
Abstract
In this study, we examined the association of fasting serum insulin (FSI) and fasting serum glucose (FSG) with cognitive impairment in the very elderly using a sample of Chinese nonagenarians/centenarians. This study used data from a survey that was conducted in 2005 on all residents aged 90 years or more in a district with 2,311,709 inhabitants. FSG, FSI, and cognitive function were analyzed. The sample included 661 unrelated Chinese individuals (aged 90–108 years; mean, 93.52 ± 3.37 years; 67.17 % women; FSI, 6.27 ± 2.27 mU/mL; FSG levels, 4.46 ± 1.45 mmol/L). The prevalence of cognitive impairment was 61.81 % and that of hypoinsulinemia was 31.92 %. Individuals with hypoinsulinemia showed lower cognitive function scores (14.81 ± 5.79 vs. 15.78 ± 5.24, t = 2.160, P = 0.031). No differences in cognitive function score between different FSI and FSG groups were significant, and no differences in FSI and FSG between individuals with and without cognitive impairment were statistically significant. Unadjusted multiple logistic regressions showed that hypoinsulinemia, impaired fasting glucose, or diabetes did not change the risk of cognitive impairment significantly. In summary, we found that in elderly subjects, cognitive function appeared associated with FSI, and higher FSI may be associated with enhanced cognitive function.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Type 2 diabetes and its related metabolic disorders including hyperinsulinemia, insulin resistance, and hyperglycemia are important conditions in the elderly (Kesavadev et al. 2003). Recent studies have discovered that the insulin metabolic disorders may be one of the important risk factors for Alzheimer’s disease (AD) (Duron and Hanon 2008; Planel et al. 2007). Some researchers have postulated that independent of the effect of glucose, the level of hyperinsulinemia correlates with cognitive decline in the elderly (van den Berg et al. 2006, 2007). However, other researchers have presented evidence showing no relationship between insulin levels and cognitive dysfunction (Kodl and Seaquist 2008; Park 2001; Kern et al. 2001). Thus, the relationship between fasting serum insulin (FSI) and cognitive dysfunction remains unknown (van den Berg et al. 2006, 2007; Kodl and Seaquist 2008; Park 2001; Kern et al. 2001). Several additional studies have shown that impaired fasting glucose and type 2 diabetes and their related metabolic disorders correlate with vascular dementia rather than AD (Craft 2009). The association of cognitive function with FSI and fasting serum glucose (FSG) has been the focus of many researchers, but no definitive conclusion has been generated (van den Berg et al. 2006, 2007; Kodl and Seaquist 2008; Park 2001; Kern et al. 2001). However, although some evidence of the correlation exists, no study has examined long-lived subjects. In this study, we provide evidence from long-lived subjects, which may prove useful in clarifying the association of cognitive function with FSI and FSG. We examine a group of Chinese nonagenarians/centenarians.
Subjects and methods
Study subjects
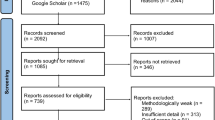
The methods used have been described previously (Zhou et al. 2010; Huang et al. 2009). In brief, a cross-sectional study for age-related diseases was conducted in 870 long-lived subjects (>90 years), which was a part of the Project of Longevity and Aging in Dujiangyan (PLAD) and was based on the Dujiangyan (located in Sichuan Province in southwest China) 2005 census. The PLAD aimed to investigate relationships between the environment, lifestyle, genetics, cognitive function, longevity, and age-related diseases. The basic health of volunteers was examined by trained physicians. Results were entered onto a standard form and included a questionnaire on lifestyles and cognitive function [measured using the 30-item Mini-Mental State Examination (MMSE)]. FSG and FSI were determined using the glucose oxidase method and RIAs, respectively. We excluded those who did not complete the MMSE test or where no information on FSG or FSI was available. Subjects with a previous diagnosis of diabetes (they may have used treatments to influence their FSG, FSI, or insulin resistance (IR)) or receiving diabetes medication were also excluded. Overall, 21 men and 26 women were excluded from the study because they had already died or moved out of the area. Of 262 men and 561 women who were interviewed, 38 men and 124 women did not complete the MMSE test. Those that did not provide FSG or FSI information or those with a previous diagnosis of diabetes did not complete MMSEs. Therefore, the study population ultimately comprised 661 long-lived subjects. Informed consents were obtained from all participants (and their legal proxies). The Research Ethics Committee of Sichuan University approved this study.
Data collection and measurements
Assessment of cognitive function
The methods used to assess cognitive function have been reported previously (Zhou et al. 2010; Huang et al. 2009). Cognitive function was measured using the 30-item MMSE, which is a global test that includes components that test orientation, attention, calculation, language, and recall. To decrease methodological errors and assure method reliability, the administrator of the test was provided with professional training comprising: (1) reviewing the MMSE procedure and grading system, as outlined in a short booklet and video; (2) observing a geriatrician conduct the MMSE on residents who were not part of the study; and (3) receiving supervision while conducting the MMSE on residents who were not part of the study. Individuals who gave consent to participate in the study were tested using the MMSE. The individuals were categorized as follows: possible dementia (scores between 0 and 18), mild cognitive impairment (scores between 19 and 24), and normal (scores between 25 and 30) (Zhou et al. 2010; Huang et al. 2009; Tombaugh and McIntyre 1992).
The MMSE relies heavily on visual and auditory abilities, in particular at advanced ages (Zhou et al. 2010; Huang et al. 2009), and there was a high prevalence of visual or hearing impairment among the nonagenarians and centenarians. Twenty-eight men and 72 women did not complete the MMSE test due to visual or hearing impairment. To address this issue, these subjects were excluded at data analysis. In the oldest-old group, only 35 subjects had scores higher than 24 (30 in men and 5 in women); therefore, we merged data from subjects with mild cognitive impairment and normal cognitive function into an “impossible” dementia group when the data were analyzed.
Measurement of FSG and FSI
Blood samples for measurement of FSG and FSI were obtained from all subjects at 08:00 following an overnight fast. FSG was measured using the glucose oxidase method (glucose B-test, Wako Pure Chemical, Osaka, Japan) (Kouzuma et al. 2002). FSI levels were determined using the RIA technique. Sera used to measure serum insulin concentrations by RIA were stored at −80 °C (Bowsher et al. 1999; Singhal et al. 2005). FSG and FSI were determined using standard laboratory techniques (performed by a technician in the biochemistry laboratory of Sichuan University). Abnormal FSG and FSI levels were defined based on criteria provided by the China Diabetes Association as follows: normal FSG, <6.00 mmol/L; IFG, 6.00–7.00 mmol/L; diabetes, >7.00 mmol/L; hypo-FSI, <5.00 mU/mL; normal FSI, 5–15.00 mU/mL; and hyper-FSI, >15.00 mU/mL (Song et al. 2011; Xu et al. 2010), respectively.
Assessment of covariates
The methods used have been described previously (Zhou et al. 2010; Huang et al. 2009). The baseline examination obtained information on age (years), gender (male/female), body mass index (BMI), serum uric acid (SUA), and serum lipid/lipoprotein levels. Blood pressure in the right arm (sitting or recumbent position) was measured twice to the nearest 2 mmHg using a standard mercury sphygmomanometer (Korotkoff phases I and V) by trained nurses or physicians. Serum lipid/lipoprotein levels (including serum triglyceride (TG), total cholesterol (TC), high density lipoprotein (HDL) cholesterol, and low density lipoprotein (LDL) cholesterol) and SUA levels were determined using standard laboratory techniques (performed by a technician in the biochemistry laboratory of Sichuan University).
Statistical analyses
All statistical analyses for this study were performed using the SPSS for Windows software package, version 11.5 (SPSS Inc., Chicago, IL, USA). Comparisons were made between baseline characteristics of the different FSI groups (out of all participants, only 5 showed hyperinsulinemia and 211 showed hypoinsulinemia; the five individuals with hyperinsulinemia were merged into the normal insulin group) and between individuals with and without cognitive impairment using unpaired Student’s t tests for continuous variables or Pearson Chi squared or Fisher’s exact tests (where an expected cell count was <5) for categorical variables. Baseline characteristics between the different FSG groups were also compared using analysis of variance for continuous variables. Multiple logistic regression was used to estimate the odds ratio and 95 % confidence interval of hypoinsulinemia or abnormal FSG as a function of increased risk for increased cognitive impairment. We adjusted age, gender, and educational levels as general covariates in model 1. In view of the fact that general or central adiposity, elevated blood pressure, dyslipidemia, hyperglycemia, and hyperuricacidemia may be components of metabolic syndrome and that they may be involved in the association of hypoinsulinemia or abnormal FSG with cognitive impairment, we adjusted BMI, serum lipid/lipoprotein, blood pressure, and SUA in model 2. We adjusted all of these covariates in model 3. A P value of <0.05 was considered to be statistically significant, and all P values were two sided.
Results
Baseline characteristics of genotype frequencies of the IR and cognitive impairment
The sample group included 661 unrelated Chinese (aged 90–108 years; mean, 93.52 ± 3.37 years; 67.3 % women; FSI, 6.27 ± 2.27 mU/mL; FSG, 4.46 ± 1.45 mmol/L; MMSE score, 15.49 ± 5.44). In this sample, 409 individuals (61.8 %) were cognitively impaired.
To demonstrate the association between demographics or clinical characteristics and FSG, the means (or percentages) of various demographic and clinical characteristics grouped by FSG are shown in Table 1. Subgroups with impaired fasting glucose and diabetes showed significantly higher SUA (F = 5.642, P = 0.004) and TC (F = 3.170, P = 0.043) levels. There were no significant differences between the different subgroups in other covariates (age, gender, FSI, serum lipid/lipoprotein levels, blood pressure, and BMI; see Table 1).
The means (or percentages) of various demographic or clinical characteristics in the hypoinsulinemia and normal insulin groups are shown in Table 2 to demonstrate the association between demographics or clinical characteristics and FSI. Fewer males showed hypoinsulinemia compared with females (χ 2 = 5.280, P = 0.029). Individuals with hypoinsulinemia showed significantly lower SUA (t = 4.486, P < 0.0001), TC (t = 5.376, P < 0.0001), HDL (t = 3.321, P = 0.010), and LDL (t = 2.353, P = 0.027) and higher diastolic blood pressure (t = 1.964, P = 0.049) levels. There were no significant differences between the different subgroups in other covariates (age, TG, SBP, and BMI; see Table 2).
The means (or percentages) of various demographic or clinical characteristics grouped by cognitive impairment are shown in Table 3 to demonstrate the association between demographics or clinical characteristics and cognitive impairment. Fewer males showed cognitive impairment compared with females (χ 2 = 56.16, P < 0.0001). Individuals with higher educational levels showed less cognitive impairment (χ 2 = 95.32, P < 0.0001). Individuals with cognitive impairment showed higher TC (t = 2.098, P = 0.036). There were no significant differences between the different subgroups in other covariates (see Table 3).
Association of cognitive impairment with FSG
Among the different FSG groups, there was no significant difference in MMSE score (F = 0.939, P = 0.392) or in prevalence of cognitive impairment (F = 0.939, P = 0.392; see Table 1). Furthermore, there was no significant difference in FSGs between those with or without cognitive impairment (t = 0.147, P = 0.883; see Tables 3 and 4).
Association of cognitive impairment with FSI
In the different FSI groups, individuals with a normal insulin level showed a significantly higher MMSE score compared with those in the hypoinsulinemia groups (t = 2.160, P = 0.031) and also showed a nonsignificant increased prevalence of cognitive impairment (χ 2 = 2.960, P = 0.228; see Table 2). There was also no significant difference in FSI between those with and without cognitive impairment (t = 1.609, P = 0.108; see Table 3). Hypoinsulinemia nonsignificantly increased the risk of cognitive impairment (see Table 5).
Discussion
This study examined the association between FSG or FSI and cognitive impairment among Chinese nonagenarians/centenarians. Using cross-sectional observations, nonagenarians/centenarians from one community who had no previous diagnosis of diabetes showed a high prevalence of cognitive impairment and hypoinsulinemia. The prevalence of impaired fasting glucose was 4.99 %, and that of diabetes was 6.20 %. This study showed that among Chinese nonagenarians/centenarians, cognitive function correlated with FSI and not FSG. Higher insulin levels may be a preventative factor for cognitive impairment.
Insulin sensitivity declines and insulin resistance increases with aging (Lin et al. 2011; Frisardi et al. 2010; Barzilai et al. 2012; Penninx et al. 2009). In this study, the prevalence of hypoinsulinemia was almost a third higher (34.53 %) than in adults in general including those aged over 60 years. However, in this sample where a high prevalence of hypoinsulinemia existed, only 12.11 % of subjects showed abnormally high FSGs. If a high prevalence of insulin resistance exists, those with hypoinsulinemia are at risk for hyperglycosemia; thus, the prevalence of insulin resistance in this sample is low. In general, it is thought that insulin resistance and hyperinsulinemia increase with aging (Lin et al. 2011; Frisardi et al. 2010; Barzilai et al. 2012; Penninx et al. 2009), that in the elderly, obesity- and insulin-resistant individuals are more long lived, and that mortality in the elderly could lead to the retention of obesity- and insulin-resistant individuals (Lamming et al. 2012; Blanchard 2005; Andres 1980). However, our results in this study of long-lived subjects provide contradictory evidence. To the best of our knowledge, this study is the only study to focus on FSI and FSG levels in nonagenarians/centenarians. These data indicate that the effectiveness and production of insulin in long-lived subjects differs from adults in general. The mechanisms underlying these differences in long-lived subjects compared with the elderly in general should be examined in future studies.
In this study, the prevalence of both hypoinsulinemia and cognitive impairment was high, FSI significantly and positively correlated with cognitive score, and subjects with hypoinsulinemia showed lower cognitive function scores than those with normal insulin levels. Together, these data show that insulin may play a key role in cognitive function (Zhong et al. 2012; Shemesh et al. 2012). Hypoinsulinemia may underlie cognitive impairment in long-lived subjects. Previous studies provided evidence of the role insulin played in cognitive processes; specifically, in hippocampal function, training on a spatial memory task increased hippocampal insulin receptor expression and hypothalamic insulin-regulated memory processes (Costello et al. 2012; McNay and Recknagel 2011). Insulin receptors are also found in the amygdala and other brain regions involved in cognitive processes (Huang et al. 2010). Our study provides important evidence from long-lived subjects in a clinic trial setting; this was the interesting finding of this study.
In our sample, the cognitive score was very low; 41 of 661 subjects showed a normal score, the mean score was only 15.48, and the prevalence of serious cognitive impairment was 61.8 % (almost two thirds). It has been confirmed that individuals with cognitive impairment show greater than double mortality rate than those without cognitive impairment (Cano et al. 2012; Sachs et al. 2011). Insulin is an important hormone with essential physiologic functions, and the high prevalence of hypoinsulinemia may be a manifestation of the deterioration in pancreatic island function with age. Individuals with hypoinsulinemia may also show a high rate of mortality (Langer et al. 1986). Therefore, due to this increased rate of mortality, at advanced ages, only those with both normal cognitive function and normal insulin levels remain. This theory is conducive with the finding that hypoinsulinemia correlated with cognitive impairment. However, the high mortality rate could underlie the phenomenon that more individuals with cognitive impairment show hypoinsulinemia but cannot explain the fact that FSI was significantly and positively correlated with cognitive scores. Thus, insulin must play a role in cognitive function.
Our study had some limitations that must be considered. First, 870 subjects aged 90 years or older volunteered for the PLAD Study. Among these 870 volunteers, only 661 had nonmissing data for the two main variables involved in this current analysis. Second, due to the cross-sectional nature of this study, the subjects might change their diets and the conditions related to the association of FSG and FSI with cognitive impairment. However, all of the nonagenarians/centenarians had lived for long periods in the country in southwest China (an underdeveloped area in China), and in that area, the diet was typically vegetarian. The lifestyles and food habits of the nonagenarians/centenarians were relatively consistent and similar. Their diets and conditions were similar; thus, it was impossible that diet and conditions affected the results of this study. Third, due to the cross-sectional nature of this study, we could not conduct analyses of causes. Fourth, because this study is part of the PLAD study, a survival bias may exist. However, this issue is inherent in a study of individuals of this age group. Finally, there was a difference in the prevalence of cognitive impairment between genders. Gender may influence the association of FSG or FSI with cognitive impairment. Data analysis based on gender may remove this influence. However, this analysis could reduce the sample size thereby preventing the generation of a conclusion.
In summary, we observed that among long-lived subjects, cognitive function appeared to correlate with FSI, and higher FSI was associated with enhanced cognitive function. Insulin and its role in cognitive function must underlie this finding.
References
Andres R (1980) Influence of obesity on longevity in the aged. Adv Pathobiol 7:238–246
Barzilai N, Huffman DM, Muzumdar RH, Bartke A (2012) The critical role of metabolic pathways in aging. Diabetes 61(6):1315–1322
Blanchard BM (2005) Obesity and longevity. N Engl J Med 352(24):2555–2556
Bowsher RR, Lynch RA, Brown-Augsburger P, Santa PF, Legan WE, Woodworth JR, Chance RE (1999) Sensitive RIA for the specific determination of insulin lispro. Clin Chem 45(1):104–110
Cano C, Samper-Ternent R, Al Snih S, Markides K, Ottenbacher KJ (2012) Frailty and cognitive impairment as predictors of mortality in older Mexican Americans. J Nutr Health Aging 16(2):142–147
Costello DA, Claret M, Al-Qassab H, Plattner F, Irvine EE, Choudhury AI, Giese KP, Withers DJ, Pedarzani P (2012) Brain deletion of insulin receptor substrate 2 disrupts hippocampal synaptic plasticity and metaplasticity. PLoS One 7(2):e31124, E
Craft S (2009) The role of metabolic disorders in Alzheimer disease and vascular dementia: two roads converged. Arch Neurol 66(3):300–305
Duron E, Hanon O (2008) Vascular risk factors, cognitive decline, and dementia. Vasc Health Risk Manag 4(2):363–381, Review
Frisardi V, Solfrizzi V, Capurso C, Imbimbo BP, Vendemiale G, Seripa D, Pilotto A, Panza F (2010) Is insulin resistant brain state a central feature of the metabolic–cognitive syndrome? J Alzheimers Dis 21(1):57–63
Huang CQ, Dong BR, Wu HM, Zhang YL, Wu JH, Lu ZC, Flaherty JH (2009) Association of cognitive impairment with serum lipid/lipoprotein among Chinese nonagenarians and centenarians. Dement Geriatr Cogn Disord 27(2):111–116
Huang CC, Lee CC, Hsu KS (2010) The role of insulin receptor signaling in synaptic plasticity and cognitive function. Chang Gung Med J 33(2):115–125
Kern W, Peters A, Fruehwald-Schultes B, Deininger E, Born J, Fehm HL (2001) Improving influence of insulin on cognitive functions in humans. Neuroendocrinology 74(4):270–280
Kesavadev JD, Short KR, Nair KS (2003) Diabetes in old age: an emerging epidemic. J Assoc Physicians India 51:1083–1094
Kodl CT, Seaquist ER (2008) Cognitive dysfunction and diabetes mellitus. Endocr Rev 29(4):494–511
Kouzuma T, Usami T, Yamakoshi M, Takahashi M, Imamura S (2002) An enzymatic method for the measurement of glycated albumin in biological samples. Clin Chim Acta 324(1–2):61–71
Lamming DW, Ye L, Katajisto P, Goncalves MD, Saitoh M, Stevens DM, Davis JG, Salmon AB, Richardson A, Ahima RS, Guertin DA, Sabatini DM, Baur JA (2012) Rapamycin-induced insulin resistance is mediated by mTORC2 loss and uncoupled from longevity. Science 335(6076):1638–1643
Langer O, Damus K, Maiman M, Divon M, Levy J, Bauman WA (1986) Link between relative hypoglycemia–hypoinsulinemia during oral glucose tolerance tests and intrauterine growth retardation. Am J Obstet Gynecol 155(4):711–716
Lin L, Saha PK, Ma X, Henshaw IO, Shao L, Chang BH, Buras ED, Tong Q, Chan L, McGuinness OP, Sun Y (2011) Ablation of ghrelin receptor reduces adiposity and improves insulin sensitivity during aging by regulating fat metabolism in white and brown adipose tissues. Aging Cell 10(6):996–1010
McNay EC, Recknagel AK (2011) Reprint of: Brain insulin signaling: a key component of cognitive processes and a potential basis for cognitive impairment in type 2 diabetes. Neurobiol Learn Mem 96(4):517–528
Park CR (2001) Cognitive effects of insulin in the central nervous system. Neurosci Biobehav Rev 25(4):311–323
Penninx BW, Nicklas BJ, Newman AB, Harris TB, Goodpaster BH, Satterfield S, de Rekeneire N, Yaffe K, Pahor M, Kritchevsky SB, ABC Health Study (2009) Metabolic syndrome and physical decline in older persons: results from the Health, Aging And Body Composition Study. J Gerontol A Biol Sci Med Sci 64(1):96–102
Planel E, Tatebayashi Y, Miyasaka T, Liu L, Wang L, Herman M, Yu WH, Luchsinger JA, Wadzinski B, Duff KE, Takashima A (2007) Insulin dysfunction induces in vivo tau hyperphosphorylation through distinct mechanisms. J Neurosci 27(50):13635–13648
Sachs GA, Carter R, Holtz LR, Smith F, Stump TE, Tu W, Callahan CM (2011) Cognitive impairment: an independent predictor of excess mortality: a cohort study. Ann Intern Med 155(5):300–308
Shemesh E, Rudich A, Harman-Boehm I, Cukierman-Yaffe T (2012) Effect of intranasal insulin on cognitive function: a systematic review. J Clin Endocrinol Metab 97(2):366–376
Singhal A, Jamieson N, Fewtrell M, Deanfield J, Lucas A, Sattar N (2005) Adiponectin predicts insulin resistance but not endothelial function in young, healthy adolescents. J Clin Endocrinol Metab 90(8):4615–4621
Song A, Xu M, Bi Y, Xu Y, Huang Y, Li M, Wang T, Wu Y, Liu Y, Li X, Chen Y, Wang W, Ning G (2011) Serum fetuin-A associates with type 2 diabetes and insulin resistance in Chinese adults. PLoS One 6(4):e19228
Tombaugh TN, McIntyre NJ (1992) The mini-mental state examination: a comprehensive review. J Am Geriatr Soc 40(9):922–935
van den Berg E, de Craen AJ, Biessels GJ, Gussekloo J, Westendorp RG (2006) The impact of diabetes mellitus on cognitive decline in the oldest of the old: a prospective population-based study. Diabetologia 49(9):2015–2023
van den Berg E, Biessels GJ, de Craen AJ, Gussekloo J, Westendorp RG (2007) The metabolic syndrome is associated with decelerated cognitive decline in the oldest old. Neurology 69(10):979–985
Xu L, Jiang CQ, Lam TH, Lin JM, Yue XJ, Cheng KK, Liu B, Jin YL, Zhang WS, Thomas GN, Guangzhou Biobank Cohort Study-CVD (2010) The metabolic syndrome is associated with subclinical atherosclerosis independent of insulin resistance: the Guangzhou Biobank Cohort Study-CVD. Clin Endocrinol 73(2):181–188
Zhong Y, Miao Y, Jia WP, Yan H, Wang BY, Jin J (2012) Hyperinsulinemia, insulin resistance and cognitive decline in older cohort. Biomed Environ Sci 25(1):8–14
Zhou Y, Flaherty JH, Huang CQ, Lu ZC, Dong BR (2010) Association between body mass index and cognitive function among Chinese nonagenarians/centenarians. Dement Geriatr Cogn Disord 30(6):517–524
Acknowledgments
This research was supported by the Discipline Construction Foundation of Sichuan University and by grants from the Project of Science and Technology Bureau of Sichuan Province (2006Z09-006-4) and the Construction Fund for Subjects of West China Hospital of Sichuan University (XK05001). The authors thank the staff of the Department of Geriatrics Medicine, West China Hospital and Dujiangyan Hospital, and all participants (and their legal proxies) for their great contribution.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Yan-Ling, Z., Chang-Quan, H., Li, Y. et al. Association of fasting serum insulin and fasting serum glucose levels with cognitive impairment in Chinese nonagenarians/centenarians. AGE 36, 427–434 (2014). https://doi.org/10.1007/s11357-013-9547-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11357-013-9547-6