to C5 ‘starting a family’.
The HLM with subjective mental health (F(5, 4349) = 397.4, p < 0.001, R2 = 0.31) showed significant associations with the baseline values (b = -0.56, p < 0.001). Compared to C2 ‘single & no children’ (b = -0.07, p = 0.03), and C5 ‘starting a family’ (b = -0.09, p = 0.03), C3 ‘employed, married & 1 child’ showed greater improvement in subjective mental health. The post-hoc test revealed no significant differences across the life course clusters.
In respect to the HLM with subjective physical health (F(5, 4349) = 250.9, p < 0.001, R2 = 0.22), the baseline values showed a significant negative association (b = -0.49, p < 0.001). Parallel to the findings with life satisfaction, compared to C1 ‘getting employed, married, & 2 + children’ (b = 0.19, p < 0.001), C2 ‘single & no children’ (b = 0.35, p < 0.001), and C5 ‘starting a family’ (b = 0.36, p < 0.001), C3 ‘employed, married & 1 child’, showed a deterioration in subjective physical health. The post-hoc test for subjective physical health confirmed this finding. Also, C4 ‘separated’ showed a greater deterioration in subjective physical health compared to C5 ‘starting a family’.
Next we examined the findings in the male sample: The HLM with life satisfaction (F(6, 4100) = 324.8, p < 0.001, R2 = 0.32) showed significant negative associations with the baseline values (b = -0.57, p < 0.001). Compared to C1 ‘entering employment, single & no children’, C5 ‘starting a family’, and C6 ‘married & children moving out by 2010’, C2 ‘leaving employment & married’ showed a greater deterioration in life satisfaction. The post-hoc test showed, for example, the highest stability in life satisfaction for C5 ‘starting a family’, compared to C2 ‘leaving employment & married’, C3 ‘separated’, and C4 ‘married & children moving out by 2005’, which showed deteriorations in life satisfaction.
The HLM with subjective mental health (F(6, 3889) = 285.6, p < 0.001, R2 = 0.30) showed a significant association with the baseline values (b = -0.55, p < 0.001). Contrary to the findings with life satisfaction, compared to C1 ‘entering employment, single & no children’, C5 ‘starting a family’, and C6 ‘married & children moving out by 2010’, C2 ‘leaving employment & married’ showed a greater improvement in subjective mental health. The post-hoc test confirmed that, compared to C1 ‘entering employment, single & no children’, C2 ‘leaving employment & married’ showed greater improvement in subjective mental health.
The HLM with subjective physical health (F(6, 3889) = 156.3, p < 0.001, R2 = 0.19) showed a significant association with the baseline values (b = -0.46, p < 0.001). Similar to the findings with life satisfaction, compared to C1 ‘entering employment, single & no children’, C5 ‘starting a family’, and C6 ‘married & children moving out by 2010’, C2 ‘leaving employment & married’ showed a greater deterioration in subjective physical health. The post-hoc test further showed that C1 ‘entering employment, single & no children’, and C5 ‘starting a family’ showed greater stability compared to C2 ‘leaving employment & married’, C3 ‘separated’, and C4 ‘married & children moving out by 2005’, which showed greater decline. Also, C6 ‘married & children moving out by 2010’ showed high stability compared to C2, C3, and C4; however was less stable than C5 ‘starting a family’.
Discussion
The present study examined clusters of employment, marital, and reproductive life courses, and their associations with change in HRQoL in women and men. Bearing in mind the importance of HRQoL in the assessment and evaluation of psychological and general health treatments (Huppert & So, 2013), preventative practice can target groups who experience certain life styles.
Despite changing attitudes towards gender roles and increasing female participation in the work force (Stavrova et al., 2012), our findings reiterated that how we lead our life is highly gendered in areas of employment and family. Life courses regarding employment still differ greatly regarding employment aspects, where men generally work full-time while women work part-time and experience frequent employment transitions. Similarly, Wahrendorf et al. (2018) found that full-time employment ending in later retirement was a more male dominated whereas predominantly part-time employment and domestic work were more female dominated life course typologies. We found that while similar life course sequences were seen across genders regarding family aspects – e.g., starting a family or marital separation – they still differed in the particulars: For instance, only for men marital separation was followed by the children moving out of the household, while for women starting a new family was coupled with a break from employment.
Departing from the traditional gender roles of breadwinners versus homemakers, feminist theories purport a more nuanced, gendered perspective, where, for instance, unpaid housework may be considered an act of love and an equal contribution to paid work (e.g., Thompson & Walker, 1989). The female life course typology that appears to integrate work and family– i.e., employed, married & 1 child – also shows one of the largest deteriorations in HRQoL. Similarly Tomczyk et al. (2021) found that time spent on household chores and childcare continues to mainly be performed by women, which ultimately reflects in poorer health outcomes. Thus, it is fair to say, that women who aim to fulfil expectations on two fronts – i.e., work and family – ultimately pay a larger health cost.
In line with the large body of research that has stresses the negative health effects of unemployment (McKee-Ryan et al., 2005), we found that for women ‘becoming employed’ – albeit part-time – was clearly related to an improvement in HRQoL and for men ‘entering non-employment’ was related to a steeper decline in subjective physical health. However, for men ‘entering non-employment’ compared to ‘leaving non-employment and becoming employed’ was also related to an improvement in subjective mental health, as if to suggest a relief from work stressors. These ambiguous findings with HRQoL of the two male non-employment typologies underlines the merit of the sequence and cluster analysis method, as this would not have been picked up by cross-sectional approaches.
A critical life event that seemingly affects men and women similarly – healthwise – is marital separation. Previous research stressed the importance of a steady partnership (Brazil & Clark, 2017). Beyond showing a great deterioration in HRQoL, individuals in the separated typologies also reported a lower household income and showed instability in employment trajectories. This indicates that marital separation may be followed by other – e.g., employment-related – critical life events or, alternatively, be a result of these life changes. Either way, this underlines the importance that health campaigns target populations who have separated from a spouse, as this may indicate imminent health deteriorations.
Finally, while life experiences are seen as vital during the diagnostic phase of mental illness (König et al., 2018), we only saw few associations with subjective mental health. This aligns with research that found that life events are related to short-term effects on mental health (Suh et al., 1996). Instead, we found distinct associations between life course typologies, and life satisfaction, as well as subjective physical health, which highlights the importance of targeting these groups in preventative campaigns for not only mental but also – or even more so – physical illness.
Strengths, Limitations, and Future Directions
One major strength of the present study was that it examined types of employment, marital, and reproductive trajectories rather than sociodemographic variables at a specific time point in relation to HRQoL. This acknowledges the dynamic processes of life experiences, especially in relation to health. The contradictory findings with HRQoL of the two male non-employment typologies, underlines the merit of this approach. Future research may want to examine the role of psychosocial resources (e.g., optimism or social support) in the relationship between life-course experiences, and HRQoL.
Naturally, our study is not without its limitations. We used a large but not representative dataset based on self-reports. While this is important to capture the subjective experience of life courses and connect it to subjective attitudes, it may also be biased, thus inflating correlations between data (i.e., method bias).
Also, we examined change in HRQoL by considering personal baseline and end values, which neglects possible period effects. However, the advantage of the present approach is, first, that it minimises the exclusion of participants who may not have been part of the panel at a set end point (e.g., 2019), and so, second, avoids having to test the associations with HRQoL of a subset that may not be representative of membership of the life-course clusters.
Conclusions
This study identified male and female typologies of employment, marital, and reproductive life courses in the general population, that showed distinct sociodemographic profiles, and associations with indicators of HRQoL. Certain life courses – e.g., entering non-employment and marital separation – appear to go hand in hand with a decline in subjective physical health, and life satisfaction, but – contrary to previous studies – less with mental health. We thus propose for health diagnostics and treatments to especially target groups with the identified ‘at risk’ life experiences.
Data Availability
This study is a secondary analysis of the German Socio-Economic Panel data (Goebel et al., 2019; Liebig et al., 2019). The data that support the findings of this study are available from German Institute for Economic Research and can be accessed following an application: https://www.diw.de/en/diw_01.c.618953.en/the_institute.html.
Notes
As this was not the focus of the current study and because we expected greater heterogeneity in homosexual person’s life courses, we only focused on heterosexual individuals.
References
Abbott, A. (1995). Sequence Analysis: New Methods for Old Ideas. Annual Review of Sociology, 21(1), 93–113. https://doi.org/10.1146/annurev.so.21.080195.000521
Boll, C., & Leppin, J. (2011). Zeitverwendung von Eltern auf Familie und Beruf im internationalen Vergleich. Retrieved January 12, 2022 from https://www.hwwi.org/fileadmin/hwwi/Publikationen/Policy/HWWI_Policy_Paper-59_Kurzfassung.pdf
Brazil, N., & Clark, W. A. V. (2017). Individual mental health, life course events and dynamic neighbourhood change during the transition to adulthood. Health & Place, 45, 99–109. https://doi.org/10.1016/j.healthplace.2017.03.007
Elzinga, C. H., & Liefbroer, A. C. (2007). De-standardization of Family-Life Trajectories of Young Adults: A Cross-National Comparison Using Sequence Analysis. European Journal of Population, 23(3–4), 225–250. https://doi.org/10.1007/s10680-007-9133-7
Forret, M. L., Mainiero, L. A., & Sullivan, S. E. (2010). Gender role differences in reactions to unemployment: Exploring psychological mobility and boundaryless careers. Journal of Organizational Behavior, 31(5), 647–666. https://doi.org/10.1002/job.703
Fox, J., & Weisberg, S. (2019). An R Companion to Applied Regression (Version Third edition) [Computer software]. Sage. Retrieved January 12, 2022 from https://socialsciences.mcmaster.ca/jfox/Books/Companion/.
Frijters, P., Haisken-DeNew, J. P., & Shields, M. A. (2004). Money Does Matter! Evidence from Increasing Real Income and Life Satisfaction in East Germany Following Reunification. The American Economic Review, (94), Article 3, 730–740. https://doi.org/10.1257/00028280
Gabadinho, A., Müller, N. S., Ritschard, G., & Studer, M. (2011a). Mining sequence data in R with the TraMineR package: A user’s guide. Geneva: Department of Econometrics and Laboratory of Demography, University of Geneva. http://mephisto.unige.ch/traminer
Gabadinho, A., Ritschard, G., Müller, N. S., & Studer, M. (2011b). Analyzing and Visualizing State Sequences in R with TraMineR. Journal of Statistical Software, 40(4). https://doi.org/10.18637/jss.v040.i04.
Gander, F., Hofmann, J., & Ruch, W. (2021). From Unemployment to Employment and Back: Professional Trajectories and Well-Being. Applied Research in Quality of Life, 16(2), 739–751. https://doi.org/10.1007/s11482-019-09797-y
Gauthier, J.‑A., Widmer, E. D., Bucher, P., & Notredame, C. (2010). 1. Multichannel Sequence Analysis Applied to Social Science Data. Sociological Methodology, 40(1), 1–38. https://doi.org/10.1111/j.1467-9531.2010.01227.x
Giudici, F., & Morselli, D. (2019). 20 Years in the world of work: A study of (nonstandard) occupational trajectories and health. Social Science & Medicine, 1982(224), 138–148. https://doi.org/10.1016/j.socscimed.2019.02.002
Goebel, J., Grabka, M. M., Liebig, S., Kroh, M., Richter, D., Schröder, C., & Schupp, J. (2019). The German Socio-Economic Panel (SOEP). Jahrbücher Für Nationalökonomie Und Statistik, 239(2), 345–360. https://doi.org/10.1515/jbnst-2018-0022
Helske, S., Steele, F., Kokko, K., Räikkönen, E., & Eerola, M. (2015). Partnership formation and dissolution over the life course: applying sequence analysis and event history analysis in the study of recurrent events. Longitudinal and Life Course Studies, 6(1), 1–25. https://doi.org/10.14301/llcs.v6i1.290
Hennig, C., & Liao, T. F. (2010). Comparing latent class and dissimilarity based clustering for mixed type variables with application to social stratification (Research Report No. 308). Department of Statistical Science, University College London.
Hothorn, T., Bretz, F., & Westfall, P. (2008). Simultaneous inference in general parametric models. Biometrical Journal: Journal of Mathematical Methods in Biosciences, 50(3), 346–363.
Huppert, F. A., & So, T. T. C. (2013). Flourishing Across Europe: Application of a New Conceptual Framework for Defining Well-Being. Social Indicators Research, 110(3), 837–861. https://doi.org/10.1007/s11205-011-9966-7
Kekäläinen, T., Freund, A. M., Sipilä, S., & Kokko, K. (2020). Cross-Sectional and Longitudinal Associations between Leisure Time Physical Activity, Mental Well-Being and Subjective Health in Middle Adulthood. Applied Research in Quality of Life, 15(4), 1099–1116. https://doi.org/10.1007/s11482-019-09721-4
König, J., Block, A., Becker, M., Fenske, K., Hertel, J., van der Auwera, S., Zymara, K., Völzke, H., Freyberger, H. J., & Grabe, H. J. (2018). Assessment of subjective emotional valence and long-lasting impact of life events: Development and psychometrics of the Stralsund Life Event List (SEL). BMC Psychiatry, 18(1), 105.
Krämer, M. D., & Rodgers, J. L. (2020). The impact of having children on domain-specific life satisfaction: A quasi-experimental longitudinal investigation using the Socio-Economic Panel (SOEP) data. Journal of Personality and Social Psychology. Advance online publication. https://doi.org/10.1037/pspp0000279
Liebig, S., Goebel, J., Schröder, C., Grabka, M., Richter, D., Schupp, J., Bartels, C., Fedorets, A., Franken, A., Jacobsen, J., Kara, S., Krause, P., Kröger, H., Kroh, M., Metzing, M., Nebelin, J., Schacht, D., Schmelzer, P., Schmitt, C., . . . Deutsches Institut Für Wirtschaftsforschung. (2019). Sozio-oekonomisches Panel (SOEP), Daten der Jahre 1984-2018. https://doi.org/10.5684/SOEP-CORE.V35
Lim, S., Liu, S. Y. S., Jacobson, M. H., Poirot, E., Crossa, A., Locke, S., Brite, J., Hamby, E., Bailey, Z., & Farquhar, S. (2020). Housing stability and diabetes among people living in New York city public housing. SSM - Population Health, 11, 100605. https://doi.org/10.1016/j.ssmph.2020.100605
Lyu, X., & Fan, Y. (2020). Research on the relationship of work family conflict, work engagement and job crafting: A gender perspective. Current Psychology. Advance online publication. https://doi.org/10.1007/s12144-020-00705-4
Maechler, M., Rousseeuw, P., Struyf, A., Hubert, M., & Hornik, K. (2019). Cluster: Cluster Analysis Basics and Extensions (Version 2.1.0). R Package.
Mariani, E., Özcan, B., & Goisis, A. (2017). Family Trajectories and Well-being of Children Born to Lone Mothers in the UK. European Journal of Population, 33(2), 185–215. https://doi.org/10.1007/s10680-017-9420-x
McKee-Ryan, F. M., Song, Z., Wanberg, C. R., & Kinicki, A. J. (2005). Psychological and physical well-being during unemployment: A meta-analytic study. The Journal of Applied Psychology, 90(1), 53–76. https://doi.org/10.1037/0021-9010.90.1.53
McKetta, S., Prins, S. J., Platt, J., Bates, L. M., & Keyes, K. (2018). Social sequencing to determine patterns in health and work-family trajectories for U.S. Women, 1968–2013. SSM - Population Health, 6, 301–308. https://doi.org/10.1016/j.ssmph.2018.10.003
Musick, K., Meier, A., & Flood, S. (2016). How Parents Fare. American Sociological Review, 81(5), 1069–1095.https://doi.org/10.1177/0003122416663917
Nübling, M., Andersen, H. H., & Mühlbacher, A. (2006). Entwicklung eines Verfahrens zur Berechnung der körperlichen und psychischen Summenskalen auf Basis der SOEP-Version des SF 12 (Algorithmus). Berlin.
Plagnol, A. C., & Scott, J. (2011). What Matters for Well-Being: Individual Perceptions of Quality of Life Before and After Important Life Events. Applied Research in Quality of Life, 6(2), 115–137. https://doi.org/10.1007/s11482-010-9119-1
Pollock, G. (2007). Holistic trajectories: A study of combined employment, housing and family careers by using multiple-sequence analysis. Journal of the Royal Statistical Society: Series a (statistics in Society), 170(1), 167–183. https://doi.org/10.1111/j.1467-985X.2006.00450.x
R Core Team. (2019). R: A language and environment for statistical computing (Version 3.6.2) [Computer software]. R Foundation for Statistical Computing. Retrieved January 12, 2022 from https://www.R-project.org/
Robinson, D., Hayes, A., & Couch, S. (2020). broom: Convert Statistical Objects into Tidy Tibbles [Computer software]. Retrieved January 12, 2022 from https://CRAN.R-project.org/package=broom
Schimmack, U., Schupp, J., & Wagner, G. G. (2008). The Influence of Environment and Personality on the Affective and Cognitive Component of Subjective Well-being. Social Indicators Research, 89(1), 41–60. https://doi.org/10.1007/s11205-007-9230-3
Searle, S. R., Speed, F. M., & Milliken, G. A. (1980). Population Marginal Means in the Linear Model: An Alternative to Least Squares Means. The American Statistician, 34(4), 216–221. https://doi.org/10.1080/00031305.1980.10483031
Signorell, A., Aho, K., Alfons, A., Anderegg, N., Aragon, T., & Arppe, A. (2021). DescTools: Tools for descriptive statistics [Computer software]. Retrieved January 12, 2022 from https://cran.r-project.org/package=DescTools
Stavrova, O., Fetchenhauer, D., & Schlösser, T. (2012). Cohabitation, Gender, and Happiness. Journal of Cross-Cultural Psychology, 43(7), 1063–1081. https://doi.org/10.1177/0022022111419030
Studer, M. (2013). WeightedCluster library manual: A practical guide to creating typologies of trajectories in the social sciences with R. LIVES Working Papers, 24. University of Geneva Institute for Demographic and Life Course Studies. https://doi.org/10.12682/lives.2296-1658.2013.24
Suh, E., Diener, E., & Fujita, F. (1996). Events and Subjective Weil-Being: Only Recent Events Matter. Journal of Personality and Social Psychology, 70(5), 1091–1102.
Thompson, L., & Walker, A. J. (1989). Gender in Families: Women and Men in Marriage, Work, and Parenthood. Journal of Marriage and the Family, 51(4), 845. https://doi.org/10.2307/353201
Tomczyk, S., Altweck, L., & Schmidt, S. (2021). How is the way we spend our time related to psychological wellbeing? A cross-sectional analysis of time-use patterns in the general population and their associations with wellbeing and life satisfaction. BMC public health, 21(1), 1–9. https://doi.org/10.1186/s12889-021-11712-w
van der Meer, P. H. (2014). Gender, Unemployment and Subjective Well-Being: Why Being Unemployed Is Worse for Men than for Women. Social Indicators Research, 115(1), 23–44. https://doi.org/10.1007/s11205-012-0207-5
van Hedel, K., Mejía-Guevara, I., Avendaño, M., Sabbath, E. L., Berkman, L. F., Mackenbach, J. P., & van Lenthe, F. J. (2016). Work-Family Trajectories and the Higher Cardiovascular Risk of American Women Relative to Women in 13 European Countries. American Journal of Public Health, 106(8), 1449–1456. https://doi.org/10.2105/AJPH.2016.303264
Wahrendorf, M., Zaninotto, P., Hoven, H., Head, J., & Carr, E. (2018). Late Life Employment Histories and Their Association With Work and Family Formation During Adulthood: A Sequence Analysis Based on ELSA. The Journals of Gerontology. Series B, Psychological Sciences and Social Sciences, 73(7), 1263–1277. https://doi.org/10.1093/geronb/gbx066
Ward, J. H. (1963). Hierarchical Grouping to Optimize an Objective Function. Journal of the American Statistical Association, 58(301), 236–244. https://doi.org/10.1080/01621459.1963.10500845
Wickham, H., & Chang, W. (2015). ggplot2 [Computer software]. Retrieved January 12, 2022 from http://ggplot2.org
Funding
Open Access funding enabled and organized by Projekt DEAL. This work was financially supported by the German Federal Ministry of Education and Research, Berlin [grant number 01UJ1911DY]. The funder had no involvement in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing Interests
The authors have no employment, financial, non-financial or other competing interests to declare.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Altweck, L., Hahm, S., Schmidt, S. et al. Even Now Women Focus on Family, Men on Work: An Analysis of Employment, Marital, and Reproductive Life-Course Typologies in Relation to Change in Health-Related Quality of Life. Applied Research Quality Life 18, 1205–1223 (2023). https://doi.org/10.1007/s11482-022-10130-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11482-022-10130-3