
Abstract
To evaluate the relationships between maternal particulate matter exposure and offspring birth weight. Studies were categorized into three subgroups: term low birth weight (TLBW) among full-term births and all births (regardless of gestational age) and low birth weight (LBW) among all births, based on the search results of MEDLINE and the Web of Science from the inception of the database to April 2022. Subgroup analyses were conducted based on the economic status, region, exposure assessment, risk of bias, and adjustment. Sixty-one studies involving 34,506,975 singleton live births in 15 countries were analyzed. Overall, the risk of bias for most studies (75%) was low. In 39 of 47 term birth studies, the pooled odds ratio of TLBW among term births for per interquartile range (IQR) increases throughout the entire pregnancy was 1.02 (1.01 to 1.03) for PM2.5 and 1.03 (1.01 to 1.05) for PM10 after adjustment for covariates. No significant relevance was detected across each trimester period for PM2.5. A stronger effect was observed during the second trimester (1.03, 1.01 to 1.06) for PM10. There was no increased risk of TLBW in all births associated with IQR increases in PM2.5 and PM10. LBW was associated with PM2.5 exposure in 4 of 7 studies, but statistical heterogeneity was considerable. In the TLBW subgroup analysis, the effects of PM2.5 and PM10 were both greater in studies conducted in advanced countries, studies with low bias, and studies that adjusted for maternal age, infant sex, and parity. Stronger effects were present for PM2.5 exposure collected from monitoring stations and PM10 exposure interpolated from the inverse distance weighting model. TLBW may be associated with prenatal exposure to particulate matter, but no critical windows were identified. Stronger associations were observed in advanced countries. Future original study designs need to consider the impact of different exposure assessment modalities and all possible confounding factors.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The global illness burden attributable to particulate matter (PM) exposure has been exacerbated (Lim et al. 2012; GBD 2019 Risk Factors Collaborators 2020). PM is a component of the atmosphere consisting of both solid particles and liquid droplets, mainly produced by human activities such as manufacturing, transportation, cooking, fuel combustion, and biomass burning (Daellenbach et al. 2020; U.S. Environmental Protection Agency 2019). Increasing epidemiologic evidence is indicating that ambient PM pollution is linked to unfavorable health impacts including total (nonaccidental) mortality (Franklin et al. 2007; Thurston et al. 2016), increased hospital admissions for major cardiovascular disease (Tian et al. 2019), a contributor to deaths from chronic obstructive pulmonary disease (Li et al. 2020a, b), and adverse birth outcomes (Yuan et al. 2019).
Birth weight is a significant indicator of the health and nutrition of both mother and infant. In 2015, low birth weight (LBW) affected about 15% of all newborns around the world (Blencowe et al. 2019), jeopardizing their survival, health, and development. Triggers of fetal growth restriction, particularly in vulnerable populations, are associated with progress toward the global nutrition goal of reducing the prevalence of LBW by 30 percent between 2012 and 2025 (WHO 2014). In addition to several determinants including hereditary, socioeconomic, dietary, and maternal complications during pregnancy (Kramer 1987), several studies have also correlated birth weight with prenatal exposure to particulate matter (Hung et al. 2023; Rosa et al. 2017a).
Several possible mechanisms could explain the impact of prenatal PM exposure on maternal and newborn health. One likely pathway manifested through inflammatory stress and endothelial function is the cardiovascular mechanisms (Brunst et al. 2018; Grevendonk et al. 2016; Rosa et al. 2017b; Kannan et al. 2006). More recent studies indicate that air pollutants (carbon nanoparticles) inhaled by pregnant women can cross the placenta and enter multiple organs such as the lungs, liver, and brain of the fetus (Bongaerts et al. 2022). Epigenetic marks of gestational PM exposure discovered in the placenta and cord blood, such as DNA methylation, histone H3 modifications, and telomere length, may also play an important role (Aguilera et al. 2022; Zhao et al. 2021; Zheng et al. 2017; Martens et al. 2017).
Despite the establishment of pathways and biological processes, causality determinations for PM exposure and birth outcomes were classified as “suggestive, but insufficient or inadequate to infer” by the United States Environmental Protection Agency (EPA) based on current research (U.S. Environmental Protection Agency 2019). Large birth cohort studies seem to document a consistent positive connection between PM exposure and term-LBW(TLBW). However, some analyses were limited to pregnant women living near air monitoring stations (Liang et al. 2019; Lavigne et al. 2018; Araban et al. 2012; Wilhelm et al. 2012), which may limit the applicability of the study findings to broader populations. It is not determined whether the inclusion of macrosomia (defined as birth weight > 4000 g) and post-term birth (≥ 42 weeks gestation) attenuate the main association. In addition, the lack of standardized assessment methods may increase maternal exposure assessment errors and differences in health effect estimates. Traditional approaches to exposure measurement, such as fixed-site monitoring, the land use regression (LUR) model, the inverse distance weighting (IDW) spatial interpolation algorithm, the dispersion model, and the Bayesian model, fail to account for spatial heterogeneity and the individual difference of time-activity patterns, which may be a source of between-study heterogeneity. Furthermore, current systematic reviews and meta-analyses that have not extensively controlled for potential confounders, including maternal age, gestational age, infant sex, passive smoking, diabetes, and hypertension during pregnancy, did not provide us with risk estimates for the impact of PM exposure on TLBW.
Given these differences, determining the exact relationship between PM exposure and TLBW is urgently needed based on available epidemiological evidence. Previous systematic reviews have summed up the evidence for associations between PM exposure and childbirth outcomes (Li et al. 2017, 2020a, b). We update those reviews, with a focus on the connection between two sizes (PM2.5 and PM10) of particle exposure and TLBW. We specifically examined how different PM exposures (including interquartile range and 10 μg/m3 increments) affect the results. Additionally, we explored the influence of country status, continent, exposure assessment, risk of bias, and adjustment for maternal age, infant sex, and parity on our results.
Methods
This study was conducted in accordance with the preferred reporting items for systematic reviews and meta-analyses (PRISMA) and the Cochrane Handbook. The protocol was registered in INPLASY (number: https://doi.org/10.37766/inplasy2022.8.0064).
Data sources and search strategy
A comprehensive search of PubMed and Web of Science was conducted from the database inception until April 7, 2022. Both subject headings and free text terms were searched for two themes of “air pollution” and “LBW” separately (Supplementary Table S1) to increase sensitivity to potentially appropriate studies. Synonymous terms were first combined with the Boolean operator “OR.” These 2 themes were then combined with the Boolean operator “AND.” No restrictions were applied to PubMed. Filters were applied to exclude review articles, meetings, and non-English publications from the Web of Science. All cited references were also checked for potential sources.
Inclusion and exclusion criteria
The following criteria were used to determine inclusion: (a) study design: birth cohort studies; observational studies; (b) study population (pregnant women and their singleton live births); (c) prenatal PM exposure was assessed using ground-level monitoring stations or validated exposure models (μg/m3); (d) PM2.5 and PM10 were treated as linear or quartile terms; (e) pregnancy outcomes were defined as dichotomous variables: TLBW(≥ 37 weeks and < 2500 g) or LBW (2500 g); (f) risk estimates were presented as hazard ratios (HRs) or odds ratios (ORs) and 95% confidence intervals (CI) with each specific increment in the PM; (g) if multiple articles reported results drawn from the same source dataset or cohort, we only included the most comprehensive study. Exclusion criteria were: (a) irrelevant studies; (b) time-series study, ecological study, and trial; (c) non-English studies; (d) studies with no standard diagnostic criteria for LBW (not < 2500 g); (e) studies with a rate of LBW < 1%, because we postulated that these studies findings may not be representative or underestimating effects; (f) abstract, review, letter, guidelines, case report, and animal or in vitro studies.
Study selection
The search results were imported into the reference management software and deduplicated. Titles and abstracts were double screened by four independent authors (JL, YMC, DL, FY) with the observed agreement between reviewers being 97%. Two reviewers (JL, YMC) independently examined the full texts of identified articles against inclusion and exclusion criteria. Disagreements or uncertainty were reconciled by discussion or by a third reviewer (QZ).
Risk of bias within individual studies
We developed a tailored version of the risk of bias tool (modified-OHAT, Supplementary Table S3) according to the Office of Health Assessment and Translation (OHAT) risk-of-bias questions and the Agency for Healthcare Research checklist (Rooney et al. 2014; Viswanathan et al. 2012), focusing on the bias questions applicable to the environmental health study designs. Two independent reviewers (JL, YMC) applied the tool to perform the quality assessment, and a third reviewer (QZ) settled discrepancies. In particular, we concentrate on the following potential sources of bias: (1) the birth cohort and reproductive data for the study population selection were gathered from the national birth certificate or birth registration database. Extreme gestational age and birth weight data (e.g., < 24 weeks, > 44 weeks, or > 5000 g) were eliminated in order to minimize their effect on the results. (2) Exposure assessment: studies used the geocoded maternal pregnancy residential address instead of infant birth addresses to determine daily prenatal exposure to PM and accounted for residential mobility during pregnancy; no restrictions on residing within 5 or 10 km of a ground monitoring site. (3) Analyses were adjusted for several potential confounding variables (such as maternal age, infant sex, parity, maternal education, and gestational age); studies compared whether there was a difference in birth weight and other parameters between children included in the analysis and those excluded due to missing data. (4) Using a uniform calculation formula, PM exposure or meteorological data are assigned to the entire pregnancy or each trimester; questionnaires or medical records were utilized to collect information on demographics, smoking history, and other factors. (5) More detailed analyses and complete data are provided in the main text or appendix; outcome reporting is not selective. Each item is categorized as having a low, moderate, high, or unclear risk of bias. Overall, the bias of a study was rated high if three or more of the five criteria were satisfied, medium if two, and low if one or fewer were met. Assessments are reported in Supplementary Table S5.
Data extraction
We developed a structured and pretested standard form to extract the following information: reference (first author, publication year), study characteristics (country and city, duration, design, setting), participant characteristics (inclusion and exclusion criteria, total sample size and the number or rate of LBW or TLBW), exposure assessment (Supplementary Table S4a-c). We also extracted information on any adjustment for covariates (Supplementary Table S7, Fig. S1). We only extracted adjusted ORs or HRs with 95% CI from the single-pollutant model. Furthermore, the detailed description of the results in the original article was extracted (Supplementary Table S6a-c). Eligible articles were extracted independently (JL, YMC) in duplicate, and all were reconciled by QZ. Attempts were made to contact authors for information that was not reported in the study.
Data synthesis and analysis
To reduce clinical heterogeneity, we grouped outcomes into three categories based on the reference birth group: TLBW among full-term births (≥ 37 weeks’ gestational age), TLBW among all births (regardless of gestational age), and LBW among all births. “Adjusted” studies were those that accounted for all three of the most significant variables (age, infant sex, and parity).
Inverse variance-weighted random effect meta-analysis was used to pool estimates. We used the most adjusted reported odds ratio when more than one potential confounding was reported. The increments were not transformed and classified into two groups (per interquartile range and per 10 μg/m3). We analyzed PM exposure for the entire pregnancy, the first, second, and third trimesters. I2 statistic was used to quantify heterogeneity. Associations between PM and TLBW were quantified and summarized (Supplementary Fig. S2-S6).
We paid specific attention to critical gestational periods or windows when exposure to PM might have had the largest impacts. Stratified analyses by the economic status of the country (a developing or advanced country according to the International Monetary Fund (2022), region of study (Asia, Europe, South America, North America), exposure assessment (LUR model, monitoring stations, IDW, dispersion model, Bayesian model), risk of bias (low, moderate, or high), and adjustment (yes versus no) were conducted to further evaluate the effects of PM on TLBW among term births. Next, we performed sensitivity analyses to evaluate the robustness of our findings by removing individual research from the initial analysis and recalculating the pooled effect (Supplementary Fig. S9). We investigated publication bias visually using funnel plots and numerically with Egger’s regression test (Supplementary Fig. S7-S8). Stata version 17 (StataCorp) was used for all statistical analyses. All tests were two-tailed with a significance threshold of 0.05.
Results
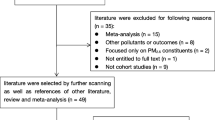
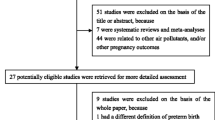
Fifteen thousand two hundred eighty-seven records were identified after removing duplicates from 18,263. Of these, 15,096 articles were excluded after the first screening based on abstracts or titles, leaving 191 articles for full-text review. Furthermore, 130 articles were excluded because of predetermined criteria. Eventually, 61 articles involving 34,506,975 singleton live births set in 15 countries were selected. Most studies covered the impacts of PM on TLBW among term birth (n = 47); six presented data on TLBW among all birth; and nine on TLBW among all birth. Figure 1 depicts the study’s flowchart.

PRISMA flow diagram
Characteristics of included studies
Nearly two-thirds (40 studies, 66.7%) of these studies occurred in advanced countries. Most studies were conducted in North America (31 studies, 50.8%, 26 from America) and Asia (17 studies, 27.9%, 10 from China), with only five studies in South America, four studies in Europe, two studies in Oceania, and one study in Africa. Thirty-five studies found a link between PM2.5 and TLBW in term births (n = 31) or all births (n = 4) and between PM10 and TLBW in term births (n = 25) or all births (n = 3). There are seven studies on the effects of PM2.5 on LBW, but only three on the effects of PM10 on LBW. Overall, 46 (75.4%) studies exhibited a low risk of bias, 11 (18%) a medium risk, and 4 (6.6%) a high risk, resulting in a low risk of bias among all included research. Table 1 summarizes the characteristics of the study population, including the number of TLBW or LBW, country status, continent, exposure assessment, risk of bias, and adjustment. Table 1 provides a summary of the study’s characteristics, including population size, nation status, continent, exposure assessment, risk of bias, and adjustment.
Relationships between prenatal PM exposure and pregnancy outcomes
TLBW among term births
Thirty-nine studies assessed the impact of PM on TLBW among term births, and the TLBW rate is 2.2% (515,719/23,311,021). There were 31 studies reporting PM2.5. TLBW was positively related to PM2.5 exposure. The pooled OR for PM2.5 exposure during pregnancy was 1.02 (1.01 to 1.03) per IQR and 1.06 (1.01 to 1.11) per 10 μg/m3 increase, respectively (Fig. 2) (Fig. S2-a, b). Additionally, we discovered that the probabilities of TLBW rose by 1.03 for each 1 μg/m3 increase in PM2.5 exposure (1.02 to 1.04; Fig. S2-d). However, no conclusions can be drawn about the specific critical window of PM2.5 exposure. Twelve studies provided PM2.5 exposure (per IQR increase) for each trimester. Nine studies reported null findings in the first and second trimesters, and only two out of twelve studies found a favorable connection in the third trimester. There was considerable heterogeneity in estimates of the odds of TLBW per IQR increase in PM2.5 exposure for each trimester (I2 > 50%).

Findings of meta-analysis of association between prenatal exposure to particulate matter and term low birth weight
There were twenty-five studies reporting PM10. TLBW was also positively related to an increased level of PM10. The pooled odds ratios of TLBW associated with an IQR change in PM10 exposure were 1.03 (1.01 to 1.05), and per 10 μg/m3 increase was also 1.03 (1.00 to 1.06) (Fig. 2) (Fig. S5-a, b). Only one study reported an increased TLBW risk of 1.07 (1.01 to 1.03) for a 1 μg/m3 increase in PM10 (Dibben and Clemens 2015). The second trimester was associated with relatively higher unfavorable correlations (1.03, 1.01 to 1.06, per IQR increase) than the other time periods. Only two of the six studies involving the first and second trimesters of PM10 exposure (per 10 µg/m3 increase) revealed a significant adverse effect.
TLBW among all births
Six studies reported the incidence of TLBW among all births (3.6%, 47,525/1303313). Four studies reported on the association between PM2.5 and TLBW during the entire pregnancy, with two studies noting a decrease in TLBW and 2 studies reporting an increase, and pooled analysis suggested no overall effect. Only one study reported that there was a statistically significant increase in risk during the first-trimester window. There were three studies reporting PM10. We found that no higher pooled risk of TLBW related to IQR increases in PM10 during the entirety of pregnancy or each trimester.
LBW
In 8 of 9 studies (one study did not specify the number of LBW), the LBW rate is 8.7% (81,393/939,598). Four out of seven studies found an association between PM2.5 exposure and LBW, with considerable statistical heterogeneity. We were unable to evaluate the effect of PM10 exposure on LBW owing to insufficient data reported in the studies. No significant variations in the risk of LBW between PM2.5 and PM10 were observed during the entire pregnancy.
Subgroup and sensitivity analyses
In TLBW subgroup analysis, the estimated effects of PM2.5 and PM10 were stronger for infants born in advanced countries, studies with low risk of bias, and those adjusted for maternal age, infant sex, and parity (Table 2 and 3). Stronger effects were present for PM2.5 exposure collected from the monitoring stations and PM10 exposure interpolated from the inverse distance weighting model. Region-subgroup analysis found substantial relationships between TLBW and PM2.5 in North America and Europe and PM10 in Asia. Subgroup analyses did not show significant heterogeneity for each trimester, except for the third trimester of the Bayesian PM2.5 assessment model. Country status, regions, monitoring station assessment, risk of bias, and adjustment all contributed significantly to the heterogeneity of the first and second trimesters of PM10.
Almost most primary studies didn’t significantly influence the pooled estimate when a study was removed, demonstrating that no single study had a major effect on the pooled estimate. However, the effects became meaningful for TLBW in the second trimester of PM10 (10 μg/m3 increase) when the study of Mueller et al. was deleted. The absence of nonsymmetry in funnel plots in the included studies indicated low reporting bias (Fig. S7). The Egger test results revealed no indication of a small study impact (P > 0.05, Fig. S8).
Discussion
Principal findings
This meta-analysis of 61 studies from 15 countries, including 34,506,975 singleton live births, confirms that there may be a correlation between prenatal exposure to PM2.5 and PM10 and the risk of TLBW in offspring. The correlation with TLBW among term births in some analyses shows this outcome rising by about 1.02-fold every IQR increase in PM2.5 and 1.03-fold in PM10. The probability of TLBW was not statistically significantly increased with exposure to PM2.5 and PM10 during the entire pregnancy when all births (including preterm and term births) were included in the pooled analysis. Associations of PM exposure with LBW appear to be weaker and less inconsistent than those with TLBW. Only 4 of 7 studies that assessed LBW and PM2.5 found an association. Three studies evaluating the association between LBW and PM10 have reported conflicting results.
Many studies have revealed relationships between different increments of PM and TLBW, such as IQR, 1 μg/m3, 5 μg/m3, 10 μg/m3, 25th percentile, and high (75th or 90th percentile) vs low exposure (25th or 10th percentile). This makes it difficult to pool the specific effects of single pollutants. However, in this study, we used two exposure indicators for PM exposure, the IQR and 10 μg/m3 increase. We discovered that both PM2.5 and PM10 exposure indicators were linked with TLBW risk.
We were unable to discern clear windows of vulnerability during pregnancy, except that PM10 exposure in the second trimester appears most important for TLBW among term births. In other studies, the associations of early pregnancy higher ambient particulate matter with smaller fetal growth parameters, such as the biparietal diameter of the abdominal circumference (AC) and birth weight, also appear robust (Aguilera et al. 2010; Hansen et al. 2008; Leung et al. 2022). While most studies suggest that ambient air pollution effects on birth weight seem to occur in the first and third trimesters (Dadvand et al. 2014; Lavigne et al. 2018; Smith et al. 2017; Wu et al. 2018), a few studies refer to the second and third trimesters (Ha et al. 2014, 2017). Particles may affect fetal development differently at various gestational phases. Mechanistic analyses will be required to explore these possibilities due to the results derived from observational studies.
Associations between PM2.5 and PM10 exposure and TLBW appear especially pronounced among infants born in advanced countries. Note, however, that most previous studies included in our analysis come from high-resource countries. 15 of the 17 studies reporting PM2.5 exposure and TLBW, as well as 8 of the 12 studies, were for developed countries. As a matter of fact, pregnant women in low and middle-income regions might be at particular risk from air pollution, including household air pollution and ambient air pollution (Cohen et al. 2017; Lee et al. 2020). Therefore, more studies on low- and middle-income settings would be welcome to generate robust worldwide estimates in the future.
We found a generally higher effect size of TLBW for PM2.5 in North America and Europe than in Asia and for PM10 in Asia than in Europe and North America. Variations in the types and origins of PM could have differential health impacts. Firstly, PM2.5 in some areas may be dominated by industrial emissions and fuel combustion whereas secondary PM derived from the precursors SO2, nitrogen, and ammonia (NH3), accounts for the bulk of PM2.5 mass (U.S. Environmental Protection Agency 2019). Studies have revealed a wide variety of birth weight-reducing effects among PM2.5 constituent chemicals. Vanadium, sulfur, sulfate, iron, elemental carbon, and titanium exposure were related to the greatest decreases in birth weight (Basu et al. 2014). Another point that should not be overlooked is that different targets for regional policies hint at different roles played by different regions in health risk reduction. Other factors, such as access to medical services, may exacerbate disparities in health between regions.
Effect estimates of PM2.5 and PM10 on TLBW varied according to the exposure model in our analysis. The results are more reliable for PM2.5 with monitoring station data and for PM10 interpolated from the inverse distance weighting model. Different exposure assessment methods, whether the fixed-site monitoring stations or the modeling approaches, such as spatial interpolation methods, LUR, and dispersion models, were used to assign ambient air pollution levels to large populations. However, these methods often fail to integrate important information into the individual activity patterns and consider ambient pollutant infiltration into the indoor environment. There may be less of a relationship between the estimated exposure and the health effect of interest if PM infiltrates a building’s envelope and alters the PM concentration’s temporal variability within (Ambade et al. 2021; Meng et al. 2007; Mohammed et al. 2016; U.S. Environmental Protection Agency 2019).
Strengths and limitations of the study
Our analysis had a larger sample size, a better subject grouping pattern, and used more rational exposure increment pooling methods than previous studies. Also, we assessed associations between PM exposure at individual time points during pregnancy and TLBW in order to identify windows of vulnerability. Notably, we considered a number of confounding factors adjusted for in the main adjusted models of each study and identified whether confounders were adjusted or not significantly affect the pooled effect size. Moreover, we developed a risk of bias tool capable of being applied to environmental health problems to enhance impartiality. For these reasons, the findings from the current pooled analysis are stouter than the conclusions regarding the impact of prenatal exposure to PM and TLBW in the previous meta-analyses.
It should be noted that our study had some limitations. We repeated the analysis using PM2.5 and PM10 data and stratified by exposure assessment. While each of the methods has attractive features, all have drawbacks. Additionally, we used single-pollutant models instead of two- or multiple-pollutant models. We also cannot exclude the possibility that other air pollutants confound the observed associations. Also, some maternal factors (e.g., education, body mass index before pregnancy, weight change during pregnancy, smoking status, prenatal care, marital status, alcohol use after conception, drug use, pregnancy complications, chronic disorders, mother with previous TLBW infant), neonatal factors (such as gestational age, ethnicity, year/season/quarter/month of birth, mode of delivery), social factors (socioeconomic status, household registration, insurance, for instance), and meteorological factors may confound the associations we observed. We were unable to control all of them in the models because some factors were not available.
Conclusion
We performed a meta-analysis of the association between prenatal exposure to particulate matter and term low birth weight in more than 30 million singleton live births. We demonstrated that, after adjusting for confounders, maternal exposure to PM during the entire pregnancy could increase the risk of TLBW among term births, although no critical windows were identified. Stronger associations were observed in studies conducted in advanced countries, studies with low bias, and studies that adjusted for maternal age, infant sex, and parity. These findings broaden our understanding of the detrimental impact of PM2.5 on birth weight, underscoring the need to identify interventions targeting PM-related conditions in pregnant women. Future original study designs need to consider the impact of different exposure assessment modalities and all possible confounding factors.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Abbreviations
- PM:
-
Particulate matter
- LBW:
-
Low birth weight
- TLBW:
-
Term low birth weight
- EPA:
-
Environmental Protection Agency
- LUR:
-
Land use regression
- IDW:
-
Inverse distance weighting
- PRISMA:
-
Preferred reporting items for systematic reviews and meta-analyses
- OHAT:
-
Office of Health Assessment and Translation
- CI:
-
Confidence interval
- HR:
-
Hazard ratios
- OR:
-
Odds ratios
- IQR:
-
Interquartile range
- EP:
-
Entire pregnancy
- 1st:
-
The first trimester
- 2nd:
-
The second trimester
- 3rd:
-
The third trimester
References
Aguilera I, Garcia-Esteban R, Iniguez C, Nieuwenhuijsen MJ, Rodriguez A, Paez M, Ballester F, Sunyer J (2010) Prenatal exposure to traffic-related air pollution and ultrasound measures of fetal growth in the INMA Sabadell cohort. Environ Health Perspect 118:705–711
Aguilera J, Han X, Cao S, Balmes J, Lurmann F, Tyner T, Lutzker L, Noth E, Hammond SK, Sampath V, Burt T, Utz PJ, Khatri P, Aghaeepour N, Maecker H, Prunicki M, Nadeau K (2022) Increases in ambient air pollutants during pregnancy are linked to increases in methylation of IL4, IL10, and IFNgamma. Clin Epigenetics 14:40
Ambade B, Kumar A, Sahu LK (2021) Characterization and health risk assessment of particulate bound polycyclic aromatic hydrocarbons (PAHs) in indoor and outdoor atmosphere of Central East India. Environ Sci Pollut Res Int 28:56269–56280
Araban M, Kariman N, Tavafian SS, Motesaddi S, Alavimajd H, Shokravi FA (2012) Air pollution and low birth weight: a historical cohort study from Tehran. East Mediterr Health J 18:556–560
Basu R, Harris M, Sie L, Malig B, Broadwin R, Green R (2014) Effects of fine particulate matter and its constituents on low birth weight among full-term infants in California. Environ Res 128:42–51
Blencowe H, Krasevec J, de Onis M, Black RE, An X, Stevens GA, Borghi E, Hayashi C, Estevez D, Cegolon L, Shiekh S, Ponce Hardy V, Lawn JE, Cousens S (2019) National, regional, and worldwide estimates of low birthweight in 2015, with trends from 2000: a systematic analysis. Lancet Glob Health 7:e849–e860
Bongaerts E, Lecante LL, Bové H, Roeffaers MBJ, Ameloot M, Fowler PA, Nawrot TS (2022) Maternal exposure to ambient black carbon particles and their presence in maternal and fetal circulation and organs: an analysis of two independent population-based observational studies. Lancet Planet Health 6:e804–e811
Brunst KJ, Sanchez-Guerra M, Chiu YM, Wilson A, Coull BA, Kloog I, Schwartz J, Brennan KJ, BosquetEnlow M, Wright RO, Baccarelli AA, Wright RJ (2018) Prenatal particulate matter exposure and mitochondrial dysfunction at the maternal-fetal interface: effect modification by maternal lifetime trauma and child sex. Environ Int 112:49–58
Cohen AJ et al (2017) Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: an analysis of data from the Global Burden of Diseases Study 2015. Lancet 389:1907–1918
Dadvand P, Ostro B, Figueras F, Foraster M, Basagana X, Valentin A, Martinez D, Beelen R, Cirach M, Hoek G, Jerrett M, Brunekreef B, Nieuwenhuijsen MJ (2014) Residential proximity to major roads and term low birth weight: the roles of air pollution, heat, noise, and road-adjacent trees. Epidemiology 25:518–525
Daellenbach KR et al (2020) Sources of particulate-matter air pollution and its oxidative potential in Europe. Nature 587:414–419
Dibben C, Clemens T (2015) Place of work and residential exposure to ambient air pollution and birth outcomes in Scotland, using geographically fine pollution climate mapping estimates. Environ Res 140:535–541
Franklin M, Zeka A, Schwartz J (2007) Association between PM2.5 and all-cause and specific-cause mortality in 27 US communities. J Expo Sci Environ Epidemiol 17:279–287
GBD 2019 Risk Factors Collaborators (2020) Global burden of 87 risk factors in 204 countries and territories, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet 396(10528):1223–1249. https://doi.org/10.1016/S0140-6736(20)30752-2
Grevendonk L, Janssen BG, Vanpoucke C, Lefebvre W, Hoxha M, Bollati V, Nawrot TS (2016) Mitochondrial oxidative DNA damage and exposure to particulate air pollution in mother-newborn pairs. Environ Health 15:10
Ha S, Hu H, Roussos-Ross D, Haidong K, Roth J, Xu X (2014) The effects of air pollution on adverse birth outcomes. Environ Res 134:198–204
Ha S, Zhu Y, Liu D, Sherman S, Mendola P (2017) Ambient temperature and air quality in relation to small for gestational age and term low birthweight. Environ Res 155:394–400
Hansen CA, Barnett AG, Pritchard G (2008) The effect of ambient air pollution during early pregnancy on fetal ultrasonic measurements during mid-pregnancy. Environ Health Perspect 116:362–369
Hung TH, Chen PH, Tung TH, Hsu J, Hsu TY, Wan GH (2023) Risks of preterm birth and low birth weight and maternal exposure to NO(2)/PM(2.5) acquired by dichotomous evaluation: a systematic review and meta-analysis. Environ Sci Pollut Res Int 30:9331–9349
Kannan S, Misra DP, Dvonch JT, Krishnakumar A (2006) Exposures to airborne particulate matter and adverse perinatal outcomes: a biologically plausible mechanistic framework for exploring potential effect modification by nutrition. Environ Health Perspect 114:1636–1642
Kramer MS (1987) Determinants of low birth weight: methodological assessment and meta-analysis. Bull World Health Organ 65:663–737
Lavigne E, Burnett RT, Stieb DM, Evans GJ, Godri Pollitt KJ, Chen H, van Rijswijk D, Weichenthal S (2018) Fine particulate air pollution and adverse birth outcomes: effect modification by regional nonvolatile oxidative potential. Environ Health Perspect 126:077012
Lee KK et al (2020) Adverse health effects associated with household air pollution: a systematic review, meta-analysis, and burden estimation study. Lancet Glob Health 8:e1427–e1434
Leung M, Weisskopf MG, Laden F, Coull BA, Modest AM, Hacker MR, Wylie BJ, Wei Y, Schwartz J, Papatheodorou S (2022) Exposure PM2.5 to during pregnancy and fetal growth in eastern Massachusetts, USA. Environ Health Perspect 130:17004
Li X, Huang S, Jiao A, Yang X, Yun J, Wang Y, Xue X, Chu Y, Liu F, Liu Y, Ren M, Chen X, Li N, Lu Y, Mao Z, Tian L, Xiang H (2017) Association between ambient fine particulate matter and preterm birth or term low birth weight: an updated systematic review and meta-analysis. Environ Pollut 227:596–605
Li C, Yang M, Zhu Z, Sun S, Zhang Q, Cao J, Ding R (2020a) Maternal exposure to air pollution and the risk of low birth weight: a meta-analysis of cohort studies. Environ Res 190:109970
Li X, Cao X, Guo M, Xie M, Liu X (2020b) Trends and risk factors of mortality and disability adjusted life years for chronic respiratory diseases from 1990 to 2017: systematic analysis for the Global Burden of Disease Study 2017. BMJ 370:m3150
Liang Z, Yang Y, Qian Z, Ruan Z, Chang J, Vaughn MG, Zhao Q, Lin H (2019) Ambient PM(2.5) and birth outcomes: estimating the association and attributable risk using a birth cohort study in nine Chinese cities. Environ Int 126:329–335
Lim SS et al (2012) A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 380:2224–2260
Martens DS, Cox B, Janssen BG, Clemente DBP, Gasparrini A, Vanpoucke C, Lefebvre W, Roels HA, Plusquin M, Nawrot TS (2017) Prenatal air pollution and newborns’ predisposition to accelerated biological aging. JAMA Pediatr 171:1160–1167
Meng QY, Turpin BJ, Lee JH, Polidori A, Weisel CP, Morandi M, Colome S, Zhang J, Stock T, Winer A (2007) How does infiltration behavior modify the composition of ambient PM2.5 in indoor spaces? An analysis of RIOPA data. Environ Sci Technol 41:7315–7321
Mohammed MOA, Song WW, Ma YL, Liu LY, Ma WL, Li WL, Li YF, Wang FY, Qi MY, Lv N, Wang DZ, Khan AU (2016) Distribution patterns, infiltration and health risk assessment of PM2.5-bound PAHs in indoor and outdoor air in cold zone. Chemosphere 155:70–85
Rooney AA, Boyles AL, Wolfe MS, Bucher JR, Thayer KA (2014) Systematic review and evidence integration for literature-based environmental health science assessments. Environ Health Perspect 122:711–718
Rosa MJ, Pajak A, Just AC, Sheffield PE, Kloog I, Schwartz J, Coull B, Enlow MB, Baccarelli AA, Huddleston K, Niederhuber JE, Rojo MMT, Wright RO, Gennings C, Wright RJ (2017a) Prenatal exposure to PM(2.5) and birth weight: a pooled analysis from three North American longitudinal pregnancy cohort studies. Environ Int 107:173–180
Rosa MJ, Just AC, Guerra MS, Kloog I, Hsu HL, Brennan KJ, Garcia AM, Coull B, Wright RJ, Tellez Rojo MM, Baccarelli AA, Wright RO (2017) Identifying sensitive windows for prenatal particulate air pollution exposure and mitochondrial DNA content in cord blood. Environ Int 98:198–203
Smith RB, Fecht D, Gulliver J, Beevers SD, Dajnak D, Blangiardo M, Ghosh RE, Hansell AL, Kelly FJ, Anderson HR, Toledano MB (2017) Impact of London’s road traffic air and noise pollution on birth weight: retrospective population based cohort study. BMJ 359:j5299
Thurston GD, Ahn J, Cromar KR, Shao Y, Reynolds HR, Jerrett M, Lim CC, Shanley R, Park Y, Hayes RB (2016) Ambient particulate matter air pollution exposure and mortality in the NIH-AARP diet and health cohort. Environ Health Perspect 124:484–490
Tian Y, Liu H, Wu Y, Si Y, Song J, Cao Y, Li M, Wu Y, Wang X, Chen L, Wei C, Gao P, Hu Y (2019) Association between ambient fine particulate pollution and hospital admissions for cause specific cardiovascular disease: time series study in 184 major Chinese cities. BMJ 367:l6572
U.S. Environmental Protection Agency (2019) Integrated science assessment (ISA) for particulate matter (final report, Dec 2019). Washington, DC. https://cfpub.epa.gov/ncea/isa/recordisplay.cfm?deid=347534#tab-3
Viswanathan M, Ansari MT, Berkman ND, Chang S, Hartling L, McPheeters M, Santaguida PL, Shamliyan T, Singh K, Tsertsvadze A, Treadwell JR (2012) Assessing the risk of bias of individual studies in systematic reviews of health care interventions. Rockville (MD) https://www.effectivehealthcare.ahrq.gov/. PMID: 22479713. Accessed 8 Mar 2012
WHO(2014) Comprehensive implementation plan on maternal infant and young child nutrition. Geneva https://www.who.int/publications/i/item/WHO-NMH-NHD-14.1 . Accessed 19 May 2014
Wilhelm M, Ghosh JK, Su J, Cockburn M, Jerrett M, Ritz B (2012) Traffic-related air toxics and term low birth weight in Los Angeles County, California. Environ Health Perspect 120:132–138
Wu H, Jiang B, Geng X, Zhu P, Liu Z, Cui L, Yang L (2018) Exposure to fine particulate matter during pregnancy and risk of term low birth weight in Jinan, China, 2014–2016. Int J Hyg Environ Health 221:183–190
Yuan L, Zhang Y, Gao Y, Tian Y (2019) Maternal fine particulate matter (PM(2.5)) exposure and adverse birth outcomes: an updated systematic review based on cohort studies. Environ Sci Pollut Res Int 26:13963–13983
Zhao Y, Wang P, Zhou Y, Xia B, Zhu Q, Ge W, Li J, Shi H, Xiao X, Zhang Y (2021) Prenatal fine particulate matter exposure, placental DNA methylation changes, and fetal growth. Environ Int 147:106313
Zheng Y et al (2017) Traffic-derived particulate matter exposure and histone H3 modification: a repeated measures study. Environ Res 153:112–119
Funding
This work was funded by the National High Level Hospital Clinical Research Funding (2022-NHLHCRF-LX-01–0301), the Clinical Research Fund of Chinese Academy of Medical Sciences (2021-I2M-C&T-B-089), and the Chinese Academy of Medical Sciences Innovation Fund for Medical Sciences (2021-I2M-049).
Author information
Authors and Affiliations
Contributions
Jing Liu: conceptualization, methodology, software, and writing—original draft preparation. Yuanmei Chen: investigation and data curation. Die Liu: data curation. Fang Ye: data curation. Qi Sun: formal analysis. Qiang Huang: formal analysis. Jing Dong: software. Tao Pei: supervision. Yuan He: methodology and validation. Qi Zhang: writing—reviewing and editing.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
All authors consent to the publication of this study.
Competing interests
The authors declare no competing interests.
Additional information
Responsible Editor: Lotfi Aleya
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Liu, J., Chen, Y., Liu, D. et al. Prenatal exposure to particulate matter and term low birth weight: systematic review and meta-analysis. Environ Sci Pollut Res 30, 63335–63346 (2023). https://doi.org/10.1007/s11356-023-26831-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-023-26831-7