
Abstract
The development of congenital heart disease (CHD) is a complicated process and affected by multiple environmental factors, as genetic factors, and the interactions among those factors. Previous studies have shown that intrauterine hypoxic environment exposure is a risk factor of CHD, but the genetic factors involved in the process are not clear. In this study, given that tetralogy of Fallot (TOF) is a CHD with hypoxemia as its primary pathophysiological manifestation, an in silico analysis was performed to reveal the relationship between potential target genes (miR-124) with the energy metabolism in non-syndromic TOF patients’ cardiomyocyte. Furthermore, the study investigated the correlation between the primary miR-124 (rs531564) polymorphism and CHD susceptibility in 432 sporadic patients and 450 controls from two different altitude provinces (city) in China. Our study indicated that the minor C allele of rs531564 correlated with reduced risk of CHD in the low altitude city. Besides, the C allele has elevated frequency in the high-altitude group. Therefore, our findings suggest that the minor C allele of rs531564 SNP may be involved in the reduction of the risk of CHD in a way that interacts with the intrauterine hypoxic environmental factors.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Congenital heart disease (CHD) is the most prevalent human birth malformation with an incidence of 1 approximately in 100 newborns. CHD is also a major cause of perinatal and infant mortality, with about 220,000 deaths worldwide each year (Marelli et al. 2014). The exact etiology of CHD is not fully understood, especially the etiology of sporadic, non-syndromic CHD. Previous studies have shown that multiple factors contribute to the risk of CHD in various geographic areas and genetic backgrounds, suggesting the complex mechanisms underlying the development of CHD, which involve numerous environmental and genetic factors, and also, the interaction between them (Hinton 2013). Intrauterine hypoxic environment exposure, caused by high-altitude hypoxic environment or placental insufficiency, is one of the risk factors for CHD (Bae et al. 2003; Gagnon 2003; Hasan 2016; Herrera et al. 2016; Miao et al. 1988; Yue and Tomanek 1999; Zheng et al. 2013). The possible molecular mechanism might be associated with the fact that chronic fetal hypoxia alters cardiac gene expression, accelerates pre-existing cardiomyocytes exit the cell cycle, increases myocyte apoptosis, and decreases in the number of cardiomyocytes (Botting et al. 2014; Osterman et al. 2015; Zhang 2005).
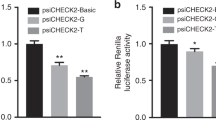
Recent studies have reported that several microRNAs (miRNAs) play pivotal roles in cardiac development under hypoxic intrauterine environment, being termed as hypoxia-responsive miRNAs (Azzouzi et al. 2015; Lock et al. 2017). Such miRNAs, as miR-199a and miR-210, presented a significant correlation with cardiac energy metabolism. Rane et al. 2009 suggested that miR-199a, is a miRNA downregulated under hypoxia, regulated cardiac metabolism by targetting hypoxia-inducible factor-1 alpha and sirtuin 1. Hu et al. 2010 reported that upregulated hypoxia-responsive miR-210 exhibits a cardio-protective effect by inhibiting Efna3 and Ptp1b, in a mouse model of myocardial infarction. Besides, it is widely reported that miR-124 is a downregulated hypoxia-responsive miRNA involved in the regulation of biological processes in a variety of cells (Gong et al. 2017; Gu et al. 2016; Li et al. 2017). Moreover, a line of evidence has demonstrated that rs531564 (G>C), a functional SNP of the primary miR-124 (pri-miR-124) sequence, is associated with the expression of mature miR-124. The G allele carriers, which represent the major population, have a higher expression level of miR-124 transcript than the C allele carriers, which represent a minor population (Chen et al. 2018; Li et al. 2017; Zou et al. 2017). The rs531564 polymorphism of pri-miR-124 is also one of the risk factors for human cervical cancer, esophageal squamous cell carcinoma, colorectal cancer, and type 2 diabetes (Gao et al. 2015; Li et al. 2015; Wu and Zhang 2014; Ye et al. 2008). The downregulated miR-124 also exhibits a cardio-protective function by attenuating endoplasmic reticulum stress (Bao et al. 2017). However, evidence supporting a correlation between the rs531564 polymorphism of pri-miR-124 and CHD is inadequate.
Tetralogy of Fallot (TOF) is one of the most common forms of cyanotic CHD. The main pathological manifestation of this type of CHD is chronic hypoxemia (Apitz et al. 2009). In the present study, gene expression and miRNA expression profiles pertaining to non-syndromic TOF were downloaded from the Gene Expression Omnibus database (Clough and Barrett 2016). These datasets were utilized to identify key genes and miRNAs that play significant roles in various biological processes in cardiomyocytes under hypoxic condition by running through three target gene prediction databases, TargetScan (Agarwal et al. 2015), miRTarBase (Chou et al. 2018), and RNA22 (Miranda et al. 2006). The results indicated the correlation between the energy metabolism in cardiomyocytes of non-syndromic TOF and the downregulation of miR-124 and several other potential target genes. We also investigated the correlation between the rs531564 polymorphism of pri-miR-124 and CHD in two groups of patients from an area with different altitudes. One group is from Beijing (altitudes ranging from 28 to 96 m); the other group is from Gansu (altitudes ranging from 1085 to 2690 m). The study also indicated that the minor C allele of rs531564 polymorphism of pri-miR-124 was associated with a reduced risk of CHD in Beijing population but not Gansu population.
Methods
Microarray data
Two gene expression profiles (GSE26125 and GSE35776) and a miRNA expression profile of GSE35490 were obtained from the GEO database. The GSE26125 dataset, based on the platform of GPL11329 (Applied CodeLink Human Whole Genome Bioarray), consisted of samples from 16 idiopathic TOF patients without the 22q11.2 deletion and five controls. The GSE35776 dataset, based on the platform of GPL5175 (Affymetrix Human Exon 1.0 ST Array), consisted of samples from 16 non-syndromic TOF patients without the 22q11.2 deletion, three fetal hearts, and eight normal controls. The miRNA expression profile of GSE35490, based on the platform of GPL8786 (Affymetrix Multispecies miRNA-1 Array), shared the same sample source as GSE35776. A more detailed description of the included samples can be found in two previously published studies (Bittel et al. 2011; O’Brien et al. 2012).
Data processing and in silico analysis
The limma package in R software was applied to perform data preprocessing and screening of differentially expressed genes (DEGs) as well as miRNAs (DEMIs) (Ritchie et al. 2015). For each dataset, DEGs or DEMIs between non-syndromic TOFs and normal controls were screened. The threshold values for the screening include the following: |log2 fold change (FC)| > 1.00 and P < 0.05. The overlap of DEGs between GSE26125 and GSE35776 was used for subsequent analysis. In the present study, three online prediction programs (TargetScan, miRTarBase, RNA22) were used for screening the potential targets of DEMIs. The overlapped portion of the results from the three online prediction programs was considered as the potential targets of DEMIs.
Gene Ontology (GO) term enrichment and Kyoto Encyclopedia of Genes and Genomes (KEGG) pathway enrichment analysis of the identified DEGs were performed using KOBAS 3.0, a most recently updated online tool for gene function annotation (Xie et al. 2011). Significant GO terms and KEGG pathways enriched with upregulated or downregulated DEGs were screened with a criterion of P < 0.05.
To explore the interactive relationships among DEGs, a protein-protein interaction network was constructed by the Search Tool for the Retrieval of Interacting Genes (STRING, version 10.0), and a combined score of 0.40 was set as the cut-off criterion (Szklarczyk et al. 2017). After filtering out target genes of DEMIs, the regulation relationships between the miRNA- mRNA and protein-protein interaction were integrated. The network was constructed using Cytoscape (www.cytoscape.org). The key gene modules were identified from PPI network by using the Molecular Complex Detection (MCODE) plugin based on Cytoscape. The number of nodes was equal or more than 5; a MCODE score more than 5 was set as cut-off criterion. The pathway enrichment analysis of genes in the modules was performed with KOBAS 3.0. P < 0.05 was considered to be significant.
Gene set enrichment analysis
The importance of Gene Set Enrichment Analysis (GSEA) is its capability to capture the correlation between weakly differential expression in gene sets and phenotypes (Subramanian et al. 2005). GSEA was able to not only verify the DEGs enrichment analysis but also cover up the shortcomings of DEGs analysis. In the present study, GSEA was used to compare the expression profiles of gene sets named h.all.v6.1.symbols.gmt [Hallmarks], which is from Molecular Signature Database, between non-syndromic TOFs and normal controls. The gene expression profiles that were analyzed by GSEA were GSE26125 and GSE35776. Normalization enrichment score (NES), P value, and false discovery rate (FDR) were calculated. A gene set is considered significantly enriched with the criteria of P < 0.05 and FDR < 0.25. GSEA was performed by using the GSEA 3.0 program, provided by Broad Institute (http://www.broadinstitute.org/gsea/index.jsp).
Samples
Blood samples were obtained from 2 independent case-control groups. In total, 432 CHD patients and 450 healthy controls were recruited in this study. The Beijing group consisted of 120 CHD patients and 130 healthy controls. The Gansu group was composed of 312 CHD patients and 320 healthy controls. Sporadic CHD patients underwent chest X-ray examination, electrocardiography, and echocardiography. Patients who were diagnosed with CHD but without recognized genetic syndrome, chromosome abnormalities, or family history of CHD were enrolled in this study. The controls were recruited from the same geographical area. They were age, gender, and ethic matched with unrelated subjects enrolled in the present study and from the same hospital for health screening. The study was approved by the Ethics Committees of Lanzhou University of Basic Medical Science (20160204) and all participants provided informed consent forms.
DNA extraction and genotyping
Genomic DNA was extracted from peripheral blood using a Cwbio® Blood Genomic DNA Mini Kit (Cwbio, Beijing, China). SNP genotyping was performed by Shanghai Genesky Bio-Tech Genetic Core Lab (Shanghai, China) using multiplex ligation detection reaction. Approximately 5% of the samples were randomly selected to validate the genotyping results by directly sequencing and the reproducibility of the genotyping results was 100%. The primers used for PCR and DNA sequencing were as follows:
Forward: 5′-TCTTCTACCCACCCCTCTTCC-3′;
Reverse: 5′-AATCTGCACACACAAGCACTC-3′.
Statistical analysis
The Hardy-Weinberg equilibrium (HWE) of the genotype distributions of the controls was determined by a goodness-of-fit chi-square (χ2) test. Continuous and categorical variables were estimated by Student’s t test and the χ2 test, respectively. Allele and genotype frequency distributions of rs531564 in patients and controls were evaluated by χ2 tests. The relationship between rs531564 polymorphism and CHD risk was analyzed by unconditional logistic regression model, and the odds ratio (OR) and the 95% confidence intervals (95% CI) with adjustments for age and gender were calculated. All statistical analyses were performed with the SPSS19.0 software package (SPSS, Chicago, IL, USA) and P < 0.05 was considered statistically significant.
Results
The downregulated miR-124 was a potential key miRNA in non-syndromic TOF
Screened with the thresholds of |log2(FC)| > 1.00 and P < 0.05, 3211 and 641 upregulated DEGs and 498 and 265 downregulated DEGs were identified from GSE26125 and GSE35776, respectively (Fig. S1a, b). Three hundred eighteen upregulated DEGs and 12 downregulated DEGs were overlapped between the two gene expression profile (Fig. S1d, e) (Supplementary Table S1). In addition, a total of 49 DEMIs, 21 upregulated miRNAs, and 28 downregulated miRNAs were identified from GSE35490 (Fig. S1c). Only those miRNA target genes that also intersect with DEGs were selected. Finally, 29 pairs of potential miRNA-mRNA interactions were identified, including 10 miRNAs and 28 mRNAs. The downregulated miR-124 (log2(FC) = − 1.26, P < 0.001) was predicted to target 10 upregulated genes, including CALU, AK3, ABHD5, LPCAT3, CHP1, MYPN, AK2, PGRMC2, ATP6V0E1, and ACAA2.
The results from the GO analysis revealed that the upregulated DEGs were significantly enriched in biological processes (BP) that were involved in cellular (P = 2.09e−23), metabolic (P = 1.14e−20), and oxidation-reduction processes (P = 1.54e−20). Based on the KEGG pathway enrichment analysis, upregulated DEGs were significantly enriched in metabolic pathways (P = 7.96e−14), oxidative phosphorylation (P = 2.27e−09), and proteasome (P = 2.99e−07). The top 10 GO biological processes and KEGG pathways enriched for upregulated DEGs were presented in Table S2.
The PPI network of DEGs was comprised of 212 nodes and 584 edges. The top four modules the PPI networks involved in the process related to the proteasome, oxidative phosphorylation, metabolic pathways, cardiac muscle contraction, and peroxisome (Fig. 1) (Table S3). After integrating with 29 miRNA-DEG regulatory pairs, the predicted target genes of DEMI miR-124 were presented in both Module 3 and Module 4, which were enriched in the processes related to oxidative phosphorylation, metabolic pathways, as well as peroxisome (Fig. 1) (Table 1).

The key modules of protein-protein interaction network. The red cycles indicate upregulation DEGs, and the green triangle represents the downregulated miR-124. Size of the nodes indicates the interaction degrees
Gene set enrichment analysis
To further confirm DEGs enrichment analysis, GSEA was conducted in two independent non-syndromic TOF GEO datasets (GSE26125 and GSE35776). The results produced 13 upregulated gene sets from non-syndromic TOF compared with control and non-downregulated gene sets (Table S4). Metabolic pathways, oxidative phosphorylation, and peroxisome gene sets were significantly enriched. Moreover, we noticed that gene sets related to hypoxia (Fig. 2a, b), glycolysis (Fig. 2c, d), DNA repair, and mTORC1 signaling were also significantly enriched in non-syndromic TOF.

Gene set enrichment analysis in non-syndromic TOF. a–d Hypoxia- or glycolysis-related gene set was enriched in GSE26125 and GSE35776, respectively. NES, normalized enrichment score. FDR, false discovery rate; e Venn diagram illustrating the overlapped area that positively correlated with hypoxia, glycolysis gene sets, and miR-124 potential targets; f potential targets of miR-124
The result demonstrated that four potential target genes of miR-124 (SDC4, PGM1, NR3C1, and GPC1) were found in the hypoxia gene set and four potential target genes (AK3, GLRX, RBCK1, and GPC1) were listed in the glycolysis gene set (Fig. 2e). Combined with the target genes found from DEGs analysis, a total number of 16 potential target genes of miR-124 were identified in both of the non-syndromic TOF mRNA profiles, GSE26125 and GSE35776 (Fig. 2f).
Characteristics of the study subjects
The characteristics of the study subjects are summarized in Table 2. The mean age of the CHD patients and controls was 9.53 ± 13.88 years and 9.48 ± 12.11 years, respectively. The gender distribution in the CHD patients was 234 males and 198 females, and there were 261 males and 189 females among the healthy controls. There was no statistical difference between the cases and the controls regarding age (P = 0.95) and gender (P = 0.25). Moreover, there was no statistical difference in terms of age and gender distribution between the cases and the controls in both the Beijing group and Gansu group.
Correlation between the rs531564 SNP and the susceptibility to CHD
The genotypes of rs531564 were in HWE in the control groups, both separately from Beijing or Gansu, and the combined control group (P = 0.16, P = 0.78, and P = 0.51, respectively) (Fig. 3). To explore the correlation between rs531564 and CHD susceptibility, both allelic and genotypic distribution were assessed. Additionally, various genetic models were applied with the adjustment for age and gender under unconditional logistic regression analyses (Table 3). The combined group data indicated that the C allele of rs531564 of pri-miR-124 is associated with the decreased risk of CHD (OR = 0.72, 95% CI = 0.55–0.93, P = 0.01). In addition, similar results were obtained by analyzing the data with other models including the following: the codominant model (OR = 0.69, 95% CI = 0.51–0.93, P = 0.03), dominant model (OR = 0.67, 95% CI = 0.50–0.91, P = 0.01), overdominant model (OR = 0.70, 95% CI = 0.52–0.95, P = 0.02), and log-additive model (OR = 0.70, 95% CI = 0.53–0.91, P = 0.01) after adjustment. In the Beijing group, the genotype distribution of rs531564 was significantly different between CHD patients and healthy controls. Our finding indicated that minor C allele was significantly associated with the decreased risk of CHD in the Beijing group. This result was consistent among the analysis with different models including the allelic model (OR = 0.36, 95% CI = 0.21–0.63, P = 3e−04), the codominant model (OR = 0.30, 95% CI = 0.16–0.56, P = 4e−04), the dominant model (OR = 0.30, 95% CI = 0.16–0.56, P = 1e−04), the overdominant model (OR = 0.30, 95% CI = 0.16–0.57, P = 1e−04), and the log-additive model (OR = 0.33, 95% CI = 0.19–0.60, P = 1e−04). However, our findings did not support a significant correlation between rs531564 SNP and the risk of CHD in the Gansu group. In addition, it was noticed that the C allele frequency in the Gansu group was higher than that in the Beijing group in both the case-only group (0.15 and 0.08, respectively, χ2 = 8.38; P = 0.0038) and overall population (0.16 and 0.14, respectively, χ2 = 1.60; P = 0.21), while it is lower in the Gansu group than that in the Beijing group if the analysis was done in the control-only group (0.17 and 0.19, respectively, χ2 = 0.61; P = 0.43).

Representative chromograph of rs531564 sequence in each indicated genotype
It was shown in the stratification analysis of subtypes of CHD that rs531564 was significantly associated with isolated CHD (OR = 0.40, 95% CI = 0.19–0.86, P = 0.01 in dominant model after adjusted by gender and age) and complex CHD (OR = 0.21, 95% CI = 0.09–0.51, P = 1e−04 in dominant model after adjusted by gender and age) in the Beijing group. More specifically, the significant association of rs531564 was found in TOF cases (OR = 0.18, 95% CI = 0.04–0.82, P = 0.01 in dominant model after adjusted by gender and age) in the Beijing group (Table 4). There was no statistical correlation between rs531564 SNP and any subtypes of CHD in the Gansu group.
In summary, our results suggested that the rs531564 SNP of pri-miR-124 correlated with the risk of CHD in the Beijing group.
Discussion
In the present study, two gene expression profiles (GSE26125 and GSE35776) of non-syndromic TOF, of which the main pathological feature is chronic hypoxemia, were used to reveal the underlying molecular mechanisms in cardiomyocytes under hypoxic condition. A total of 330 DEGs were identified in non-syndromic TOF samples, including 318 upregulated genes and 12 downregulated genes. Functional and pathway enrichment analysis in DEGs revealed that genes involved in metabolic pathways and oxidative phosphorylation were significantly enriched. Besides the oxidative phosphorylation gene set, the GSEA found that the gene sets related to hypoxia, glycolysis, and fatty acid metabolism were enriched in non-syndromic TOF. In addition, the oxidative phosphorylation gene set was seen to be more statistically significant enriched than the glycolysis gene set. The above-mentioned results indicated that glycolysis and oxidative phosphorylation were upregulated in cardiomyocytes of non-syndromic TOF and the upregulated oxidative phosphorylation may predominantly relate to the maintenance of energy production. For TOF patients, anatomic defects lead to oxygen deficiency from the decreased pulmonary blood flow. Traditionally, cardiomyocyte energy metabolism shifts from oxidative phosphorylation to glycolysis to maintain ATP levels under the stressful hypoxic conditions (Azzouzi et al. 2015; Balaban 2012). However, ATP is produced solely from glycolysis only if the oxygen concentration limits the function of oxidative phosphorylation, which is the case in severe hypoxia (Hollinshead and Tennant 2016). The changes of metabolism found in non-syndromic TOF patients may be attributed to the effect of chronic mild hypoxia on oxidative phosphorylation.
MiRNAs is a class of non-coding short RNAs with 19 to 24 nucleotides and regulates gene expression by binding to the 3′ untranslated region of target mRNA at the post-transcriptional level (Azzouzi et al. 2015). Therefore, miRNAs influence various cellular processes such as metabolism, differentiation, proliferation, and apoptosis. As part of this study, we also screened DEMIs in the TOF-related miRNA profile GSE35490. Finally, 29 pairs of miRNA-mRNA, including 10 miRNAs and 28 mRNAs, were identified by integrated analysis of three target gene prediction databases. We found that the downregulated miR-124 is likely to be associated with metabolic pathways in addition to oxidative phosphorylation by modulating the potential target genes (AK2, AK3, ACAA2) in key modules of the PPI network. Besides, seven potential target genes (SDC4, PGM1, NR3C1, GPC1, AK3, GLRX, and RBCK1) of miR-124 were positively correlated with hypoxia and glycolysis gene sets in non-syndromic TOF. The entire above-mentioned miR-124 target genes have been considered to be related to metabolism (Garcia-Esparcia et al. 2015; Laforet et al. 2017). In addition, previous studies have suggested that hypoxia induces miR-124 downregulation which promotes prostate cancer cell survival, leads to chondrogenesis, and promotes proliferation of pulmonary artery smooth muscle cells. These functions are mediated by the regulation of PIM1, NFATc1, and GRB2, respectively (Gong et al. 2017; Gu et al. 2016; Li et al. 2017). The downregulated miR-124 also exhibits a cardio-protective effect by attenuating endoplasmic reticulum stress (Bao et al. 2017). Therefore, it is reasonable that miR-124 may play an important role in regulating myocardial metabolism in non-syndromic TOF. Given that metabolism, especially folate metabolism, has an important influence on cardiac development and gene expression specificity at different stages of organ development, further investigation is needed to unveil the relationship between miR-124 and folate metabolism or heart development under hypoxic conditions (Blom and Smulders 2011; Cripps and Olson 2002).
It is critical for healthy heart development in a hypoxic intrauterine environment during early fetal life, but long-term exposure to the hypoxic environment may lead to fetal intrauterine growth restriction (Bae et al. 2003; Gagnon 2003; Herrera et al. 2016; Yue and Tomanek 1999). Chronic intrauterine hypoxia also affects heart development at some stages, and possible molecular mechanisms include that chronic fetal hypoxia alters cardiac gene expression, accelerates pre-existing cardiomyocytes exit the cell cycle, increases myocyte apoptosis, and reduces in the number of cardiomyocytes (Botting et al. 2014; Osterman et al. 2015; Zhang 2005). Furthermore, studies have shown that the incidence rate and the severity of CHD are higher in high-altitude areas. Hypoxic environment was considered as a risk factor of congenital heart disease in high-altitude areas (Hasan 2016; Miao et al. 1988; Zheng et al. 2013). As mentioned above, miR-124 is involved in the regulation of cardiomyocyte metabolism under hypoxic conditions. Moreover, it is widely reported that the G allele of rs531564, in pri-miR-124, is associated with increased mature miR-124 expression (Chen et al. 2018; Li et al. 2017; Zou et al. 2017). In this study, we evaluated the association between the rs531564 polymorphism of pri-miR-124 and CHD in two independent groups of Chinese patients who were from Beijing (with altitudes ranging from 28 to 96 m) or Gansu (with altitudes ranging from 1085 to 2690 m). Our findings revealed that the C allele of rs531564 of pri-miR-124 is associated with the decreased risk of CHD, especially complex CHD, in the group from Beijing, but not in the Gansu group. The correlation between the different geographical areas and CHD risk is different for the rs531564 SNP in this study. It seems to be consistent with the report that the etiology of sporadic, non-syndromic CHD involves the interaction of multiple genetic and environmental factors (Hinton 2013). The decrease risk of CHD risk associated with the C allele of rs531564 may be partly explained by the lower expression level of mature miR-124 than that of the G allele. Low levels of miR-124 expression contribute to the maintenance of cardiomyocyte metabolism under hypoxic conditions caused by placental insufficiency or hypoxic environmental exposure. Additionally, we noticed that although there was no statistical correlation between the C allele and CHD in the tested patients from Gansu, where the altitude is high, the C allele frequency in the Gansu group was higher than that in the Beijing group in the case-only group or overall population. These data indicated that the higher frequency of the C allele in the Gansu group is likely to be related to environmental selection pressure (Verhulst and Neale 2016). Further investigation is needed to explore whether this SNP is associated with positive selection for high-altitude hypoxic adaptation.
In summary, two mRNA profiles as well as a miRNA profile of non-syndromic TOF provided evidence that miR-124 is involved in the regulation of cardiomyocyte metabolism under hypoxic conditions. This study also revealed a significant correlation between the rs531564 SNP of pri-miR-124 and the risk of CHD in population from area with low altitude, but not in population from areas with high altitude. Our results provide new insights into the etiology of sporadic, non-syndromic CHD. However, given the limitations of this study in terms of sample size, narrow range of the altitude of the involved area and the single ethnicity, more comprehensive studies with larger sample size, different regions, and ethnic groups are needed to confirm our findings.
References
Agarwal V, Bell GW, Nam JW, Bartel DP (2015) Predicting effective microRNA target sites in mammalian mRNAs. Elife 12, 4
Apitz C, Webb GD, Redington AN (2009) Tetralogy of Fallot. Lancet 374(9699):1462–1471
Azzouzi HE, Leptidis S, Doevendans PA, De Windt LJ (2015) HypoxamiRs: regulators of cardiac hypoxia and energy metabolism. Trends Endocrinol Metab 26(9):502–508
Bae S, Xiao Y, Li G, Casiano CA, Zhang L (2003) Effect of maternal chronic hypoxic exposure during gestation on apoptosis in fetal rat heart. Am J Physiol Heart Circ Physiol 285(3):983–990
Balaban RS (2012) Perspectives on: SGP symposium on mitochondrial physiology and medicine: metabolic homeostasis of the heart. J Gen Physiol 139(6):407–414
Bao Q, Chen L, Li J, Zhao M, Wu S, Wu W, Liu X (2017) Role of microRNA-124 in cardiomyocyte hypertrophy induced by angiotensin II. Cell Mol Biol (Noisy-le-grand) 63(4):23–27
Bittel DC, Butler MG, Kibiryeva N, Marshall JA, Chen J, Lofland GK, O’Brien JE (2011) Gene expression in cardiac tissues from infants with idiopathic conotruncal defects. BMC Med Genet 4:1
Blom HJ, Smulders Y (2011) Overview of homocysteine and folate metabolism. With special references to cardiovascular disease and neural tube defects. J Inherit Metab Dis 34(1):75–81
Botting KJ, McMillen IC, Forbes H, Nyengaard JR, Morrison JL (2014) Chronic hypoxemia in late gestation decreases cardiomyocyte number but does not change expression of hypoxia-responsive genes. J Am Heart Assoc 3(4)
Chen S, Chen Y, Gao Y, Zuo Y, Zhou X (2019) Effect of single-nucleotide polymorphism in pri-microRNA-124 on poststroke motor function recovery. J Cell Biochem 119(5):7125-7132
Chou CH, Shrestha S, Yang CD, Chang NW, Lin YL, Liao KW, Huang WC, Sun TH, Tu SJ, Lee WH, Chiew MY, Tai CS, Wei TY, Tsai TR, Huang HT, Wang CY, Wu HY, Ho SY, Chen PR, Chuang CH, Hsieh PJ, Wu YS, Chen WL, Li MJ, Wu YC, Huang XY, Ng FL, Buddhakosai W, Huang PC, Lan KC, Huang CY, Weng SL, Cheng YN, Liang C, Hsu WL, Huang HD (2018) miRTarBase update 2018: a resource for experimentally validated microRNA-target interactions. Nucleic Acids Res 46(D1):D296–D302
Clough E, Barrett T (2016) The gene expression omnibus database. Methods Mol Biol 1418:93–110
Cripps RM, Olson EN (2002) Control of cardiac development by an evolutionarily conserved transcriptional network. Dev Biol 246(1):14–28
Gagnon R (2003) Placental insufficiency and its consequences. Eur J Obstet Gynecol Reprod Biol 110(Suppl 1):S99–S107
Gao XR, Wang HP, Zhang SL, Wang MX, Zhu ZS (2015) Pri-miR-124 rs531564 polymorphism and colorectal cancer risk. Sci Rep 5:14818
Garcia-Esparcia P, Hernandez-Ortega K, Ansoleaga B, Carmona M, Ferrer I (2015) Purine metabolism gene deregulation in Parkinson’s disease. Neuropathol Appl Neurobiol 41(7):926–940
Gong M, Liang T, Jin S, Dai X, Zhou Z, Gao M, Huang S, Luo J, Zou L, Zou X (2017) Methylation-mediated silencing of miR-124 facilitates chondrogenesis by targeting NFATc1 under hypoxic conditions. Am J Transl Res 9(9):4111–4124
Gu H, Liu M, Ding C, Wang X, Wang R, Wu X, Fan R (2016) Hypoxia-responsive miR-124 and miR-144 reduce hypoxia-induced autophagy and enhance radiosensitivity of prostate cancer cells via suppressing PIM1. Cancer Med 5(6):1174–1182
Hasan A (2016) Relationship of high altitude and congenital heart disease. Indian Heart J 68(1):9–12
Herrera EA, Rojas RT, Krause BJ, Ebensperger G, Reyes RV, Giussani DA, Parer JT, Llanos AJ (2016) Cardiovascular function in term fetal sheep conceived, gestated and studied in the hypobaric hypoxia of the Andean altiplano. J Physiol 594(5):1231–1245
Hinton RB (2013) Genetic and environmental factors contributing to cardiovascular malformation: a unified approach to risk. J Am Heart Assoc 2(3):e000292–e000292
Hollinshead KE, Tennant DA (2016) Mitochondrial metabolic remodeling in response to genetic and environmental perturbations. Wiley Interdiscip Rev Syst Biol Med 8(4):272–285
Hu S, Huang M, Li Z, Jia F, Ghosh Z, Lijkwan MA, Fasanaro P, Sun N, Wang X, Martelli F, Robbins RC, Wu JC (2010) MicroRNA-210 as a novel therapy for treatment of ischemic heart disease. Circulation 122(11 S):S124–S131
Laforet P, Malfatti E, Vissing J (2017) Update on new muscle glycogenosis. Curr Opin Neurol 30(5):449–456
Li Y, Zhang Y, Li X, Shi L, Tao W, Shi L, Yang M, Wang X, Yang Y, Yao Y (2015) Association study of polymorphisms in miRNAs with T2DM in Chinese population. Int J Med Sci 12(11):875–880
Li Q, Qian Z, Wang L (2017) Pri-microRNA-124 rs531564 polymorphism minor allele increases the risk of pulmonary artery hypertension by abnormally enhancing proliferation of pulmonary artery smooth muscle cells. Int J Chron Obstruct Pulmon Dis 12:1351–1361
Lock MC, Botting KJ, Tellam RL, Brooks D, Morrison JL (2017) Adverse intrauterine environment and cardiac miRNA expression. Int J Mol Sci 18(12):2628
Marelli AJ, Ionescu-Ittu R, Mackie AS, Guo L, Dendukuri N, Kaouache M (2014) Lifetime prevalence of congenital heart disease in the general population from 2000 to 2010. Circulation 130(9):749–756
Miao CY, Zuberbuhler JS, Zuberbuhler JR (1988) Prevalence of congenital cardiac anomalies at high altitude. J Am Coll Cardiol 12(1):224–228
Miranda KC, Huynh T, Tay Y, Ang YS, Tam WL, Thomson AM, Lim B, Rigoutsos I (2006) A pattern-based method for the identification of MicroRNA binding sites and their corresponding heteroduplexes. Cell 126(6):1203–1217
O’Brien JE, Kibiryeva N, Zhou XG, Marshall JA, Lofland GK, Artman M, Chen J, Bittel DC (2012) Noncoding RNA expression in myocardium from infants with tetralogy of Fallot. Circ Cardiovasc Genet 5(3):279–286
Osterman H, Lindgren I, Lindstrom T, Altimiras J (2015) Chronic hypoxia during development does not trigger pathologic remodeling of the chicken embryonic heart but reduces cardiomyocyte number. Am J Phys Regul Integr Comp Phys 309(10):1204–1214
Rane S, He M, Sayed D, Vashistha H, Malhotra A, Sadoshima J, Vatner DE, Vatner SF, Abdellatif M (2009) Downregulation of miR-199a derepresses hypoxia-inducible factor-1alpha and Sirtuin 1 and recapitulates hypoxia preconditioning in cardiac myocytes. Circ Res 104(7):879–886
Ritchie ME, Phipson B, Wu D, Hu Y, Law CW, Shi W, Smyth GK (2015) limma powers differential expression analyses for RNA-sequencing and microarray studies. Nucleic Acids Res 43(7):e47
Subramanian A, Tamayo P, Mootha VK, Mukherjee S, Ebert BL, Gillette MA, Paulovich A, Pomeroy SL, Golub TR, Lander ES, Mesirov JP (2005) Gene set enrichment analysis: a knowledge-based approach for interpreting genome-wide expression profiles. Proc Natl Acad Sci U S A 102(43):15545–15550
Szklarczyk D, Morris JH, Cook H, Kuhn M, Wyder S, Simonovic M, Santos A, Doncheva NT, Roth A, Bork P, Jensen LJ, von Mering C (2017) The STRING database in 2017: quality-controlled protein-protein association networks, made broadly accessible. Nucleic Acids Res 45(D1):D362–D368
Verhulst B, Neale MC (2016) Minor allele frequency changes the nature of genotype by environment interactions. Behav Genet 46(5):726–733
Wu H, Zhang J (2014) miR-124 rs531564 polymorphism influences genetic susceptibility to cervical cancer. Int J Clin Exp Med 7(12):5847–5851
Xie C, Mao X, Huang J, Ding Y, Wu J, Dong S, Kong L, Gao G, Li CY, Wei L (2011) KOBAS 2.0: a web server for annotation and identification of enriched pathways and diseases. Nucleic Acids Res 39:316–322
Ye Y, Wang KK, Gu J, Yang H, Lin J, Ajani JA, Wu X (2008) Genetic variations in microRNA-related genes are novel susceptibility loci for esophageal cancer risk. Cancer Prev Res (Phila) 1(6):460–469
Yue X, Tomanek RJ (1999) Stimulation of coronary vasculogenesis/angiogenesis by hypoxia in cultured embryonic hearts. Dev Dyn 216(1):28–36
Zhang L (2005) Prenatal hypoxia and cardiac programming. J Soc Gynecol Investig 12(1):2–13
Zheng JY, Tian HT, Zhu ZM, Li B, Han L, Jiang SL, Chen Y, Li DT, He JC, Zhao Z, Cao Y, Qiu YG, Li TC (2013) Prevalence of symptomatic congenital heart disease in Tibetan school children. Am J Cardiol 112(9):1468–1470
Zou L, Zhang G, Liu L, Chen C, Cao X, Cai J (2017) A MicroRNA-124 polymorphism is associated with fracture healing via modulating BMP6 expression. Cell Physiol Biochem 41(6):2161–2170
Acknowledgments
We express our appreciation to the original DNA donors who made this study possible.
Funding
This work was supported by a grant from the National Natural Science Foundation of China (31670379) and the Health Industry Research Project of Gansu Province (GSWSKY2016-04).
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
This study was approved by the Ethics Committees of Lanzhou University of Basic Medical Science (20160204) and all participants provided informed consent forms.
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Responsible editor: Philippe Garrigues
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Fig. S1
Identification of DEGs and DEMIs. a, b, c Volcano plot of GSE26125, GSE35776, and GSE35490 under the thresholds of |log2(FC)| > 1.00 and P < 0.05; d, e Venn diagram illustrating the overlapped upregulated DEGs and downregulated miRNA potential targets, downregulated DEGs and upregulated miRNA potential targets. (PNG 149 kb)
Table S1
(XLS 121 kb)
Table S2
(DOC 41 kb)
Table S3
(DOC 33 kb)
Table S4
(DOC 36 kb)
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Yang, W., Yi, K., Yu, H. et al. Correlation between pri-miR-124 (rs531564) polymorphism and congenital heart disease susceptibility in Chinese population at two different altitudes: a case-control and in silico study. Environ Sci Pollut Res 26, 21983–21992 (2019). https://doi.org/10.1007/s11356-019-05350-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11356-019-05350-4