
Abstract
Backgrounds
Obstructive sleep apnea (OSA) is common in patients on hemodialysis, but its correlation with chronic kidney disease (CKD) is not clear. We aimed to clarify the relationship between OSA without hypertension or diabetes and incidence of CKD in Taiwan.
Methods
This population-based cohort study consisted of patients with newly diagnosed OSA between 2000 and 2009. The comparison cohort was matched for age, sex, diabetes mellitus, and hypertension. All subjects previously diagnosed with acute or chronic kidney disease were excluded. The primary end point was newly diagnosed CKD.
Results
We identified 6866 subjects with OSA during the 10-year study period. The median duration until development of CKD in the OSA cohort was 3.2 years, 2.5 months earlier than that in the non-OSA cohort. After exclusion of hypertension and diabetes, 4319 OSA patients was identified and the hazard ratio (HR) of CKD with OSA was 1.37 (95 % confidence interval [CI], 1.05–1.77; p = 0.019). In the subgroup analysis, an increased incidence of CKD in OSA was observed in women (HR, 1.41; 95 % CI, 1.12–1.78; p = 0.0036).
Conclusions
This longitudinal population-based cohort study provides evidence that patients with OSA even without diabetes or hypertension are at higher risk of developing CKD over the next 3 years and nearly 2.5 months earlier than the non-OSA cohort, particularly women.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Obstructive sleep apnea (OSA) is a disorder that affects 2–4 % of adults in the general population of Taiwan and worldwide [1, 2]. OSA patients increase hypertension and diabetes mellitus risk [3–6]. Cardiovascular and neurocognitive complications are the most common and severe consequences noted in these patients [7]. The underlying mechanisms are complex and involve oxidative stress and inflammation, sympathetic tone stimulation, and fluid shifting, which may negatively affect kidney function; thus, it is not surprising that OSA is highly prevalent among patients on hemodialysis [8–10].
Chronic kidney disease (CKD) affects 10–13 % of the general population in Taiwan and is associated with substantial morbidity and mortality rates, particularly with regard to cardiovascular diseases and end-stage kidney disease [11]. Diabetes and hypertension are the two major risk factors for CKD [12–14]. Our previous study found that patients with OSA without diabetes and hypertension have a higher prevalence of impaired renal function [15]. Sim et al. reported an association of OSA and CKD in cross-sectional study and Ahmed et al, reported that nocturnal hypoxia may have a higher prevalence for loss of kidney function [16–18]. TAHRANI reported a small diabetes cohort that higher prevalence of OSA will enhance the declaration of eGFR in 2-year follow up [19]. Molnar reported higher incidence of CKD associated to OSA veterans in a 3 million USA cohort subgroup analysis [20]. Recently, Lee reported OSA patients predisposing to the development of CKD and end-stage renal disease (ESRD) [21]. However, the interaction between CKD and pure OSA without hypertension or diabetes is not confirmed due to selection bias. To clarify the relationship of OSA and CKD, we aimed to design this retrospective longitudinal population-based case-control cohort study especially focused on pure OSA without diabetes or hypertension.
Materials and methods
Data source
This was a retrospective cohort study that used the Longitudinal Health Insurance Database 2000 (LHID2000) in Taiwan, a subset of the National Health Insurance Research Database (NHIRD) (http://nhird.nhri.org.tw/date_01.html), containing all original claims data for one million randomly sampled insured patients in 2000. The NHIRD comprises medical and pharmacy claims including inpatient and outpatient diagnoses and procedures based on the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9-CM). The data are considered reasonably representative of Taiwan residents, since >99 % of Taiwan’s population was enrolled in the NHI program [22].
All personal identifiers were encrypted by the Bureau of NHI prior to being released to researchers. The institutional review board of Chang Gung Memorial Hospital approved this retrospective study (IRB number 101-5057B) and waived the requirement for informed consent.
Study and comparison cohort
The study cohort consisted of 6866 adult patients (aged ≥18 years) with newly diagnosed OSA between 2000 and 2009. A diagnosis of OSA included sleep apnea with hypersomnia (ICD-9-CM 780.53), sleep apnea with insomnia (ICD-9-CM 780.51), and sleep apnea unspecified (ICD-9-CM 780.57) as previously reported [23]. Due to Taiwan’s medical coverage system, there must be a diagnosis for further disease checkup in clinic; we only enrolled patients with OSA diagnosis completing three or more outpatient verification visits within 1 year or those who had been hospitalized with a diagnosis of OSA. The index date for each patient was that of the first OSA diagnosis.
Acute or chronic kidney disease diagnosis is based on the ICD-9-CM code including 581 (nephritic syndrome), 582 (chronic glomerulonephritis), 583 (nephritis and nephropathy not specified as acute or chronic), 584 (acute kidney failure), and 585 (chronic kidney disease) OSA patients, and patients who were previously diagnosed with acute or CKD (ICD-9-CM 581-585) before the index date were excluded from the analyses.
The comparison cohort consisted of adults (age ≥18 years) without OSA (non-OSA) who were randomly selected from the remaining individuals after excluding any diagnosis with OSA in the LHID2000 database. All non-OSA subjects were matched with the study cohort for age, sex, diabetes (ICD-9-CM 250), hypertension (ICD-9-CM 401.0, 401.1, and 401.9), and index year. None of the non-OSA subjects had been previously diagnosed with acute or CKD (ICD-9-CM 581-585) before the index year. All study and comparison cohort members were followed up for at least 1 year. Details are described on the right of the flow chart (Fig. 1, right side) and Table 1.

Flow chart of ascertainment of OSA and non-OSA cohort
Events of chronic kidney disease
The primary end point was newly diagnosed CKD during the study period. The CKD diagnosis included 582 (chronic glomerulonephritis), 583 (nephritis and nephropathy not specified as acute or chronic), and 585 (chronic kidney disease) as previous reported on AJKD, and the nephritic syndrome was excluded due to the urine protein loss could not be confirmed from the database system. Newly diagnosed cases of CKD were identified as those who visited the outpatient care clinic or were hospitalized with a diagnosis of CKD (ICD-9-CM 582, 583, 585). However, to eliminate enrollment bias, we excluded the CKD episodes that occurred during the first year of follow up in this cohort study.
Statistical analyses
For this analysis, follow-up time began on the index date of OSA and ended at the time of the CKD diagnosis, when the patient quit insurance, or on January 31, 2011, whichever came first. The descriptive results were displayed by the number of baseline characteristics among the OSA and non-OSA cohorts. The incidence of CKD was calculated based on person-years of follow-up for 2000–2011. Person-years of follow-up were estimated for each individual from the index date until the date of the CKD diagnosis, when the patient quit insurance, or on January 31, 2011. Kaplan-Meier methods and the log-rank test were used to examine the cumulative probability of CKD development according to the presence of OSA. The Cox proportional hazards models were used to analyze the association of baseline OSA with the risk of CKD with or without adjustment for age, sex, diabetes, and hypertension at baseline. The proportional hazards assumption was not violated, and hazard ratios (HRs) with 95 % confidence intervals (CIs) were calculated. Two-tailed tests were used and p values <0.05 were considered significant. The statistical analyses were performed using SAS version 9.2 (SAS Institute Inc., Cary, NC, USA) and STATA version 14.0 (STATA Corp, College Station, TX, USA).
Results
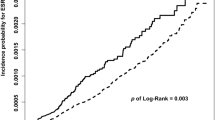
The baseline demographics and clinical characteristics of the OSA and non-OSA cohorts are given in Table 1. There were no important differences between cohorts as expected due to the sample matching. We identified 6866 subjects with OSA who were followed up for a median of 4.4 years (total person-years = 33,402.5). In the non-OSA cohort, 34,330 subjects were matched to the OSA cohort and followed up for a median of 4.4 years (total person-years = 167,146.1). Of the 41,196 study subjects, 1082 reported CKD during the course of the study: 215 in the OSA cohort (median follow-up years, 3.2) and 867 in the non-OSA cohort (median follow-up years, 3.4). Patients in the OSA cohort developed CKD 2.5 months earlier than those in the non-OSA cohort did. The crude CKD event rate was higher for patients with OSA (23.3 outcomes per 1000 person-years) than for those without OSA (19.6 outcomes per 1000 person-years). With the Cox proportional hazards model, estimated HR (95 % CI) for risk of CKD with OSA versus non-OSA was 1.24 (1.07–1.44; p = 0.0045) (Table 2). After adjustment for age, sex, hypertension, and diabetes, the association between OSA and first CKD event remained significant. After excluding the confounding factors of CKD, hypertension, and diabetes, the risk of incident CKD persisted in the OSA cohort (HR, 1.37; 95 % CI, 1.05–1.77; p = 0.019) (Table 3). Figure 2 shows the cumulative probability of CKD development by OSA presence. The OSA cohort had higher cumulative incidence of CKD. The difference was statistically significant according to the log-rank test in comparison with the non-OSA cohort (p = 0.0045).

The cumulative probability of CKD development among the OSA and non-OSA cohort
Subgroup analyses
Table 3 also shows the relationship between OSA and the incidence of CKD in patients aged 18–39 years and ≥40 years as well as in men and women separately. An increase in the HR of the incidence of CKD due to OSA was observed in persons ≥40 years of age (HR, 1.21; 95 % CI, 1.03–1.42; p = 0.022) and borderline significant in persons 18–39 years of age (HR, 1.52; 95 % CI, 1.01–2.28; p = 0.045). Similarly, the risk of developing CKD was higher for women with OSA than for those without it (HR, 1.41; 95 % CI, 1.12–1.79; p = 0.0039). However, the risk of developing CKD among men with OSA was not significant.
Discussion
Our group is the first to report a correlation between CKD and OSA severity in 40 OSA patients without hypertension and diabetes [15]. Later, Y et al. reported the association with a worse estimated glomerular filtration rate in 100 patients with CKD stage 3–4 and OSA [24, 25]. However, all these are small prevalence studies. Previous large longitudinal OSA cohort studies such as the Sleep Heart Health Study (SHHS) and Wisconsin Sleep Cohort Study (WSS) reported the associated adverse outcomes of hypertension, stroke, and mortality but not CKD outcomes [3, 4, 26]. Lee reported the predisposing association between OSA and CKD recently using the same Taiwan’s medical insurance database. However, due to statistic limitation, the selection bias about hypertension and diabetes cannot be clarified in their follow-up model. Also, the importance at young adult is difficult to evaluate due to the age selection (over 30 years old) and excluded from their study population. Our study from Taiwan’s one million medical insurance databases is the first large population-based cohort study to use a prospective statistical model to identify the increasing 1.37-fold incidence of CKD risk in pure OSA patients in Taiwan after excluding hypertension and diabetes. In addition to a higher risk of developing CKD, the OSA cohort developed CKD 2.5 months earlier than the non-OSA cohort did.
Previous studies have mounting evidences of OSA accelerating diabetes nephropathy [19, 27], and a small study and case report showed that CPAP treatment may improve proteinuria in diabetes patients [28, 29]. There are many factors including sleep cycle and the renin-angiotensin-aldosterone system [30, 31], intermittent hypoxia-induced endothelial dysfunction and artery stiffness [32–34], and renal tubular dysfunction-related nocturnal natriuresis [29, 35, 36] that may impact kidney function from OSA. In recent reviews, Dr Adeseun emphasizes intermittent hypoxia and sleep fragmentation-related kidney injury mechanism and possible more direct insults from intermittent hypoxia to CKD [37]. Dr Hanly reported more evidences suggest that OSA having direct impact on CKD especially from direct effect of intrarenal hypoxia and activation of the systemic and renal renin-angiotensin system but need further studies [38]. From the finding of our study, the evidence is obvious that OSA patients have impact on the deterioration of kidney function in a 12-year follow up. It is important to emphasize regularly checking the renal function and even the early renal injury markers in OSA patients, especially on the patients coexisting with other risk factors such as diabetes or hypertension. It is also important to emphasize the treatment of OSA such as CPAP therapy on the view of preventing the CKD.
Second, a difference in the outcomes between the sexes was noted by the SHHS and WSS, with a higher risk in men for stroke and hypertension, but all studies enrolled only patients >40 years with OSA. We found that the incidence of CKD was persistently high with a 1.5-fold risk in the OSA group aged 18–39 years, which has not been reported previously and needs further verification and evaluation. Finally, although the same trend was seen, the risk of CKD was statistically confirmed in women only. This interesting finding may be impacted by other inaccessible factors from this study, such as Chinese herb drug usage including aristolochic acid, which requires further verification [39].
However, there are limitations relating to the population-based ICD-9 code-recording database itself and others [19, 22]. First, environmental and risk factors such as aging, smoking, obesity, and metabolic syndrome could not be identified from the database and adjusted for in the analysis.
Second, the exact detailed laboratory data such as polysomnography information and proteinuria severity were inaccessible. Therefore, this study reported results from patients with OSA based on clinical diagnosis alone. This may underestimate the effects of severe OSA on CKD development. A prospective OSA cohort study is needed in the future to clarify the relationship between OSA severity and CKD.
In conclusion, this longitudinal population-based cohort study using a statistically prospective model provides the first evidence that patients with pure OSA without hypertension or diabetes are at higher risk of developing CKD over the next 3 years and nearly 2.5 months earlier than the non-OSA cohort, particularly women.
References
Mirrakhimov AE, Sooronbaev T, Mirrakhimov EM (2013) Prevalence of obstructive sleep apnea in Asian adults: a systematic review of the literature. BMC Pulm Med 13:10. doi:10.1186/1471-2466-13-10
Chuang LP, Hsu SC, Lin SW, Ko WS, Chen NH, Tsai YH (2008) Prevalence of snoring and witnessed apnea in Taiwanese adults. Chang Gung Med J 31(2):175–181
Quan SF, Howard BV, Iber C, Kiley JP, Nieto FJ, O’Connor GT, Rapoport DM, Redline S, Robbins J, Samet JM, Wahl PW (1997) The Sleep Heart Health Study: design, rationale, and methods. Sleep 20(12):1077–1085
Young T (2009) Rationale, design and findings from the Wisconsin Sleep Cohort Study: toward understanding the total societal burden of sleep disordered breathing. Sleep Medicine Clinics 4(1):37–46. doi:10.1016/j.jsmc.2008.11.003
Anothaisintawee T, Reutrakul S, Van Cauter E, Thakkinstian A (2015) Sleep disturbances compared to traditional risk factors for diabetes development: systematic review and meta-analysis. Sleep Med Rev 30:11–24. doi:10.1016/j.smrv.2015.10.002
Kendzerska T, Gershon AS, Hawker G, Tomlinson G, Leung RS (2014) Obstructive sleep apnea and incident diabetes. A historical cohort study. Am J Respir Crit Care Med 190(2):218–225. doi:10.1164/rccm.201312-2209OC
Somers VK, White DP, Amin R, Abraham WT, Costa F, Culebras A, Daniels S, Floras JS, Hunt CE, Olson LJ, Pickering TG, Russell R, Woo M, Young T, American Heart Association Council for High Blood Pressure Research Professional Education Committee CoCC, American Heart Association Stroke C, American Heart Association Council on Cardiovascular N, American College of Cardiology F (2008) Sleep apnea and cardiovascular disease: an American Heart Association/American College of Cardiology Foundation Scientific Statement from the American Heart Association Council for High Blood Pressure Research Professional Education Committee, Council on Clinical Cardiology, Stroke Council, and Council on Cardiovascular Nursing. In collaboration with the National Heart, Lung, and Blood Institute National Center on Sleep Disorders Research (National Institutes of Health). Circulation 118(10):1080–1111. doi:10.1161/CIRCULATIONAHA.107.189375
Kutner N, Zhang R, Johansen K, Bliwise D (2013) Associations among nocturnal sleep, daytime intradialytic sleep, and mortality risk in patients on daytime conventional hemodialysis: US Renal Data System special study data. Hemodialysis international International Symposium on Home Hemodialysis 17(2):223–229. doi:10.1111/hdi.12005
Ahmad S, Gupta M, Gupta R, Dhyani M (2013) Prevalence and correlates of insomnia and obstructive sleep apnea in chronic kidney disease. N Am J Med Sci 5(11):641–646. doi:10.4103/1947-2714.122306
Unruh ML (2007) Sleep apnea and dialysis therapies: things that go bump in the night? Hemodialysis international International Symposium on Home Hemodialysis 11(4):369–378. doi:10.1111/j.1542-4758.2007.00203.x
Wen CP, Cheng TY, Tsai MK, Chang YC, Chan HT, Tsai SP, Chiang PH, Hsu CC, Sung PK, Hsu YH, Wen SF (2008) All-cause mortality attributable to chronic kidney disease: a prospective cohort study based on 462 293 adults in Taiwan. Lancet 371(9631):2173–2182. doi:10.1016/S0140-6736(08)60952-6
Haroun MK, Jaar BG, Hoffman SC, Comstock GW, Klag MJ, Coresh J (2003) Risk factors for chronic kidney disease: a prospective study of 23,534 men and women in Washington County, Maryland. J Am Soc Nephrol 14(11):2934–2941
Gooneratne IK, Ranaweera AK, Liyanarachchi NP, Gunawardane N, Lanerolle RD (2008) Epidemiology of chronic kidney disease in a Sri Lankan population. Int J Diabetes in Developing Countries 28(2):60–64. doi:10.4103/0973-3930.43101
Retnakaran R, Cull CA, Thorne KI, Adler AI, Holman RR, Group US (2006) Risk factors for renal dysfunction in type 2 diabetes: U.K. Prospective Diabetes Study 74. Diabetes 55(6):1832–1839. doi:10.2337/db05-1620
Chou YT, Lee PH, Yang CT, Lin CL, Veasey S, Chuang LP, Lin SW, Lin YS, Chen NH (2011) Obstructive sleep apnea: a stand-alone risk factor for chronic kidney disease. Nephrol Dial Transplant 26(7):2244–2250. doi:10.1093/ndt/gfq821
Sim JJ, Rasgon SA, Kujubu DA, Kumar VA, Liu IL, Shi JM, Pham TT, Derose SF (2009) Sleep apnea in early and advanced chronic kidney disease: Kaiser Permanente Southern California cohort. Chest 135(3):710–716. doi:10.1378/chest.08-2248
Turek NF, Ricardo AC, Lash JP (2012) Sleep disturbances as nontraditional risk factors for development and progression of CKD: review of the evidence. Am J Kidney Dis 60(5):823–833. doi:10.1053/j.ajkd.2012.04.027
Ahmed SB, Ronksley PE, Hemmelgarn BR, Tsai WH, Manns BJ, Tonelli M, Klarenbach SW, Chin R, Clement FM, Hanly PJ (2011) Nocturnal hypoxia and loss of kidney function. PLoS One 6(4):e19029. doi:10.1371/journal.pone.0019029
Tahrani AA, Ali A, Raymond NT, Begum S, Dubb K, Altaf QA, Piya MK, Barnett AH, Stevens MJ (2013) Obstructive sleep apnea and diabetic nephropathy: a cohort study. Diabetes Care 36(11):3718–3725. doi:10.2337/dc13-0450
Molnar MZ, Mucsi I, Novak M, Szabo Z, Freire AX, Huch KM, Arah OA, Ma JZ, Lu JL, Sim JJ, Streja E, Kalantar-Zadeh K, Kovesdy CP (2015) Association of incident obstructive sleep apnoea with outcomes in a large cohort of US veterans. Thorax 70(9):888–895. doi:10.1136/thoraxjnl-2015-206970
Lee YC, Hung SY, Wang HK, Lin CW, Wang HH, Chen SW, Chang MY, Ho LC, Chen YT, Liou HH, Tsai TC, Tseng SH, Wang WM, Lin SH, Chiou YY (2015) Sleep apnea and the risk of chronic kidney disease: a nationwide population-based cohort study. Sleep 38(2):213–221. doi:10.5665/sleep.4400
Lin YS, Liu PH, Wu LS, Chen YM, Chang CJ, Chu PH (2014) Major adverse cardiovascular events in adult congenital heart disease: a population-based follow-up study from Taiwan. BMC Cardiovasc Disord 14:38. doi:10.1186/1471-2261-14-38
Tien KJ, Chou CW, Lee SY, Yeh NC, Yang CY, Yen FC, Wang JJ, Weng SF (2014) Obstructive sleep apnea and the risk of atopic dermatitis: a population-based case control study. PLoS One 9(2):e89656. doi:10.1371/journal.pone.0089656
Sakaguchi Y, Shoji T, Kawabata H, Niihata K, Suzuki A, Kaneko T, Okada N, Isaka Y, Rakugi H, Tsubakihara Y (2011) High prevalence of obstructive sleep apnea and its association with renal function among nondialysis chronic kidney disease patients in Japan: a cross-sectional study. Clin J Am Soc Nephrol 6(5):995–1000. doi:10.2215/CJN.08670910
Sakaguchi Y, Hatta T, Hayashi T, Shoji T, Suzuki A, Tomida K, Okada N, Rakugi H, Isaka Y, Tsubakihara Y (2013) Association of nocturnal hypoxemia with progression of CKD. Clin J Am Soc Nephrol 8(9):1502–1507. doi:10.2215/CJN.11931112
Redline S, Yenokyan G, Gottlieb DJ, Shahar E, O’Connor GT, Resnick HE, Diener-West M, Sanders MH, Wolf PA, Geraghty EM, Ali T, Lebowitz M, Punjabi NM (2010) Obstructive sleep apnea-hypopnea and incident stroke: the sleep heart health study. Am J Respir Crit Care Med 182(2):269–277. doi:10.1164/rccm.200911-1746OC
Leong WB, Nolen M, Thomas GN, Adab P, Banerjee D, Taheri S (2014) The impact of hypoxemia on nephropathy in extremely obese patients with type 2 diabetes mellitus. J Clin Sleep Med 10(7):773–778. doi:10.5664/jcsm.3870
Masuda T, Honma S, Sasaki N, Hanawa-Yazawa S, Iwazu Y, Kusano E, Asano Y (2012) Effect of continuous positive airway pressure on proteinuria in obstructive sleep apnea. Clin Kidney J 5(3):257–260. doi:10.1093/ckj/sfs046
Kinebuchi S, Kazama JJ, Satoh M, Sakai K, Nakayama H, Yoshizawa H, Narita I, Suzuki E, Gejyo F (2004) Short-term use of continuous positive airway pressure ameliorates glomerular hyperfiltration in patients with obstructive sleep apnoea syndrome. Clin Sci 107(3):317–322. doi:10.1042/CS20040074
Charloux A, Gronfier C, Lonsdorfer-Wolf E, Piquard F, Brandenberger G (1999) Aldosterone release during the sleep-wake cycle in humans. Am J Physiol 276(1 Pt 1):E43–E49
Follenius M, Krieger J, Krauth MO, Sforza F, Brandenberger G (1991) Obstructive sleep apnea treatment: peripheral and central effects on plasma renin activity and aldosterone. Sleep 14(3):211–217
van Bussel BC, Schouten F, Henry RM, Schalkwijk CG, de Boer MR, Ferreira I, Smulders YM, Twisk JW, Stehouwer CD (2011) Endothelial dysfunction and low-grade inflammation are associated with greater arterial stiffness over a 6-year period. Hypertension 58(4):588–595. doi:10.1161/HYPERTENSIONAHA.111.174557
Doonan RJ, Scheffler P, Lalli M, Kimoff RJ, Petridou ET, Daskalopoulos ME, Daskalopoulou SS (2011) Increased arterial stiffness in obstructive sleep apnea: a systematic review. Hypertens Res 34(1):23–32. doi:10.1038/hr.2010.200
Peralta CA, Jacobs DR Jr, Katz R, Ix JH, Madero M, Duprez DA, Sarnak MJ, Criqui MH, Kramer HJ, Palmas W, Herrington D, Shlipak MG (2012) Association of pulse pressure, arterial elasticity, and endothelial function with kidney function decline among adults with estimated GFR >60 mL/min/1.73 m(2): the Multi-Ethnic Study of Atherosclerosis (MESA). Am J Kidney Dis 59(1):41–49. doi:10.1053/j.ajkd.2011.08.015
Rodenstein DO, D’Odemont JP, Pieters T, Aubert-Tulkens G (1992) Diurnal and nocturnal diuresis and natriuresis in obstructive sleep apnea. Effects of nasal continuous positive airway pressure therapy. Am Rev Respir Dis 145(6):1367–1371. doi:10.1164/ajrccm/145.6.1367
Casserly LF, Chow N, Ali S, Gottlieb DJ, Epstein LJ, Kaufman JS (2001) Proteinuria in obstructive sleep apnea. Kidney Int 60(4):1484–1489. doi:10.1046/j.1523-1755.2001.00952.x
Adeseun GA, Rosas SE (2010) The impact of obstructive sleep apnea on chronic kidney disease. Curr Hypertens Rep 12(5):378–383. doi:10.1007/s11906-010-0135-1
Hanly PJ, Ahmed SB (2014) Sleep apnea and the kidney: is sleep apnea a risk factor for chronic kidney disease? Chest 146(4):1114–1122. doi:10.1378/chest.14-0596
Yang WC, Hwang SJ (2008) Incidence, prevalence and mortality trends of dialysis end-stage renal disease in Taiwan from 1990 to 2001: the impact of national health insurance. Nephrol Dial Transplant 23(12):3977–3982. doi:10.1093/ndt/gfn406
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
National Sciences Council, Taiwan (NSC 102-2314-B-182A-060-MY2u) and Chang Gung Memorial Hospital, Taiwan (CMRPG5D101 for Dr Lin, CMRPG3B1311 for Dr Chu and CMRPG391233, NMRPG3C0042, CMRPG3D1011 for Dr Chen) provided financial support in the form of researcher funding. The sponsor had no role in the design or conduct of this research.
Conflict of interest
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements) or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed consent
All personal identifiers were encrypted by the Bureau of NHI prior to being released to researchers. The institutional review board of Chang Gung Memorial Hospital approved this retrospective study (IRB number 101-5057B) and waived the requirement for informed consent. This study is based in part on data from the National Health Insurance Research Database provided by the Bureau of National Health Insurance, Department of Health and managed by the National Health Research Institutes. The interpretation and conclusions contained herein do not represent those of the Bureau of National Health Insurance, Department of Health or National Health Research Institutes.
Additional information
Yu-Sheng Lin and Pi-Hua Liu contributed equally to this work.
Rights and permissions
Open Access This article is distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium, provided you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made.
About this article

Cite this article
Lin, YS., Liu, PH., Lin, SW. et al. Simple obstructive sleep apnea patients without hypertension or diabetes accelerate kidney dysfunction: a population follow-up cohort study from Taiwan. Sleep Breath 21, 85–91 (2017). https://doi.org/10.1007/s11325-016-1376-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11325-016-1376-2