
Abstract
When cooking with biomass and fossil fuels, their incomplete burning can lead to air pollution, which can trigger pernicious effects on people’s health, especially among the elderly, who are more vulnerable to toxic and harmful environmental damage. This study explored the association between different cooking fuel types and the risk of cancer and all-cause mortality among seniors constructing Cox regression models. Data were obtained by linking waves of 6, 7, and 8 of the Chinese Longitudinal Healthy Longevity Survey, which included a total of 7269 participants who were 65 years old and over. Cooking fuels were categorized as either biomass, fossil, or clean fuels. And the effects of switching cooking fuels on death risk were also investigated using Cox regression models. The results indicate that, compared with the users of clean fuels, individuals using biomass or fossil fuels were at a greater death risk for cancer [HR (95% CI): biomass, 1.13 (1.05–1.20); fossil, 1.16 (1.06–1.25)] and all causes [HR (95% CI): biomass, 1.29 (1.16–1.42); fossil, 1.32 (1.22–1.50)]. Furthermore, compared with sustained users of biomass fuels, individuals converting from biomass to clean fuels significantly reduced death risk for cancer [HR (95% CI): 0.81 (0.72–0.95)] and all causes [HR (95% CI): 0.76 (0.64–0.93)]. Similarly, all-cause death risk [HR (95% CI): 0.77 (0.62–0.93)] was noticeably reduced among these participants converting from fossil to clean fuels than persistent users of fossil fuels. Subgroup analyses revealed that males had a greater cancer and all-cause death risk when exposed to unclean fuels. These findings can inform the development of policies and the implementation of measures related to cooking fuel use to promote the health of older people and reduce the burden of disease on society.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Since humans first used wood as fuel to make a fire for cooking, the use and development of cooking fuels have been inextricably linked with human life. Undeniably, biomass fuels (e.g., wood, agricultural residues, and charcoal) and later fossil fuels (e.g., coal, kerosene, gas) do bring many benefits to human life, but at the same time, they have also caused adverse health impacts on people and posed a substantial disease burden to society (Smith et al. 2014). These health impacts mainly include asthma (Mishra 2003; Wong et al. 2013), cardiovascular disease (CVD) (Yu et al. 2018), chronic obstructive pulmonary disease (COPD) (Salvi and Barnes 2009; Lee et al. 2020), cancer (Reid et al. 2012), and all-cause death rate (Yin et al. 2020). Moreover, studies have suggested that incomplete burning of fuels can produce the main toxic pollutants that contribute to household air pollution (HAP) when solid fuels (e.g., biomass fuels and coal) are used for human activities like heating or cooking (Chen et al. 2016; Gordon et al. 2014). And according to the relevant findings of Global Burden of Disease Study, HAP is an environmental risk factor and is associated with more than one million deaths per year globally (GBD 2013 Risk Factors Collaborators 2015; GBD 2017 Risk Factor Collaborators 2018).
As reported by the International Energy Agency (IEA), with the socio-technical and economic developments, although the amount of folks who are unable to cook with clean fuels is gradually decreasing, thanks to some national clean-up programs and policies (International Energy Agency 2022a), globally there are still over 2.5 billion people who primarily use biomass or fossil fuels as of 2019 (International Energy Agency 2022a). In China, despite the country continuing to urbanize, the use of unclean fuels is still a general phenomenon, particularly in some rural areas (Hou et al. 2017) and among the older population (Hystad et al. 2019; Zhang and Smith 2007), where many people still use traditional fuels for cooking. In addition, the number of people cooking with unclean fuels may further increase during the COVID-19 pandemic due to the impacts of the lockdowns and the ensuing stagnation to global economic activities and the disruptions to global supply chains on fuel prices, household incomes, transportation, etc. (International Energy Agency 2022b; Shupler et al. 2021; Ali and Khan 2022; Ravindra et al. 2021).
The earlier studies have confirmed the association between the utilization of cooking fuels and the risk of common diseases in the elderly, such as hypertension, cognitive impairment, and COPD (Deng et al. 2020; Du et al. 2021; Li et al. 2019). The limited physical activities and vulnerable health conditions of the elderly force them to stay more at home, which can expose them to more pollutants generated by cooking fuels. In particular, as people are living longer and the ageing of society in China, Chinese elderly people can also suffer long-term damage from exposure to cooking fuel emissions (Liu et al. 2018, 2020).
Meanwhile, the role of cooking fuel use in mortality has also been the focus of previous studies. One study, for example, found higher risks of cardiovascular, respiratory, and all-cause mortality among users of solid fuels, and these risks can be reduced by discontinuing the utilization of such fuels (Yu et al. 2020). Cancer ranks among the top causes of death worldwide and is more prevalent in older individuals, for whom it poses a greater risk of mortality is greater (Pedersen et al. 2016). Despite this, there is a paucity of research investigating the relationship between cooking fuels and cancer mortality. In addition, the relevant researches have primarily concentrated on biomass fuels, and there is a dearth of studies examining the impact of fossil fuels. Indeed, until recently, kerosene remains a common cooking fuel, and one study found that kerosene use was linked to greater risk of CVD, respiratory disease, and all-cause death by surveying multiple low-income and middle-income countries (Arku et al. 2020). Furthermore, the impacts on the life and health of the elderly of long-term use of a certain cooking fuel and switching the varieties of cooking fuel remain to be studied.
Therefore, given the substantial disease burden on society caused by cooking fuel use and the specificities of the elderly, we need to continually work on the health impacts of diverse types of cooking fuels on elderly people in different circumstances. We constructed cox regression models to concentrated on assessing the relationship of the types of cooking fuels individuals used and the conversion of midway cooking fuel types with the death of cancer and all causes in a nationwide prospective cohort study of older Chinese. The main contributions of our study are (i) adding to the evidence on the association between cooking fuels and cancer mortality in older people, (ii) expanding upon previous research by exploring the use of fossil fuels and providing a more comprehensive classification of cooking fuels, and (iii) the hazards of long-term cooking fuel use in older people and the impact of switching cooking fuel types can be more fully studied through the cohort survey with 8 years of follow-up.
Methods
Study design and participants
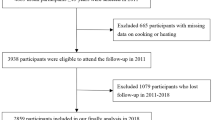
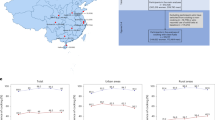
For the present research, data extracted from the Chinese Longitudinal Healthy Longevity Survey (CLHLS) were used for analysis. The CLHLS study was initiated in 1998, and was followed up in 2000 (second wave), 2002 (third wave), 2005 (fourth wave), 2008 (fifth wave), 2011 (sixth wave), 2014 (seventh wave), and 2018 (eighth wave), and fresh participants were recruited at each wave of follow-up. Initially, the CLHLS was conducted in 22 provinces in China, and a total of 23 provinces were eventually covered after adding Hainan Province in the sixth wave. In the first two waves of the survey, only the elderly who were 80 years old and over were recruited, and the seniors aged 65–75 years have also been added to the survey since 2002. Thus, information on the personal health situations and living conditions of Chinese seniors who were 65 years old and over was investigated. Additional details on the designs and methodologies had been presented elsewhere (Lv et al. 2018; Zeng et al. 2017). Only data collected in 2011, 2014, and 2018 were included in our study because information on cooking fuels was not collected during the prior survey waves (first to fifth waves). The baseline information for this study was collected in the sixth wave from 2011 to 2012, which included the question “Which fuel do you usually use for cooking at home?” Subsequent follow-up visits in 2014 and 2018 were conducted through interviewing the surviving participants or with a relative of the deceased participants. At the sixth wave (2011/2012), 9765 Chinese seniors were included in the cohort; the specific distribution of the sample across the 23 provinces in mainland China is shown in Figure S1. After excluding participants who were missed in 2014 (n = 820) and in 2018 (n = 1345), 8945 and 7600 participants (including surviving participants and relatives of deceased participants) remained in the cohort at the seventh wave and the eighth wave, respectively. Then, we further excluded those who had lost cooking fuels data (n = 198), those who never cooked (n = 124), and those who used other cooking fuels (n = 9), respectively. Total 7269 seniors were finally admitted in the analyses. Figure 1 shows greater details about the process of inclusion and exclusion for participants in the research.

The flowchart of the inclusion of available participants
The CLHLS study was implemented with the approval of the Research Ethics Committee of Peking University (IRB00001052-13,074), and an informed consent form was required all participants or proxy interviewees to sign.
Assessment of cooking fuel exposure
Relevant information about participants’ cooking fuel exposure types were measured through a questionnaire, with answering the question “What types of fuel do you usually use for cooking at home?” by the respondents themselves at the baseline interview and by the surviving respondents at follow-up interview. The question “What types of fuel did the participants usually use for cooking before death?” was answered by a relative of the deceased participants at follow-up. Cooking fuels were grouped by type into clean fuel group (including electricity, solar energy, and natural gas), biomass fuel group (including charcoal, firewood and straw), and fossil fuels group (coal, coal oil and coal gas). We carried out comparisons of the predominant use of biomass, fossil and clean fuels. In addition, based on the information on cooking fuel use collected from 2011 to 2018 (a total of 3 waves of surveys), we also compared participants switching cooking fuel types (i.e., primarily cooked with one fuel type at baseline, but switched cooking fuel type to another during follow-up) with those who had not changed their cooking fuel types.
Outcome
Information on participants’ survival status, date of death, and whether they had cancer was obtained by interviewing the surviving participants or with a relative of the deceased participants in 2014 and 2018, respectively. All participants were followed from baseline until their death was ascertained, and follow-up was lost, or July 2018.
Covariates
Confounding factors for potentially influenced cooking fuel use and outcomes were adjusted, with sociodemographic characteristics including age (continuous), gender (male/female), type of residence (rural/urban), education level (illiterate/1–6 years/7 years or more), marital status (married/other), annual household income [low (≤ 10,000 RMB)/medium (10,001–30,000 RMB)/high (≥ 30,001 RMB)], independent living [yes (living alone)/no (living with family or living in an aged care facility], and geographical location (North, Hebei, Beijing, Shanxi, Tianjin; Northeast, Jilin, Liaoning, Heilongjiang; East, Jiangxi, Jiangsu, Shanghai, Zhejiang, Fujian; Center, Henan, Shandong, Hubei, Anhui, Hunan; South, Guangdong, Hainan, Guangxi; West, Shaanxi, Sichuan, Chongqing), lifestyle factors including smoking behavior (never/past/current) and drinking behavior (never/past/current), and health status including body mass index [BMI, obese (≥ 28)/overweight (24–27.9)/normal(18.5–23.9)/underweight (< 18.5)], limited in activities (yes/no), and comorbidities (stroke, hypertension, diabetes, heart disease, cancer and dementia; yes/no).
Statistical analysis
Participants were grouped according to cooking fuel type, and mean ± standard deviation and frequencies with percentages were used to conduct descriptive analyses of continuous variables and categorical variables of their baseline characteristics, respectively. The chi-square test and ANOVA were applied to categorical variables and continuous variables to test the statistical significance of differences in the kinds of cooking fuel used between the different characteristic subgroups, respectively. Three Cox regression models were constructed to examine the relationship of the utilization of cooking fuels with cancer and all-cause mortality by adjusting for different covariates, and results were expressed in terms of hazard ratio (HR) with a 95% confidence interval (CI). See supplementary document 1 for the mathematical form and construction of the Cox regression model. Model 1 was the unadjusted model. Model 2 was adjusted for sex, age, education level, smoking behavior, drinking behavior, marital status, annual household income, BMI, and independent living. Model 3 was further adjusted for comorbidities, type of residence, and geographic location based on model 2. Hazard ratios describing the relationship of converting cooking fuel types with cancer and all-cause mortality were also estimated by these models. Furthermore, we performed subgroup analyses tiered by sex, smoking behavior, drinking behavior, type of residence, and geographic location to reveal the relationship of cooking fuel use or converting cooking fuel types with the death of cancer and all causes in different subgroups.
Sensitivity analyses were carried out to ensure the robustness of the major analysis results. Firstly, we removed the data that did not have complete information of participants. Secondly, we removed the data of deceased participants in the initial year of this study period. Thirdly, we further adjusted other potential variables, including limited activities, dementia, and type of residence.
All analyses were based on two-sided tests, and statistical significance was indicated when p < 0.05. The statistical tests were all carried out using R software version 4.0.5 (R Foundation for Statistical Computing). See supplementary document 1 for the resource and system characteristics.
Results
Description of participants’ baseline characteristics
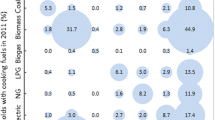
Table 1 contains information on the characteristics of participants at baseline. Total 7269 participants were admitted in this study, of which 3983 were females (54.79%). Their mean (SD) age approximately was 86.03 (11.39) years. According to the baseline report, 3429 (47.17%) participants cooked with biomass fuels and 2300 (31.64%) participants cooked with fossil fuels. Most of the participants who cooked with biomass fuels were illiterate (65.30 vs. 52.02%), had low annual household income (47.54 vs. 20.39%), were currently smoking (19.11 vs. 16.08%), never drink (69.74 vs. 66.51%), were underweight (30.38 vs. 26.59%), were not living independently (19.07 vs. 11.93%), and were rural (98.09% vs. 67.27%) compared with those who were the users of clean fuels. To further explore survival status, all-cause mortality, and cancer mortality among participants at baseline, we also conducted analyses grouped by participants’ different characteristics (Table S1). Long-term follow-up leads to a decrease in follow-up rate, so we compared the baseline characteristics of the population who were failed to follow with those who were followed up successfully, and found no significant differences between the two populations for sex and drinking behavior (Table S2).
Relationship of cooking fuels use with cancer and all-cause mortality
Table 2 summarizes the results of the analysis of the relationship between cooking fuel types and the death of cancer and all causes. During the investigation period from 2011 to 2018, 4195 deaths were ascertained, of which 246 deaths were from cancer. All unadjusted and multivariable-adjusted models showed that biomass fuel or fossil fuel users had a higher death risk for cancer and all causes than clean fuel users. In model 1 (i.e., unadjusted model), being biomass fuel users [HR (95% CI): cancer, 1.14 (1.07–1.21); all causes, 1.40 (1.25–1.56)] and being fossil fuel users [HR (95% CI): cancer, 1.18 (1.10–1.26); all causes, 1.33 (1.19–1.46)] were risk factors for cancer and all-cause deaths. Model 3 still showed that being biomass fuel users [HR (95% CI): cancer, 1.13 (1.05–1.20); all causes, 1.29 (1.16–1.42)] and being fossil fuel users [HR (95% CI): cancer, 1.16 (1.06–1.25); all causes, 1.32 (1.22–1.50)] were risk factors for cancer and all-cause deaths. Moreover, compared with participants who were the users of biomass fuels, fossil fuel users can bring a more significant effect on the death risk for cancer and all causes in the two adjusted models.
Relationship of converting cooking fuel types (2014) with cancer and all-cause mortality
Of the 902 survivors who were clean fuel users at baseline, 541 participants continued to use clean fuels and 129 participants converted from clean to biomass fuels, 232 participants converted from clean to fossil fuels at follow-up in 2014, respectively. Crude rates of cancer and all-cause death events were greater for participants reporting a conversion from clean to fossil or biomass fuels between 2014 and 2018 than for the sustained users of clean fuels (cancer, 5.1, 4.0, and 6.5/1000 person-years; all causes, 57.7, 72.5, and 64.9/1000 person-years), but no meaningful relationship was found between converting from clean to fossil or biomass fuels and death risk for cancer and all causes (Table 3). Of the 2143 survivors who were biomass fuel users at baseline, 1463 participants remained on biomass fuels and 247 participants converted from biomass to clean fuels, 433 participants converted from biomass to fossil fuels at follow-up in 2014, respectively. And all unadjusted and multivariable-adjusted models showed that compared with participants who were the sustained users of biomass fuels, those converting from biomass to clean fuels had a noticeably lower death risk for cancer [HR (95% CI): model 1, 0.82 (0.72–0.94); model 3, 0.81 (0.72–0.95)] and all causes [HR (95% CI): model 1, 0.74 (0.65–0.88); model 3, 0.76 (0.64–0.93)] (Table 3). Of the 1316 survivors who were fossil fuel users at baseline, 854 participants continued to use fossil fuels and 289 participants converted from fossil to clean fuels, 173 participants converted from fossil to biomass fuels at follow-up in 2014, respectively. And the results showed that compared with participants who were the sustained users of fossil fuels, those converting from fossil to clean fuels had a lesser death risk for all causes [HR (95% CI): model 1, 0.84 (0.71–0.99); model 3, 0.77 (0.62–0.93)], while no evidence was found for a relationship between converting from fossil to clean fuels and cancer mortality [HR (95% CI): model 1, 0.97 (0.84–1.11); model 3, 0.93 (0.81–1.08)] (Table 3). We also found that compared with participants who were the sustained users of fossil fuels, those converting from fossil to biomass fuels were at a greater death risk for cancer [HR (95% CI): model 1, 1.22 (1.06–1.46); model 3, 1.27 (1.06–1.49)] and all causes [HR (95% CI): model 1, 1.28 (1.06–1.55); model 3, 1.29 (1.05–1.58)] (Table 3).
Subgroup analyses
We performed a gender-stratified subgroup analysis to discuss the relationship of cooking fuel types with the death risk for cancer and all causes. All unadjusted and multivariable-adjusted models revealed that compared with clean fuel users, cooking with biomass or fossil fuels was positively related to the death risk for cancer and all causes in both two subgroups (Table 4). Compared with females, the use of biomass or fossil cooking fuels had a greater effect on the death risk for cancer and all causes in males (Table 4). After stratifying by sex, we also explored the relationship of converting cooking fuel types with cancer and all-cause mortality in two subgroups (Table S3). In addition, we discussed the relationship of cooking fuel types with cancer and all-cause mortality stratified by drinking behavior, smoking behavior, type of residence, and geographic location and found that rural biomass or fossil fuel users had a greater death risk for cancer and all causes (Table S4).
Sensitivity analyses
When we removed the data of participants with any missing values in the information (Table S5), further removed the data of deceased participants in the initial year of this study period (Table S6), or further adjusted for potential variables (including limited in activities, dementia, and ventilation) (Table S7), it was still shown that participants who cooked with biomass or fossil fuels had a greater death risk for cancer and all causes than those cooking with clean fuels. As shown in Table S7, compared with using clean fuels for cooking, using biomass fuels increased the death risk of cancer by 14.7% (HR = 1.147, 95% CI: 1.046–1.264) and all causes by 20.7% (HR = 1.207, 95% CI: 1.076–1.311), respectively; using fossil fuels also increased the death risk of cancer by 21.9% (HR = 1.219, 95% CI: 1.110–1.331) and all causes by 31.4% (HR = 1.314, 95% CI: 1.140–1.455), respectively. Thus, our results were robust.
Discussion
Our study revealed that the usage of biomass or fossil cooking fuels was strongly related to a greater death risk for cancer and all causes. Participants who converted from biomass or fossil to clean fuels resulted in an evident reduction in death risk compared to those who use biomass fuels sustainably. And no evidence was found that switching from clean to fossil or biomass fuels was related to a lower death risk for cancer and all causes. In subgroup analyses, we found that males were at greater death risk for cancer and all causes when cooking with biomass or fossil fuels.
The findings of some studies are concordant with our results. For instance, a study of 31,490 participants aged 35–70 years in China, Tanzania, South Africa, and India indicated that individuals cooking with kerosene fuel had a greater death risk for all causes (HR = 1.32, 95% CI: 1.14–1.53) than clean fuel users (Arku et al. 2020). Similarly, another study of 55,687 participants among China’s rural population revealed that participants who cooked with solid fuels, primarily biomass, had a greater death risk for all causes (HR = 1.11, 95% CI: 1.02–1.26) than clean fuel users (Qiu et al. 2021). Same as the previous researches (Yu et al. 2018; Chan et al. 2019; Xu et al. 2022), our study demonstrated that converting from unclean to clean fuels can potentially reduce the death risk, suggesting that cooking with unclean fuels is an independent risk contributor to health problems in seniors. However, no evidence was observed for the correlation between converting from clean to unclean fuels and the death risk for cancer and all causes, as compared with consistently using clean fuels. The reasons for this are unknown in this study, but we speculate that this result may be related to the time duration and toxicity of polluting gases emitted from cooking fuels. Health damage from exposure to air pollution may be impacted by many factors (e.g., level and duration of exposure) (Li et al. 2018; Brook et al. 2010). One study also showed that the unobserved effect between the utilization of solid fuels and death risk can be explained by insufficient exposure duration (Mitter et al. 2016). Therefore, in our study, insufficient exposure time duration to pollutants after switching cooking fuel types may influence the association with mortality risk.
Some studies have presented ideas that are inconsistent with our results. An urban and rural epidemiology study recruited 91,350 individuals in 11 low-income and middle-income countries found no statistically significant difference in the death risk for all causes (HR = 1.12, 95% CI: 0.95–1.31) between cooking with clean fuels like natural gas and using solid fuels like wood or charcoal (Hystad et al. 2019). Moreover, Yu et al. (Yu et al. 2020) and Mitter et al. (Mitter et al. 2016) found that cooking with unclean fuels posed a greater death risk for all causes in women than men. However, in our study, the risk of all-cause death for men was greater than that of women. In general, women are more likely to cook in families. However, if men are unmarried, divorced, or widowed, they will be more likely to cook by themselves. Thus, the high proportion of unmarried, divorced, or widowed in this male population we studied may increase men’s exposure to unclean cooking fuels. In addition, men are more probably to smoke and drink than women. The effects of these factors on health may enhance the death risk for males.
There were two studies from the same population as our study, one focused on exploring the association between biomass fuels (firewood/straw, charcoal) and mortality risk (Xu et al. 2022), and the other focused on solid fuels (coal, charcoal, firewood, wood, and animal dung) (Shen et al. 2021). However, these two studies focused only on all-cause mortality. Unlike their findings, our study added a section on the death risk for cancer and specifically investigated the impacts of switching among different cooking fuel types on the death risk for cancer and all causes during the follow-up period. Our study is more representative of the overall mortality risk than those studies focused on exploring the correlation between the utilization of cooking fuels and death risk of a specific disease (e.g., lung, liver, and gastrointestinal cancers) (Barone-Adesi et al. 2012; Chan et al. 2020; Sheikh et al. 2020). Furthermore, the definite mechanisms of how cooking fuels affect the health of individuals are unclear, but researches have suggested that different types of fuel combustion would produce different emissions of air pollutants (Chen et al. 2017; Smith et al. 2014), resulting in different health effects. So, our study classified cooking fuel exposure types in more detail including clean fuels, biomass fuels, and fossil fuels, which is different from other studies. Another important reason is that the target population of the study is different, as our study population is predominantly middle- and high-aged elderly in urban and rural areas, who average 86.03 years old and has a more equal proportion of men and women. These are a good supplement to further explore the effects of diverse cooking fuels on the death risk for cancer and all causes.
There are a few limitations to this study. First, due to the shortage of accurate information on participants’ exposure doses, exposure durations, and household air pollutants, we were unable to explore the dose–response mechanisms associated with health impairment in the elderly because of the use of cooking fuels. Second, we only investigated whether participants converted cooking fuel types, but ignored the accurate time of change and subsequent duration of use, so we were unavailable to assess the effect of converting cooking fuel types on the death risk in seniors on a time scale. Third, a comprehensive investigation of factors affecting air pollution exposure in the elderly, such as the use of ventilated facilities and ventilated cook stoves, was also missing from the baseline survey, which may be associated with a lower death risk (Yu et al. 2020; Hystad et al. 2019). Fourth, despite the best efforts of the project staff, this study still has a high loss of follow-up rate (22.17%). The results may be affected by the significant differences between the baseline education level, marital status, household income level, registered residence type, and geographical region of people in different response states. Fifth, the utilization of biomass and fossil fuels is more prevalent in rural areas than in urban areas, and urban areas have better economic level and kitchen ventilation facilities than rural areas, which will increase the death risk in rural areas. Finally, the differences in air quality among geographical regions will also bias the results. For example, due to fossil fuel heating, the air quality in Northeast China is more varied than that in South China, which leads to a greater death risk for cancer and all causes in Northeast China than in South China. Although we have already made adjustments for various confounding factors related to mortality, there may still be unknown residual confounding. Therefore, we need to advance related studies constantly in future research.
Conclusions
Our study clearly established that cooking with biomass and fossil fuels is positively related to the death risk for all-cause and cancer among the elderly in China, especially for males, and that converting from biomass or fossil to clean fuels may lead to reduced risk of death. Based on these results, this study highlights the significance of the adverse effects caused by fossil fuels and emphasizes that the utilization of unclean fuels is a risk factor for cancer in the elderly population. Furthermore, the study suggests the need for more research on gender differences in the detrimental effects of cooking fuel usage. Accelerating the implementation of measures and policies to replace unclean fuels with clean ones in some human activities like cooking or heating is significant for reducing health impairment in the elderly and reducing the burden of disease in society.
Data availability
The CLHLS questionnaires are available at https://sites.duke.edu/centerforaging/programs/chinese-longitudinal-healthy-longevity-survey-clhls/survey-documentation/questionnaires/. The full datasets used in this analysis are available upon reasonable request.
References
Ali J, Khan W (2022) Factors affecting access to clean cooking fuel among rural households in India during COVID-19 pandemic. Energy Sustain Dev 67:102–111. https://doi.org/10.1016/j.esd.2022.01.006
Arku RE, Brauer M, Duong M, Wei L, Hu B, Ah Tse L, Mony PK, Lakshmi PVM, Pillai RK, Mohan V, Yeates K, Kruger L, Rangarajan S, Koon T, Yusuf S, Hystad P, investigators PS, (2020) Adverse health impacts of cooking with kerosene: A multi-country analysis within the Prospective Urban and Rural Epidemiology Study. Environ Res 188:109851. https://doi.org/10.1016/j.envres.2020.109851
Barone-Adesi F, Chapman RS, Silverman DT, He X, Hu W, Vermeulen R, Ning B, Fraumeni JF Jr, Rothman N, Lan Q (2012) Risk of lung cancer associated with domestic use of coal in Xuanwei, China: retrospective cohort study. BMJ 345:e5414. https://doi.org/10.1136/bmj.e5414
Brook RD, Rajagopalan S, Pope CA 3rd, Brook JR, Bhatnagar A, Diez-Roux AV, Holguin F, Hong Y, Luepker RV, Mittleman MA, Peters A, Siscovick D, Smith SC Jr, Whitsel L, Kaufman JD, American Heart Association Council on E, Prevention CotKiCD, Council on Nutrition PA,Metabolism (2010) Particulate matter air pollution and cardiovascular disease: An update to the scientific statement from the American Heart Association. Circulation 121:2331–78. https://doi.org/10.1161/CIR.0b013e3181dbece1
Chan KH, Kurmi OP, Bennett DA, Yang L, Chen Y, Tan Y, Pei P, Zhong X, Chen J, Zhang J, Kan H, Peto R, Lam KBH, Chen Z, China Kadoorie Biobank Collaborative G (2019) Solid Fuel Use and Risks of Respiratory Diseases. A Cohort Study of 280,000 Chinese Never-Smokers. Am J Respir Crit Care Med 199:352–61. https://doi.org/10.1164/rccm.201803-0432OC
Chan KH, Bennett DA, Kurmi OP, Yang L, Chen Y, Lv J, Guo Y, Bian Z, Yu C, Chen X, Dong C, Li L, Chen Z, Lam KBH, China Kadoorie Biobank Study G (2020) Solid fuels for cooking and tobacco use and risk of major chronic liver disease mortality: a prospective cohort study of 0.5 million Chinese adults. Int J Epidemiol 49:45–55. https://doi.org/10.1093/ije/dyz216
Chen Y, Shen G, Liu W, Du W, Su S, Duan Y, Lin N, Zhuo S, Wang X, Xing B, Tao S (2016) Field measurement and estimate of gaseous and particle pollutant emissions from cooking and space heating processes in rural households, northern China. Atmos Environ 125:265–271. https://doi.org/10.1016/j.atmosenv.2015.11.032
Chen J, Li C, Ristovski Z, Milic A, Gu Y, Islam MS, Wang S, Hao J, Zhang H, He C, Guo H, Fu H, Miljevic B, Morawska L, Thai P, Lam YF, Pereira G, Ding A, Huang X, Dumka UC (2017) A review of biomass burning: Emissions and impacts on air quality, health and climate in China. Sci Total Environ 579:1000–1034. https://doi.org/10.1016/j.scitotenv.2016.11.025
Deng Y, Gao Q, Yang D, Hua H, Wang N, Ou F, Liu R, Wu B, Liu Y (2020) Association between biomass fuel use and risk of hypertension among Chinese older people: A cohort study. Environ Int 138:105620. https://doi.org/10.1016/j.envint.2020.105620
Du M, Tao L, Zhu L, Liu J (2021) Association between biomass fuel use and the risk of cognitive impairment among older populations in China: a population-based cohort study. Environ Health 20:21. https://doi.org/10.1186/s12940-021-00706-1
GBD 2013 Risk Factors Collaborators (2015) Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks in 188 countries, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. The Lancet 386:2287–2323. https://doi.org/10.1016/s0140-6736(15)00128-2
GBD 2017 Risk Factor Collaborators (2018) Risk Factor Collaborators (2018) Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. The Lancet 392:1923–1994. https://doi.org/10.1016/s0140-6736(18)32225-6
Gordon SB, Bruce NG, Grigg J, Hibberd PL, Kurmi OP, K-bH L, Mortimer K, Asante KP, Balakrishnan K, Balmes J, Bar-Zeev N, Bates MN, Breysse PN, Buist S, Chen Z, Havens D, Jack D, Jindal S, Kan H, Mehta S, Moschovis P, Naeher L, Patel A, Perez-Padilla R, Pope D, Rylance J, Semple S, Martin WJ (2014) Respiratory risks from household air pollution in low and middle income countries. Lancet Respir Med 2:823–860. https://doi.org/10.1016/s2213-2600(14)70168-7
Hou BD, Tang X, Ma C, Liu L, Wei YM, Liao H (2017) Cooking fuel choice in rural China: results from microdata. J Clean Prod 142:538–547. https://doi.org/10.1016/j.jclepro.2016.05.031
Hystad P, Duong M, Brauer M, Larkin A, Arku R, Kurmi OP, Fan WQ, Avezum A, Azam I, Chifamba J, Dans A, du Plessis JL, Gupta R, Kumar R, Lanas F, Liu Z, Lu Y, Lopez-Jaramillo P, Mony P, Mohan V, Mohan D, Nair S, Puoane T, Rahman O, Lap AT, Wang Y, Wei L, Yeates K, Rangarajan S, Teo K, Yusuf S (2019) Health Effects of Household Solid Fuel Use: Findings from 11 Countries within the Prospective Urban and Rural Epidemiology Study. Environ Health Perspect 127:57003. https://doi.org/10.1289/EHP3915
International Energy Agency (2022a) SDG7: Data and Projections. IEA, Paris, France. https://www.iea.org/reports/sdg7-data-and-projections. Accessed 2023-01-10
International Energy Agency (2022b) Tracking SDG7: The Energy Progress Report. IEA, Paris, France. https://www.iea.org/reports/tracking-sdg7-the-energy-progress-report-2022b. Accessed 2023-01-10
Lee KK, Bing R, Kiang J, Bashir S, Spath N, Stelzle D, Mortimer K, Bularga A, Doudesis D, Joshi SS, Strachan F, Gumy S, Adair-Rohani H, Attia EF, Chung MH, Miller MR, Newby DE, Mills NL, McAllister DA, Shah ASV (2020) Adverse health effects associated with household air pollution: a systematic review, meta-analysis, and burden estimation study. Lancet Glob Health 8:e1427–e1434. https://doi.org/10.1016/s2214-109x(20)30343-0
Li T, Zhang Y, Wang J, Xu D, Yin Z, Chen H, Lv Y, Luo J, Zeng Y, Liu Y, Kinney PL, Shi X (2018) All-cause mortality risk associated with long-term exposure to ambient PM2·5 in China: a cohort study. Lancet Public Health 3:e470–e477. https://doi.org/10.1016/s2468-2667(18)30144-0
Li J, Qin C, Lv J, Guo Y, Bian Z, Zhou W, Hu J, Zhang Y, Chen J, Cao W, Yu C, Li L (2019) Solid Fuel Use and Incident COPD in Chinese Adults: Findings from the China Kadoorie Biobank. Environ Health Perspect 127:57008. https://doi.org/10.1289/EHP2856
Liu J, Hou B, Ma XW, Liao H (2018) Solid fuel use for cooking and its health effects on the elderly in rural China. Environ Sci Pollut Res Int 25:3669–3680. https://doi.org/10.1007/s11356-017-0720-9
Liu Z, Li J, Rommel J, Feng S (2020) Health impacts of cooking fuel choice in rural China. Energy Econ 89:104811. https://doi.org/10.1016/j.eneco.2020.104811
Lv YB, Gao X, Yin ZX, Chen HS, Luo JS, Brasher MS, Kraus VB, Li TT, Zeng Y, Shi XM (2018) Revisiting the association of blood pressure with mortality in oldest old people in China: community based, longitudinal prospective study. BMJ 361:k2158. https://doi.org/10.1136/bmj.k2158
Mishra V (2003) Effect of indoor air pollution from biomass combustion on prevalence of asthma in the elderly. Environ Health Perspect 111:71–78. https://doi.org/10.1289/ehp.5559
Mitter SS, Vedanthan R, Islami F, Pourshams A, Khademi H, Kamangar F, Abnet CC, Dawsey SM, Pharoah PD, Brennan P, Fuster V, Boffetta P, Malekzadeh R (2016) Household Fuel Use and Cardiovascular Disease Mortality: Golestan Cohort Study. Circulation 133:2360–2369. https://doi.org/10.1161/CIRCULATIONAHA.115.020288
Pedersen JK, Engholm G, Skytthe A, Christensen K (2016) Cancer and aging: Epidemiology and methodological challenges. Acta Oncol 55(Suppl 1):7–12. https://doi.org/10.3109/0284186x.2015.1114670
Qiu S, Chen X, Chen X, Luo G, Guo Y, Bian Z, Li L, Chen Z, Wu X, Ji JS (2021) Solid fuel use, socioeconomic indicators and risk of cardiovascular diseases and all-cause mortality: a prospective cohort study in a rural area of Sichuan, China. Int J Epidemiol. https://doi.org/10.1093/ije/dyab191
Ravindra K, Kaur-Sidhu M, Mor S, Chakma J, Pillarisetti A (2021) Impact of the COVID-19 pandemic on clean fuel programmes in India and ensuring sustainability for household energy needs. Environ Int 147:106335. https://doi.org/10.1016/j.envint.2020.106335
Reid BC, Ghazarian AA, DeMarini DM, Sapkota A, Jack D, Lan Q, Winn DM, Birnbaum LS (2012) Research opportunities for cancer associated with indoor air pollution from solid-fuel combustion. Environ Health Perspect 120:1495–1498. https://doi.org/10.1289/ehp.1204962
Salvi SS, Barnes PJ (2009) Chronic obstructive pulmonary disease in non-smokers. Lancet 374:733–743. https://doi.org/10.1016/s0140-6736(09)61303-9
Sheikh M, Poustchi H, Pourshams A, Khoshnia M, Gharavi A, Zahedi M, Roshandel G, Sepanlou SG, Fazel A, Hashemian M, Abaei B, Sotoudeh M, Nikmanesh A, Merat S, Etemadi A, Moghaddam SN, Islami F, Kamangar F, Pharoah PD, Dawsey SM, Abnet CC, Boffetta P, Brennan P, Malekzadeh R (2020) Household Fuel Use and the Risk of Gastrointestinal Cancers: The Golestan Cohort Study. Environ Health Perspect 128:67002. https://doi.org/10.1289/EHP5907
Shen S, Luo M, Meng X, Deng Y, Cheng S (2021) All-Cause Mortality Risk Associated With Solid Fuel Use Among Chinese Elderly People: A National Retrospective Longitudinal Study. Front Public Health 9:741637. https://doi.org/10.3389/fpubh.2021.741637
Shupler M, Mwitari J, Gohole A, Anderson de Cuevas R, Puzzolo E, Cukic I, Nix E,Pope D (2021) COVID-19 impacts on household energy & food security in a Kenyan informal settlement: The need for integrated approaches to the SDGs. Renew Sustain Energy Rev 144: None. https://doi.org/10.1016/j.rser.2021.111018
Smith KR, Bruce N, Balakrishnan K, Adair-Rohani H, Balmes J, Chafe Z, Dherani M, Hosgood HD, Mehta S, Pope D, Rehfuess E, Group HCRE (2014) Millions dead: how do we know and what does it mean? Methods used in the comparative risk assessment of household air pollution. Annu Rev Public Health 35:185–206. https://doi.org/10.1146/annurev-publhealth-032013-182356
Wong GWK, Brunekreef B, Ellwood P, Anderson HR, Asher MI, Crane J, Lai CKW (2013) Cooking fuels and prevalence of asthma: a global analysis of phase three of the International Study of Asthma and Allergies in Childhood (ISAAC). Lancet Respir Med 1:386–394. https://doi.org/10.1016/S2213-2600(13)70073-0
Xu M, Ke P, Wang C, Di H, Meng X, Xia W, Gan Y, He Y, Tian Q, Jiang H, Lu Z (2022) Cooking with biomass fuels and mortality among Chinese elderly people: A prospective cohort study. Indoor Air 32:e12954. https://doi.org/10.1111/ina.12954
Yin P, Brauer M, Cohen AJ, Wang H, Li J, Burnett RT, Stanaway JD, Causey K, Larson S, Godwin W, Frostad J, Marks A, Wang L, Zhou M, Murray CJL (2020) The effect of air pollution on deaths, disease burden, and life expectancy across China and its provinces, 1990–2017: an analysis for the Global Burden of Disease Study 2017. Lancet Planet Health 4:e386–e398. https://doi.org/10.1016/s2542-5196(20)30161-3
Yu K, Qiu G, Chan KH, Lam KH, Kurmi OP, Bennett DA, Yu C, Pan A, Lv J, Guo Y, Bian Z, Yang L, Chen Y, Hu FB, Chen Z, Li L, Wu T (2018) Association of Solid Fuel Use With Risk of Cardiovascular and All-Cause Mortality in Rural China. JAMA 319:1351–1361. https://doi.org/10.1001/jama.2018.2151
Yu K, Lv J, Qiu G, Yu C, Guo Y, Bian Z, Yang L, Chen Y, Wang C, Pan A, Liang L, Hu FB, Chen Z, Li L, Wu T, Chen J, Chen Z, Clarke R, Collins R, Guo Y, Li L, Lv J, Peto R, Walters R, Avery D, Boxall R, Chang Y, Chen Y, Chen Z, Clarke R, Du H, Gilbert S, Hacker A, Hill M, Holmes M, Iona A, Kartsonaki C, Kerosi R, Kong L, Kurmi O, Lancaster G, Lewington S, Lin K, McDonnell J, Millwood I, Nie Q, Radhakrishnan J, Ryder P, Sansome S, Schmidt D, Sherliker P, Sohoni R, Stevens B, Turnbull I, Walters R, Wang J, Wang L, Wright N, Yang L, Yang X, Bian Z, Guo Y, Han X, Hou C, Lv J, Pei P, Liu C, Tan Y, Yu C, Pang Z, Gao R, Li S, Wang S, Liu Y, Du R, Zang Y, Cheng L, Tian X, Zhang H, Zhai Y, Ning F, Sun X, Li F, Lv S, Wang J, Hou W, Zeng M, Jiang G, Zhou X, Yang L, He H, Yu B, Li Y, Xu Q, Kang Q, Guo Z, Wang D, Hu X, Wang H, Chen J, Fu Y, Fu Z, Wang X, Weng M, Guo Z, Wu S, Li Y, Li H, Fu Z, Wu M, Zhou Y, Zhou J, Tao R, Yang J, Su J, Liu F, Zhang J, Hu Y, Lu Y, Ma L, Tang A, Zhang S, Jin J, Liu J, Tang Z, Chen N, Huang Y, Li M, Meng J, Pan R, Jiang Q, Lan J, Liu Y, Wei L, Zhou L, Chen N, Wang P, Meng F, Qin Y, Wang S, Wu X, Zhang N, Chen X, Zhou W, Luo G, Li J, Chen X, Zhong X, Liu J, Sun Q, Ge P, Ren X, Dong C, Zhang H, Mao E, Wang X, Wang T, Zhang X, Zhang D, Zhou G, Feng S, Chang L, Fan L, Gao Y, He T, Sun H, He P, Hu C, Zhang X, Wu H, He P, Yu M, Hu R, Wang H, Qian Y, Wang C, Xie K, Chen L, Zhang Y, Pan D, Gu Q, Huang Y, Chen B, Yin L, Liu H, Fu Z, Xu Q, Xu X, Zhang H, Long H, Li X, Zhang L, Qiu Z (2020) Cooking fuels and risk of all-cause and cardiopulmonary mortality in urban China: a prospective cohort study. Lancet Glob Health 8:e430–e439. https://doi.org/10.1016/s2214-109x(19)30525-x
Zeng Y, Feng Q, Hesketh T, Christensen K, Vaupel JW (2017) Survival, disabilities in activities of daily living, and physical and cognitive functioning among the oldest-old in China: a cohort study. The Lancet 389:1619–1629. https://doi.org/10.1016/s0140-6736(17)30548-2
Zhang JJ, Smith KR (2007) Household air pollution from coal and biomass fuels in China: measurements, health impacts, and interventions. Environ Health Perspect 115:848–855. https://doi.org/10.1289/ehp.9479
Acknowledgements
We are very grateful to all the participants and all the staff who contributed to the data collection and collation in this study.
Funding
The CLHLS was supported by funds from the US National Institute on Aging (NIA), the China Natural Science Foundation, the China Social Science Foundation, and the United Nations Fund for Population Activities (UNFPA) and was managed by the Center for Healthy Aging and Development Studies, Peking University.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Conceptualization, methodology, formal analysis, data curation, design and data analysis were performed by Gang Tian. The first draft of the manuscript, validation, and figures were performed by Yulan Ma. Assisting with drafting, writing, review and editing the paper by Yiran Cui and Wenyan Yang. The manuscript prepared for publication by Jingliang Shuai. Conceptualization, funding acquisition, supervision, and guidance at all stages including the analyses were performed by Yan Yan.
Corresponding author
Ethics declarations
Ethical approval
The CLHLS study was implemented with the approval of the Research Ethics Committee of Peking University (IRB00001052-13074).
Consent to participate
Informed written consent was taken voluntarily from each eligible participant or proxy interviewee.
Consent to publish
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Responsible Editor: Lotfi Aleya
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.

Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

{kind=link}
Cite this article
Tian, G., Ma, Y., Cui, Y. et al. Association of cooking fuel use with risk of cancer and all-cause mortality among Chinese elderly people: a prospective cohort study. Environ Sci Pollut Res 30, 78653–78664 (2023). https://doi.org/10.1007/s11356-023-27873-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-023-27873-7