
Abstract
Purpose
Forensic verification of cyanide (CN) poisoning by direct CN analysis in postmortem blood is challenging due to instability of CN in biological samples. CN metabolites, thiocyanate (SCN−) and 2-aminothiazoline-4-carboxylic acid (ATCA), have been proposed as more stable biomarkers, yet it is unclear if either is appropriate for this purpose. In this study, we evaluated the behavior of CN biomarkers in postmortem swine and postmortem blood to determine which serves as the best biomarker of CN exposure.
Methods
CN, SCN−, and ATCA were measured in postmortem swine (N = 8) stored at 4 °C and postmortem blood stored at 25 °C (room temperature, RT) and 37 °C (typical human body temperature, HBT).
Results
Following CN poisoning, the concentration of each CN biomarker increased well above the baseline. In postmortem swine, CN concentrations declined rapidly (t1/2 = 34.3 h) versus SCN− (t1/2 = 359 h, 15 days) and ATCA (t1/2 = 544 h, 23 days). CN instability in postmortem blood increased at RT (t1/2 = 10.7 h) and HBT (t1/2 = 6.6 h). SCN− and ATCA were more stable than CN at all storage conditions. In postmortem swine, the t1/2s of SCN− and ATCA were 15 and 23 days, respectively. While both the t1/2s of SCN− and ATCA were relatively lengthy, endogenous levels of SCN− were much more variable than ATCA.
Conclusion
While there are still questions to be answered, ATCA was the most adept forensic marker of CN poisoning (i.e., ATCA produced the longest half-life, the largest increase above baseline levels, and most stable background concentrations).
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Cyanide (HCN(g), HCN(aq), and CN− all inclusively represented herein as CN) is a potent lethal chemical agent due to its toxic characteristic profile (i.e., CN inhibits cellular respiration and blocks the electron transport chain of cytochrome c oxidase) [1,2,3,4,5,6]. Because of its toxicity, ease of use, and ready availability (e.g., approximately 750,000 tons of CN is produced annually for extensive industrial applications in the U.S.) [7, 8], CN has been commonly used as a poison. In cases of CN poisoning, the determination of the cause of death has long been recognized as a significant and continuing problem in the field of forensic toxicology [2, 6, 9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24].
CN poisoning can occur through various routes of exposure, such as inhalation, ingestion, or skin contact [2, 7, 8, 23, 25,26,27]. The clinical symptoms of CN poisoning (e.g., chest pain, confusion, dizziness, eye pain, difficulty breathing, headache, abdominal cramping, nausea, rapid or slow heart rate, rapid or slow breathing, restlessness, shortness of breath, vomiting, weakness, and wheezing) are generally nonspecific, and often mimic other common illnesses such as flu or food poisoning [2, 4, 5, 7, 8, 23, 25, 26]. Therefore, CN poisoning can be easily confused with other medical conditions or causes of toxicity or death [19, 25, 28,29,30]. More specific indicators of CN poisoning are a “bitter almond” odor from the victim and pink lividity (i.e., a pinkish or rosy skin discoloration during postmortem examination). These indicators may help investigators identify CN-related fatalities but are difficult to identify, may rapidly disappear, and may be difficult to detect for certain individuals [2, 23, 26, 27, 31]. For example, pink lividity can arise from alternative conditions such as carbon monoxide poisoning. In addition, the olfactory smell of bitter almonds is contingent upon highly variable circumstances, including the quantity of CN present and its metabolic breakdown. It is also estimated that only 60% of people can recognize the “bitter almond” smell of CN [22, 30, 32,33,34,35,36]. Because of the nature of CN poisoning, it is often not immediately apparent to investigators that CN may have been utilized. Consequently, the collection and/or analysis of blood samples, which can serve as crucial evidence, is typically delayed until there is a growing suspicion of cyanide involvement [37, 38]. The duration of this delay can vary significantly, ranging from a few days to several weeks before samples are finally secured for analysis [31, 38, 39]. In addition, even if collection of blood is done immediately, it may not be analyzed for days, and in the interim, may be stored under non-ideal conditions.
While it is possible to directly analyze CN from biological samples in an attempt to verify CN poisoning, it is difficult to use CN as a biomarker in all but the earliest times following exposure [2, 27, 40]. This is because CN is highly unstable in biological matrices due to its chemical characteristics, including reactivity, volatility, and active metabolism of CN by normal biological processes. CN readily participates in certain reactions due to its nucleophilic nature. CN can bind tightly to iron and other metals and reacts readily with disulfides and thiol moieties in biological molecules [2, 10, 27]. The volatility of CN is another factor contributing to its loss from biological samples. CN exists predominantly as HCN(aq) under biological conditions (pKa = 9.3 under standard conditions, and 9.2 at 37 °C). If blood samples are not properly handled and stored, HCN(aq) can quickly off gas from the sample [2, 3, 10, 27, 41]. Aside from its chemical reactivity and volatility, CN is metabolized efficiently by the human body [i.e., the half-life (t1/2) of CN in humans ≈ 20–60 min]. This rapid metabolism and chemical reactivity often return CN to background levels quickly [2, 27, 42]. If there is either an extended postmortem period before collection of samples or inadequate/prolonged storage before analysis, CN concentrations will likely decrease considerably, potentially back to baseline [2, 27, 43]. Another problem inherent in CN determination is the presence of small (<10 µM), but ubiquitous, endogenous concentrations in biological samples. These CN concentrations are present based on diet and natural metabolic processes [2, 4]. Therefore, to link CN poisoning to toxicity or death, blood concentrations of CN must be significantly elevated above background levels. Overall, the chemical and biological characteristics of CN make its direct use as an indicator of CN poisoning challenging unless blood samples are gathered, properly stored, and analyzed soon after exposure, which is not possible in most cases [2, 38].
An alternative to analyzing CN directly is to analyze its metabolites, thiocyanate (SCN−) and 2-aminothiazoline-4-carboxylic acid (ATCA), as biomarkers of CN poisoning (Fig. 1) [2, 39, 40]. SCN−, the major metabolic product of CN, accounts for approximately 80% of CN metabolism [44,45,46]. It is formed through a rhodanese-catalyzed reaction of CN with a sulfur donor, such as thiosulfate. Compared to CN, SCN− is approximately 200 times less toxic and exhibits a longer half-life (t1/2 ≈ 96–192 h), making it a more persistent biomarker for CN exposure [2, 3, 5]. However, while SCN− offers the advantages of abundance and stability, there are significant limitations for its use as a biomarker for CN exposure mainly due to its large and highly variable background concentrations [2,3,4, 27]. Notably, SCN− is naturally present in common food sources and can arise from biological processes unrelated to CN metabolism [1, 2, 40]. Consequently, elevated levels of SCN− may not result from CN poisoning and do not necessarily correlate with CN toxicity, especially under uncontrolled conditions [2, 4, 5, 32, 39, 47]. Therefore, distinguishing between elevated SCN− concentrations due to CN exposure versus other natural sources is challenging. While SCN− can be valuable in conjunction with blood CN concentrations and clinical symptoms, it has not been proven effective as a useful biomarker of CN exposure.

Characteristics of the biomarkers of CN exposure for forensic analysis. Dashed lines separate characteristics which are advantages (above the dashed line) and disadvantages for use of the biomarker for forensic purposes
The in vivo conversion of cyanide to ATCA (Fig. 1), via direct reaction of CN with cystine, was initially reported by Wood and Cooley. [48] ATCA is a marker of CN exposure which is generally stable under almost all storage conditions and has low background concentrations in biological fluids [2, 32]. ATCA accounts for only a small amount of CN metabolism, but the concentration of ATCA is directly proportional to CN concentrations [2, 32, 39]. Moreover, besides the cyanide-mediated pathway, no other endogenous pathways for ATCA production within the human body have been identified [27, 32, 39, 49]. Extended studies of ATCA stability in biological samples have shown remarkable preservation of ATCA concentrations for prolonged periods at all temperatures tested [2, 27, 49]. Consequently, ATCA has garnered significant attention as a promising biomarker for forensic determination of CN poisoning.
While evidence is mounting that ATCA may be a highly stable and reliable marker of CN exposure, the stability of ATCA in biological samples has only been evaluated under controlled storage conditions, which may not be similar to postmortem decay. Therefore, the objective of this study was to determine if ATCA is valuable as a marker to verify CN poisoning under typical situations where blood samples are not immediately obtained and/or analysis is delayed. In addition, the behavior of CN and SCN− was also evaluated. By examining these biomarkers in parallel, our study aimed to directly assess their interrelationships, offering valuable insights into their dynamics and their advantages and disadvantages as indicators of CN poisoning under the identical conditions.
Experimental
Materials
Reagents
All reagents used in this study were of analytical standard grade. The solvents, HPLC-grade methanol (MeOH), phosphoric acid (H3PO4, 85%), ammonium hydroxide (NH4OH, 29% by weight), LC–MS-grade and HPLC-grade acetonitrile (ACN), formic acid (CH2O2, 98%), and ammonium acetate (C2H3O2NH4) were purchased from Fisher Scientific (Fair Lawn, NJ, USA). Potassium cyanide (KCN), sodium hydroxide (NaOH), sulfuric acid (H2SO4), potassium dihydrogen phosphate (KH2PO4), and dibasic potassium phosphate (K2HPO4) were purchased from Fisher Scientific (Hanover Park, IL). Potassium thiocyanate (KSCN) was purchased from Acros Organics (Morris Plains, NJ, USA). 2,3-Naphthalene dialdehyde (NDA) was obtained from TCI America (Portland, OR). 2-Aminoethane sulfonic acid (taurine) and sodium metaborate tetrahydrate (NaBO2·4H2O) were purchased from Alfa Aesar (Ward Hill, MA). Monobromobimane (MBB) was purchased from Fluka Analytical through Sigma-Aldrich (St. Louis, MO, USA). Ellman's reagent (5,5′-dithiobis-2-nitrobenzoic acid) was obtained from Thermo Scientific (Hanover Park, IL, USA). Isotopically labeled internal standards, NaS13C15N and Na13C15N, were acquired from Isotech (Miamisburg, OH, USA). The ATCA internal standard (C313CH615N2O2S; ATCA-13C,15N2) was obtained from Toronto Research Chemical, Inc. (North York, Canada). The mixed-mode cation-exchange sorbent (Oasis-MCX®) was purchased from Waters Corporation (Milford, MA, United States). Ammonium formate (NH4HCO2) was purchased from Sigma-Aldrich (St. Louis, MO, USA). Pyrrolidine was purchased from Acros Organics (Morris Plains, NJ, USA). Purified water with a resistivity of 18.2 MΩ-cm was obtained using a water PRO PS polisher from Labconco (Kansas City, KS, USA).
Standard solutions
Phosphate borate buffer (0.01 M; pH 8.0) and NaOH (0.01 M) were prepared in deionized water and placed into a plastic bottle and stored on the benchtop. A solution of H2SO4 (2 M) was prepared using deionized water and ethanol and was kept at room temperature for storage. A stock solution of NDA (0.002 M) was prepared in a phosphate/borate buffer (0.01 M; pH 8.0) along with 40% methanol. NDA was dissolved completely in methanol before adding the buffer to ensure proper dissolution, transferred to an amber vial, and stored at room temperature, where it was stored for up to 6 months. A taurine solution (0.1 M) was prepared in phosphate/borate buffer (0.01 M; pH 8.0) and stored for up to 3 months at room temperature. An Ellman’s reagent solution (0.01 M) was prepared in ethanol, pyrrolidine solution (0.01 M) was prepared in deionized water, and an MBB solution (0.04 M) was prepared phosphate/borate buffer (in 0.01 M; pH 8.0). These solutions were stored at 4 °C in the dark up to 3 months, 2 weeks, and 4 days, respectively. NH4OH (5%) was prepared from NH4OH (29%) and diluted with MeOH. ATCA-13C, 15N2 was prepared and diluted in methanol to produce a 50 µM standard. Ammonium acetate (0.005 and 0.03 M) was prepared in deionized water. These solutions were stored at 4 °C. KCN and KSCN stock solutions (10 mM each) were prepared in 10 mM NaOH and diluted into a 1 mM mixture of KCN and KSCN with 10 mM of aqueous NaOH. The obtained mixture was diluted to the desired working concentrations with 10 mM aqueous NaOH for all standards. The calibration standards for CN and SCN− were prepared at concentrations of 10–500 µM and 5–200 µM, respectively. The calibration standards for ATCA were prepared and at concentrations of 30–300 µM. Prior to use, the working standard solutions for CN, SCN−, and ATCA were prepared by diluting the suitable stock solutions with swine postmortem blood to achieve the desired concentrations.
Caution: It is crucial to be aware that CN poses a significant risk to both humans and animals due to its highly toxic nature. Therefore, handling CN solids and solutions requires utmost care and caution. When solutions fall below a pH of about 10 (i.e., pKa of CN is 9.2), CN is released as HCN(g). To prevent this potentially hazardous situation, all aqueous standards containing CN were prepared in a 10 mM NaOH solution, ensuring the non-volatile state of CN. Furthermore, all CN solutions were exclusively handled within a well-ventilated hood.
Methods
CN exposures
Note: The animals used for this study were control animals used in a separate research study for the evaluation of a potential next-generation cyanide antidote. Our study utilized blood samples from these animals to add value to the drug development study under ethical principles of maximizing the utility of existing samples and minimizing the need for additional animal use.
Blood samples from eight pigs (Species: Sus scrofa; Breed: Yorkshire cross; Weight: 45–55 kg) were obtained at the Department of Emergency Medicine at the University of Colorado (Anschutz Medical Campus, Aurora, CO). Before CN exposure, blood samples were drawn to establish a baseline (“zero”) time point. Pigs were then exposed to intravenous CN at 0.2 mg/kg/min and after meeting euthanization criteria, were euthanized with sodium pentobarbital. Two pigs (Pigs 2 and 8) met euthanasia criteria earlier, at 40 and 38 min following CN exposure, respectively. Previous cyanide toxicity studies demonstrated that a sustained mean arterial blood pressure of less than 30 mmHg for 10 min is terminal. Animals meeting this criteria were euthanized. All other animals were euthanized after a 90-min observation period. Heparin (10,000 units) was administered in an attempt to limit coagulation of the animal’s blood postmortem. Following euthanasia, animals were transferred to a walk-in cold room where they were stored at 4 °C to obtain blood samples. Blood samples were collected from a central venous catheter placed in the external jugular as follows: the catheter was flushed with 5 mL normal saline to clear the catheter, 10 mL of blood was collected and discarded to minimize the potential for contamination of the sample, then a 3-mL blood sample was collected for analysis. Following blood collection, the jugular catheter was flushed with 10 mL of normal saline followed by 3 mL of heparin to prevent clotting within the catheter. Blood samples were collected into heparinized blood collection tubes at 1, 2, 4, 24, 48, 72, 120, and 168 h after death, where possible. Despite heparinization, clotting blood blocked most catheters before the end of the experiment. Table 1 shows the blood samples collected for each pig and the N value at each time point. Following collection, blood samples were flash-frozen in liquid nitrogen, stored in a –80 °C freezer, and then shipped on dry ice to South Dakota State University. Upon receipt, all blood samples were stored at −80 °C until analyzed.
All animals were cared for in compliance with the “Principles of Laboratory Animal Care” formulated by the National Society for Medical Research and the “Guide for the Care and Use of Laboratory Animals” prepared by the National Institutes of Health (National Academic Press, 1996). The University of Colorado's Institutional Animal Care and Use Committee (IACUC) approved the CN exposure study which complied with the regulations and guidelines of the Animal Welfare Act and the American Association for Accreditation of Laboratory Animal Care.
Preparation of CN and SCN− for analysis
Postmortem blood samples were prepared for HPLC–MS/MS analysis of CN and SCN− following the established method developed by Alluhayb et al. [50] where detailed instructions and additional information can be found. Briefly describing the method, the blood samples were thawed at room temperature, vortexed for 1 min, and centrifuged at 3600×g (Sorvall™ Legend™ X1 Centrifuge with TX-400 Rotor Adapter, Thermo Scientific™) prior to analysis. Postmortem blood (100 μL of control or sample) was obtained and subsequently spiked with a Na13C15N and NaS13C15N mixed internal standard solution (500 μM each, 10 μL). After thorough vortexing, the blood sample was divided into two portions for CN (25 μL) and SCN− (75 μL) sample preparation.
Cyanide was prepared for analysis using active microdiffusion. Reagent solutions (200 µL each) containing NDA (2 mM), taurine (100 mM), and pyrrolidine (10 mM) were added to the reagent chamber of a two-chamber sample preparation cartridge. Postmortem blood (25 µL) was added to the sample chamber and diluted with 50 µL of water. Aqueous H2SO4 (200 µL) was added to the sample chamber. The sample and reagent chambers were sealed, and air was passed through the sample chamber into the capture chamber. This facilitated the transfer of HCN(g) to the capture solution. Within the capture chamber, the CN reacted with NDA and taurine to form a CN-NDA-taurine complex. For SCN−, postmortem blood (75 µL) was treated with ACN (1000 μL) to precipitate proteins. After vortexing for 1 min and centrifugation for 10 min (−5 °C) at 16,700xg (Sorvall™ Legend™ Micro 21R Microcentrifuge with 24 × 1.5/2.0 mL Rotor with ClickSeal™ Biocontainment Lid, Thermo Scientific™), the supernatant (750 μL) was transferred and dried. The dried sample was reconstituted with 10 mM aqueous ammonium formate (75 μL). Ellman’s reagent (10 mM, 50 μL) was added to react with free thiols, followed by vortex mixing. Subsequently, MBB (4 mM, 50 μL) was added to form the SCN-bimane complex.
The prepared CN and SCN− solutions, 550 μL of the CN capture chamber solution and 175 μL of the prepared SCN− solution, were combined for subsequent HPLC–MS/MS analysis in a 4-mL glass screw top vial. The mixture was then filtered through a 0.22-μm polytetrafluoroethylene (PTFE) filter into a 150-μL glass insert for follow-on HPLC–MS/MS analysis.
Note that multiple species of cyanide exist. CN is used in this manuscript to denote any and all cyanide species (i.e., including CN−(aq), HCN(aq), and HCN(g)). This is done because cyanide speciation is complex where CN− exists in blood and urine, but with the pH of blood (approximately 7.2) and the pKa of HCN(aq) (approximately 9.2), HCN(aq) is the dominant form of “free” cyanide [i.e., in a simple aqueous system, over 99% of the cyanide exists as HCN(aq)]. While HCN(aq) is the predominant species in solution, cyanide can also be protein bound (i.e., it reacts with cysteine residues), it can be bound to hemoglobin and can react with glutathione, and there may be microenvironments where the pH is higher and cyanide may exist as CN-. Since the blood is acidified during the sample preparation, the method here detects a combination of all the cyanide species.
Preparation of ATCA for analysis
Postmortem blood samples were prepared for HPLC–MS/MS analysis of ATCA following the established method of Giebułtowicz et al. [49] with slight modifications. Briefly, the blood samples were thawed, vortexed, and centrifuged at 3600×g prior to analysis. Postmortem blood (100 µL of control or sample) was placed in an Eppendorf test tube and mixed with DI water (100 µL) for 1 min by hand, followed by 3 min of vortexing. Cold ACN (750 µL) was added, vortexed for 2 min, and placed in a freezer for 20 min at –20 °C. Then the sample was centrifuged for 5 min at 16,700xg. Subsequently, the supernatant (800 µL), H3PO4 (85%, 20 µL), ATCA-13C, 15N2 (100 µM, 50 µL), and ACN (130 µL) were combined in a separate Eppendorf test tube containing solid MCX sorbent (10 mg). The mixture was then placed on a laboratory shaker for 5 min. The sorbent was washed separately with ACN (1 mL) and ammonium acetate (500 µL of 0.03 M), with vortexing for 1 min and centrifugation for 5 min at 16,700xg after each wash. Subsequently, NH4OH (5%, 500 µL) was added and vortexed for 30 min to elute the ATCA from the MCX sorbent. The supernatant (450 µL) was transferred to a glass test tube and evaporated to dryness using a nitrogen stream at 40 °C. The sample was then reconstituted with ACN (350 µL) and ammonium acetate (0.005M, 15 µL) and transferred to an HPLC–MS/MS vial for analysis.
HPLC–MS/MS conditions for analysis of CN, SCN−, and ATCA
Prepared samples were analyzed using a Shimadzu HPLC (LC20AD, Shimadzu Corp., Kyotu, Japan) coupled with an AB Sciex Q-trap 5500 triple quadrupole mass spectrometer (Applied Biosystems, Foster City, CA, USA) to detect CBI (N-substituted 1-cyano [f] benzoisoindole) and SCN-bimane using negative ionization, and ATCA using positive ionization. Data acquisition and peak integration for analytes were carried out using Analyst™ software 1.4.1. (Framingham, MA, USA).
For CBI and SCN-bimane, HPLC was conducted with a ZORBAX RRHT Eclipse Plus C18 column (100 mm × 3.0 mm, 1.8 μm, 95 Å) protected by a ZORBAX RRHD Eclipse Plus C18 UHPLC guard column (5 mm × 3.0 mm, 1.8 μm, 95 Å) (both from Agilent Technologies, California, USA). For the separation of CBI and SCN-bimane, a gradient of 10 mM ammonium formate in water (Mobile phase A) and 10 mM ammonium formate in methanol (Mobile phase B) was used. The details of the method, including MS parameters, are given in Alluhayb et al. [50].
For ATCA, an Atlantis Premier BEH Z-HILIC Column (50 mm × 2.1 mm, 5 µm) (Waters Corporation, Milford, MA) was used. The mobile phases consisted of HPLC-grade water with 0.1% formic acid as eluent A and acetonitrile with 0.1% formic acid as eluent B at a flow rate of 0.5 mL/min and 40 °C. Detailed MS parameters are given in Giebułtowicz et al. [49].
Stability kinetics
Kinetic parameters were assessed using the methodologies established and detailed by the World Health Organization and Shargel et al. [51, 52]. The concentration–time curves were utilized to calculate the elimination half-life (t1/2) and the elimination constants (Ke) through extrapolation. To determine the ratio Cmax/Cbaseline, the maximum blood concentration was divided by the endogenous (baseline) concentration.
Stability of CN, SCN−, and ATCA in sampled postmortem blood
To evaluate the stability of CN, SCN−, and ATCA in postmortem blood under potentially important conditions for forensic analysis, we stored aliquots of the 2-h postmortem blood sample at room temperature (RT) and typical human body temperature (HBT) and measured CN, SCN−, and ATCA immediately following, and 1, 2, 4, 8, 12, 24, 48, 72, 120, 168, and 240 h (10 days) of storage. The stability of the biomarkers of CN was calculated as a percentage of the initial concentration of the respective analyte.
Results
Pigs in the study were exposed to a potentially lethal concentration of CN and were euthanized either when they met approved criteria or after a 90-min observation period. Following this CN exposure, the initial postmortem blood sample, obtained 1 h postmortem, showed dramatic escalations of blood concentrations of CN and its metabolites compared to background in postmortem swine samples. Specifically, CN's half-life (t1/2) was observed to be 34.3 h, indicating a rapid decline in concentration postmortem. In contrast, SCN− (t1/2 = 359 h, 15 days) and ATCA (t1/2 = 544 h, 23 days) demonstrated significantly greater stability.
The pattern of instability in CN was accentuated under varying storage temperatures. At room temperature (RT, 25 °C), CN’s half-life (t1/2) was reduced to 10.7 h, and at human body temperature (HBT, 37 °C), it declined further to 6.6 h. This resulted in CN concentrations falling below baseline levels within 50, 74, and 120 h for postmortem swine stored at 4 °C, and in postmortem blood at RT and HBT, respectively. Conversely, SCN− and ATCA exhibited far greater stability under these conditions. For postmortem swine, SCN−’s half-life (t1/2) was 15 days, and ATCA’s was 23 days. For blood stored at RT and HBT, SCN−’s half-lives (t1/2s) were 18–19 days, and ATCA’s were 24–27 days.
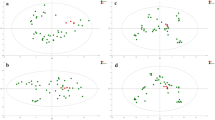
Figure 2 in the study presents the stability of CN, SCN−, and ATCA in postmortem CN-exposed swine under these different conditions, differentiating storage at RT and HBT. Error bars in the figure represent the standard error of mean (± SEM) for each set of measurements (N = 8). Table 2 provides detailed stability and kinetic parameters for CN, SCN−, and ATCA in postmortem blood of CN-exposed pigs stored at 4 °C and in postmortem swine blood stored at RT and HBT. It includes environment-specific half-lives and the ratios of the initial concentration 1 h postmortem (C1h) to the background concentrations (Cbackground) for each biomarker.

The stability of CN, SCN−, and ATCA in postmortem CN-exposed swine. The circles connected via solid lines represent the stability of these compounds in postmortem pigs. Blood stored at room temperature (25 °C) is indicated by triangles and dash lines, while blood stored at a typical body temperature (37 °C) is shown by squares connected by dotted lines. Error bars represent standard error of mean (±SEM) (N = 8)
Discussion
Stability of CN, SCN−, and ATCA in postmortem CN-exposed pigs
Following CN exposure, the initial postmortem blood sample, obtained 1 h postmortem, showed dramatic escalations of blood concentrations of CN and its metabolites compared to background. Table 2 lists the ratios of the initial concentration of each CN biomarker (i.e., 1 h postmortem blood) compared to its respective background concentration (C1h:Cbackground) (i.e., concentrations from antemortem blood collected from the same animal prior to CN exposure). The C1h:Cbackground ratio decreases from ATCA > CN > SCN−. Therefore, ATCA is the most elevated marker of CN exposure compared to its background concentration even though SCN− has the highest absolute blood concentration at this time. A higher C1h:Cbackground ratio is advantageous for use as a marker of CN exposure since it is easier to differentiate elevated levels from background concentrations. The C1h:Cbackground ratio for SCN− is approximately five times lower than for ATCA because of the relatively high background concentrations of SCN−. The high background concentrations of SCN− were expected based mainly on dietary exposure to SCN−. While the increase for all markers of CN exposure at 1 h could be interpreted as evidence that each of these markers could be used to confirm acute exposure to lethal CN concentrations, it is important to note that the conditions in this study were ideal for preserving forensic information. These conditions include animals housed under controlled conditions (including a controlled diet), known background concentrations of each marker for each animal, immediate storage of animals at 4 °C following euthanasia, and deliberate handling of blood samples with immediate freezing and subsequent storage at −80 °C until analysis. In a more realistic situation, a victim’s diet is not controlled, the background concentrations of these biomarkers are not available, and it is unlikely that blood samples are immediately gathered and properly stored. It should be noted that CN drops below its background concentrations at 120 h. This is likely because generation of CN from diet or normal metabolism has ceased, and redistribution occurs postmortem.
Following the immediate sharp rise in the concentration of CN, it relatively rapidly decreases to baseline levels by 120 h, whereas ATCA and SCN− exhibit a steady, slow, decrease in the postmortem swine over the course of the experiment, maintaining well above the initial blood concentration. As shown in Figs. 2, S1A, and S2A, CN decreased markedly faster than SCN− and ATCA, producing the lowest t1/2 = 34.3 h of the markers of CN exposure (Table 2 and Figure S2A). The rapid decrease in CN concentration is consistent with multiple other studies which also observe a rapid decrease in CN concentrations in blood under a variety of storage conditions [53,54,55,56,57,58]. The inherent instability of CN is problematic for its use as a forensic biomarker of CN poisoning.
The alternative markers of CN exposure analyzed in this study, SCN− and ATCA, showed more stability versus CN in postmortem pigs, but the half-life of ATCA (t1/2 = 544.3, h = 23 d) was nearly double that of SCN− (t1/2 = 326.4, h = 15 d) (Table 2 and Fig. S2A). The increased stability of SCN− and ATCA is advantageous for forensic purposes, allowing for a longer window-of-opportunity to verify if the cause of death is CN poisoning. Therefore, because ATCA is the most stable marker of CN poisoning, it is more advantageous for forensic purposes, especially if ideal conditions cannot be achieved.
Stability of CN, SCN−, and ATCA in postmortem blood at elevated temperatures
Under more typical circumstances of CN poisoning, deceased victims would not be immediately transitioned to cold storage (4 °C). In addition, the time between a poisoning event and cooled storage may be lengthy and/or cooled storage may not even occur. Therefore, the postmortem stability of CN, SCN−, and ATCA in victims of CN poisoning at RT and HBT is of interest. Figure 2 shows the stability of CN, SCN−, and ATCA in 2 h postmortem blood samples of CN-exposed pigs stored at RT (dashed lines) and HBT (dotted lines) over 10 days (240 h). CN exhibited pronounced instability at these temperatures, measured as a rapid decrease in CN concentrations with near complete elimination by 74 h, as illustrated in Fig. 2, S1B, S1C, and S2C. The stability of CN in postmortem blood at RT and HBT is much lower than in postmortem swine stored at 4 °C. The t1/2s of CN at RT and HBT (Table 2 and Figure S2B and C) show the rapid degradation of CN in postmortem blood at elevated temperatures. Compared to postmortem swine at 4 °C, postmortem blood produces a 3× and 5× decrease in t1/2 for RT and HBT, respectively.
The stability of SCN− and ATCA in postmortem blood (at RT and HBT) was much higher than CN (Figs. 2, S1B, and S1C). To quantify this relationship, the t1/2s for each biomarker and storage condition pair are reported in Table 2. The t1/2s for SCN− and ATCA are approximately 40× and 53× higher than CN at RT, respectively, and 68× and 99× higher than CN at HBT for SCN− and ATCA, respectively. In a real-world scenario, where ideal conditions are rare, this study indicates that ATCA and SCN− offer more persistent markers of CN poisoning, with ATCA being about 1.5× more stable than SCN−.
ATCA is a reliable postmortem biomarker of CN poisoning
The relatively low stability of CN in postmortem CN-exposed pigs and in postmortem blood at RT and HBT presents a major problem for direct analysis of CN as a marker of CN poisoning. Specifically, CN concentrations rapidly declined, particularly at RT and HBT. The rapid degradation of CN can lead to challenges in forensic analyses, particularly when trying to ascertain whether an individual was exposed to lethal concentrations of CN. The inherent instability of CN not only affects its potential as a consistent marker but also casts a shadow on the reliability of forensic analysis of CN when CN poisoning is suspected as a cause of death. Thus, if direct analysis of CN is to be used for this purpose, immediate sample collection, proper storage, and timely analysis are imperative to ensure trustworthy forensic information.
The degradation behavior of SCN− and ATCA was comparable under the conditions tested, but ATCA was about 1.5× more stable. Although SCN− can be considered to have acceptable stability, the major disadvantage of SCN− for forensic analysis is its high and variable endogenous concentrations (i.e., SCN− produced the highest background concentrations but the most variable). Elevated concentrations of SCN− relative to CN and ATCA are based on efficient metabolism of CN and SCN− consumed via diet. The dependence of background concentrations of SCN− on diet is disadvantageous since it is more difficult to determine if elevated SCN− concentrations are produced from CN exposure. Further, while the absolute concentrations of SCN− following CN exposure were the largest in this study (Fig. 2), the increase in SCN− relative to its baseline concentration was small compared to CN and ATCA (Table 2). Factors such as age, health, genetics, and gut microbiota also influence the conversion of CN to SCN−, leading to increased variability among individuals. Therefore, SCN− suffers from large and variable background concentrations and limited increase relative to its respective background concentration. Therefore, while SCN− can be a valuable marker for assessing CN exposure in the context of other evidence, elevated concentrations are likely not conclusive evidence of CN poisoning under most conditions.
2-Aminothiazoline-4-carboxylic acid demonstrated the slowest elimination dynamics among the three analytes, maintaining concentrations nearest the initial postmortem swine blood draw (1 h) throughout the study (10 days) while it was the most stable marker, it still decreased over time under all study conditions. This decrease is likely be due to redistribution of ATCA following death or changes in the postmortem blood matrix. Regardless of the time elapsed and inherent postmortem blood transformation over time, ATCA levels remain remarkably consistent. This distinguishes it from CN and SCN−, which can show more significant degradation. Moreover, the large increase in ATCA above background levels is advantageous for forensic purposes, providing a longer runway to confidently determine elevated levels of ATCA. Based on its properties of detectability, stability, and relative increase directly related to CN exposure, ATCA can be used as a forensic marker to verify CN exposure.
While this study answered an important question in the field of forensic analysis related to CN poisoning, there are other questions important to definitely answer: (1) “Is ATCA the most advantageous marker when blood is obtained from the heart (i.e., the heart is a common location to draw blood postmortem)?,” (2) “Is ATCA the most appropriate marker when death from CN poising is delayed (i.e., when active metabolism of ATCA occurs over a significant amount of time)?,” and (3) “What effect would tissue decay have on the postmortem concentrations of ATCA?.” There have been studies that shed light on question 2, such as Bhandari et al., [3] which showed ATCA tracked CN concentrations, producing a t1/2 of only 40.7 and 13.9 min in rabbits and swine, respectively. ATCA concentrations decline faster when metabolism is active because it is excreted through normal metabolic pathways. Overall, active metabolism directly impacts the persistence of ATCA. Therefore, confirmation of ATCA’s behavior during active metabolism must be considered. For question 3, our study did not address the effect of biological decay on the behavior of CN, SCN−, or ATCA. For example, after death, CN can continue to be produced due to various biological processes [41, 55, 59,60,61,62,63]. This postmortem production of CN could lead to formation of ATCA in the presence of cysteine. If this process is common, ATCA measured in postmortem blood may not necessarily originate from CN poisoning. Future research is needed to address these questions to solidify the situations where the use of ATCA as a forensic biomarker for cyanide exposure in forensic investigations is appropriate.
Conclusion and future work
The findings of this study highlight the advantages of ATCA as a biomarker of CN poisoning based on its relative stability in postmortem pigs at 4 °C and in postmortem blood at RT and HBT. ATCA demonstrated the slowest elimination and produced a high C1h:Cbackground ratio. The slow and predictable decline of ATCA over extended intervals provides a long window-of-opportunity to detect ATCA above background levels during postmortem analysis of blood from suspected CN poisoning victims, particularly in real-world scenarios, where ideal conditions are rare. Given its pronounced postmortem stability, ATCA emerged as the best candidate for use as a biomarker of CN poisoning.
References
Jackson R, Oda RP, Bhandari RK, Mahon SB, Brenner M, Rockwood GA, Logue BA (2014) Development of a fluorescence-based sensor for rapid diagnosis of cyanide exposure. Anal Chem 86(3):1845–1852. https://doi.org/10.1021/ac403846s
Logue BA, Hinkens DM, Baskin SI, Rockwood GA (2010) The analysis of cyanide and its breakdown products in biological samples. Crit Rev Anal Chem 40(2):122–147. https://doi.org/10.1080/10408340903535315
Bhandari RK, Oda RP, Petrikovics I, Thompson DE, Brenner M, Mahon SB, Logue BA (2014) Cyanide toxicokinetics: the behavior of cyanide, thiocyanate and 2-amino-2-thiazoline-4-carboxylic acid in multiple animal models. J Anal Toxicol 38(4):218–225. https://doi.org/10.1093/jat/bku020
Bhandari RK, Manandhar E, Oda RP, Rockwood GA, Logue BA (2014) Simultaneous high-performance liquid chromatography-tandem mass spectrometry (HPLC-MS-MS) analysis of cyanide and thiocyanate from swine plasma. Anal Bioanal Chem 406(3):727–734. https://doi.org/10.1007/s00216-013-7536-3
Bhandari RK, Oda RP, Youso SL, Petrikovics I, Bebarta VS, Rockwood GA, Logue BA (2012) Simultaneous determination of cyanide and thiocyanate in plasma by chemical ionization gas chromatography mass-spectrometry (CI-GC-MS). Anal Bioanal Chem 404(8):2287–2294. https://doi.org/10.1007/s00216-012-6360-5
Nishio T, Toukairin Y, Hoshi T, Arai T, Nogami M (2022) Assessment of blood 2-aminothiazoline-4-carboxylic acid concentrations: age and sex differences, and correlation with carboxyhemoglobin in fire victims. Legal Med 59:102111. https://doi.org/10.1016/j.legalmed.2022.102111
Chalela JA, Burnett WT (2012) Chemical terrorism for the intensivist. Mil Med 177(5):495–500. https://doi.org/10.7205/MILMED-D-11-00363
Jones KR (2008) Hydroxocobalamin (Cyanokit): a new antidote for cyanide toxicity. Adv Emerg Nurs J 30(2):112–121. https://doi.org/10.1097/01.tme.0000319922.66978.96
Sundermann TR, Schmitt G, Bartel M (2021) Modified congener analysis: Quantification of cyanide in whole blood, other body fluids, and diverse beverages. Drug Test Anal 13(2):412–418. https://doi.org/10.1002/dta.2927
Lindsay AE, Greenbaum AR, O’Hare D (2004) Analytical techniques for cyanide in blood and published blood cyanide concentrations from healthy subjects and fire victims. Anal Chim Acta 511(2):185–195. https://doi.org/10.1016/j.aca.2004.02.006
Nishio T, Toukairin Y, Hoshi T, Arai T, Nogami M (2023) Quantification of cyanide metabolite 2-aminothiazoline-4-carboxylic acid in postmortem dried blood spot samples by liquid chromatography–tandem mass spectrometry. J Chromatogr B 1215:123580. https://doi.org/10.1016/j.jchromb.2022.123580
Hung DZ, Tsan YT, Yu YJ, Hsu CL (2009) Cyanide poisoning in Taiwan. Lancet 374(9696):1212. https://doi.org/10.1016/S0140-6736(09)61033-3
Peddy SB, Rigby MR, Shaffner DH (2006) Acute cyanide poisoning. Pediatr Crit Care Med 7(1):79–82. https://doi.org/10.1097/01.PCC.0000192508.92993.D1
Chin RG, Calderon Y (2000) Acute cyanide poisoning: a case report. J Emerg Med 18(4):441–445. https://doi.org/10.1016/S0736-4679(00)00161-X
Abeyasinghe NL, Perera HJM, Weerasinghe DSK (2011) Case report–death by subcutaneous injection of cyanide in Sri Lanka. J Forensic Legal Med 18(4):182–183. https://doi.org/10.1016/j.jflm.2011.02.010
Le Garff E, Delannoy Y, Mesli V, Allorge D, Hédouin V, Tournel G (2016) Cyanide suicide after deep web shopping: a case report. Am J Forensic Med Pathol 37(3):194–197. https://doi.org/10.1097/paf.0000000000000241
Harmon E, Lebin J, Murphy D, Watsjold B (2019) Fatality from potassium gold cyanide poisoning. BMJ Case Rep 12(7):e229947. https://doi.org/10.1136/bcr-2019-229947
Lee SK, Rhee JS, Yum HS (2012) Cyanide poisoning deaths detected at the national forensic service headquarters in Seoul of Korea: a six-year survey (2005∼2010). Toxicol Res 28(3):195–199. https://doi.org/10.5487/TR.2012.28.3.195
Hendry-Hofer TB, Ng PC, Witeof AE, Mahon SB, Brenner M, Boss GR, Bebarta VS (2019) A review on ingested cyanide: risks, clinical presentation, diagnostics, and treatment challenges. J Med Toxicol 15:128–133. https://doi.org/10.1007/s13181-018-0688-y
Lee J, Mahon SB, Mukai D, Burney T, Katebian BS, Chan A, Bebarta VS, Yoon D, Boss GR, Brenner M (2016) The vitamin B12 analog cobinamide is an effective antidote for oral cyanide poisoning. J Med Toxicol 12:370–379. https://doi.org/10.1007/s13181-016-0566-4
Yan P, Huang G, Li D, Li L (2012) Homicide due to intravenous metallic mercury injection followed by sodium cyanide injection. Am J Forensic Med Pathol 33(3):273–275. https://doi.org/10.1097/paf.0b013e318221b693
Parker-Cote JL, Rizer J, Vakkalanka JP, Rege SV, Holstege CP (2018) Challenges in the diagnosis of acute cyanide poisoning. Clin Toxicol 56(7):609–617. https://doi.org/10.1080/15563650.2018.1435886
Eckstein M (2008) Enhancing public health preparedness for a terrorist attack involving cyanide. J Emerg Med 35(1):59–65. https://doi.org/10.1016/j.jemermed.2007.03.040
Tusiewicz K, Wachełko O, Zawadzki M, Szpot P (2023) The stability of cyanide in human biological samples. A systematic review, meta-analysis and determination of cyanide (GC-QqQ-MS/MS) in an authentic casework 7 years after fatal intoxication. Toxicol Mech Methods 34(3):271–282. https://doi.org/10.1080/15376516.2023.2280212
Bhattacharya R, Flora SJ (2009) Cyanide toxicity and its treatment. In: Gupta RC (ed) Handbook of toxicology of chemical warfare agents. Elsevier, Amsterdam, pp 255–270. https://doi.org/10.1016/B978-0-12-374484-5.00019-5
Shafi H, Subhani A, Imran M, Watoo SA, Sarwar M, Saeed-ul-Hassan S, Latif A, Ashiq MZ, Tahir MA, Tahir AM (2015) Determination of cyanide in biological and non-biological matrices by headspace gas chromatography coupled to flame-ionization detector. Arab J Forensic Sci Forensic Med 230(1856):1–6. https://doi.org/10.12816/0011256
Logue BA, Hinkens DM (2008) The analysis of cyanide and its metabolites in biological samples. Chemistry and Biochemistry Faculty Publications. 39. Open PRAIRIE, South Dakota State University
Anseeuw K, Delvau N, Burillo-Putze G, De Iaco F, Geldner G, Holmström P, Lambert Y, Sabbe M (2013) Cyanide poisoning by fire smoke inhalation: a European expert consensus. Eur J Emerg Med 20(1):2–9. https://doi.org/10.1097/mej.0b013e328357170b
Petrikovics I, Thompson DE, Rockwood GA, Logue BA, Martin S, Jayanna P, Yu JC (2011) Organ-distribution of the metabolite 2-aminothiazoline-4-carboxylic acid in a rat model following cyanide exposure. Biomarkers 16(8):686–690. https://doi.org/10.3109/1354750X.2011.626528
Jorn CC, Martin S, Nasr J, Stafford K, Thompson D, Petrikovics I (2012) LC-MS/MS analysis of 2-aminothiazoline-4-carboxylic acid as a forensic biomarker for cyanide poisoning. World J Methodol 2(5):33. https://doi.org/10.5662/wjm.v2.i5.33
Gill JR, Marker E, Stajic M (2004) Suicide by cyanide: 17 deaths. J Forensic Sci 49(4):JFS2003278. https://doi.org/10.1520/jfs2003278
Musshoff F, Schmidt P, Daldrup T, Madea B (2002) Cyanide fatalities: case studies of four suicides and one homicide. Am J Forensic Med Pathol 23(4):315–320. https://doi.org/10.1097/00000433-200212000-00002
Brown KS, Robinette RR (1967) No simple pattern of inheritance in ability to smell solutions of cyanide. Nature 215(5099):406–408. https://doi.org/10.1038/215406b0
Fernando GC, Busuttil A (1991) Cyanide ingestion: case studies of four suicides. Am J Forensic Med Pathol 12(3):241–246. https://doi.org/10.1097/00000433-199109000-00014
Gambaro V, Arnoldi S, Casagni E, Dell’Acqua L, Pecoraro C, Froldi R (2007) Blood cyanide determination in two cases of fatal intoxication: comparison between headspace gas chromatography and a spectrophotometric method. J Forensic Sci 52(6):1401–1404. https://doi.org/10.1111/j.1556-4029.2007.00570.x
Zuccarello P, Carnazza G, Raffino C, Barbera N (2022) Diagnosis of lethal cyanide poisoning. Analysis by anion-exchange chromatography with pulsed amperometric detection. J Forensic Sci 67(4):1617–1623. https://doi.org/10.1111/1556-4029.15046
Li SY, Petrikovics I, Yu J (2019) The potential use of 2-aminothiazoline-4-carboxylic acid (ATCA) as a forensic marker for cyanide exposure in medicolegal death investigation: a review. Forensic Sci Rev 31(1):45–58
Jackson R, Logue BA (2017) A review of rapid and field-portable analytical techniques for the diagnosis of cyanide exposure. Anal Chim Acta 960:18–39. https://doi.org/10.1016/j.aca.2016.12.039
Yu JCC, Mozayani A (2015) Medicolegal and forensic factors in cyanide poisoning. In: Hall AH, Isom GE, Rockwood GA (eds) Toxicology of cyanides and cyanogens: experimental, applied and clinical aspects. John Wiley and Sons, Hoboken, pp 276–282. https://doi.org/10.1002/9781118628966.ch20
Ma J, Dasgupta PK (2010) Recent developments in cyanide detection: a review. Anal Chim Acta 673(2):117–125. https://doi.org/10.1016/j.aca.2010.05.042
Nelson L (2006) Acute cyanide toxicity: mechanisms and manifestations. J Emerg Nurs 32(4):S8–S11. https://doi.org/10.1016/j.jen.2006.05.012
Bortey-Sam N, Jackson R, Gyamfi OA, Bhadra S, Freeman C, Mahon SB, Brenner M, Rockwood GA, Logue BA (2020) Diagnosis of cyanide poisoning using an automated, field-portable sensor for rapid analysis of blood cyanide concentrations. Anal Chim Acta 1098:125–132. https://doi.org/10.1016/j.aca.2019.11.034
Paul BD, Smith ML (2006) Cyanide and thiocyanate in human saliva by gas chromatography-mass spectrometry. J Anal Toxicol 30(8):511–515. https://doi.org/10.1093/jat/30.8.511
Luo PJ, Yu YX, Wu D, Li XT, Dai CJ, Chen XF, Li GL, Wu YN (2019) Simultaneous determination of cyanide and thiocyanate in swine plasma by high-performance liquid chromatography with fluorescence detection based on a novel D–π–A carbazole-based turn-on fluorescence labeling reagent. Anal Methods 11(23):2983–2990. https://doi.org/10.1039/c9ay00784a
Youso SL, Rockwood GA, Logue BA (2012) The analysis of protein-bound thiocyanate in plasma of smokers and non-smokers as a marker of cyanide exposure. J Anal Toxicol 36(4):265–269. https://doi.org/10.1093/jat/bks017
Wood JL, Cooley SL (1956) Detoxication of cyanide by cystine. J Biol Chem 218(1):449–457. https://doi.org/10.1016/s0021-9258(18)65908-3
Giebułtowicz J, Sobiech M, Rużycka M, Luliński P (2019) Theoretical and experimental approach to hydrophilic interaction dispersive solid-phase extraction of 2-aminothiazoline-4-carboxylic acid from human post-mortem blood. J Chromatogr A 1587:61–72. https://doi.org/10.1016/j.chroma.2018.12.028
Alluhayb AH, Severance C, Hendry-Hofer T, Bebarta VS, Logue BA (2023) Concurrent determination of cyanide and thiocyanate in human and swine antemortem and postmortem blood by high-performance liquid chromatography–tandem mass spectrometry. Anal Bioanal Chem 415(26):6595–6609. https://doi.org/10.1007/s00216-023-04939-6
Goulding R (1986) Environmental Health Criteria 57 Principles of Toxicokinetic Studies. World Health Orgnization, Geneva. https://doi.org/10.1177/146642408610600642
Shargel L, Andrew BC, Wu-Pong S (1999) Applied biopharmaceutics and pharmacokinetics. Appleton and Lange Reviews/McGraw-Hill, Medical Pub, Stamford New York
Moriya F, Hashimoto Y (2001) Potential for error when assessing blood cyanide concentrations in fire victims. J Forensic Sci 46(6):1421–1425. https://doi.org/10.1520/jfs15165j
Chikasue F, Yashiki M, Kojima T, Miyazaki T, Okamoto I, Ohtani M, Kodama K (1988) Cyanide distribution in five fatal cyanide poisonings and the effect of storage conditions on cyanide concentration in tissue. Forensic Sci Int 38(3–4):173–183. https://doi.org/10.1016/0379-0738(88)90164-8
McAllister JL, Roby RJ, Levine B, Purser D (2008) Stability of cyanide in cadavers and in postmortem stored tissue specimens: a review. J Anal Toxicol 32(8):612–620. https://doi.org/10.1093/jat/32.8.612
Ballantyne B (1976) Changes in blood cyanide as a function of storage time and temperature. J Forensic Sci Soc 16(4):305–310. https://doi.org/10.1016/s0015-7368(76)71077-6
Moriya F, Hashimoto Y (2003) Chemical factors affecting the interpretation of blood cyanide concentrations in fire victims. Legal Med 5:S113–S117. https://doi.org/10.1016/s1344-6223(02)00079-2
Ferrino-McAllister JL (2010) Fire victim blood cyanide stability and the development of a cyanide uptake model. ProQuest Dissertations and Theses Global, University of Maryland Baltimore.
Kala M, Chudzikiewicz E (2003) The influence of post-mortem changes in biological material on interpretation of toxicological analysis results. Probl Forensic Sci 54:32–59
Lokan RJ, James RA, Dymock RB (1987) Apparent post-mortem production of high levels of cyanide in blood. J Forensic Sci Soc 27(4):253–259. https://doi.org/10.1016/s0015-7368(87)72754-6
Karhunen PJ, Lukkari I, Vuori E (1991) High cyanide level in a homicide victim burned after death: evidence of post-mortem diffusion. Forensic Sci Int 49(2):179–183. https://doi.org/10.1016/0379-0738(91)90077-v
Noguchi TT, Eng JJ, Klatt EC (1988) Significance of cyanide in medicolegal investigations involving fires. Am J Forensic Med Pathol 9(4):304–309. https://doi.org/10.1097/00000433-198812000-00007
Catanese C (2016) Color atlas of forensic medicine and pathology. Taylor and Francis, Boca Raton Florida
De Matteis M, Giorgetti A, Viel G, Giraudo C, Terranova C, Lupi A, Fais P, Puggioni A, Cecchetto G, Montisci M (2021) Homicide and concealment of the corpse. Autopsy case series and review of the literature. Int J Legal Med 135:193–205. https://doi.org/10.1007/s00414-020-02313-0
Gentile G, Galante N, Tambuzzi S, Zoja R (2021) A forensic analysis on 53 cases of complex suicides and one complicated assessed at the Bureau of Legal Medicine of Milan (Italy). Forensic Sci Int 319:110662. https://doi.org/10.1016/j.forsciint.2020.110662
Acknowledgements
We gratefully acknowledge the support of CounterACT Program, the support of the office of Neurological Disorders and Stroke (NINDS) of the National Institutes of Health under award number R44NS97066-01A1, and the support of the SD Board of Regents. Furthermore, the HPLC–MS/MS instrument used in this work was supported by the U.S. Joint Executive Office for Chem Bio Defense, Joint Program Management-Protection contract W911SR-09-C-0059. The opinions, assertions, findings, and conclusions or recommendations expressed herein are solely those of the authors and do not necessarily reflect the official views of the NIH, the State of South Dakota, the University of Colorado, and Seacoast Science, Inc.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
All animals were cared for in compliance with the “Principles of Laboratory Animal Care” formulated by the National Society for Medical Research and the “Guide for the Care and Use of Laboratory Animals” prepared by the National Institutes of Health (National Academic Press, 1996). The University of Colorado's Institutional Animal Care and Use Committee (IACUC) approved the CN exposure study (ethics committee: Carter Severance, Genna Nault, Tara Hendry-Hofer, Nathan Wetmore). It complied with the regulations and guidelines of the Animal Welfare Act and the American Association for Accreditation of Laboratory Animal Care.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Alluhayb, A.H., Severance, C., Hendry-Hofer, T. et al. Can the cyanide metabolite, 2-aminothiazoline-4-carboxylic acid, be used for forensic verification of cyanide poisoning?. Forensic Toxicol (2024). https://doi.org/10.1007/s11419-024-00690-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11419-024-00690-4