
Abstract
Maternal exposure to fine particulate matter (PM2.5) is associated with adverse pregnancy and neonatal health outcomes. To explore the mechanism, we performed mRNA sequencing of neonatal cord blood. From an ongoing prospective cohort, Air Pollution on Pregnancy Outcome (APPO) study, 454 pregnant women from six centers between January 2021 and June 2022 were recruited. Individual PM2.5 exposure was calculated using a time-weighted average model. In the APPO study, age-matched cord blood samples from the High PM2.5 (˃15 ug/m3; n = 10) and Low PM2.5 (≤ 15 ug/m3; n = 30) groups were randomly selected for mRNA sequencing. After selecting genes with differential expression in the two groups (p-value < 0.05 and log2 fold change > 1.5), pathway enrichment analysis was performed, and the mitochondrial pathway was analyzed using MitoCarta3.0. The risk of preterm birth (PTB) increased with every 5 µg/m3 increase of PM2.5 in the second trimester (odds ratio 1.391, p = 0.019) after adjusting for confounding variables. The risk of gestational diabetes mellitus (GDM) increased in the second (odds ratio 1.238, p = 0.041) and third trimester (odds ratio 1.290, p = 0.029), and entire pregnancy (odds ratio 1.295, p = 0.029). The mRNA-sequencing of cord blood showed that genes related to mitochondrial activity (FAM210B, KRT1, FOXO4, TRIM58, and FBXO7) and PTB-related genes (ADIPOR1, YBX1, OPTN, NFkB1, HBG2) were upregulated in the High PM2.5 group. In addition, exposure to high PM2.5 affected mitochondrial oxidative phosphorylation (OXPHOS) and proteins in the electron transport chain, a subunit of OXPHOS. These results suggest that exposure to high PM2.5 during pregnancy may increase the risk of PTB and GDM, and dysregulate PTB-related genes. Alterations in mitochondrial OXPHOS by high PM2.5 exposure may occur not only in preterm infants but also in normal newborns. Further studies with larger sample sizes are required.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Fine particulate matter (PM2.5) is the main contributor to air pollution and is the fourth leading risk factor for death and disability worldwide (Anderson et al. 2012). PM2.5 can penetrate deeply into the lungs and circulate through the bloodstream, causing serious health effects, including cardiac arrhythmia, coronary heart disease, and premature death (Brook et al. 2010). These particles can also pass through the maternal–fetal placental barrier (Bové et al. 2019; Wick et al. 2010), which can adversely affect mothers and newborns, resulting in preterm birth, elevated blood pressure, gestational diabetes mellitus, and low birth weight (Shah and Balkhair 2011; Zhang et al. 2018; Madhloum et al 2019). In particular, according to the Developmental Origins of Health and Diseases theory, prenatal exposure to PM2.5 can have lifelong consequences because perturbations in the intrauterine environment are involved in the development of disease in later life (Barker 1990).
The mechanisms underlying PM-induced health effects include increased oxidative stress and inflammation (Kelly 2003; Schins et al. 2004). Various components of PM, including environmentally persistent radicals, peroxides, aromatic compounds, and dissolved metals, can generate reactive oxygen species (ROS), leading to oxidative stress and consequently enhancing various biological processes, such as inflammation and cell death (Jiang et al. 2019; Kamdar et al. 2008; Møller et al. 2014). Mitochondria are major locations for ROS production and cellular targets for the damaging effects of PM (Fetterman et al. 2017; Jin et al. 2018). ROS generation and the subsequent increase in oxidative stress have been recognized as a major contributor to cell damage, cell death, DNA damage, and inflammation due to PM2.5 exposure (Kamdar et al. 2008; Li, et al. 2003). As ROS are mainly produced in the mitochondria as by-products of cellular respiration (Ward 2017), the disruption of mitochondrial electron transport (oxidative phosphorylation, OXPHOS) can further augment ROS production and amplify oxidative stress (Ward 2017). However, studies on the specific connections between PM2.5 exposure and mitochondria in a prospective cohort study are limited.
The regulation of gene expression is fundamental for linking genotypes to phenotypes. The synthesis and maturation of RNAs are tightly controlled and form complex gene expression networks that ultimately drive biological processes (Marguerat and Bähler 2010). High-throughput mRNA sequencing (mRNA-seq) can derive millions of nucleotide sequences from individual transcripts (Stark et al. 2019). These nucleotide sequences provide multiple coverages of the entire transcriptome. RNA-seq is widely used in the study of diseases and biological processes because it can identify genes that are actively transcribed in a sample and quantify the level at which alternative transcripts of a gene are transcribed (Ura et al. 2022).
In this study, we report the association between adverse pregnancy outcomes and PM2.5 exposure in pregnant women recruited from the ongoing prospective cohort, Air Pollution on Pregnancy Outcome (APPO) study. We report on the genes associated with preterm birth (PTB) and mitochondrial dysfunction associated with oxidative stress and inflammation using mRNA-seq of cord blood.
Methods
Study population
In the Air Pollution on Pregnancy Outcome (APPO) study, an ongoing prospective cohort, 454 pregnant women (all singleton) were recruited for this study by the APPO study group at six centers between January 2021 and June 2022. Details of the APPO cohort study were previously reported (Hur et al. 2023). The hospitals were located in a metropolitan area, an industrial complex, or a mountainous area. Pregnant women were > 19 years of age before 28 weeks gestation without underlying diseases. Participating mothers completed study questionnaires during early- or mid-term pregnancy to provide detailed information on maternal age, pre-pregnancy body mass index (BMI), maternal education, occupation, smoking status, alcohol consumption, and use of medication. We collected clinical data on obstetric history, ultrasound sonography, and routine blood tests, including white blood cell counts and high-sensitivity C-reactive protein (hs-CRP) levels as inflammatory markers. After delivery, pregnancy outcomes were recorded, including gestational age at delivery, delivery mode, neonatal sex, birth weight, birth height, APGAR score, and neonatal intensive care unit admission. Blood (5 ml) and urine (15 ml) samples were collected during each trimester of pregnancy, and cord blood (5 ml) was collected at delivery. After sample collection, urine was stored at − 80 ℃ within 30 min, blood was centrifuged, and plasma and buffy coat were stored at − 80 ℃.
This study was approved by the Ethical Research Committees of the six centers (Ewha Womans University Mokdong Hospital, EUMC 2021–04-032; Ewha Womans University Seoul Hospital, 2021–04-022; Yonsei University Severance Hospital, 4–2021-0414; Kangwon National University Hospital, KNUH-B-2021–04-012–008; Keimyung University Dongsan Medical Center, 2021–04-073; and Korea University Guro Hospital, 2021GR0233) and conducted according to the ethical principles of the Helsinki Declaration. All the participants provided written informed consent.
PM2.5 exposure assessment
Daily outdoor PM2.5 concentrations were collected from a nearby urban atmospheric measurement network based on the residential addresses of the study subjects. The Urban Air Monitoring Station data used in this study were obtained from Air Korea (https://www.airkorea.or.kr/web) of The Korean Ministry of the Environment.
The household indoor PM2.5 concentrations were measured by AirguardK® (Kweather, Co., Korea), a small electronic device with a light-scattering laser photometer sensor that can detect air pollution levels. The device was placed in the participants’ homes for at least 1 week during each trimester of pregnancy to measure the household indoor air quality. The measured indoor PM2.5 data were transmitted to the indoor air quality monitoring platform over a long-term evolution communication network to prevent data loss and to collect and store data per minute.
We calculated individual PM2.5 exposure using a time-weighted average model that considers the duration and location of various activities, using collected outdoor and indoor PM2.5 concentrations, and time-activity patterns of pregnant women (Edwards et al. 2001). The equation is shown below.
where,
- Cind:
-
individual PM2.5 exposure
- Chousehold indoor:
-
household indoor PM2.5 concentration
- Thousehold indoor:
-
time spent indoors at home
- Cindoor not at home:
-
average of household indoor PM2.5 concentration of all participants
- Tindoor not at home:
-
time spent indoors not at home
- Coutdoor:
-
outdoor PM2.5 concentration based on address
- Toutdoor:
-
time spent outdoors
mRNA sequencing in cord blood
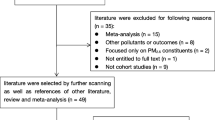
To perform mRNA sequencing on cord blood, we categorized the participants into two groups based on individual PM2.5 exposure during pregnancy:15 µg/m3 or less for the low PM2.5 exposure (Low PM2.5) and 15 µg/m3 or more for high PM2.5 exposure (High PM2.5) groups (Fig. 1). This concentration followed the recommended level of 24-h average PM2.5 according to the WHO 2021 air quality guidelines. We randomly selected extracted total RNA from the buffy coats of cord blood samples from Low PM2.5 (n = 30) and High PM2.5 (n = 10) groups using the Qiagen RNA extraction kit. Following quality assessment using an Agilent Tapestation 4200 (Agilent Technologies, Santa Clara, CA, USA), RNA was subjected to poly (A) enrichment using the NEBNext Poly(A) mRNA Magnetic Isolation Module and cDNA library generation with the xGen Broad-Range RNA Library Prep kit using xGen Normalase UDI primers (Integrated DNA Technologies, Coralville, IA, USA). Subsequently, paired-end sequencing was performed using the Illumina NovaSeq 6000 platform (Illumina Inc., San Diego, CA, USA). Through the sequencing process, 10 high concentrations and 30 low concentrations were generated, resulting in 40 paired-end RNA libraries. The raw and trimmed readings were inspected for quality using FastQC and MultiQC (Ewels et al. 2016), and Cutadapt was used to minimize adapter content and quality (Martin 2011).

Study flow chart. PTB, preterm birth; GDM, gestatonal diabetes mellitus; OXPHOS, oxidative phosphorylation
Sequencing data analysis
Preprocessing was performed by aligning the sequences using STAR (v.2.7.3a) (Dobin et al. 2013) and quantifying them using HTSeq (v.0.11.2) (Anders et al. 2015), where GRCh38 was used as the reference genome along with its annotation. While aligning the raw data (i.e., FASTQ files) through STAR, we optimally adjusted parameters such as “outFilterScoreMinOverLread” to 0 and “outFilterMatchNminOverLread” to 0.1 to maximize the number of uniquely mapped reads. Subsequently, we applied the transcripts per million method (Risso et al. 2014) with DGEobj.utils R package (Thompson et al. 2022) to the gene expression levels for normalization and carried out principal component analysis (PCA) (Karl Pearson 1901) with prcomp embedded in the stats R package and differential analyses including gene ontology (GO) analysis between the Low and High PM2.5 groups.
Differential expression analysis was conducted using the R package DESeq2 (Love et al. 2014). Significantly differentially expressed genes (DEGs) were visualized through volcano plots using the EnhancedVolcano R package (Kevin et al. 2021), and significantly enriched GO terms were shown as dot plots using the clusterProfiler R package (Wu et al. 2021). Two additional pathway enrichment analyses were performed: (i) Gene Set Enrichment Analysis (GSEA) (Subramanian et al. 2005; Mootha et al. 2003), whose visualization was achieved by mapping into Cytoscape (version 3.10.0) (Shannon et al. 2003) with the visualization app EnrichmentMap (Merico et al. 2010), and (ii) fast Gene Set Enrichment Analysis (FGSEA) (Korotkevich et al. 2021) illustrated through lollipop plots. For these analyses, two distinct gene sets were used, one of which was the whole aligned gene list and the other was the Mitocarta3.0 (Rath et al. 2021) gene list.
Statistical analysis
All statistical analyses were performed using SPSS Software (version 21.0; IBM, Armonk, NY, USA). Descriptive statistics for the general characteristics of all participants (n = 454) recruited from the ongoing APPO study are presented in Table 1. Continuous variables are expressed as mean ± standard deviation, and categorical variables are expressed as total number (n) and percentage (%). To explore the association between PM2.5 levels and adverse pregnancy outcomes, multiple logistic regression was conducted, controlling for maternal age, pre-pregnancy BMI, education, income, birth weight, and infant sex.
Results
Environmental characteristics of the prospective APPO cohort study population
We calculated the individual PM2.5 exposure of pregnant women using address-based outdoor PM2.5, household indoor PM2.5 concentrations, and time-activity analysis in the first, second, and third trimesters of pregnancy. Figure 2 shows the correlation between individual PM2.5 exposure and outdoor and household indoor PM2.5 concentrations in pregnant women. The positive correlations between address-based outdoor PM2.5 and indoor PM2.5 in every trimester were relatively low (first trimester, r = 0.062; second trimester, r = 0.126; third trimester, r = 0.182). However, individual PM2.5 exposure showed a significantly high positive correlation with household indoor PM2.5 concentrations (first trimester, r = 0.978; second trimester, r = 0.964; third trimester, r = 0.963). In the time-activity analysis, pregnant women spent more than 18 h at home, approximately 5 h indoors somewhere other than home, and approximately 1 h outdoors.

Correlation analysis between personal PM2.5 exposure, outdoor, and household indoor PM2.5 concentrations
Population characteristics of the prospective APPO cohort study
The general and lifestyle characteristics of the pregnant women are shown in Table 1. In total, 454 pregnant women were included with an average age of 33.6 years, a pre-pregnancy BMI of 22.3, and 67.2% of them were primiparous. Of the newborns, 54% were boys, with an average birth weight of 3139 g. Table 2 shows the results of the logistic regression of adverse pregnancy outcomes for every 5 µg/m3 increase in PM2.5 according to the exposure period during pregnancy. During the entire pregnancy or each trimester, PTB did not significantly increase after increases in the individual PM2.5. However, the incidence of gestational diabetes mellitus (GDM) significantly increased with every 5 µg/m3 increase PM2.5 in the third trimester and throughout pregnancy. After adjusting for maternal age, pre-pregnancy BMI, education, infant sex, and birth weight, PTB was significantly increased in the second trimester (odds ratio 1.391, p = 0.019), and GDM was significantly increased in the second (odds ratio 1.238, p = 0.041) and third (odds ratio 1.290, p = 0.029) trimesters, and entire PM2.5 level (odds ratio 1.295, p = 0.029).
Characteristics of subjects analyzed by mRNA sequencing in cord blood
To analyze the effects of PM2.5 on neonatal health through mRNA sequencing in cord blood, the characteristics of 40 pregnant women were randomly selected from the APPO study. The results are summarized in Table 3. There were no significant differences in maternal age, pre-pregnancy BMI, PTB, or GDM between the Low and High PM2.5 groups. However, PTB significantly increased in the second trimester (odds ratio 2.208, p = 0.027), following every 5 µg/m3 increase in the individual PM2.5 exposure (Supple. Table 1).
DEGs between the High and Low PM2.5 groups
Principal component analysis of the RNA-seq data showed that the High PM2.5 group (n = 10) was generally distinguished from the Low PM2.5 group (n = 30) (Fig. 3A). Through the analysis of DEGs between the two groups, we first collected 4375 genes expressed in either the High or Low PM2.5 group, and identified 370 DEGs (48 upregulated and 322 downregulated genes) in the High PM2.5 group (i.e., p-value < 0.05, and a log2 fold change > 1.5, Supple. Table 2), as shown in Fig. 3B. Among the top genes that were significantly upregulated in the High PM2.5 group, some genes, such as FAM210B, KRT1, FOXO4, TRIM58, and FBXO7 were found to be involved in mitochondria-associated activity, whereas others such as ADIPOR1, OPTN, HBG2, YBX1 (YB-1), and NFkB1 were associated with common obstetric issues, including PTB. The top genes significantly downregulated in the High PM2.5 group, including PF4V1, PF4, and S100A9 were found to be associated with inflammatory processes (Fig. 3B).

Principal component analysis plot and differentially expressed genes (DEGs) between the High PM2.5 (> 15 µg/m3 during pregnancy) and Low PM2.5 (≤ 15 µg/m3) groups. A PCA plot. B Volcano plot. Dotted lines represent the cut-offs for the log2 fold change (1.5) and p-value (0.05). Red and green dots denote the 48 upregulated and 322 downregulated genes in the High PM2.5 group, respectively
Enriched pathways in the High and Low PM2.5 groups
We examined cellular processes by GSEA-based network analysis, illustrated in Fig. 4A, which displayed seven clusters, where six of them were in the High PM2.5 group and only one was in the Low PM2.5 group. The six clusters were composed of vesicular pathways, protein catabolic process, response to toxic substance, pigment metabolic process, energy metabolism, and ribosome. While the upregulated clusters of the High PM2.5 group represented consistent findings including mitochondria-associated process (i.e., cellular respiration and OXPHOS) and protein catabolic process. The only upregulated cluster of the Low PM2.5 group, however, showed pathways associated with immune response which was in line with the previously described GO analysis. FGSEA also demonstrated that OXPHOS and other direct/indirect associated pathways were enhanced in the High PM2.5 group. As shown in Fig. 4B, complex I, complex I subunits, complex V, complex V subunits, and complex III subunits were upregulated in the High PM2.5 group among the protein complexes that are associated with OXPHOS. In the metabolism-associated pathways, ROS and glutathione metabolism, nucleotide synthesis and processing, and iron homeostasis were upregulated in the High PM2.5 group, and heme-containing proteins, and coenzyme A metabolism were upregulated in the Low PM2.5 group (Fig. 5C). Interestingly, PTBs (n = 3) in the High PM2.5 group were upregulated in OXPHOS‑associated pathways compared with the full term delivered group with the 10 lowest concentrations (Supple. Figure 1).

Enriched pathways in the High and Low PM2.5 groups. Gene ontology biological processes (GOBPs) enriched by the genes that were up- and downregulated in the High PM2.5 compared with that in the Low PM2.5 group. A Dot plot of the enriched pathways in the two groups. The significant genes for the enrichment analysis were selected with p-value < 0.05, and the absolute value of log2 fold-change > 0.2 for all genes in the pathways were selected with p-value < 0.05 and q-value < 0.1. B The significant genes within the MitoCarta 3.0 gene list were selected with p-value < 0.5, based on the results of differential expression analysis. The pathways were selected with a p-value < 0.05 and q-value < 0.1. The blue color density is represented by the significance (p-value) of the GOBPs, and the circle size revealed the effect size


Network of enriched pathways and lollipop plots involving mitochondria in the High and Low PM2.5 groups. A Network figure of the enriched pathways in the two groups. The red nodes indicate upregulated pathways in the High PM2.5 group and the blue nodes denote upregulation in the Low PM2.5 group. The selected pathways were filtered for FDR < 0.1 and edge similarity > 0.375. B OXPHOS pathways in High and Low PM2.5 groups. C Mitochondrial metabolic pathways in the High and Low PM2.5 groups, which exhibited the top 15 absolute NES values. D Heatmap of the z- and t-scores of genes associated with OXPHOS in the High and Low PM2.5 groups. E Path view of OXPHOS pathway with MitoCarta genes (p-value < 0.5) based on KEGG pathways. The red box indicates upregulation and green box indicates downregulation
Discussion
The main finding of this study was that exposure to high concentrations of fine particulate matter during pregnancy was associated with an increased risk of PTB by upregulating PTB-related genes and mitochondrial OXPHOS dysfunction due to complex subunits alterations. This is the first prospective pregnancy cohort study to identify the mechanism of the association among PM2.5 exposure, PTB, and neonatal health threats. Furthermore, our findings suggest that exposure to high levels of PM2.5 during pregnancy may congenitally alter mitochondrial OXPHOS in preterm infants as well as in full term newborns.
Fine particulate matter, major ambient air pollutant, is a complex mixture of organic and inorganic particles. Maternal exposure to ambient PM2.5 can increase the risk of adverse pregnancy outcomes, including PTB, GDM, low birth weight, and small for gestational age. People typically spend up to 90% of their day indoors (Selevan et al. 2000; Zhu et al. 2015); therefore, indoor PM concentrations have an important impact on individual exposure. It has been recorded that indoor PM concentrations can exceed outdoor concentrations (Klepeis et al. 2001). The sources of indoor PM include aerosol sprays, cooking, candle burning, heating/cooking with solid fuels, improperly tuned gas stoves and furnaces, pets, dust mites, cleaning, and smoking. Indoor air is also affected by the infiltration of outdoor air (Goyal and Kumar 2013), potentially affecting PM concentrations. Depending on the outdoor PM levels, this infiltration can cause an increase or decrease in indoor PM levels (Hegde et al. 2020).
This study used a time-weighted average model with household indoor and outdoor PM2.5 concentrations, and time-activity records to calculate individual PM2.5 exposure and found that every 5 µg/m3 increase was associated with a higher risk of PTB and GDM. The individual PM2.5 exposure was most affected by household indoor PM2.5 concentrations because pregnant women spent more than 95% of their time indoors. However, individual exposure estimates were not affected by home-address-based outdoor PM2.5. None of the pregnant women smoked during pregnancy, and only 5% were exposed to household smoking, suggesting that the contribution was minimal. Future studies should investigate the sources of indoor PM2.5 and analyze its association with pregnancy outcomes.
Adverse pregnancy outcomes due to maternal exposure to fine PM affect fetal growth and development (Zhu et al. 2015). Low birth weight and PTB are well known to be associated with increased neonatal morbidity and mortality as well as possible increased morbidity in adulthood (Behrman and Butler 2007). These adverse pregnancy outcomes from PM2.5 exposure are primarily related to their ability to induce oxidative stress and inflammation (Jiang et al. 2019; Kamdar et al. 2008; Møller et al. 2014). The large surface area of PM2.5 and the presence of heavy metals adsorbed on its surface can generate higher amounts of hydroxyl radicals compared to larger particles (PM10) (Kumar and Morawska 2013; Morawska et al. 2001). Studies have shown that environmental pollutants primarily target mitochondria and have several detrimental effects. Several studies have linked in-utero PM exposure to mitochondrial oxidative dysfunction (Grevendonk et al. 2016; Brunst et al. 2018; Cosemans et al. 2022). One study reported that PM10 exposure increased mitochondrial 8-hydroxy-2′-deoxyguanosine (8-OHdG) levels in maternal and cord blood, which was associated with increased systemic oxidative stress at the mitochondrial level (Grevendonk et al. 2016). Another study reported that increased exposure to PM2.5 during pregnancy was associated with decreased mitochondrial DNA copy number (mtDNAcn) in the cord blood, depending on the fetal sex (Brunst et al. 2018). Another study reported that in-utero exposure to PM2.5 during the first trimester of pregnancy was associated with cord blood MT-ND4L10550A>G heteroplasmy in newborns, which was associated with higher childhood weight (Cosemans et al. 2022). Although many studies have been conducted on mitochondrial dysfunction and fine particles, there is a significant lack of studies reporting the mechanisms between maternal exposure to PM2.5, and redox imbalance mechanisms in neonatal cord blood.
The results of mRNA-seq analysis in cord blood showed that among the top gene list with significant log2 fold changes, only FAM210B, a mitochondrial protein, is known to be linked to erythroid differentiation (Kondo et al. 2016), whereas KRT1 and FOXO4 are associated with oxidative stress (Yang et al. 2022; Collard et al. 2001). Also, TRIM58 and FBXO7 are involved in the ubiquitin-dependent protein catabolic pathway (Lee et al. 2023). Using DEG, three pathway enrichment analyses, including GO, GSEA, and FGSEA, revealed that the enriched pathways in the High PM2.5 group were mainly involved in mitochondrial- and apoptosis-related pathways. In addition, changes in mitochondrial activity and ribosome assembly suggest a possible alteration in proteostasis by maintaining proteome homeostasis (Lu and Guo 2020). In contrast, pathways related to the immune response and inflammatory mechanisms were enriched in the Low PM2.5 group. Further, GO analysis using Mitokarta 3.0 showed upregulation of energy metabolism, mainly through precursor metabolites and energy production, energy derivation by oxidation of organic compounds, cellular respiration, aerobic respiration, and OXPHOS.
With the development of next-generation sequencing techniques, the number of genes with mutations known to cause mitochondrial diseases has increased substantially (Carroll et al. 2014). To date, mutations have been described in nuclear genes encoding OXPHOS structural proteins, as well as factors involved in virtually every step of OXPHOS biogenesis, including mtDNA replication and maintenance, mitochondrial transcription and translation, import, assembly, synthesis, and incorporation of redox cofactors, as well as proteins required for proper mitochondrial cristae shape, lipid milieu composition, and detoxification pathways (Fernandez-Vizarra and Zeviani 2021). In OXPHOS disorders caused by mutations in the structural subunits and assembly factors, the severity of biochemical and assembly defects is highly variable and largely depends on the location of the protein in the assembly process and the nature of the mutation (Fernandez-Vizarra et al. 2009; Ghezzi and Zeviani 2018).
Mitochondrial DNA encodes the proteins of the electron transport chain (ETC; 13 subunits of complexes I, III, and IV; and ATP synthase (complex V)) that are essential for OXPHOS (Taanman 1999). During mitochondrial respiration, electrons from complexes I and III react with molecular oxygen to form superoxides, which damage ROS (Andreyev et al. 2005). Because of its lack of histones, which protect against oxidative stress, and its close proximity to the ETC, the primary source of ROS, mtDNA is more vulnerable to the accumulation of ROS-induced damage than nuclear DNA (Ballinger et al. 2000; Tatarenkov and Avise 2007). In our results, the High PM2.5 group had upregulated complex I, complex I subunits, complex V, complex V subunits, and complex III subunits. These findings suggest that exposure to high levels of fine particulate matter may affect the ETC complex and structural subunits.
The Low PM2.5 group showed upregulated complex II and coenzyme A metabolism. Complex II (succinic dehydrogenase, SDH) is an enzyme involved in the ETC and the Krebs cycle that oxidizes succinate to fumarate and transfers electrons to CoQ. The pathogenesis of mutations and deficiencies in the CII subunit appears to be related to succinate accumulation, which is associated with a control mechanism that activates the hypoxic program of cells (Selak et al. 2005). Complex III constitutes the central part of the ETC, which accepts two electrons from reduced CoQ (CoQH2) and donates them to cytochrome c. Mutations and deficiencies in the CIII subunit are associated with sporadic myopathy, exercise intolerance, recurrent metabolic crisis, insulin-responsive hyperglycemia, and lactic acidosis (Gaignard et al. 2013; Gusic et al. 2020). Thus, our results suggest that despite limitations in the literature, high levels of PM2.5 in mother-neonate pairs may affect mitochondrial oxidative stress dysfunction in newborns, which may be involved in their growth and later development of disease.
While our transcriptomic analysis primarily revealed mitochondrial-associated changes, other important alterations were also demonstrated and significant changes were identified, with some genes associated with obstetrical issues, consistent with previous studies. In fetal and placental development, YB-1 has been shown to play a crucial role during the gestation period (Meyer et al. 2020). For uterine or pregnancy-related functions, ADIPOR1 has been proposed to influence uterine contractility, suggesting a possible connection between plasma membrane adiponectin receptors and preterm birth (Vyas et al. 2019). Also, OPTN has been associated with nuclear factor-kappa B activity (Akizuki et al. 2013), and NFkB1 and HBG2 have been directly/indirectly involved in PTB (Pique-Regi et al. 2019; Fang et al. 2022). Additionally, while inflammatory-associated pathways in the Low PM2.5 group and cell-death-associated pathways in the High PM2.5 group were both upregulated, ribonucleoside triphosphate metabolic process in the Low PM2.5 group and proteasome-mediated ubiquitin-dependent protein catabolic process in the High PM2.5 group are known to be associated with Nrf2 signaling pathways (Gao et al. 2020). Therefore, we propose that exposure to high levels of fine particulate matter during pregnancy can increase the risk of PTB by affecting uterine contractions, NFkB activity, and cell death. We further propose that alterations in mitochondrial OXPHOS caused by exposure to high levels of PM have health consequences for both preterm and neonatal infants.
The limitations of this study are that although most pregnant women spent a lot of time indoors at home, the sample size was small and household indoor PM2.5 could not be measured during the entire pregnancy period. In addition, the identification of PM2.5-related genes in cord blood requires validation in a larger population. Nevertheless, the strength of this study is reported the association between PM2.5, PTB, and GDM in a maternal health effect analysis using personal PM2.5 exposure through IOT-based indoor and addressee-based outdoor PM2.5 measurement, and time-activity pattern.
Conclusion
In an ongoing prospective cohort, the APPO study, PTB and GDM were associated with every 5 µg/m3 increase in individual PM2.5 exposure. In addition, neonatal cord blood samples from high PM2.5 exposure may induce dysfunction of genes associated with common obstetric problems, including PTB, and mitochondrial OXPHOS dysfunction through changes in some ETC complex proteins. This suggests that maternal exposure to fine particulate matter affects PTB-related gene activity, growth, and subsequent health via mitochondrial impairment in preterm infants, including newborns. Further analysis of the sources of household indoor PM and composition of household indoor PM in relation to oxidative damage is needed to support this study, and further studies with larger cohorts are warranted.
Data availability
All data generated or analyzed during this study are included in this published article [and its additional information files]. Raw data of mRNA sequencing will be made available on request.
Abbreviations
- PM2.5:
-
Fine particulate matter
- PTB:
-
Preterm birth
- GDM:
-
Gestational diabetes mellitus
- OXPHOS:
-
Oxidative phosphorylation
- ROS:
-
Reactive oxygen species
- BMI:
-
Body mass index
- hs-CRP:
-
High-sensitivity C-reactive protein
- PCA:
-
Principal component analysis
- DEG:
-
Differentially expressed gene
- FGSEA:
-
Fast gene set enrichment analysis
- mtDNA:
-
Mitochondrial DNA
- ETC:
-
Electron transport chain
References
Akizuki M, Yamashita H, Uemura K, Maruyama H, Kawakami H, Ito H et al (2013) Optineurin suppression causes neuronal cell death via NF-kappa B pathway. J Neurochem 126:699–704
Anders S, Pyl PT, Huber W (2015) HTSeq-A Python framework to work with high-throughput sequencing data. Bioinformatics 31:166–169
Anderson JO, Thundiyil JG, Stolbach A (2012) Clearing the air: a review of the effects of particulate matter air pollution on human health. J Med Toxicol 8:166–175
Andreyev AY, Kushnareva YE, Starkov A (2005) Mitochondrial metabolism of reactive oxygen species. Biochemistry (mosc) 70:200–214
Ballinger SW, Patterson C, Yan CN, Doan R, Burow DL, Young CG et al (2000) Hydrogen peroxide–and peroxynitrite-induced mitochondrial DNA damage and dysfunction in vascular endothelial and smooth muscle cells. Circ Res 86:960–966
Barker DJ (1990) The fetal and infant origins of adult disease. BMJ 301:1111
Behrman RE, Butler AS (2007) Preterm birth: causes, consequences, and prevention. Washington. National Academies. https://doi.org/10.17226/11622
Bové H, Bongaerts E, Slenders E, Bijnens EM, Saenen NB, Gyselaers W et al (2019) Ambient black carbon particles reach the fetal side of human placenta. Nat Commun 10:3866
Brook RD, Rajagopalan S, Pope CA, Brook JR, Bhatnagar A, Diez-Roux AV et al (2010) Particulate matter air pollution and cardiovascular disease: an update to the scientific statement from the American heart association. Circulation 121:2331–2378
Brunst KJ, Sanchez-Guerra M, Chiu YM, Wilson A, Coull BA, Kloog I et al (2018) Prenatal particulate matter exposure and mitochondrial dysfunction at the maternal-fetal interface: effect modification by maternal lifetime trauma and child sex. Environ Int 112:49–58
Carroll CJ, Brilhante V, Suomalainen A (2014) Next-generation sequencing for mitochondrial disorders. Br J Pharmacol 171:1837–1853
Collard CD, Montalto MC, Reenstra WR, Buras JA, Stahl GL (2001) Endothelial oxidative stress activates the lectin complement pathway: role of cytokeratin 1. Am J Pathol 159:1045–1054
Cosemans C, Wang C, Alfano R, Martens DS, Sleurs H, Dockx Y et al (2022) In utero particulate matter exposure in association with newborn mitochondrial ND4L10550A>G heteroplasmy and its role in overweight during early childhood. Environ Health 21:88
Dobin A, Davis CA, Schlesinger F, Drenkow J, Zaleski C, Jha S et al (2013) STAR: ultrafast universal RNA-seq aligner. Bioinformatics 29:15–21
Edwards RD, Jurvelin J, Saarela K, Jantunen M (2001) VOC concentrations measured in personal samples andresidential indoor, outdoor and workplace microenvironments in EXPOLIS-Helsinki, Finland. Atmos Environ 35:4531–4543
Ewels P, Magnusson M, Lundin S, Käller M (2016) MultiQC: summarize analysis results for multiple tools and samples in a single report. Bioinformatics 32:3047–3048
Fang D, Fang Y, Zhang W, Xiang Y, Cheng X, Liang M et al (2022) Comprehensive analysis of quantitative proteomics with DIA mass spectrometry and ceRNA network in intrahepatic cholestasis of pregnancy. Front Cell Dev Biol 10:854425
Fernandez-Vizarra E, Zeviani M (2021) Mitochondrial disorders of the OXPHOS system. FEBS Lett 595:1062–1106
Fernandez-Vizarra E, Tiranti V, Zeviani M (2009) Assembly of the oxidative phosphorylation system in humans: what we have learned by studying its defects. Biochim Biophys Acta 1793:200–211
Fetterman JL, Sammy MJ, Ballinger SW (2017) Mitochondrial toxicity of tobacco smoke and air pollution. Toxicology 391:18–33
Gaignard P, Menezes M, Schiff M, Bayot A, Rak M, Ogier, de B.H., et al (2013) Mutations in CYC1, encoding cytochrome c subunit of respiratory chain complex III, cause insulin-responsive hyperglycemia. Am J Hum Genet 93:384–389
Gao L, Kumar V, Vellichirammal NN, Park SY, Rudebush TL, Yu L et al (2020) Functional, proteomic and bioinformatic analyses of Nrf2- and Keap1- null skeletal muscle. J Physiol 598:5427–5451
Ghezzi D, Zeviani M (2018) Human diseases associated with defects in assembly of OXPHOS complexes. Essays Biochem 62:271–286
Goyal R, Kumar P (2013) Indoor-outdoor concentrations of particulate matter in nine microenvironments of a mix use commercial building in megacity Delhi. Air Qual Atmos Health 6:747–757
Grevendonk L, Janssen BG, Vanpoucke C, Lefebvre W, Hoxha M, Bollati V et al (2016) Mitochondrial oxidative DNA damage and exposure to particulate air pollution in mother-newborn pairs. Environ Health 15:10
Gusic M, Schottmann G, Feichtinger RG, Du C, Scholz C, Wagner M et al (2020) Bi-allelic UQCRFS1 variants are associated with mitochondrial complex III deficiency. Cardiomyopathy, and alopecia totalis. Am J Hum Genet 106:102–111
Hegde S, Min KT, Moore J, Lundrigan P, Patwari N, Collingwood S et al (2020) Indoor household particulate matter measurements using a network of low-cost. Sens Aerosol Air Qual Res 20:381–394
Hur YM, Park S, Kwon E, You YA, Ansari A, Kim SM et al (2023) The introduction to air pollution on pregnancy outcome (APPO) study: a multicenter cohort study. OGS 66:69–180
Jiang X, Xu F, Qiu X, Shi X, Pardo M, Shang Y et al (2019) Hydrophobic organic components of ambient fine particulate matter (PM2.5) associated with inflammatory cellular response. Environ Sci Technol 53:10479–10486
Jin X, Xue B, Zhou Q, Su R, Li Z (2018) Mitochondrial damage mediated by ROS incurs bronchial epithelial cell apoptosis upon ambient PM2.5 exposure. J Toxicol Sci 43:101–111
Kamdar O, Le W, Zhang J, Ghio AJ, Rosen GD, Upadhyay D (2008) Air pollution induces enhanced mitochondrial oxidative stress in cystic fibrosis airway epithelium. FEBS Lett 582:3601–3606
Karl Pearson FRS (1901) On lines and planes of closest fit to systems of points in space. Philos Mag 2(6):559–572. https://doi.org/10.1080/14786440109462720
Kelly FJ (2003) Oxidative stress: its role in air pollution and adverse health effects. Occup Environ Med 60:612–616
Kevin B, Sharmila R, Myles L (2021) EnhancedVolcano: Publication-ready volcano plots with enhanced colouring and labeling. Retrieved from https://github.com/kevinblighe/EnhancedVolcano. Accessed 1 June 2021
Klepeis NE, Nelson WC, Ott WR, Robinson JP, Tsang AM, Switzer P et al (2001) The National Human Activity Pattern Survey (NHAPS): a resource for assessing exposure to environmental pollutants. J Expo Anal Environ Epidemiol 11:231–252
Kondo A, Fujiwara T, Okitsu Y, Fukuhara N, Onishi Y, Nakamura Y et al (2016) Identification of a novel putative mitochondrial protein FAM210B associated with erythroid differentiation. Int J Hematol 103:387–395
Korotkevich G, Sukhov V, Budin N, Shpak B, Artyomov MN, Sergushichev A (2021) Fast gene set enrichment analysis. bioRxiv 060012. https://doi.org/10.1101/060012
Kumar P, Morawska L (2013) Energy-pollution nexus for urban buildings. Environ Sci Technol 47:7591–7592
Lee SH, Lee YJ, Jung S, Chung KC (2023) E3 ligase adaptor FBXO7 contributes to ubiquitination and proteasomal degradation of SIRT7 and promotes cell death in response to hydrogen peroxide. J Biol Chem 299:102909
Li N, Sioutas C, Cho A, Schmitz D, Misra C, Sempf J et al (2003) Ultrafine particulate pollutants induce oxidative stress and mitochondrial damage. Environ Health Perspect 111:455–460
Love MI, Huber W, Anders S (2014) Moderated estimation of fold change and dispersion for RNA-seq data with DESeq2. Genome Biol 15:550
Lu B, Guo S (2020) Mechanisms linking mitochondrial dysfunction and proteostasis failure. Trends Cell Biol 30:317–328. https://doi.org/10.1016/j.tcb.2020.01.008
Madhloum N, Nawrot TS, Gyselaers W, Roels HA, Bijnens E, Vanpoucke C et al (2019) Neonatal blood pressure in association with prenatal air pollution exposure, traffic, and land use indicators: an ENVIRONAGE birth cohort study. Environ Int 130:104853
Marguerat S, Bähler J (2010) RNA-seq: from technology to biology. Cell Mol Life Sci 67:569–579
Martin M (2011) Cutadapt removes adapter sequences from high-throughput sequencing reads. EMBnet J 17:10. https://doi.org/10.14806/ej.17.1.200
Merico D, Isserlin R, Stueker O, Emili A, Bader GD (2010) Enrichment map: a network-based method for gene-set enrichment visualization and interpretation. PLoS One 5:e13984
Meyer N, Schumacher A, Coenen U, Woidacki K, Schmidt H, Lindquist JA et al (2020) Y-Box Binding Protein 1 expression in trophoblast cells promotes fetal and placental development. Cells 9:1942
Møller P, Danielsen PH, Karottki DG, Jantzen K, Roursgaard M, Klingberg H et al (2014) Oxidative stress and inflammation generated DNA damage by exposure to air pollution particles. Mutat. Res. Rev Mutat Res 762:133–166
Mootha VK, Lindgren CM, Eriksson KF, Subramanian A, Sihag S, Lehar J et al (2003) PGC-1alpha-responsive genes involved in oxidative phosphorylation are coordinately downregulated in human diabetes. Nat Genet 34:267–273
Morawska L, He C, Hitchins J, Gilbert D, Parappukkaran S (2001) The relationship between indoor and outdoor airborne particles in the residential environment. Atmos Environ 35:3463–3473
Pique-Regi R, Romero R, Tarca AL, Sendler ED, Xu Y, Garcia-Flores V et al (2019) Single cell transcriptional signatures of the human placenta in term and preterm parturition. elife 8:e52004
Rath S, Sharma R, Gupta R, Ast T, Chan C, Durham TJ et al (2021) MitoCarta3.0: an updated mitochondrial proteome now with sub-organelle localization and pathway annotations. Nucleic Acids Res 49:D1541–D1547
Risso D, Ngai J, Speed T (2014) Normalization of RNA-seq data using factor analysis of control genes or samples. Nat Biotechnol 32:896–902
Schins RP, Lightbody JH, Borm PJ, Shi T, Donaldson K, Stone V (2004) Inflammatory effects of coarse and fine particulate matter in relation to chemical and biological constituents. Toxicol Appl Pharmacol 195:1–11
Selak MA, Armour SM, MacKenzie ED, Boulahbel H, Watson DG, Mansfield KD et al (2005) Succinate links TCA cycle dysfunction to oncogenesis by inhibiting HIF-alpha prolyl hydroxylase. Cancer Cell 7:77–85
Selevan SG, Kimmel CA, Mendola P (2000) Identifying critical windows of exposure for children’s health. Environ Health Perspect 108:451–455
Shah PS, Balkhair T (2011) Air pollution and birth outcomes: a systematic review. Environ Int 37:498–516
Shannon P, Markiel A, Ozier O, Baliga NS, Wang JT, Ramage D et al (2003) A software environment for integrated models of biomolecular interaction networks. Genome Res 13:2498–2504
Stark R, Grzelak M, Hadfield J (2019) RNA sequencing: the teenage years. Nat Rev Genet 20:631–656
Subramanian A, Tamayo P, Mootha VK, Mukherjee S, Ebert BL, Gillette MA et al (2005) Gene set enrichment analysis: a knowledge-based approach for interpreting genome-wide expression profiles. Proc Natl Acad Sci USA 102:15545–15550
Taanman JW (1999) The mitochondrial genome: structure, transcription, translation and replication. Biochim et Biophys Acta (BBA) - Bioenerg 1410:103–123
Tatarenkov A, Avise JC (2007) Rapid concerted evolution in animal mitochondrial DNA. Proc Biol Sci 274:1795–1798
Thompson J, Brett C, Neuhaus I, Thompson R (2022) DGEobj.utils: differential gene expression (DGE) analysis utility toolkit. R package version 1.0.6. https://cran.rstudio.com/web/packages/DGEobj.utils/index.html. Accessed 1 Oct 2021
Ura H, Togi S, Niida Y (2022) A comparison of mRNA sequencing (RNA-Seq) library preparation methods for transcriptome analysis. BMC Genomics 23:303
Vyas V, Guerra DD, Bok R, Powell T, Jansson T, Hurt KJ (2019) Adiponectin links maternal metabolism to uterine contractility. FASEB J 33:14588–14601
Ward JPT (2017) From physiological redox signalling to oxidant stress. Adv Exp Med Biol 967:335–342
Wick P, Malek A, Manser P, Meili D, Maeder-Althaus X, Diener L et al (2010) Barrier capacity of human placenta for nanosized materials. Environ Health Perspect 118:432–436
Wu T, Hu E, Xu S, Chen M, Guo P, Dai Z et al (2021) clusterProfiler 40: a universal enrichment tool for interpreting omics data. Innovation 2:100141
Yang X, Zhang F, Liu X, Meng J, Du S, Shao J, Liu J et al (2022) FOXO4 mediates resistance to oxidative stress in lens epithelial cells by modulating the TRIM25/Nrf2 signaling. Exp Cell Res 420:113340
Zhang M, Mueller NT, Wang H, Hong X, Appel LJ, Wang X (2018) Maternal exposure to ambient particulate matter </=2.5 microm during pregnancy and the risk for high blood pressure in childhood. Hypertension 72:194–201
Zhu X, Liu Y, Chen Y, Yao C, Che Z, Cao J (2015) Maternal exposure to fine particulate matter (PM2.5) and pregnancy outcomes: a meta-analysis. Environ Sci Pollut Res Int 22:3383–3396
Acknowledgements
The members of the APPO study group are listed below.
Young-Han Kim6, Sung Hun Na7, Mi Hye Park8, Jin-Gon Bae9, Geum Joon Cho10, Soo-Jeong Lee11
6Department of Obstetrics and Gynecology, College of Medicine, Yonsei University, Seoul, Republic of Korea
7Department of Obstetrics and Gynecology, Kangwon National University Hospital, School of Medicine Kangwon National University, Chuncheon, Korea
8Department of Obstetrics and Gynecology, College of Medicine, Ewha Womans University Seoul Hospital, Seoul, Korea
9Department of Obstetrics and Gynecology, Keimyung University Dongsan Medical Center, Daegu, Republic of Korea
10Department of Obstetrics and Gynecology, Korea University, Guro Hospital, Seoul, Korea
11Department of Obstetrics and Gynecology, University of Ulsan College of Medicine, Ulsan University Hospital, Ulsan 44033, Republic of Korea
Funding
This study was supported by the National Institute of Health research project (project No. 2021-ER1208-01) and supported by the RP-Grant 2021 from Ewha Womans University (Young-Ah You).
Author information
Authors and Affiliations
Consortia
Contributions
KYJ: conceptualization, methodology, writing—review and editing, supervision, funding acquisition; KMS: formal analysis, methodology, software, visualization, writing—original draft and review and editing; YAY: investigation, resources, data analysis, writing—original draft; PSW and HYM: PM2.5 data and clinical data curation; KEJ: formal analysis, methodology; KYA: formal analysis, software, visualization; LG and KSM: data curation, manage clinical samples; SJM: data curation; the APPO study group (KYH, NSH, PMH, BJG, CKJ, LSJ): clinical data curation.
Corresponding author
Ethics declarations
Ethics approval
This study was approved by the Ethical Research Committees of the six centers (Ewha Womans University Mokdong Hospital, EUMC 2021–04-032; Ewha Womans University Seoul Hospital, 2021–04-022; Yonsei University Severance Hospital, 4–2021-0414; Kangwon National University Hospital, KNUH-B-2021–04-012–008; Keimyung University Dongsan Medical Center, 2021–04-073; and Korea University Guro Hospital, 2021GR0233) and conducted according to the ethical principles of the Helsinki Declaration.
Consent to participate
All the participants provided written informed consent prior to enrolment.
Consent for publication
All authors declare their consent to publish this article.
Competing interests
The authors declare no competing interests.
Additional information
Responsible Editor: Lotfi Aleya
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
You, YA., Park, S., Kwon, E. et al. Maternal PM2.5 exposure is associated with preterm birth and gestational diabetes mellitus, and mitochondrial OXPHOS dysfunction in cord blood. Environ Sci Pollut Res 31, 10565–10578 (2024). https://doi.org/10.1007/s11356-023-31774-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-023-31774-0