
Abstract
Particulate matter emitted during autopsies can serve as a vector for numerous viruses or bacteria and can lead to infections. Reducing the exposure of those particles in indoor working environments is, therefore, an important issue. To assess the health risk for employees in forensic medicine, we measure particulate matter in the ambient air during autopsies by using an aerosol spectrometer. The autopsies were performed with either an ordinary oscillating saw or an adapted saw with a suction unit. The particle emissions from both saws were compared to each other in order to evaluate whether a technical adaption leads to a particle reduction. Furthermore, the particle exposure reduction by wearing a face mask and variations in the background concentration in the room were analyzed. High particle concentrations were measured while using the ordinary saw. By using the adapted saw or wearing a face mask, the particle exposure could mostly be avoided. On the majority of the working days, an increase in the background concentration could be observed. Based on this knowledge, the use of a proper suction unit and wearing a face mask during autopsies is necessary. Besides, it is important to have sufficient ventilation in the room so that long-lasting high background concentrations can be prevented.
Graphical abstract

Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Particulate matter (PM) consists of a complex mixture of solid and liquid particles in the air. These particles are emitted, for example, during combustion or abrasion processes. Particle formation, which takes place through chemical reactions of emitted precursor substances, also contributes to the total concentration (EPA 2020). PM consists of particles with a wide range of aerodynamic diameters. In monitoring air quality, mostly the categories PM10 (particulate matter with an aerodynamic diameter less than 10 µm), PM2.5 (particulate matter with an aerodynamic diameter less than 2.5 µm), PM1 (particulate matter with an aerodynamic diameter less than 1 µm), and PMcoarse (particles with diameters between 2.5 and 10 µm) are used (Air Quality Expert Group 2005).
High exposure to PM has numerous negative influences on human health and is therefore a major and current research field in medicine and environmental sciences. Even short-term exposures with high concentrations have a harmful potential and can lead to an increase in cardiovascular and respiratory mortality (Katsouyanni et al. 1997; Delfino et al. 1998; Orellano et al. 2020). Likewise, disorders in blood coagulation and an increase in the incidence of strokes can result from short-term exposure to high concentrations of PM (Wei et al. 2019; Matsuo et al. 2016). Under long-term exposure, the consequences can be even worse. Especially chronic respiratory diseases like chronic obstructive pulmonary disease (COPD), asthma, or cancer can be linked to chronic exposure to high concentrations of PM (Han et al. 2020; Yorifuji and Kashima 2019). Depending on their size, there are major differences in where they deposit in the respiratory tract. Whereas coarse particles tend to deposit in the upper airways, small particles can reach the area of the gas exchange and have the potential to act systemically (Brown et al. 2013; Darquenne 2012). According to an EU guideline, there is a limit value for the daily mean PM10 concentration of 50 µg/m3, which must not be exceeded on more than 35 days per year (Directive 2008/50/EC 2008).
Because people in Central Europe spend 80–90% of the day indoors (Federal Ministry for Environment, Nature Conservation and Nuclear Safety 2020), the composition of the ambient air in the rooms is a crucial factor for the total daily PM uptake. High concentrations of PM can last for hours due to the limited volume and the reduced ventilation. The indoor PM concentration is strongly affected by indoor sources (Meier et al. 2015). Depending on the occupation and the working environment, the PM uptake differs significantly. Employees in forensic medicine are one of these occupational groups with a notable risk of being exposed to a high amount of PM (Kernbach-Wighton et al. 1996, 1998; Pluim et al. 2018).
Autopsies are required, for example, when there is evidence of a nonnatural cause of death. For proper execution of the autopsy, the opening of the cranium is indispensable (Federal Office of Justice 2021). Therefore, commonly oscillating saws are used. The usage of these saws leads to high emission of potentially respirable material during the sawing process, which is scattered over several meters (Kernbach-Wighton et al. 1996; Wenner et al. 2017; Jones and Brosseau 2015; Noble et al. 1963). This material consists of bone dust, liquid aerosol, large droplets of blood, and cerebrospinal fluid with a high percentage of PM in its particle size distribution (Green and Yoshida 1990). In contrast to PM from natural sources or from burning fossil fuels, PM emitted during autopsies has further negative effects on human health. For instance, this kind of material can serve as a vector for numerous different biological hazards, like bacteria or viruses and other microbes. The morphology of these particles is very variable. Especially serrated particles have a high ability to adhere to mucous membranes and favor infections (Kernbach-Wighton et al. 1996). It has already been proven that there occurs an entry of tubercle bacteria into the ambient air during autopsies (Templeton et al. 1995). First studies also indicate that corpses of deceased COVID-19 patients have to be considered potentially infective during autopsies (Plenzig et al. 2021). Likewise, the human papillomavirus has been transferred, while material was scattered during surgery (Barrett and Garber 2003). Besides infection, intoxications can also occur. For example, cyanide poisoning occurred while a deceased person with cyanide poisoning was opened for a forensic autopsy (Seyit et al. 2020).
The purpose of this study is to evaluate the health risk for employees in forensic medicine by monitoring PM emissions during forensic autopsies. It was analyzed whether reduction of PM emission could be achieved by a technical adaption of the oscillating saw. Furthermore, the influence of wearing a particle filtering face mask while using the saw was analyzed.
Materials and methods
Oscillating autopsy saws
In this study, two different types of oscillating autopsy saws were used and compared. The autopsy saw from Bühler Instrumente (article number 30.219.20) is an ordinary oscillating saw (OS) with a maximum of 24,000 oscillations per minute (Fig. 1a). The saw has no further equipment. The other autopsy saw used during the autopsies is from Kugel Medical (type SF-4000) with a maximum of 12,000 oscillations per minute (Fig. 1b). This saw is an adapted oscillating saw (AS) equipped with a suction unit to reduce the amount of material that is scattered in the surrounding area.

Oscillating saws used during the autopsies from a Bühler Instrumente (OS) and b Kugel Medical (AS)
Measurement of particulate matter
In this study, the PM concentration during autopsies was measured by an aerosol spectrometer of type GRIMM 11-R, which was connected to a laptop of the type Fujitsu Lifebook. Every 6 s, a value was generated for the PM fractions PM10, PM2.5, and PM1. The PMcoarse values are equal to the difference between PM10 and PM2.5. Besides a constant measurement of PM, temperature and humidity were monitored.
Measurement protocol
The measuring interval was limited to the time interval around the opening of the cranium because of high variations in the duration of the autopsies. Measurement started 5 min before the saw was used to generate a proper value for the mean background concentration. The measurement continued for the whole time of using the saw and lasted for a further 5 min to maximize the amount of particles that moved in the direction of the spectrometer and finally gets analyzed.
The aerosol spectrometer was located 1.5 m away from the body in direction of the feet so that a realistic scenario for the exposure to the employees could be ensured.
Measurements took place at the Institute of Legal Medicine Frankfurt am Main in the period between May 31, 2016, and June 28, 2016. The measurements were carried out during normal autopsy time (9:00–16:30). The exact point of time when the autopsies took place was based on the circumstances of death and personnel availability. In total, 16 measurements were carried out and analyzed while the OS without the suction unit was used (OS 1–OS 16). Another 16 measurements were carried out and analyzed while the AS equipped with the suction unit was used (AS 1–AS 16). The dates and the point of time of the single measurements are given in Table 1.
The average sawing time when using the OS was 69 s. Due to the higher weight and a slightly restricted view during sawing, the sawing time is longer when using the AS. Here, an average working time of 141 s was necessary to completely open the cranium. The quality of the work is not affected by the suction unit.
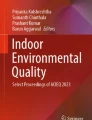
In order to quantify the influence of particle filtering masks on particle exposure, another 5 measurements with the same protocol were carried out while the OS was in use. Here, measurements were performed simultaneously with two aerosol spectrometers of type GRIMM 11-R. The sample inlets were integrated into two dummy heads. One head was equipped with a face mask (FFP2 CE norm 2834) (Fig. 2).

Dummy heads with face mask (1) and without face mask (2) with sample inlets (3) connected to the aerosol spectrometers (4)
Statistics
The concentration of PM was measured separately for each autopsy. The background value (PMbkgd) was generated out of the mean concentration measured in a 5-min time interval before the saw was used. The PM value assigned to the sawing process (PMsaw) was the mean PM concentrations measured during the sawing time itself and for another 5 min afterward. PMbkgd and PMsaw were compared with a Wilcoxon signed-rank test. The measurements with the different saws are analyzed separately from each other.
For the comparison of the particle size distribution between PMbkgd and PMsaw, the particles were grouped in the size categories of 2.5–10 µm, 1–2.5 µm, and < 1 µm. For the calculation of the range of particles with diameters between 2.5 and 10 µm, the concentration of PM2.5 was subtracted from the concentration of PM10. For the range of particles with a diameter between 1 and 2.5 µm, the concentration of PM1 was subtracted from the concentration of PM2.5.
The absolute concentration differences (PM∆) measured after the use of the saw were calculated by subtracting the value for PMbkgd from that of PMsaw. The concentration differences measured during the autopsies performed with the OS and those measured during the autopsies performed with the AS were compared to each other with a Mann–Whitney U-test. Particles of the fractions PMcoarse, PM10, PM2.5, and PM1 were analyzed separately.
To determine the exposure reduction that can be achieved by wearing a face mask, the simultaneously measured values were compared with each other. In previous simultaneous test measurements without the use of a mask in the autopsy room during normal operation, an average deviation of 1.5% was found between the two aerosol spectrometers in the determination of the total particle mass. Due to this very small value, the deviation can be neglected when interpreting the values in the following measurements.
The single background concentrations, measured before each autopsy within one working day, were compared to each other in order to characterize shifts in the PM background level.
The statistical analyzes were performed using Graphpad Prism 9.
Results
Autopsies performed with the OS
The values for the PM background concentrations and the PM concentration while using the OS are given in Table 2.
Throughout the entire measurement period, maximum short-term concentrations (6-s values) of 11,735.4 µg/m3 for the PMcoarse fraction, 12,580.7 µg/m3 for the PM10 fraction, 845.3 µg/m3 for the PM2.5 fraction and 244.9 µg/m3 for the PM1 fraction were measured while using the OS.
The concentration differences (PMΔ) between PMbkgd and PMsaw for every single autopsy carried out with the OS are given in Table 3. Figure 3 shows the PMbkgd values and the corresponding values for PMsaw for the PM10 fraction for all 16 measurements.

Comparison of the PMbkgd values for the PM10 fraction and the corresponding values for PMsaw for all 16 autopsies performed (different symbol for each autopsy) with the OS (OS 1–16)
A comparison of the concentrations for PMbkgd and PMsaw shows that sawing with the OS leads to PM concentration increases for the fractions PMcoarse, PM10, and PM2.5. Also, for the PM1 fraction, increases were measured for most autopsies. However, there was a slight decrease in the measured values during three autopsies.
The Wilcoxon signed-rank test shows for all fractions significant differences between PMbkgd and PMsaw (Table 4).
There were significant differences in the increase in particle concentration and particle size distribution between the single autopsies measured (Fig. 4).

Examples of the particle concentrations and particle size distributions (background and sawing) measured during different autopsies performed with the OS for a OS 3, b OS 5, c OS 13, and d OS 15
The coarse particles always show the highest concentration increases. For that reason, there is a shift of the particle size distribution in favor of the coarse particles in all measurements.
Autopsies performed with the AS
The values for the PM background concentrations and the PM concentration while using the AS are given in Table 5.
Throughout the entire measurement period, maximum short-term concentrations (6-s values) of 61.2 µg/m3 for the PMcoarse fraction, 85.2 µg/m3 for the PM10 fraction, 59.9 µg/m3 for the PM2.5 fraction, and 55.3 µg/m3 for the PM1 fraction were measured while using the AS.
The concentration differences (PMΔ) between PMbkgd and PMsaw for every single autopsy carried out with the AS are given in Table 6. Figure 5 shows the PMbkgd values for the PM10 fraction and the corresponding values for PMsaw for all 16 measurements.

Comparison of the PMbkgd values for the PM10 fraction and the corresponding values for PMsaw for all 16 autopsies (different symbol for each autopsy) performed with the AS (AS 1–16)
No trend can be observed when using the AS. From the time sawing begins, there are both concentration increases and decreases. The Wilcoxon signed-rank test shows no significant differences for all fractions between the background values and the corresponding values measured while the saw is used (Table 7).
The particle size-specific analysis also does not show a consistent pattern (Fig. 6).

Examples of the particle concentrations and particle size distributions (background and sawing) measured during different autopsies performed with the AS for a AS 6, b AS 7, c AS 13, and d AS 14
Overall, the changes in the particle size spectrum are only marginal. There are slight shifts in favor of the finer particles as well as slight shifts in favor of the coarse particles.
Comparison between the OS and the AS
When comparing the PMΔ values measured when working with the OS with those measured when working with the AS, significant differences can be observed (Fig. 7).

Comparison between the PMΔ values from the autopsies performed with the OS and those performed with the AS
The Mann–Whitney U-test shows a significant difference for all particle size fractions (Table 8).
Influence of a face mask on the PM exposure
A comparison of PM concentration measured with and without a face mask in front of the sample inlet of an aerosol spectrometer shows significant differences (Fig. 8).

PM Concentration profile during an autopsy measured with and without a face mask in front of the sample inlet of an aerosol spectrometer
Before sawing begins, it is already apparent that a reduction in PM exposure can be achieved through the use of a mask. However, it is only after the saw has been used that the full potential of the protective effect becomes apparent. If a very high exposure occurs without the mask, the exposure level remains approximately constant at a low level when the mask is used. Table 9 shows the reduction of PMsaw by measuring behind a face mask.
For all particle fractions, a significant reduction in particle concentration can be achieved if measurements were performed behind a face mask for each individual autopsy.
Shifts in the background concentration during the working days
Both increases and decreases can be observed when analyzing the shifts in the background concentration. Figure 9 shows background concentration profiles for four different working days with their characteristic shifts.

Examples for changes in the background concentrations for PM10 during a working day measured on a June 2, 2016, b June 3, 2016, c June 7, 2016, and d June 15, 2016. Red arrows: concentration increases, green arrows: concentration decreases
The PMbkgd trends for June 2, 2016, and June 3, 2016 show increases in the background concentration within the working days. On both days, solitary the OS was used.
On June 7, 2016, despite high emissions during the sawing processes (1st and 2nd autopsy), there was a drop in the background concentration later in the day.
Although no increase in concentration was measured during sawing with the AS on June 15, 2016 (1st and 2nd autopsy), a slight increase in the background concentration could be observed.
Overall, over the entire measurement period, rather increases in the background concentration during the working days could be observed.
Temperature and relative humidity
The measured values for temperature and relative humidity during the autopsies on single working days are given in Table 10.
There were minor fluctuations in temperature and relative humidity within the different working days.
Discussion
PM concentrations measured during the autopsies
Oscillating autopsy saws lead to high emission of potentially respirable material during the sawing process (Kernbach-Wighton et al. 1996). Because this material can serve as a vector for many different biological hazards or toxic substances, it can cause infection or poisoning when inhaled. Within the framework of the study conducted, these emissions were characterized.
It could be observed that the particle concentration increased significantly during an autopsy when sawing with the OS. The increase in the whole particle concentration is mainly due to an increase in the concentration of the coarse particles. The particle concentration of the medium and finer fraction increased only slightly. In some exceptional cases, there was even a slight decrease in the finest particle fraction. This can be explained by an increase in collision processes between fine and coarse particles at a higher number of coarse particles in total. These collisions result in further growth of the coarse particles (Zarzycki et al. 2020).
In terms of absolute particle concentration after sawing, large differences could be observed.
The measurements were carried out under real conditions so that different sawing times and cutting patterns were necessary depending on the condition of the human body. The bodies can also show differences in the degree of moisture. This can have an overall effect on the amount of material that is emitted into the ambient air during the sawing process (Pluim et al. 2018). Furthermore, under real working conditions, it cannot be ruled out that the air circulation in the autopsy room changes. Rapid movements of the employees or a slight air draft can already cause the emitted particles to spread to the opposite side of the spectrometer.
Generally, no significant increase in the particle concentration could be observed for any fraction when the AS with the suction unit was used. In the direct comparison of both saws, the very high emission of coarse particles, in particular, did not occur while using the AS. The suction unit is therefore suitable for preventing an increase in the total particle load in the ambient air, especially for the coarse particles, while working with an oscillating saw. Since the AS was normally operated at a lower oscillation frequency than the OS, it can be assumed that an additional particle reduction was thus achieved (Pluim et al. 2018).
Concentration increases in isolated autopsies are probably due to the inability of the suction device to sufficiently eliminate particles at certain cutting angles or cutting speeds.
The measurements with the particle filtering mask show that face masks can lead to a significant reduction in PM exposure.
Background concentration
When observing the changes in the background concentration in the autopsy room during one day, no clear trend could be identified. Despite very high emissions during the autopsies, in many cases, the background value increased only slightly during the day. For example, when on June 3, 2016, the first autopsy was performed with the OS, an enormous increase of 928.1 µg/m3 was detected for the fraction PM10 after the saw was used. Two hours later, only a value of 36.7 µg/m3 was measured as background before the following autopsy began. This is only a concentration increase of 12.5 µg/m3 compared to the background level earlier that day. On other working days, there was even a slight drop in background concentration despite high emissions during the sawing process.
Occasionally, increasing background values could be observed despite the lack of emissions during autopsies with the suction unit. Different reasons might be crucial factors to influence variations in the background concentration during a day. For example, changes in relative humidity may affect particle concentration. An increase in the relative humidity in indoor air leads to a significant elimination of the particles. On the other side, decreases in the relative humidity can lead to a high burden of PM in the ambient air (Kraus and Šenitková 2017). During one working day, both increases and decreases in relative humidity occurred. The influence of the temperature on the PM indoor concentration is rather low (Kraus and Šenitková 2017). In addition, coarse particles normally are deposited from the ambient air within hours by sedimentation processes (Qian et al. 2008). In the present study, in particular, these kinds of particles were emitted during sawing. Fine particles can also be eliminated from the ambient air through collision processes (Zarzycki et al. 2020). Changes in the ventilation of the room can also influence the particle distribution and thus the concentration at the autopsy table throughout the day (Fromme et al. 2007).
Overall, the background concentration seems to depend on a complex interaction of particle input in the ambient air as well as sedimentation, variations in humidity, and air circulation in the autopsy room. Considering all working days studied, increases rather than decreases in concentration could be observed. In addition to particle reduction during sawing itself, regular ventilation of the autopsy room is necessary to reduce the accumulation processes.
Medical risk assessment
During the sawing process, mainly particles were generated, which can be assigned to the coarse fraction. However, finer particles were also emitted into the ambient air. In medical risk assessment, the initial focus is on the finer particle fraction. These particles have such a small aerodynamic diameter that they can reach the alveoli region and act systemically. The coarse particles that are mainly formed during the sawing process do not have the ability to reach the alveoli region. They usually deposit in the upper respiratory tract and can be eliminated by the mucociliary system (Brown et al. 2013; Darquenne 2012). In principle, their systemically harmful potential is significantly lower than that of the finer particles.
In the case of an autopsy, it must be considered that the particles emitted have the potential to promote infections and intoxications if they come into contact with the mucous membranes (Kernbach-Wighton et al. 1996).
There are no definitive indoor limit values for PM. However, a guideline of the World Health Organization (WHO) assumes that there are no differences in the harmful potential between PM from indoor sources and PM from outdoor sources, so the limit values can be adopted (WHO Regional Office for Europe 2010).
Of the 16 PMsaw values measured during the autopsies performed with the OS, 12 exceeded the limit value of 50 µg/m3. From the autopsies with the AS, only 2 values exceeded the limit value. Even if values in this magnitude decrease relatively quickly, it must be assumed that on very busy days with low air exchange, exceedances of the limit values can also occur as a daily average. The highest PM value measured during an autopsy was 12,581 µg/m3. Although these high PM concentrations only last for a short period of time, they can have a significant impact on human health (Katsouyanni et al. 1997; Delfino et al. 1998).
Overall, it can be assumed that employees in forensic medicine are exposed to a high particle concentration when using an OS. The use of a suitable suction unit can significantly reduce this risk.
In former studies within a controlled environment, it has already been proven that a lower sawing frequency and a higher contact load lead to lower particle concentrations (Pluim et al. 2018). The use of manual saws or an oscillating saw with an integrated spray tube that runs on water can also reduce the emission of PM (Kernbach-Wighton et al. 1996; Wenner et al. 2017). Furthermore, a particle reduction can be achieved by using a table with a built-in ventilation system (Orellano et al. 2020; Pluim et al. 2018). For an adapted saw with a suction unit, a significant reduction in particle number concentration was observed for particles < 5 µm (Kernbach-Wighton et al. 1998). Numerous methods are therefore available to significantly reduce the particle concentration at the autopsy table. If the use of an oscillating saw without a suction unit or other additional protective mechanisms is unavoidable, it is advisable to wear medical protective equipment consisting of a particle filtering mask and safety goggles. In particular, the effectiveness of a face mask was demonstrated in this study. In addition to adjusting the saw itself or wearing protective equipment, attention should be paid to adequate ventilation of the autopsy room.
Conclusion
In this study, it could be demonstrated under real conditions that ordinary oscillating saws used in forensic autopsies have the potential to cause high emissions of PM. Short-term values for the PM10 fraction of 12,581 µg/m3 were measured. The average PM values during the sawing process reached values up to 952.3 µg/m3 for the PM10 fraction. PM concentrations of this magnitude have a high potential to harm human health. The emitted particles mainly belonged to the coarse fraction. Although these coarse particles emitted during autopsies cannot reach the deeper respiratory tract and are largely eliminated by the mucociliary system, they can still lead to infections or intoxications.
While working with the AS, it could be observed that the suction unit reliably prevented the increase in particle concentration. However, careful handling is a prerequisite for this. Even if the work with the AS is associated with a slightly increased expenditure of time, this should not be dispensed with. Wearing particle filtering masks is another effective measure that can significantly reduce PM exposure.
It was shown that there were increases in the background concentration during the majority of the working days. Thus, in addition to the use of a suction unit, sufficient ventilation of the room is necessary.
If a technical adaptation of the saw, for example, with a suction unit, is not available, it is even more important to pay attention to sufficient protective equipment.
Data availability
All data generated or analyzed during this study are included in the supplementary material of this article.
References
Air Quality Expert Group (2005) Particulate matter in the United Kingdom. Defra, London, UK
Barrett WL, Garber SM (2003) Surgical smoke: a review of the literature. Is this just a lot of hot air? In Surgical endoscopy 17(6):979–987. https://doi.org/10.1007/s00464-002-8584-5
Brown JS, Gordon T, Price O, Asgharian B (2013) Thoracic and respirable particle definitions for human health risk assessment. In Particle and Fibre Toxicology 10:12. https://doi.org/10.1186/1743-8977-10-12
Darquenne C (2012) Aerosol deposition in health and disease. In Journal of Aerosol Medicine and Pulmonary Drug Delivery 25(3):140–147. https://doi.org/10.1089/jamp.2011.0916
Delfino RJ, Zeiger RS, Seltzer JM, Street DH (1998) Symptoms in pediatric asthmatics and air pollution: differences in effects by symptom severity, anti-inflammatory medication use and particulate averaging time. In Environmental Health Perspectives 106(11):751–761. https://doi.org/10.1289/ehp.98106751
Directive 2008/50/EC (2008): Directive 2008/50/EC of the European Parliament and of the Council of 21 May 2008 on ambient air quality and cleaner air for Europe. Available online at http://news.cleartheair.org.hk/wp-content/uploads/2013/02/lexuriserv.pdf. Accessed 14 July 2021
EPA (2020): National ambient air quality standards (NAAQS) for PM | US EPA. Available online at https://www.epa.gov/pm-pollution/national-ambient-air-quality-standards-naaqs-pm. updated on 6/10/2021. Accessed 3 Feb 2022
Federal Ministry for Environment, Nature Conservation and Nuclear Safety (2020): Innenraumluft - was ist das problem? Available online at https://www.bmu.de/themen/gesundheit-chemikalien/gesundheit-und-umwelt/innenraumluft/innenraumluft-was-ist-das-problem/. Accessed 24 Nov 2021
Federal Office of Justice (2021): Strafprozessordnung. Source: §89 Umfang der Leichenöffnung
Fromme H, Twardella D, Dietrich S, Heitmann D, Schierl R, Liebl B, Rüden H (2007) Particulate matter in the indoor air of classrooms—exploratory results from Munich and surrounding area. In Atmospheric Environment 41(4):854–866. https://doi.org/10.1016/j.atmosenv.2006.08.053
Green FHY, Yoshida K (1990) Characteristics of aerosols generated during autopsy procedures and their potential role as carriers of infectious agents. In Applied Occupational and Environmental Hygiene 5(12):853–858. https://doi.org/10.1080/1047322X.1990.10387806
Han C, Oh J, Lim Y, Kim S, Hong Y (2020) Long-term exposure to fine particulate matter and development of chronic obstructive pulmonary disease in the elderly. In Environment International 143:105895. https://doi.org/10.1016/j.envint.2020.105895
Jones RM, Brosseau LM (2015) Aerosol transmission of infectious disease. In Journal of Occupational and Environmental Medicine 57(5):501–508. https://doi.org/10.1097/JOM.0000000000000448
Katsouyanni K, Touloumi G, Spix C, Schwartz J, Balducci F, Medina S et al (1997) Short-term effects of ambient sulphur dioxide and particulate matter on mortality in 12 European cities: results from time series data from the APHEA project. Air Pollution and Health: a European Approach. In BMJ (Clinical research ed.) 314(7095):1658–1663. https://doi.org/10.1136/bmj.314.7095.1658
Kernbach-Wighton G, Kuhlencord A, Roβbach K, Fischer G (1996) Bone-dust in autopsies: reduction of spreading. In Forensic Science International 83(2):95–103. https://doi.org/10.1016/s0379-0738(96)02020-8
Kernbach-Wighton G, Kuhlencord A, Saternus KS (1998) Knochenstäube bei der Autopsie Entstehung, Ausbreitung Kontamination. In Der Pathologe 19(5):355–360. https://doi.org/10.1007/s002920050297
Kraus M, Šenitková IJ (2017) Particulate matter mass concentration in residential prefabricated buildings related to temperature and moisture. In IOP Conf Ser: Mater Sci Eng. 245:42068. https://doi.org/10.1088/1757-899X/245/4/042068
Matsuo R, Michikawa T, Ueda K, Ago T, Nitta H, Kitazono T, Kamouchi M (2016) Short-term exposure to fine particulate matter and risk of ischemic stroke. In Stroke 47(12):3032–3034. https://doi.org/10.1161/STROKEAHA.116.015303
Meier R, Eeftens M, Phuleria HC, Ineichen A, Corradi E, Davey M et al (2015) Differences in indoor versus outdoor concentrations of ultrafine particles, PM2.5, PMabsorbance and NO2 in Swiss homes. In Journal of exposure science & environmental epidemiology 25(5):499–505. https://doi.org/10.1038/jes.2015.3
Noble WC, Lidwell OM, Kingston D (1963) The size distribution of airborne particles carrying micro-organisms. In the Journal of Hygiene 61:385–391. https://doi.org/10.1017/s0022172400020994
Orellano P, Reynoso J, Quaranta N, Bardach A, Ciapponi A (2020) Short-term exposure to particulate matter (PM10 and PM2.5), nitrogen dioxide (NO2), and ozone (O3) and all-cause and cause-specific mortality: systematic review and meta-analysis. In Environment international 142:105876. https://doi.org/10.1016/j.envint.2020.105876
Plenzig S, Bojkova D, Held H, Berger A, Holz F, Cinatl J et al (2021) Infectivity of deceased COVID-19 patients. In International Journal of Legal Medicine 135(5):2055–2060. https://doi.org/10.1007/s00414-021-02546-7
Pluim JME, Jimenez-Bou L, Gerretsen RRR, Loeve AJ (2018) Aerosol production during autopsies: the risk of sawing in bone. In Forensic Science International 289:260–267. https://doi.org/10.1016/j.forsciint.2018.05.046
Qian J, Ferro AR, Fowler KR (2008) Estimating the resuspension rate and residence time of indoor particles. In Journal of the Air & Waste Management Association (1995) 58(4):502–516. https://doi.org/10.3155/1047-3289.58.4.502
Seyit M, Yilmaz A, Ozen M, Dogan C, Kantar AA (2020) Inhaler intoxications developed during autopsy of the corpse due to cyanide intake: case series. In the American Journal of Emergency Medicine 38(7):1542.e5-1542.e8. https://doi.org/10.1016/j.ajem.2020.03.053
Templeton GL, Illing LA, Young L, Cave D, Stead WW, Bates JH (1995) The risk for transmission of mycobacterium tuberculosis at the bedside and during autopsy. In Annals of Internal Medicine 122(12):922–925. https://doi.org/10.7326/0003-4819-122-12-199506150-00005
Wei Y, Wang Y, Di Q, Choirat C, Koutrakis P, Zanobetti A et al (2019) Short term exposure to fine particulate matter and hospital admission risks and costs in the Medicare population: time stratified, case crossover study. In BMJ (clinical Research Ed) 367:l6258. https://doi.org/10.1136/bmj.l6258
Wenner L, Pauli U, Summermatter K, Gantenbein H, Vidondo B, Posthaus H (2017) Aerosol generation during bone-sawing procedures in veterinary autopsies. In Veterinary Pathology 54(3):425–436. https://doi.org/10.1177/0300985816688744
WHO Regional Office for Europe (2010): WHO Guidelines for indoor air quality. Selected Pollutants. Geneva: World Health Organization. Available online at http://gbv.eblib.com/patron/FullRecord.aspx?p=1582967. Accessed 16 July 2021
Yorifuji T, Kashima S (2019) Long-term exposure to fine particulate matter and cancer mortality in Japan. In Environmental Epidemiology 3:457. https://doi.org/10.1097/01.EE9.0000611164.49484.4b
Zarzycki R, Włodarczyk R, Kobyłecki R, Bis Z (2020) Impact of collisions between fine and coarse particles on the terminal velocity of coarse particles. In Powder Technology 363:181–186. https://doi.org/10.1016/j.powtec.2020.01.018
Funding
Open Access funding enabled and organized by Projekt DEAL.
Author information
Authors and Affiliations
Contributions
Conceptualization: Janis Dröge, David A. Groneberg, Marcel A. Verhoff; methodology: Janis Dröge; formal analysis and investigation: Janis Dröge; data curation: Janis Dröge, Ibrahim El Moussaoui; validation: Janis Dröge, David A. Groneberg, Marcel A. Verhoff, Stefanie Plenzig; visualization: Janis Dröge, Doris Klingelhöfer; writing—original draft preparation: Janis Dröge; writing—review and editing: Doris Klingelhöfer, Ibrahim El Moussaoui, David A. Groneberg, Marcel A. Verhoff, Stefanie Plenzig, Hannelore Held; resources: David A. Groneberg, Marcel A. Verhoff; supervision: Janis Dröge.
Corresponding author
Ethics declarations
Ethics approval
This research does not contain any studies with human participants or animals.
Consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare no competing interests.
Additional information
Responsible Editor: Lotfi Aleya
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Dröge, J., Moussaoui, I.E., Klingelhöfer, D. et al. Particulate matter emissions during autopsies: a method to reduce exposure. Environ Sci Pollut Res 29, 60519–60530 (2022). https://doi.org/10.1007/s11356-022-20021-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-022-20021-7