
Abstract
Significant regional variability in lifespan in Europe is influenced by environmental factors and lifestyle behaviors, including diet. This study investigates the impact of geographical region on the lifespan of European rulers spanning from the fourteenth century to the present day. By analyzing historical records and literature, we aim to identify region-specific dietary patterns and lifestyle factors that may have contributed to longer lifespans among rulers. The hypothesis to be tested is that rulers from Southern European countries, where the traditional Mediterranean diet is consumed by the local people, may exhibit longer lifespans compared to rulers from other regions, due to the well-documented health benefits associated with this dietary pattern. We extracted comprehensive information for each ruler, encompassing their sex, birth and death dates, age, age of enthronement, duration of rulership, country, and cause of death (natural vs. non-natural). To determine their nationality, we coded rulers based on their hypothetical present-day residence (2023). Utilizing the EuroVoc Geographical classification, we categorized the countries into four regions: Northern, Western, Southern, Central and Eastern Europe. While Cox regression models did not find significant differences in survival rates among regions, further analysis stratified by time periods revealed intriguing trends. Contrary to our initial predictions, the Northern region displayed better survival rates compared to the Southern region between 1354 and 1499, whereas survival rates were similar across regions from 1500 to 1749. However, after 1750, all regions, except the Southern region, exhibited significantly improved survival rates, suggesting advancements in healthcare and lifestyle factors. These findings underscore the dynamic influence of both region and time period on health and longevity. Interestingly, despite the prevalence of the Mediterranean diet in the Southern region of Europe, rulers from this region did not demonstrate longer lifespans compared to their counterparts in other regions. This suggests that additional lifestyle factors may have played a more prominent role in their longevity. In conclusion, our study sheds light on the intricate relationship between region, time period, and lifespan among European rulers. Although the Mediterranean diet is often associated with health benefits, our findings indicate that it alone may not account for differences in ruler longevity across regions. Further research is warranted to explore the impact of other lifestyle factors on the health and lifespan of European rulers throughout history.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Research suggests that there may be regional variation in the rate of aging, with some populations aging more slowly than others [1]. An important example is the significant lifespan variation in Europe, with some countries boasting longer life expectancies than others. While genetic factors may play a role, environmental factors such as access to healthcare, socioeconomic status, and lifestyle behaviors also have a significant impact on the rate of aging and thereby lifespan. In modern times, countries in Northern Europe, such as Iceland and Norway, tend to have longer lifespans than countries in Eastern Europe [2]. Additionally, recent studies have found that income inequality and poverty can have a significant impact on the rate of aging and lifespan, with individuals living in poverty aging more unsuccessfully and having shorter lifespans than those with higher incomes [3]. Understanding lifespan variation in Europe is crucial for developing effective public health policies and interventions aimed at improving overall health outcomes and reducing premature mortality. By identifying the factors that contribute to healthier aging and longer lifespans in the populations of certain countries, policymakers and health professionals can work to implement strategies to promote healthier behaviors and improve health outcomes in countries with shorter lifespans.
There are different methods to elucidate the mechanisms underlying lifespan variation, including genetic, epidemiological, and demographic studies. By utilizing these various approaches, researchers can gain a better understanding of the complex factors that contribute to differences in lifespan across populations. Analyzing historical data, such as birth and death records, can provide insights into the mechanisms underlying lifespan variation in Europe, such as the impact of region-specific lifestyle factors on mortality rates. Historical data can also help identify trends and patterns in lifespan over time, which can inform public health policies and interventions aimed at promoting healthy aging.
Diet is one of several lifestyle factors that may contribute to regional variation in lifespan, with certain dietary patterns, such as the Mediterranean diet, associated with a reduced risk of chronic age-associated diseases [4], including ischemic heart disease, stroke, vascular cognitive impairment, type 2 diabetes, and certain types of cancer [5]. Therefore, understanding the relationship between regional variation in diet and life expectancy can provide important insights into the health of populations in different regions.
In this study, we aim to investigate regional variation in the lifespan of European rulers throughout history by analyzing the documented longevity of kings and other rulers. Through this analysis, we hope to uncover historical trends in regional variation of lifespan and shed light on the relationship between region-specific lifestyle factors, such as regional cuisine and life expectancy. Analyzing the lifespans of rulers from different regions and time periods is a valuable tool for exploring the potential impact of diet and other region-specific lifestyle factors on lifespan because this information is often available in historical records. Birth and death records of commoners are typically not available or are incomplete, making it difficult to study the lifespan of the general population over longer time periods. Importantly, this approach also removes socioeconomic factors from the analysis. As rulers throughout history had access to the best available food and medical care, independent of their countries’ economic background, their lifespan can provide insight into the potential impact of diet on longevity, independent of other socioeconomic factors.
Our hypothesis is that rulers of Southern European countries, where the traditional Mediterranean diet is consumed, may have longer lifespans than rulers from other regions due to the well-documented health benefits of this diet [6]. The Mediterranean diet, which is rich in plant-based foods, fish, and healthy fats, has been linked to a reduced risk of chronic age-associated diseases and improved overall health outcomes, according to previous research [5,6,7,8]. In addition, we aimed to test our hypothesis that rulers of Northern countries, where diets high in saturated fats are more common and ingredients of the Mediterranean diet are not readily available, may exhibit reduced life expectancy. To explore this hypothesis, we conducted a detailed analysis of the lifespans of European rulers from different geographic regions throughout history.
Methods
Population
To gather our data on European rulers, we utilized various online sources, including Wikipedia. While some may question the accuracy of such sources, studies have shown that the science entries on Wikipedia are nearly as reliable as traditional sources like the Encyclopedia Britannica [9, 10]. To ensure the validity of our data, we cross-referenced our population of rulers with the dynastic tables found in Morby’s Dynasties of the World (2002) [11]. We began our data collection with rulers who were already in power by 1354, a year marked by the devastation of the Black Death across Europe between 1346 and 1353, which often caused rulers to succumb to infection [12]. Our data collection continued until the last ruler of a country that ceased to be a monarchy or the first ruler still alive if the country remained a monarchy. We limited our analysis to European rulers to maintain consistency in our sample population.
Variables
We extracted various kinds of information for each ruler, including their sex, birth and death date, age, age of enthronement, duration of rulership, country, and cause of death (natural vs. non-natural death). The definition of non-natural death included the deaths caused by unexpected events, poisoning, accidents, murders, execution, or war. If we did not have any specific information regarding the cause of death, we assumed a natural death occurred. To ensure the accuracy of our data, deaths were coded separately by two investigators, and in case of disagreement, consensus was reached through discussion. We also coded the nationality of each ruler based on where they would have lived at the present day (2023). If a ruler governed in more than one country or moved to another country, their nationality was coded according to where they lived the longest. Finally, we classified the countries into the following regions based on the EuroVoc Geographical classification: Northern, Western, Southern, Central and Eastern Europe (as shown in Fig. 1) [13].

Classification of European sub-regions based on EuroVoc, with country borders representing the divisions as of 2023
Statistical analysis
Normal distribution of continuous variables was tested with Shapiro-Wilk test. As continuous variables followed a non-normal distribution, Kruskal-Wallis tests were used to compare continuous variables (age, age of enthronement, and duration of rule) among regions. Cox-regression models were created for natural vs. non-natural death as outcome and age as follow-up. Only those participants were included in the analysis who reached at least age 40, the approximate life expectancy up until the twentieth century [14, 15]. Since the Mediterranean diet is often associated with health benefits [6], we used the Southern region as reference in all our analyses. Popes (n = 59) and Doges of Venice (n = 67) were excluded from the Southern region, as they were significantly older when first elected, and thus would have led to bias. The popes and Doges of Venice stood out with a mean age of enthronement at 64 and 70, and a mean age of 70 and 77, respectively, indicating significantly better survival rates than rulers in other regions. For comparison, the mean age of enthronement and mean age for rest of the rulers in the Southern region was 27 and 57, respectively (Table 1 and Fig. 2). In the regression models, covariates included birth year and region. Birth year was centered around 1700. Linear and quadratic time terms were also introduced in the regression models. Additional analyses were conducted for three time periods: 1354–1499, 1500–1749, and 1750+. From the regression models, rate ratios (RRs) and 95% confidence intervals were calculated. Finally, Kaplan-Meier curves were plotted showing how survival changed over the three time periods by region, and how survival of every region compared to each other over the three time periods. Statistical significance was set at p < 0.05. All statistics were conducted in SPSS 24. Kaplan-Meier survival curves were constructed using R (“survminer” package).

Kaplan-Meier survival curves for rulers in the Southern region, as well as for popes and Doges of Venice. The x-axis shows survival after age 40, while the y-axis displays the survival probability
Results
We identified a total of 863 European rulers, excluding Popes and Doges of Venice. Of these, 190 were excluded because they died before the age of 40, resulting in a final sample of 673 rulers from the four regions: Northern (n = 57), Eastern, and Central European (n = 76), Western (n = 377), and Southern (n = 166). A total of 582 rulers died of natural causes, while 91 were recorded as non-natural death. The earliest born ruler in our sample was Luigi Gonzaga, born in 1268, and the latest ruler added was Elizabeth II, who passed away in 2022. The majority of the rulers in our sample were male (92%). We observed significant differences in age among the regions, but age of enthronement and duration of rule were similar across regions (Table 2). Cox regression analysis showed that hazards did not differ significantly from the Southern Region (Table 2), and these findings were supported by the Kaplan-Meier curves (Fig. 3).

Kaplan-Meier survival curves for all rulers grouped by region. The x-axis represents survival after age 40, while the y-axis displays the probability of survival
When we stratified our analysis by time periods, we found that age of rulers and age of enthronement were similar across regions from 1354 to 1749, but differed significantly after 1750. Duration of rule was similar across all three time periods. Within the Western and Northern regions, age of rulers and age of enthronement significantly increased over time, while they remained stable in the Southern and Central and Eastern European regions. Duration of rule significantly decreased over time in the Southern and Western regions but remained stable in the other two regions (Table 3). Cox regression analysis showed that from 1354 to 1499, the Northern region had significantly better survival compared to the Southern region (RR: 0.48; 95% CI: 0.28–0.84), but survival did not differ significantly from the reference between 1500 and 1749. After 1750, the Western (RR: 0.44; 95% CI: 0.28–0.68), Northern (RR: 0.39; 95% CI: 0.20–0.76), and Central and Eastern European (RR: 0.52; 95% CI: 0.28-0.98) regions all exhibited better survival than the Southern region (Table 4). These findings were supported by the Kaplan-Meier curves (Fig. 4). When we examined each region separately, we found that survival of rulers in the Southern region was stable over all three time periods. In the Northern region, survival initially declined between 1500 and 1749 and then increased, while in both the Western and Central and Eastern European regions, survival increased prominently only after 1750 (Fig. 5).

Comparison of Kaplan-Meier survival curves for regions by time periods

Changes in survival rates for each region over three distinct time periods. Each line represents a different region, and the x-axis shows the timeline. The y-axis displays the survival rate, indicating the proportion of rulers who survived until a specific age. The three time periods are: 1354–1499, 1500–1749, and after 1750. The graph provides a visual representation of how survival rates have changed over time in each region and how the regions compare to one another
Discussion
The results of our analysis provide insight into the survival rates of European rulers across different regions and time periods. While our Cox regression models did not find significant differences in survival rates among regions, further analysis stratified by time periods revealed interesting trends. Contrary to our prediction, the Northern region exhibited significantly better survival rates compared to the Southern region between 1354 and 1499. In contrast, survival rates were similar among regions between 1500 and 1749, indicating that health and longevity may have become more evenly distributed across Europe during that time. However, after 1750, all regions except the Southern region exhibited significantly better survival rates, suggesting possible improvements in healthcare and lifestyle factors that benefited European rulers in those regions. These findings are further supported by the Kaplan-Meier curves, which illustrate how survival rates varied across regions and time periods. The relatively high survival rates of the Northern region between 1354 and 1499 followed by a decline between 1500 and 1749 and subsequent increase after 1750 is particularly noteworthy, as it illustrates that regional differences in health and longevity of elites can be dynamic and subject to change over time. Overall, our findings highlighted the influence of region and time period on health and longevity. The results of our investigation extend the findings of previous studies examining the lifespan of European royalty, indicating a significant increase in life expectancy from 800 to 1800, independent of the decline in violent deaths [16]. Interestingly, these studies revealed a gradient in the lifespan of the European elite society, with longer lifespans observed from south to north and from east to west [16].
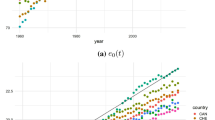
These gradients partially still exist today; however, the east-to-west gradient is stronger than the south-to-north one for life expectancy at birth [2]. The highest life expectancy at birth in Europe (2020) is observed in Norway (83.3 years) and Switzerland (83.1), while the lowest is found in Romania (74.2) and Bulgaria (73.6) [17]. If we examine smaller geographic regions, the highest life expectancy can be observed in French Corsica (84), the Balearic Islands in Spain (83,9), and in the Epirus region of Greece (83.8), while the lowest is found in the North-West Region of Bulgaria (72.1) [17].
Some of these present-day differences in longevity can be explained by the economic differences, and one of the indicators of these developments is the gross domestic product (GDP) value of the different countries. GDP shows a strong correlation with life expectancy [18]. In 2020, Norway had the highest GDP per capita (68,850 USD) followed by Switzerland (60,040 USD), whereas the lowest was found in Albania (3810 USD) and North Macedonia (4100 USD) [19]. Socioeconomic differences and inequalities in Europe affect the health of the population directly [20]. However, it is interesting to note that the correlation between GDP and life expectancy is not linear. For example, in both Greece and the Netherlands, the life expectancy at birth approximates 81.4 years, while the GDP per capita of the Netherlands is twice as high as it is in Greece [2, 19]. The same is true for Germany and Portugal too [2, 19].
Apart from GDP, lifestyle factors, such as smoking, physical activity, and diet, also influence longevity and may be responsible for the regional differences in life expectancy. In modern times, smoking is one of the most important health-related risk factors that also negatively impacts longevity [21]. According to the Eurostat in 2019, the countries with the highest proportion of daily smokers were Bulgaria (28.7%), Greece (23.6%), Latvia (22.1%), Germany (21.9%), and Croatia (21.8%). Meanwhile, the lowest smoking prevalence was observed in Sweden (6.4%), Finland (9,9%), Luxembourg (10.5%), and Portugal (11.5 %) [22]. Physical activity also plays a pivotal role in healthy lifestyle. In 2022, according to a survey conducted by the European Commission, the physically most active countries were Finland (71%), Luxemburg (63%), and the Netherlands (60%), whereas the highest levels of inactivity were found in Portugal (73%), Greece (68%), and Poland (65%) [23]. In terms of diet, in 2019 the highest fruit and vegetable consumption rates were observed in Italy, Spain, Belgium, and Ireland (more than 75%), while the lowest was found in Latvia and Romania (< 50%) [24].
As we can see from the data, northwest Europe is generally better off in terms of longevity. However, the South, for instance Greece, is also competing with the North and West even with its lower GDP per capita, higher rates of smoking, and less frequent physical activity. In our opinion, this may be partially explained by dietary factors like the Mediterranean diet of the region. This is why we hypothesized that regional variation in diet, particularly the consumption of a Mediterranean diet, is a major determinant of lifespan variation between different European countries based on previous research showing the positive impact of this dietary pattern on health outcomes and the reduced risk of chronic age-related diseases [5].
The Mediterranean diet is a dietary pattern that is traditionally followed in countries located along the Mediterranean Sea, such as Spain, Italy, and Greece in Europe as well as Turkey, Egypt, Tunisia, Morocco, and others [5]. However, it is important to note that there are variations in the specific foods consumed in each country depending on cultural, religious, and economic factors [5]. The Mediterranean diet is characterized by high consumption of fruits, vegetables, whole grains, legumes, nuts, and olive oil, moderate consumption of fish and seafood, low to moderate consumption of dairy products, and low consumption of red meat and processed foods [6]. The Mediterranean diet has been widely studied for its potential anti-aging health benefits, including a reduced risk of chronic age-associated diseases [5, 7] and improved longevity in Greece, Italy, and in the Mediterranean region [5, 7]. Several studies have found that adherence to the Mediterranean diet is associated with a reduced risk of mortality from cardiovascular disease and cancer [5,6,7,8]. There is growing evidence that individual components of the Mediterranean diet exert multifaceted anti-aging effects both in pre-clinical studies and clinical investigations. Resveratrol is a polyphenolic compound that is found in red wine, grapes, and other berries. It has been shown to have anti-inflammatory, antioxidant, and anti-cancer properties [25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41] and may also promote longevity by activating certain enzymes and transcription factors (i.e., SIRT-1 [42], and Nrf2 [43, 44]) that are involved in the regulation of cellular and molecular processes of aging. In addition to resveratrol, several other compounds present in the Mediterranean diet have been shown to exert significant anti-aging effects. One such compound is hydroxytyrosol [45,46,47,48], which is found in high concentrations in extra virgin olive oil. Hydroxytyrosol has been found to exert strong antioxidant effects, which may help to protect against oxidative stress and inflammation. Additionally, flavonoids such as quercetin, which is found in onions, apples, berries, citrus fruits, leafy green vegetables, tomatoes, and broccoli, have also been shown to possess potent antioxidant and anti-inflammatory effects, potentially contributing to the anti-aging effects of the Mediterranean diet [49,50,51].
In this study, we aimed to explore the potential impact of the Mediterranean diet and geographic location on the lifespan of European rulers. By examining the dietary patterns of European rulers from different geographic regions, we hoped to shed light on the potential impact of the Mediterranean diet on longevity and gain a better understanding of the factors that contribute to overall lifespan. Throughout history, the diets of royals have been the subject of fascination and curiosity, as they often reflect not only personal tastes but also cultural and societal norms. In the following sections, we will explore what is known about the royal diets through the centuries, from the medieval times to modern day, and the factors that have influenced their dietary patterns.
Before the New World: 1354–1499
The evolution of nutrition over the centuries has been significant, with royalty having access to the finest ingredients and rarely experiencing hunger [52]. Meals were not only about satisfying hunger but also had social significance for the nobility. A well-laid table, the number of courses, and the composition of the dishes were all regulated by court etiquette. The abundance of food served as an expression of wealth, prosperity, and power, while the feast itself established a clear social hierarchy [52, 53].
The cuisine of a given region is influenced by various factors, including climate and geographic location. For instance, Southern Europe’s natural geography limits food production to lowlands and hilly areas, resulting in a shortage of basic foodstuffs such as cereals but abundant seafood [54]. Near the Mediterranean Sea, viticulture and cultivation of olives were important. In contrast, Central Europe’s temperate climate favored cereal production and animal husbandry [55]. In Western Europe, animal husbandry was a mainstay of the agricultural economy [56]. Barley and wheat were the most important crops in most European regions; oats and rye were also grown, along with a variety of vegetables and fruits. In Iberia, the Arab Agricultural Revolution introduced a large number of new crops, which continued to be cultivated, including sugar cane, rice, citrus, and figs [57]. In the North, agriculture was less sustainable, with scarce arable land mainly used for barley and millet and pastures mainly used for cattle and sheep [58], while animal husbandry, hunting, and fishing were also practiced [59]. Vegetables such as cabbages, onions, peas, and beans were widely cultivated in Europe. In comparison to the Mediterranean region [60], where the dry summer weather limited the availability of animal feed, livestock held greater significance in Northern Europe [61]. The primary farm animals in the Mediterranean were sheep and goats, while in Northern Europe, both cattle and pigs played significant roles.
The economic circumstances played a significant role in shaping the culture and cuisine of these regions. Following the devastating impact of the Black Death between 1346 and 1353, which claimed the lives of at least one-third of Europe’s population, there was a notable shift in food availability [12]. The reduced population meant that the same amount of natural resources was distributed among fewer individuals, resulting in a surplus of food [62]. As a consequence, a wider range of meats became accessible to a larger segment of the population until the sixteenth century, when population growth led to bread once again becoming the dominant component of meals [62]. Another crucial element to consider in the development of regional cuisines is the primary source of fat, which varies based on climate and culture. In different European regions, the usage of oil and butter (or fat) as cooking fats, along with the consumption of beer and wine, played an important role in shaping the culinary traditions. These regional variations reflect the unique agricultural practices and food preferences that emerged in response to the geographical and cultural contexts of each area.
Contrary to our initial prediction, our study found that rulers from regions where the Mediterranean diet was prevalent did not live longer than those from other regions. The underlying reasons for this are likely to be multifaceted and may involve the differences between the dietary habits of the general population and the ruling elite and a complex interplay of genetic, environmental, and lifestyle factors.
While climate and geography do impact the availability and variety of food and the prevalence of the consumption of Mediterranean diets, the cuisine enjoyed by European nobility may have remained relatively consistent throughout the ages in accordance with the fashions of the time and the support of the trade. The ability to consume copious amounts of food and drink was viewed as a demonstration of strength and valor, with meat being a particularly prized ingredient [63]. It was not uncommon for whole roasted animals to be served and carved at the table immediately before consumption [64]. Additionally, smaller animals like lambs and rabbits, or other ingredients like eggs, mushrooms, and vegetables, were often placed inside larger animals like cattle, deer, or pigs and cooked whole [64]. Over time, new ingredients and dishes were introduced, such as sugar and later colonial goods. The quality and quantity of food were indicators of social status and wielded as tools of power and diplomacy, along with the indulgence of pleasures.
The European Middle Age kitchen was greatly influenced by the Roman Empire. The Roman kitchen is relatively well-known thanks to the ancient recipes published by Apicius [65]. The diet of the time contained ingredients, such as fish, wine, herbs, spices, pork, poultry, and bread made with sourdough [65]. Popular vegetables were Brussels sprout, beets, lettuce, onions, cucumbers, asparagus, while commonly consumed fruits were peaches, grapes, apples along with nuts and sweet chestnuts [65].
To gain insight into the diet of the nobility, reports from feasts and cookbooks with recipes of the upper classes provide the best sources [66]. In one of the first cookbooks after antiquity, The Book for Cook (Libro per cuoco) by an unknown author of the mid-1300s, it was evident that Venice was the main hub of the European spice trade, and the nobility there had easy access to a wide variety of luxury spices [66]. For example, recipe LXXIII in The Book for Cook is a mixture of pepper, cinnamon, ginger, cloves, and saffron that was used as a pre-prepared spice mixture ingredient for other recipes [67]. The high consumption of spices and herbs may be explained by two factors. First, they were expensive and a symbol of social status, and second, they were also consumed as a medicine based on the humoral pathological concept of the time [66, 68]. The recipe collections of the fourteenth and fifteenth centuries in Western Europe and Italy were very similar to each other because of the culture of adding spices to everything [66]. The nobility consumed vast amounts of meat seasoned with imported spices along with white bread and delicacies, such as almonds, dates, and luxury products [66].
While there were likely some notable differences in dietary patterns between regions, other factors such as physical activity, high levels of stress from political, personal, or societal pressures, excessive alcohol use and even genetics (e.g., royal families with significant inbreeding) may have had a greater impact on lifespan. These findings highlight the complex interplay between diet and other factors that contribute to overall health and longevity. A possible explanation for the significantly better survival observed for the Northern region — could be that Nordic countries were possibly less engaged in military activities than the other regions in this period. The lower number of conflicts and higher economic stability (e.g., founding of the Kalmar union in 1397 [69]) could have granted a better quality of life for the rulers of the Northern region [70]. Another factor that may explain the better survival of rulers in the Northern region is the lack of malaria at higher altitudes [71, 72], as our database indicates that only Southern and Western rulers were documented to have died of malaria during this time period. Other possible explanations may be linked to infectious diseases. The Scandinavian region was one of the most severely affected region by the Black Death plague that ended in 1353 [73]. The decrease of population resulted in a relative prosperity and an increase in food availability in the coming years [62]. However, it is less likely that this would have directly affected the survival of the rulers in this region, who always had access to sufficient amounts of food regardless of the prosperity of the general population.
The age of exploration and geographic discoveries — transformations in a Brave New World: 1500–1749
Contrary to our prediction, survival rates were similar among regions during the period of exploration and great geographic discoveries from 1500 to 1749. Notably, the Northern rulers’ advantage observed in the previous period disappeared. There could be various reasons for this, including changes in dietary habits, as well as geopolitical changes, conflicts, and weather conditions. For instance, the Northern countries engaged in a higher number of conflicts than before, which could have had a detrimental effect on their economy after the dissolution of the Kalmar Union in 1523 [69]. The Thirty Years’ War had a profound impact on Europe, both in terms of loss of life and destruction of property. Moreover, the Little Ice Age period from the middle of the sixteenth century to the middle of the nineteenth century resulted in a colder climate in the Northern Hemisphere [74]. This led to famine and the death of approximately one-quarter to one-third of the population of Finland in 1696–1697 [62, 75].
During this period, significant changes occurred in the world of cuisine; feasts were still a tool of power and a platform to meet and build agreements. For instance, Cristofor da Messibugo, the steward of the Duke of Ferrara, documented the four courses of the banquet held by the Este family in Ferrara in 1529, which consisted of a wide variety of meat, fish, pastry, fruits, and spices [66, 76]. John Dickie calculated that if the 104 guests ate an equal share of the courses, they would have consumed an astonishing amount of food, including eighteen portions of eleven different fish, three whole birds the size of capons, another five smaller birds, three portions of meat, and four portions of sausage, salami or ham, fifteen small pastries, plus assorted blancmanges, fritters, and salads [66]. The eating habits of influential families like the Spinola family from Genoa were also studied. Frank Spooner compared their eating habits to those of the local hospital and found that while the hospital’s diet was primarily cereal-based (81% of calories were from cereals compared to 53% in the diet of the Spinola family), the Spinola family consumed twice as much meat and three times as much dairy products [62, 77]. Herb and spice consumption began to decline among the nobility during this time period, as spices like black pepper became more accessible and no longer symbolized status. Instead, tea, coffee, tobacco, chocolate, and liquors became the new luxury items. Additionally, a variety of new vegetables and fruits such as artichoke, green peas, green beans, green pepper, and melon started appearing on the rulers’ tables [62]. The explorations and the agricultural revolution also introduced potato, tomato, and corn to meals in the nineteenth and eighteenth centuries [66].
The Industrial Epoch — is knowledge power? After 1750
Our initial prediction was also contradicted by our findings that showed a clear trend of increasing lifespan among rulers in Northern and Western regions after 1750, while the Southern region did not experience a similar improvement in life expectancy. This discrepancy in lifespan trends between regions highlights the need for further investigation into the complex interplay of socioeconomic, environmental, and lifestyle factors that may have contributed to these differences. The striking increases in the lifespan of rulers in the Northern and Western regions after 1750 are particularly noteworthy. In this time period, the Industrial Revolution, which originated in Great Britain, brought several technological advancements that boosted the economy and quality of life in most regions [78]. However, since the Southern region was the last to experience the industrial revolution’s effects, its economy and quality of life may have been adversely affected [79]. The period after 1750 also saw significant advancements in the field of medicine. The discovery of vaccination by Edward Jenner in 1796 was a major breakthrough in the prevention of infectious diseases [80]. The development of anesthesia in the mid-nineteenth century revolutionized surgery and made complex surgical procedures possible [81]. In addition, the discovery of the germ theory by Louis Pasteur in the late nineteenth century paved the way for the development of antibiotics, which have saved countless lives [82]. During the eighteenth and nineteenth centuries, countries in the Western region, including the predecessors of modern France and Germany, the Habsburg Empire and the UK were at the forefront of medical research and practice. It is possible that the advancements in medicine in the Western region during this time period played a role in the longer lifespans of rulers in these areas, as improved medical knowledge and practices may have led to better healthcare for rulers in these societies.
Diet also changed significantly in this time period. From 1600 to 1800, spices continued losing their prominence due to colonization, leading to the emergence of more distinct national culinary traditions [66]. However, the royal taste across Europe remained still quite similar during this time, as noted by John Dickie [66]. Danielle De Vooght argues that “fashions spread from court to court through their continuing contact with each other” [83], supporting the claim that the courts’ food choices were likely homogenous and characterized by excessive consumption of meat, luxurious items, and alcohol. In the eighteenth century, there was a notable disparity between economic development and population growth, leading to occasional food scarcity and starvation among the masses. It took time for the production and consumption ratios to align once again. However, with the advancement of animal husbandry and agriculture, the elimination of fallow land, the implementation of crop rotation involving cereals and legumes, and the introduction of fertilization techniques, along with the spread of new high-yield crops such as rice, maize, and potatoes, a potential famine crisis was averted. Nevertheless, while food supply became more secure, it also became increasingly one-sided and socially differentiated [62]. The diet of the poor became simpler and more limited, with wheat and meat becoming less accessible and being replaced by corn and potatoes. The growth of the population had a negative impact on nutritional culture until the mid-nineteenth century. Initially, the diet of the poor primarily revolved around cereals, but gradually, both quantitative and qualitative changes occurred. The introduction of new cooling and canning techniques towards the end of the nineteenth century, along with improved milling processes that produced cleaner wheat, made white bread more widely available to a larger segment of the population [62]. Technological progress eventually facilitated greater access to meat and bread, resulting in a better and more secure food supply for common people, but the nobility continued to demand more sophisticated and elaborate dishes, turning the dining table into a spectacle focused on representation [62]. Although the economic processes had a limited direct influence on the diet of the nobility, they indirectly impacted the eating habits and supplies found on the tables of nobles across different regions.
Another factor that could contribute to the lower survival rates in the Southern region is the prevalence of poisonings. This region has a long history of poisonings, dating back to the Roman Empire [84,85,86]. Our database indicates that 18 Southern rulers were potentially assassinated by poison, compared to seven Western and four Central European and Eastern rulers, with the possibility that some “natural” deaths were actually caused by hidden poisons.
The last factor that could contribute to the lower survival rates of Southern rulers is the outbreak of infectious diseases. According to Giulio Alfani, the Italian peninsula in the seventeenth century was more susceptible to infectious diseases than other regions [87]. Although outbreaks began decreasing in the eighteenth century Europe [87], they could still have had an impact on the survival rates of royalties both directly and indirectly, by reducing the availability and quality of food and overall quality of life [62]. However, the nobility was often fortunate enough to isolate themselves from outbreaks by retreating to the countryside [88].
European rulers led a markedly distinct lifestyle from that of common folk. Still, they represent a relatively homogenous group who had access to the highest quality and quantity of food and quality health care and are protected from causes of death, such as starvation, war, and infectious diseases related to lack of hygiene and overcrowding, that often decimated the general population. Rulers were probably more similar to each other than the populations they ruled over who may have differed greatly by geographic region and political situation enabling a somewhat more precise estimation of lifespan by geography without having access to potential confounders that may have biased our results if we would have examined the general population without the adjustment for these confounders.
Limitation
One major limitation of our study is the inability to eliminate the influence of immortal time bias. We considered age as the underlying time and only included rulers who were crowned, which meant that rulers were effectively immortal until their coronation. As a result, rulers who were crowned later in life had a distinct advantage over those crowned at a younger age since they had already survived for a longer time and were more likely to live to an older age. A further limitation of our study may be the arbitrary selection of large regions that do not necessarily represent uniform cuisines. Cuisines could differ from country to country within the same region, which may have influenced our results. Moreover, we had no information on the specific diet of individual rulers and whether the Southern rulers truly adapted the Mediterranean diet. A subsequent limiting factor is the accuracy of historical records leading to possible misclassifications for the cause of death. Another limitation is the lack of access to possible confounding factors that can significantly impact lifespan, such as smoking, alcohol consumption, or diseases. Furthermore, we did not take into consideration genetic relations either, which may also play an important factor in longevity, because the common dynastic intermarriages, frequent location changes, and consanguineous marriages make it hard to clearly account for these factors. From a statistical point of view, the Northern and Central and Eastern regions had significantly fewer rulers leading to statistical power issues. We were also not able to examine male and female rulers separately because of the small number of female rulers overall, which may have led to statistical power issues. Finally, our results are not generalizable to the whole population either, as our sample consists of highly privileged individuals that do not reflect the lifestyle of common folks, and the differences observed in our study may be probably contributed to other factors other than diet that we were not able to identify due to lack of information on these variables.
Conclusion
The findings of our study suggest that the lifespan of Southern European rulers was not longer than that of their counterparts in other regions. In fact, after 1750, life expectancy in this area may have been even lower. Our results partially support those of a previous study that found a gradient of longer lifespans for the European elite society from South to North and East to West between 800 and 1800 [16]. However, it should be noted that our regions were quite large, which may have made it difficult to identify subtle differences. Furthermore, life expectancy is influenced by numerous factors apart from nutrition, and it is possible that our results were affected by other variables, such as geopolitical conflicts, outbreaks of infectious diseases, changing residency, regional variability in the level of medical care or the gradual expansion of the Industrial Revolution. It is also important to note that the rulers in Southern Europe may not have followed the Mediterranean diet that has been linked to a lower risk of cardiovascular disease and other chronic illnesses not to mention the possible lacking important socio-cultural aspect of the diet too [7, 8]. Common people were more likely to follow this diet, characterized by high consumption of plant-based foods such as herbs, vegetables, fruits, and pulses, as well as low consumption of red meat and also lived a physically more active lifestyle [6, 7, 66, 89]. In contrast, the cuisine of the courts may have been more similar to each other than different [66, 83], and rulers had access to a wide range of foods that may not have been available to the general population. Therefore, the dietary habits of the rulers in our study may not have been representative of the Mediterranean diet. Other factors, such as protection against physical assault and infectious diseases, economic stability, and access to the best healthcare of the time, may have also played a role in the overall longevity of European rulers. It is possible that these factors offset any differences in diet between the regions and contributed to the lack of apparent differences in our study.
Data availability
Data is available upon request.
References
Pes GM, et al. Diet and longevity in the blue zones: a set-and-forget issue? Maturitas. 2022;164:31–7. https://doi.org/10.1016/j.maturitas.2022.06.004.
Eurostat. Life expectancy by age and sex in 2020. https://ec.europa.eu/eurostat/databrowser/bookmark/e3f138df-5165-4db9-805c-f48ff25d621b?lang=en. Accessed 12 Apr 2023.
Bor J, Cohen GH, Galea S. Population health in an era of rising income inequality: USA, 1980-2015. Lancet. 2017;389(10077):1475–90. https://doi.org/10.1016/s0140-6736(17)30571-8.
You W, et al. Total meat intake is associated with life expectancy: a cross-sectional data analysis of 175 contemporary populations. Int J Gen Med. 2022:1833–51. https://doi.org/10.2147/IJGM.S333004.
Guasch-Ferré M, Willett WC. The Mediterranean diet and health: a comprehensive overview. J Intern Med. 2021;290(3):549–66. https://doi.org/10.1111/joim.13333.
Bach-Faig A, et al. Mediterranean diet pyramid today. Science and cultural updates. Public Health Nutr. 2011;14(12a):2274–84. https://doi.org/10.1017/s1368980011002515.
Keys A, et al. The diet and 15-year death rate in the seven countries study. Am J Epidemiol. 1986;124(6):903–15. https://doi.org/10.1093/oxfordjournals.aje.a114480.
Dinu M, et al. Mediterranean diet and multiple health outcomes: an umbrella review of meta-analyses of observational studies and randomised trials. Eur J Clin Nutr. 2018;72(1):30–43. https://doi.org/10.1038/ejcn.2017.58.
Giles J. Internet encyclopaedias go head to head. Nature. 2005;438(7070):900–1. https://doi.org/10.1038/438900a.
Rosenzweig R. Can history be open source? Wikipedia and thefuture of the past. J Am Hist. 2006;93(1):117–46. https://doi.org/10.2307/4486062.
Morby JE. Dynasties of the world. Oxford: Oxford University Press; 2002.
Benedictow OJ. The black death, 1346-1353: the complete history. Boydell & Brewer; 2004. p. 456.
Publications Office of the European Union - Geographical division of Europe. https://eur-lex.europa.eu/browse/eurovoc.html?params=72,7206,5781#arrow_5781. Accessed 10 Oct 2022.
Lancaster HO. Expectations of life: a study in the demography, statistics, and history of world mortality. Springer Science & Business Media; 2012.
Riley JC. Estimates of regional and global life expectancy, 1800–2001. Popul Dev Rev. 2005;31(3):537–43. https://doi.org/10.1111/j.1728-4457.2005.00083.x.
Cummins N. Lifespans of the European elite, 800–1800. J Econ Hist. 2017;77(2):406–39. https://doi.org/10.1017/S0022050717000468.
Eurostat. Life expectancy across EU regions in 2020. https://ec.europa.eu/eurostat/web/products-eurostat-news/-/ddn-20220427-1. Accessed 12 Apr 2023.
Deaton A. Income, health, and well-being around the world: evidence from the Gallup World Poll. J. Econ. Perspect. 2008;22(2):53–72. https://doi.org/10.1257/jep.22.2.53.
Eurostat. Real GDP per capita of Europe 2020. https://ec.europa.eu/eurostat/databrowser/view/SDG_08_10/bookmark/table?lang=en&bookmarkId=c4de0f60-b965-4cb2-a890-79191b798c28. Accessed 12 Apr 2023.
Hernández-Quevedo C, et al. Socioeconomic inequalities in health: a comparative longitudinal analysis using the European Community Household Panel. Soc Sci Med. 2006;63(5):1246–61. https://doi.org/10.1016/j.socscimed.2006.03.017.
Wynder EL, Graham EA. Tobacco smoking as a possible etiologic factor in bronchiogenic carcinoma; a study of 684 proved cases. J Am Med Assoc. 1950;143(4):329–36. https://doi.org/10.1001/jama.1950.02910390001001.
Eurostat. Daily smokers of the EU 2019. https://ec.europa.eu/eurostat/web/products-eurostat-news/-/edn-20211112-1. Accessed 12 Apr 2023.
Eurostat. Sport and physical activity in the EU - Summary 2022. https://europa.eu/eurobarometer/surveys/detail/2668?fbclid=IwAR35CxWTqmFpwArx-cnPxrzGEi64m1BMoYLKrGDF0HpGVkE0MGJdR0Lje2k. Accessed 12 Apr 2023.
Eurostat. Nutritional habits statistics. https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Nutritional_habits_statistics#Consumption_of_fruit_and_vegetables. Accessed 12 Apr 2023.
Baur JA, et al. Resveratrol improves health and survival of mice on a high-calorie diet. Nature. 2006;444(7117):337–42. https://doi.org/10.1038/nature05354.
Baur JA, Sinclair DA. Therapeutic potential of resveratrol: the in vivo evidence. Nature rev. 2006;5(6):493–506. https://doi.org/10.1038/nrd2060.
Pearson KJ, et al. Resveratrol delays age-related deterioration and mimics transcriptional aspects of dietary restriction without extending life span. Cell Metab. 2008;8(2):157–68. https://doi.org/10.1016/j.cmet.2008.06.011.
Aziz MH, et al. Chemoprevention of skin cancer by grape constituent resveratrol: relevance to human disease? FASEB J. 2005;19(9):1193–5. https://doi.org/10.1096/fj.04-3582fje.
Sale S, et al. Pharmacokinetics in mice and growth-inhibitory properties of the putative cancer chemopreventive agent resveratrol and the synthetic analogue trans 3,4,5,4'-tetramethoxystilbene. Br J Cancer. 2004;90(3):736–44. https://doi.org/10.1038/sj.bjc.6601568.
Signorelli P, Ghidoni R. Resveratrol as an anticancer nutrient: molecular basis, open questions and promises. J Nutr Biochem. 2005;16(8):449–66. https://doi.org/10.1016/j.jnutbio.2005.01.017.
Bernier M, et al. Resveratrol supplementation confers neuroprotection in cortical brain tissue of nonhuman primates fed a high-fat/sucrose diet. Aging (Albany NY). 2016;8(5):899–916. https://doi.org/10.18632/aging.100942.
Csiszar A, et al. Resveratrol prevents monocrotaline-induced pulmonary hypertension in rats. Hypertension. 2009;54(3):668–75. https://doi.org/10.1161/HYPERTENSIONAHA.109.133397.
Csiszar A, et al. Resveratrol induces mitochondrial biogenesis in endothelial cells. Am J Physiol Heart Circ Physiol. 2009. https://doi.org/10.1152/ajpheart.00368.2009.
Csiszar A, et al. Vasoprotective effects of resveratrol and SIRT1: attenuation of cigarette smoke-induced oxidative stress and proinflammatory phenotypic alterations. Am J Physiol Heart Circ Physiol. 2008;294(6):H2721–35. https://doi.org/10.1152/ajpheart.00235.2008.
Csiszar A, et al. Resveratrol attenuates TNF-{alpha}-induced activation of coronary arterial endothelial cells: role of NF-{kappa}B inhibition. Am J Phys. 2006;291(4):H1694–9. https://doi.org/10.1152/ajpheart.00340.2006.
Csiszar A, et al. Age-associated proinflammatory secretory phenotype in vascular smooth muscle cells from the non-human primate Macaca mulatta: reversal by resveratrol treatment. J Gerontol A Biol Sci Med Sci. 2012;67(8):811–20. https://doi.org/10.1093/gerona/glr228.
Mattison JA, et al. Resveratrol prevents high fat/sucrose diet-induced central arterial wall inflammation and stiffening in nonhuman primates. Cell Metab. 2014;20(1):183–90. https://doi.org/10.1016/j.cmet.2014.04.018.
Toth P, et al. Aging exacerbates hypertension-induced cerebral microhemorrhages in mice: role of resveratrol treatment in vasoprotection. Aging Cell. 2015;14(3):400–8. https://doi.org/10.1111/acel.12315.
Toth P, et al. Resveratrol treatment rescues neurovascular coupling in aged mice: role of improved cerebromicrovascular endothelial function and downregulation of NADPH oxidase. Am J Physiol Heart Circ Physiol. 2014;306(3):H299–308. https://doi.org/10.1152/ajpheart.00744.2013.
Ungvari Z, et al. Resveratrol attenuates mitochondrial oxidative stress in coronary arterial endothelial cells. Am J Physiol Heart Circ Physiol. 2009;297(5):H1876–81. https://doi.org/10.1152/ajpheart.00375.2009.
Zhang H, et al. Resveratrol improves endothelial function: role of TNF{alpha} and vascular oxidative stress. Arterioscler Thromb Vasc Biol. 2009;29(8):1164–71. https://doi.org/10.1161/ATVBAHA.109.187146.
Price NL, et al. SIRT1 is required for AMPK activation and the beneficial effects of resveratrol on mitochondrial function. Cell Metab. 2012;15(5):675–90. https://doi.org/10.1016/j.cmet.2012.04.003.
Csiszar A, et al. Resveratrol encapsulated in novel fusogenic liposomes activates Nrf2 and attenuates oxidative stress in cerebromicrovascular endothelial cells from aged rats. J Gerontol A Biol Sci Med Sci. 2014. https://doi.org/10.1093/gerona/glu029.
Ungvari Z, et al. Resveratrol confers endothelial protection via activation of the antioxidant transcription factor Nrf2. Am J Physiol Heart Circ Physiol. 2010;299(1):H18–24. https://doi.org/10.1152/ajpheart.00260.2010.
de Pablos RM, et al. Hydroxytyrosol protects from aging process via AMPK and autophagy; a review of its effects on cancer, metabolic syndrome, osteoporosis, immune-mediated and neurodegenerative diseases. Pharmacol Res. 2019;143:58–72. https://doi.org/10.1016/j.phrs.2019.03.005.
Terracina S, et al. Antioxidant intervention to improve cognition in the aging brain: the example of hydroxytyrosol and resveratrol. Int J Mol Sci. 2022;23(24). https://doi.org/10.3390/ijms232415674.
Boronat A, et al. Cardiovascular benefits of tyrosol and its endogenous conversion into hydroxytyrosol in humans. A randomized, controlled trial. Free Radic Biol Med. 2019;143:471–81. https://doi.org/10.1016/j.freeradbiomed.2019.08.032.
Ikonomidis I, et al. Association of hydroxytyrosol enriched olive oil with vascular function in chronic coronary disease. Eur. J Clin Investig. 2023:e13983. https://doi.org/10.1111/eci.13983.
Kaindl U, et al. The dietary antioxidants resveratrol and quercetin protect cells from exogenous pro-oxidative damage. Food Chem Toxicol. 2008;46(4):1320–6. https://doi.org/10.1016/j.fct.2007.09.002.
Islam MT, et al. Senolytic drugs, dasatinib and quercetin, attenuate adipose tissue inflammation, and ameliorate metabolic function in old age. Aging Cell. 2023;22(2):e13767. https://doi.org/10.1111/acel.13767.
Krzystyniak A, et al. Combination of dasatinib and quercetin improves cognitive abilities in aged male Wistar rats, alleviates inflammation and changes hippocampal synaptic plasticity and histone H3 methylation profile. Aging (Albany NY). 2022;14(2):572–95. https://doi.org/10.18632/aging.203835.
Montanari M, Katalin K. Éhség és bőség: a táplálkozás európai kultúrtörténete / La fame e l’abbondanza. Storia dell’alimentazione in Europa [The culture of food]. Atlantisz; 1999. p. 212.
Ferguson PP. A cultural field in the making: gastronomy in 19th-century France. Am J Sociol. 1998;104(3):597–641. https://doi.org/10.1086/210082.
Pérez-Lloréns JL, Acosta Y, Brun FG. Seafood in Mediterranean countries: a culinary journey through history. Int J Gastron Food Sci. 2021;26:100437.https://doi.org/10.1016/j.ijgfs.2021.100437.
Morin GA. Nations Unies, and Organisation des Nations Unies pour l'alimentation et l'agriculture. UN: Long-term historical changes in the forest resource; 1996.
Cosman MP. Fabulous feasts: medieval cookery and ceremony; 1976. p. 224.
Watson AM. The Arab agricultural revolution and its diffusion, 700–1100. J Econ Hist. 1974;34(1):8–35. https://doi.org/10.1017/S0022050700079602.
Pedersen E, Widgren M. Agriculture in Sweden 800BC to AD 1000. 2011:46–71. https://doi.org/10.2307/jj.919480.
Zvelebil M, Dolukhanov P. The transition to farming in Eastern and Northern Europe. J World Prehist. 1991;5(3):233–78. https://doi.org/10.1007/BF00974991.
Astill GG, Langdon J. Medieval farming and technology: the impact of agricultural change in Northwest Europe, vol. 1. Brill; 1997. p. 312.
Sweeney D. Agriculture in the middle ages: technology, practice, and representation. University of Pennsylvania Press; 2016. p. 416.
Braudel F. A mindennapi élet struktúrái: a lehetséges és a lehetetlen Anyagi kultúra, gazdaság és kapitalizmus, XV–XVIII. század. I. kötet / Civilisation materielle, économie et capitalisme, XVe-XVIIIe siècle. Volume 1, Les structures du quotidien: Le possible et l’ impossible [Civilization and capitalism 15th-18th century, Vol. 1: the structures of everyday life]. Gutta Kiadó; 2004. p. 602.
Katz J. Tradition and crisis: Jewish society at the end of the Middle Ages. Syracuse University Press; 2000. p. 410.
Dembinska M. Food and drink in medieval Poland: rediscovering a cuisine of the past. University of Pennsylvania Press; 1999. p. 256.
Apicius MG. Szakácskönyv a római korból/Marci Gavii Apicii decem libri qui dicuntur de re coquinaria et excerpta a Vinidario conscripta [On the subject of cooking]. Budapest: Enciklopédia; 1996. p. 224.
Dickie J. Delizia!: the epic history of the Italians and their food. Hodder & Stoughton; 2008. p. 420.
Veneziano A. Libro di cucina del sec. XIV a curoe di Ludovico Frati. Livorno; 1899. https://www.mori.bz.it/gastronomia/Anonimo%20Veneziano%20-%20Libro%20di%20cucina.pdf. Accessed 10 June 2022.
Montanari M. Food is culture. Columbia University Press; 2006. p. 168.
Gustafsson H. A state that failed? Scand J Hist. 2006;31(3-4):205–20. https://doi.org/10.1080/03468750600930720.
Rohleder N. Chronic stress and disease. In: Insights to neuroimmune biology. Elsevier; 2016. p. 201–14. https://doi.org/10.1016/B978-0-12-801770-8.00009-4.
CDC (Center for Disease Control and Prevention). Where malaria occurs. https://www.cdc.gov/malaria/about/distribution.html. Accessed 1 Mar 2023.
Boualam MA, et al. Malaria in Europe: a historical perspective. Front Med (Lausanne). 2021;8:691095. https://doi.org/10.3389/fmed.2021.691095.
Jedwab R, Johnson ND, Koyama M. The economic impact of the Black Death. J Econ Lit. 2022;60(1):132–78. https://doi.org/10.1257/jel.20201639.
Mann ME. Little ice age. In: Encyclopedia of global environmental change, vol. 1; 2002. p. 504–9.
Jutikkala E. The great finnish famine in 1696–97. Scand Econ Hist Rev. 1955;3(1):48–63. https://doi.org/10.1080/03585522.1955.10411468.
Messisbugo C. Banchetti compositioni di vivande; 1549. https://books.google.hu/books?id=VSM8AAAAcAAJ&hl=hu&pg=PP5#v=onepage&q&f=false. Accessed 10 June 2022.
Spooner F. Régimes alimentaires d’autrefois. Annales; 1961. p. 568–74. https://www.persee.fr/doc/ahess_0395-2649_1961_num_16_3_3397. Accessed 10 June 2022.
Mason DS. A concise history of modern Europe: liberty, equality, solidarity. Rowman & Littlefield. 2022:257.
Encyclopaedia Britannica, Chmielewski K. A map depicting the spread of the Industrial Revolution through Europe in the 19th century. https://www.britannica.com/summary/Industrial-Revolution-Key-Facts. Accessed 7 Mar 2023.
Riedel S. Edward Jenner and the history of smallpox and vaccination. Proc (Baylor Univ Med Cent). 2005;18(1):21–5. https://doi.org/10.1080/08998280.2005.11928028.
Robinson DH, Toledo AH. Historical development of modern anesthesia. J Investig Surg. 2012;25(3):141–9. https://doi.org/10.3109/08941939.2012.690328.
Smith KA. Louis pasteur, the father of immunology? Front Immunol. 2012;3:68. https://doi.org/10.3389/fimmu.2012.00068.
De Vooght D. Royal taste: food, power and status at the European Courts after 1789. Routledge; 2016. p. 210.
Cilliers L, Retief F. Poisons, poisoning and the drug trade in ancient Rome. Akroterion. 2000;45(1):88–100. https://doi.org/10.7445/45-0-166.
Dash M. Chapter 6 - Aqua Tofana. In: Wexler P, editor. Toxicology in the Middle Ages and Renaissance. Academic Press; 2017. p. 63–9. https://doi.org/10.1016/B978-0-12-809554-6.00006-8.
Karamanou M, et al. Toxicology in the Borgias period: the mystery of Cantarella poison. Toxic Res App. 2018;2:2397847318771126. https://doi.org/10.1177/2397847318771126.
Alfani G. Plague in seventeenth-century Europe and the decline of Italy: an epidemiological hypothesis. Eur Rev Econ Hist. 2013;17(4):408–30. https://doi.org/10.1093/ereh/het013.
Boccaccio G, Witte K. Das Dekameron. Anaconda; 2013.
Riva, B.d., Meraviglie di Milano / Bonvesino dalla Riva ; traduzione dal testo latino, introduzione e commenti del dott. Ettore Verga. 1921: L. F. Cogliati. 160. https://archive.org/details/digitami_CUB0126467/mode/2up. Accessed 10 June 2022.
Funding
Open access funding provided by Semmelweis University. Project no. TKP2021-NKTA-47 has been implemented with the support provided by the Ministry of Innovation and Technology of Hungary from the National Research, Development and Innovation Fund, financed under the TKP2021-NKTA funding scheme. Funding for the project through the National Cardiovascular Laboratory Program (RRF-2.3.1-21-2022-00003) was provided by the Ministry of Innovation and Technology of Hungary from the National Research, Development and Innovation Fund. This work was also supported by grants from the National Institute on Aging (RF1AG072295, R01AG055395, R01AG068295, R01AG070915, and K01AG073614), the National Institute of Neurological Disorders and Stroke (R01NS100782), the National Cancer Institute (R01CA255840), and the Presbyterian Health Foundation.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. Dr. Adam G. Tabak serves as Associate Editor for GeroScience. Dr. Zoltan Ungvari serves as Editor-in-Chief for GeroScience.
Disclaimer
The funding sources had no role in the study design; in the collection, analysis and interpretation of data; in the writing of the report; and in the decision to submit the article for publication. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health, the American Heart Association, or the Presbyterian Health Foundation.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Madarász, B., Fazekas-Pongor, V., Szarvas, Z. et al. Survival and longevity of European rulers: geographical influences and exploring potential factors, including the Mediterranean diet — a historical analysis from 1354 to the twentieth century. GeroScience (2023). https://doi.org/10.1007/s11357-023-00957-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11357-023-00957-5