
Abstract
Objectives
This systematic review and meta-analysis examines the efficacy of physical activity interventions in the reduction of antisocial behavior in children and adults. Several possible moderators, including study design, sample characteristics (age, proportion male, and sample type), control group, and outcome characteristics (type of activity, duration, frequency), were also investigated.
Methods
A literature search was performed in the following databases: PubMed, Ebsco/SportDiscus, Ebsco/APA PsycINFO, Ebsco/ERIC, Ebsco/Criminal Justice Abstracts, Embase.com, and Clarivate Analytics/Web of Science Core Collection from inception to June 2021. Studies were eligible if they reviewed the effect of chronic physical activity interventions on antisocial behavior compared to wait-list, no-exercise, or attention control samples. The following studies were excluded: animal studies, studies reporting on acute exercise, studies including yoga or mindfulness as the sole measure of physical activity, and studies including substance (ab)use and/or smoking as the only outcome measure. A random effects model was used to calculate pooled effect sizes. The risk of bias was assessed using the Cochrane risk-of-bias tool (version 2).
Results
The search yielded 29 studies, of which 20 were included in the meta-analysis. Results indicate a significant small-to-medium effect (g = − 0.26) with a 95% confidence interval ranging from − 0.48 to − 0.04 in favor of physical activity interventions. Significant moderators included type of control group, type of physical activity, and type of antisocial behavior, with larger effect sizes for comparisons with inactive control groups (g = − 0.31), interventions containing walking, jogging, or running as the main type of physical activity (g = − 0.87), and anger/hostility as an antisocial outcome measure (g = − 0.42).
Conclusions
Physical activity interventions may be a promising way to reduce antisocial behavior in children and adults. However, due to the overall high risk of bias in the included studies, more sound evaluation research is needed to better understand the functioning and to improve the possible implementation of physical activity interventions.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Antisocial behavior is a heterogeneous group of behaviors, including criminal offenses, aggression, and conduct problems. Such behavior violates societal rules or the rights of others (Moffitt, 2013) and affects both the perpetrator and the victim (Cohen & Piquero, 2009; Heap, 2021). Conventional treatments aimed at reducing antisocial behavior mostly rely on cognitive behavioral theory (Bennett & Gibbons, 2000), yet with limited efficacy (Bennett & Gibbons, 2000; Dodge & McCourt, 2010; Frick, 2016; Lipsey & Cullen, 2007; Reid & Gacono, 2000). Re-offending rates after treatment are at 60% or higher (Fazel & Wolf, 2015; van der Put et al., 2016) and non-completion rates (i.e., percentage of participants dropping out before treatment completion) range from 20 to 40% (Rubin et al., 2006), indicating the need for additional interventions.
One proposed alternative intervention encompasses physical activity (i.e., any skeletal muscle-induced movement requiring energy expenditure (Caspersen, Powell, & Chistenson, 1985)). Physical activity interventions may offer an accessible and inexpensive substitute for current interventions with multiple health benefits, including improved physical and mental well-being (Daskalopoulou et al., 2017; Lubans et al., 2012; Paluska & Schwenk, 2000). Physical activity has been suggested to improve several facets related to antisocial behavior, including enhanced self-control and emotion regulation (Boat & Cooper, 2019), greater feelings of social inclusion (Perks, 2007), and a more positive self-identity and self-worth (Bowker, 2006; Liu et al., 2015). Physical activity programs have been increasingly used by local governments and institutes (e.g., prisons, youth offender institutions) worldwide to rehabilitate offenders and prevent maladaptive or problematic behavior (Ekholm et al., 2013; Hartmann & Depro, 2006; Jones-Palm & Palm, 2005; Kelly, 2013; Makkai et al., 2003; Meek, 2018; Nelson et al., 2006; Nichols, 2010; Taylor et al., 2015), yet their effectiveness remains largely unclear.
To date, two previous meta-analytic reviews have examined the effect of physical activity on externalizing behavior in youth (Harwood et al., 2017; Spruit et al., 2016). The first review investigated the effect of martial arts on the reduction of aggression, anger, and violence in youth aged < 18. The authors included 12 studies with a comparison group but no randomized controlled trials (RCT). They found an average significant effect of martial arts on aggression, but only after removing the three studies that consisted of one-time comparisons (as opposed to interventional, longitudinal, and cross-sectional studies) (Harwood et al., 2017). The second meta-review quantified the effect of physical activity interventions on four psychosocial outcomes, including externalizing problems (i.e., aggression, delinquency, or other conduct problems) in adolescents (aged 10–21). A study was included if a considerable part of the intervention included sports or (aerobic) exercise and the design was experimental (i.e., a comparison group available). They found a significant small-to-moderate effect of physical activity interventions on the reduction of externalizing problems, with larger effect sizes for comparisons with other types of intervention (i.e., psychosocial or other leisure activities) and no effect for comparisons with waitlist or no-treatment groups (Spruit et al., 2016).
Regarding adult populations, the effect of physical activity interventions has only been previously examined in adults assessed through the Diagnostic and Statistical Manual of Mental Disorders (DSM: (American Psychiatric Association, 2022)) as nicotine, alcohol, and illicit drug (e.g., heroin, cocaine) abusers (Wang et al., 2014). The authors included 22 RCTs on physical activity (including aerobic exercise, resistance training, and mind–body exercises such as yoga, tai chi, and qi gong). They found physical activity interventions to significantly decrease withdrawal symptoms and increase abstinence rates, with larger effects in illicit drugs users compared to nicotine and alcohol abusers (Wang et al., 2014). However, 30% of the included studies (n = 7) contained elements of mindfulness (Auty et al., 2017), classifying mind–body exercises such as yoga and qi gong as physical activity. Mindfulness has been shown to be effective in the reduction of antisocial behavior (Gillions et al., 2019; Tao et al., 2021) and thus the question remains if physical activity without mindfulness can elicit the same results in adults.
Recently, a meta-analytic review was published on the effect of sports programs on crime-related outcomes including reconviction, drug use, anger, self-control, and impulsivity in a sample containing both children and adults (Jugl et al., 2021). Studies were eligible if the design was quasi-experimental or a RCT. The authors analyzed 10 studies in individuals at risk of (re)-offending or from the general population, if the program was designed to prevent criminal behavior (mean age 25, age range 7–59 years). Martial arts programs, outdoor activities, and adventure activities were excluded, but no other restrictions were put on the type of sports program. Their results indicate a significant positive effect on criminal behavior with no moderating effect of program, sample, or study characteristics.
Although previous reviews suggest a positive effect of physical activity on antisocial behavior, they do not address the heterogeneous nature of antisocial behavior (Popovici et al., 2014) or they are limited due to methodological issues. Specifically, the existing meta-review on martial arts (Harwood et al., 2017) did not account for elements of mindfulness associated with martial arts (Miyata et al., 2020) which may have affected the results (Gillions et al., 2019; Tao et al., 2021). In addition, the inclusion of cross-sectional studies hampers causal statements regarding the effect of physical activity (Harwood et al., 2017). Furthermore, the meta-analysis of Spruit et al. on physical activity interventions contained a relatively small number of studies (n = 14) which may have limited generalizability. They also examined three other interrelated psychosocial outcomes (internalizing problems, academic achievement, and self-concept). As the authors state, the results of the individual meta-analyses should therefore not be interpreted independently due to the high level of interrelatedness (Spruit et al., 2016). Finally, both meta-analytic reviews were limited to adolescents or young adults (aged < 21). Thus far, only Jugl and colleagues included both children and adults, yet most of their sports programs specifically aimed to promote personal development (e.g., improving prosocial behavior and self-confidence) rather than to improve fitness parameters (Jugl et al., 2021). This resulted in the inclusion of a range of activities that were not always related to physical activity, such as reading and numeracy lessons. Furthermore, 2 studies examined the effects of yoga (containing mindfulness: (Auty et al., 2017)) which could have affected the results as described earlier. In summary, the effects of physical activity on antisocial behavior in both children and adults remain unclear.
As existing physical activity programs target both youth and adults (Ekholm et al., 2013; Hartmann & Depro, 2006; Jones-Palm & Palm, 2005; Kelly, 2013; Makkai et al., 2003; Meek, 2018; Nelson et al., 2006; Nichols, 2010; Taylor et al., 2015), it is important to assess efficacy across different age groups. Moreover, due to the highly heterogeneous nature of antisocial behavior, it is possible that not all types of antisocial behavior are affected similarly by physical activity interventions, depending on the underlying reason for the displayed behavior. For example, aggressive tendencies may be acquired through social learning, such as conditioning and observation (Bandura, 1973), whereas hostility is defined as an emotional state (Tsikandilakis et al., 2020). Thus, different effects may be expected. This is illustrated by a study where an additional after-school volleyball program significantly improved physical and verbal aggression and anger, but not hostility in adolescents, compared to a no-intervention control sample (Trakjovic et al., 2020). Similarly, different types of physical activity interventions may have different impacts. For example, one study found positive effects on hostility after high-intensity strength training but no effect after cardiovascular plus resistance training in prisoners (Battaglia et al., 2015). To date, no meta-review exists on the effect of physical activity that considers the possible effects of both a heterogeneous predictor and outcome.
The current meta-analysis attempts to fill this gap by examining the efficacy of physical activity interventions in the reduction of antisocial behavior (e.g., aggression, externalizing behavior, delinquency, hostility, anger, and other maladaptive or disruptive behaviors) in both children and adults. By addressing a broader range of antisocial behavior and physical activity interventions (excluding elements of mindfulness) and only including RCTs and (quasi)-experimental designs, the present review aims to take the next step in research on physical activity as a treatment reducing antisocial behavior. In addition, by coding and analyzing multiple possible moderators (Spruit et al., 2016), including study design, operationalization of outcome, type of physical activity, and sample characteristics, we hope to gain more insight into who could benefit most from physical activity interventions, and how. This may aid in the individual tailoring of interventions, possibly increasing treatment efficacy (Frick, 2016; Rubin et al., 2006). To increase generalizability and comparability between outcome measures (Hofer & Piccinin, 2009), we did not include studies on nicotine and substance (ab)use. Physical activity interventions included all interventions for children and adults in which sports and/or (aerobic) exercise were the main treatments. We focused on chronic (i.e., regular) (Guiney & Machado, 2013) physical activity as opposed to acute (i.e., a single bout) physical activity (Chang et al., 2012).
Methods
Literature search
This meta-analytic review was conducted and reported following the preferred reporting items for systematic reviews and meta-analysis (PRISMA) guidelines (Page et al., 2021). The PRISMA checklist can be found in Appendix A. A comprehensive search was performed in the databases: PubMed, Ebsco/SportDiscus, Ebsco/APA PsycINFO, Ebsco/ERIC, Ebsco/Criminal Justice Abstracts, Embase.com, and Clarivate Analytics/Web of Science Core Collection, from inception to June 28th, 2021, in collaboration with a medical information specialist (JCFK). The search included controlled terms and free text terms for synonyms of “exercise” or “sports” combined with synonyms of “aggression” or “antisocial” and “young adult” and “RCTs” or “SRs” or “cohort studies,” with the exclusion of “animal studies” or specific terms like “spectator aggression.” The search was performed without restrictions for date or language. The full search strategies can be found in Appendix B. Duplicate articles were excluded by a medical information specialist (JCFK) using Endnote X20.0.1 (Clarivatetm), following the Amsterdam Efficient Deduplication (AED)-method (Otten et al., 2019) and the Bramer-method (Bramer et al., 2016). This review is registered in the systematic review registry Prospero (registration number: CRD42020198123). We did not prepare a review protocol.
Selection criteria
The eligibility of included studies was assessed using the web-based program Rayyan (Ouzzani et al., 2016) with the following criteria: (a) participants from general or clinical populations; (b) the intervention involved any chronic physical activity intervention; (c) controls were either wait-list, no-exercise, or attention control groups; (d) outcome measures were related to antisocial behavior including self-report and observational measures; (e) the design permitted the computation of a reliable effect size, i.e., RCT or quasi-experimental design with a control group; (f) post-intervention outcome measures were obtainable; and (g) the study was published in English or Dutch or translations were obtainable. Animal studies were excluded, as were studies reporting only on the effect of acute exercise, studies including yoga or mindfulness as a measure of physical activity, studies including substance (ab)use and/or smoking as only outcome measure, and studies without a control sample. Grey literature, e.g., conference abstracts, posters, and theses, was searched and included if relevant. The first and second author screened all records (i.e., abstracts and full texts) for eligibility independently. Any discrepancies between the reviewers were resolved by a third author. In the case of missing data, the original authors were contacted.
Coding the data and potential moderators
Information on study design, sample characteristics, intervention characteristics, and outcome measures was coded by the first author and discussed with the second author to test possible moderators (Lipsey & Wilson, 2001). The study design was coded as RCT or quasi-experimental, since the latter may be more prone to bias and show larger effect sizes (MacLehose et al., 2000). In addition, the control group was coded as active (i.e., sedentary attention, receiving the same amount of interpersonal interaction without a physical activity intervention) or inactive (i.e., waitlist or no intervention), as this might influence the expected effect of the intervention (Spruit et al., 2016).
Regarding sample characteristics, the proportion of males (Fredricks & Eccles, 2008; Wong et al., 2013), mean age (Park et al., 2017), and sample type (Özer et al., 2012) were coded and included as possible moderators. Sample type was coded as students, clinical (i.e., receiving care, diagnosed by a clinician, or meeting criteria without a diagnosis), offenders, and other (i.e., sedentary students and university faculty (i.e., no regular physical activity in the preceding year as determined by the Leisure Time Physical Activity questionnaire), students with overweight (i.e., ≥ 85th percentile body mass index), students receiving special education, and students with a high risk of offending). Sedentary and overweight students were separated from the students’ category as these characteristics have previously been shown to have a positive association with antisocial behavior such as anger and aggression (Hasler et al., 2004; Malmir & Nedaee, 2019). Thus, as these students may show elevated levels of antisocial behavior at baseline, different treatment effects may be expected compared to students who are not sedentary or overweight. This also applies to the other two groups, i.e., students receiving special education (Dickson et al., 2005) and students identified with a high risk of offending (Spruit et al., 2018). Age and the proportion of males were scored continuously.
Several intervention characteristics were also coded, i.e., type of physical activity, duration, and frequency of the intervention. Type of physical activity was first coded as string, and later subdivided based on existing data in aerobic exercise, sports (e.g., swimming, volleyball, soccer), walking (including jogging and running), martial arts, and other types of physical activity (i.e., dancing, weightlifting, or mixed). It is expected that different types of physical activity elicit different treatment effects (Battaglia et al., 2015; Lubans et al., 2012). Additionally, the duration (in weeks) and frequency (minutes per week) of the intervention were coded, as these may influence the strength of the effect of physical activity interventions (Taylor et al., 2015). Lastly, the outcome measure was coded based on the data as problem behavior (i.e., general antisocial behavior including externalizing behavior), externalizing behavior (i.e., rule-breaking and aggressive behavior), disruptive classroom behavior (i.e., problematic behavior in a classroom setting, including disciplinary referrals), aggressive behavior, anger expression, and hostility.
The risk of bias was assessed with the risk of bias tool (RoB 2: Sterne et al., 2019). This tool addresses five domains: randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result. The risk of bias in these domains was estimated as low risk, some concerns, or high risk. The first author assessed the risk of bias. The results were then discussed with the second author. Any disagreements were solved with a third author. Results are summarized in Table 1.
Effect size calculation and analysis
Pre- and post-intervention means and standard deviations were extracted to calculate standardized mean differences (SMDs) and standardized errors using Hedges’ g statistic (Harrer et al., 2021; Hedges, 1981). No study reported the correlation coefficient (r) between pre- and post-treatment scores needed to calculate the effect size. We therefore conducted sensitivity analyses imputing different values for r (see Appendix C, Table C1). As the results were similar, we used an estimate of r = 0.7, as recommended by Rosenthal (1986). If a study reported multiple outcome measures, only the best-validated outcome measure was included. If all measures were similarly validated, the field’s most use was selected to calculate an effect size, to prevent violation of the assumption of independent effect sizes. All analyses were performed using R version 4.0.4. Effect sizes were calculated using the “escalc” function within the metafor package (Viechtbauer, 2010) and reported in Hedges’ g (Hedges, 1981). We also reported several measures of heterogeneity (I2, tau2, and the prediction interval) (Borenstein et al., 2017; IntHout et al., 2016). We queried the authors of 9 studies to obtain missing information. In total, 7 authors responded, of which 2 replied that the data could not be obtained. Thus, additional data was received for 5 studies. They were included in the meta-review.
Meta-regression and subgroup analyses were performed with the meta- (Balduzzi et al., 2019) and metafor-packages (Viechtbauer, 2010) using a random effects model (as between-study heterogeneity was expected). Heterogeneity was examined using I2 as the proportion of observed effects-variation due to true effects-variation, tau2 as the amount of heterogeneity in true effects, and the prediction interval as an estimation of the true effects in future studies (Borenstein et al., 2017; IntHout et al., 2016). A high I2 indicates non-homogenous effect sizes meaning moderators or outliers should be identified. In contrast, a low I2 may indicate homogenous effect sizes, with the I2 interval as an index for the level of certainty for this result (Borenstein et al., 2017). The Knapp and Hartung (Knapp & Hartung, 2003) adjustment was used to calculate the corresponding confidence intervals (Inthout et al., 2014; Langan et al., 2019). Furthermore, to detect the individual contribution of each study to the heterogeneity, Baujat plots were used (Baujat et al., 2002). Possible outliers were detected using the “find.outliers” function of the dmetar-package (Harrer et al., 2019), which identifies studies for which the upper bound of the 95% confidence interval is lower than the lower bound of the pooled effect confidence interval, or for which the lower bound of the interval is higher than the upper bound of the pooled effect confidence interval. Next, we performed sensitivity analyses, excluding these outliers, to examine the possible influence on effect size. Finally, publication bias (i.e., an overestimation of the true effect size due to the exclusion of unpublished studies with non-significant findings (Rosenthal, 1979)) was tested with funnel plot asymmetry according to Egger’s method (Egger et al., 1997) and the trim and fill plot (Duval & Tweedie, 2000) using the “trimmfill” function in the metafor-package (Viechtbauer, 2010). In the case of an asymmetrical funnel plot (indicating publication bias), the trim and fill procedure would correct this by imputing estimations of the missing effect sizes based on existing effect sizes. These estimations were then included in a new meta-analysis showing the influence of the missing effect sizes on the overall effect size.
Results
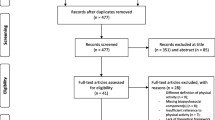
The search yielded 34,036 studies. After removing duplicates, 23,524 abstracts were screened, of which 162 studies were assessed for eligibility. No full-text was available for 33 articles, resulting in 129 full-text articles. After reading the full-text articles, 102 additional reports were excluded (see Fig. 1 for exclusion reasons). The two most common exclusion reasons were study design (n = 32), e.g., observational or case study; and no outcome measures related to antisocial behavior (n = 16), e.g., antisocial behavior was mentioned but not measured, or only measured at baseline. The current meta-analytic review consists of 29 studies, of which 20 reported on sufficient information to calculate effect sizes (6 studies did not report on post-treatment scores, and 3 additional studies did not report on pre-treatment scores). The flow chart of the selection process is visualized in Fig. 1 (Figure adapted from: Page et al., 2021).

Prisma flow diagram
Basic characteristics of studies
An overview of the basic characteristics can be found in Table 2. A total of k = 29 studies were included in the systematic review, of which k = 20 reported sufficient information to calculate effect size (3 studies only reported on post-treatment means). Thus, for the meta-analysis, we report on k = 20 studies that include N = 2250 participants. In total, n = 1209 participated in a physical activity intervention and n = 1041 served as the control group (of whom 1171 participants received no intervention or were placed on a waitlist and 32 participants received a sedentary-attention intervention). Eight studies included students from the general population (3 included elementary school students and 5 included high school students) and 6 studies included students receiving care (n = 1) or meeting criteria for a behavioral disorder (n = 5). One study reported on sedentary high school students and university faculty, one on low-level or special education students, one on high school students with overweight, and three studies reported on an offender population. Five interventions were aerobic-based exercises; 6 were (team) sports (e.g., soccer, swimming, volleyball); 2 included walking, jogging, or running; 3 were based on martial arts; 3 were mixed (i.e., martial arts and sports, strength and running, and exercises with resistance training); and 1 included weightlifting. The intervention duration ranged from 2.5 to 39 weeks with a frequency varying between multiple daily sessions and single weekly sessions. Included outcome measures were aggressive behavior (n = 7), externalizing behavior (n = 4), anger expression (n = 3), disruptive classroom behavior including disciplinary referrals (n = 2), hostile behavior, or a combination of externalizing, bullying, and other problematic behaviors (n = 2).
Of the remaining k = 9 studies not included in the meta-analysis, 6 described a significant positive effect of physical activity on antisocial behavior (Basile et al., 1995; Goldshtrom et al., 2011; Palermo et al., 2006; Pan, 2010; Yılmaz & Soyer, 2018; Zivin et al., 2001), and 3 studies could not find a significant effect (Bunketorp Käll et al., 2015; Carter et al., 2017; Welland et al., 2020). Of the studies reporting on a significant intervention effect, n = 4 included a clinical population (maltreated children (n = 1), children with a behavioral disorder (n = 2), boys with autism spectrum disorder (n = 1)), and n = 2 reported on other samples (children with mild intellectual disorder and boys at risk for antisocial behavior). The non-significant studies included elementary school students (n = 3), and offenders (n = 1). The type of physical activity in the significant studies was martial arts (n = 2), sports, i.e., swimming (n = 1), walking/jogging/running (n = 1), rhythmic exercises (n = 1), and mixed, i.e., balance and coordination play events (n = 1). For the non-significant studies, this included aerobic exercises (n = 2), and sports, i.e., rugby (n = 1). In the significant studies, 4 included measures of disruptive classroom behavior, one study included aggression, and one study included temperament. The non-significant studies examined externalizing behavior (n = 1), problem behavior (n = 1), and pro-criminal attitudes (n = 1).
Efficacy of physical activity
Pooled effect sizes were calculated with a random effects model (see Fig. 2 and Table 3). We found an overall significant small-to-medium effect (g = − 0.26), representing a reduction of antisocial behavior after physical activity interventions versus no physical activity intervention, waitlist, or attention-control. The trim-and-fill plot (Appendix C, Figure C1) and Egger’s test (intercept = 0.96, 95% CI = − 1.09; − 2.91, t = 0.89, p = 0.386) did not indicate publication bias. The substantial percentage of variability in effect sizes (I2 = 82.5) indicated possible moderators or outliers. Furthermore, the prediction interval ranged from g = − 1.18 to 0.66, indicating the effect of physical activity in future studies may be beneficial or not beneficial. Three outliers were detected: Harvey et al. (2018), Phung and Goldberg (2021), and Shachar et al. (2016). Results from the sensitivity analysis excluding these outliers are reported in Table 3. Removing these outliers resulted in moderate-substantial heterogeneity (I2 = 63.5) and small-to-medium effect size (g = − 0.24). The prediction interval ranged from g = − 1.17 to 0.70. Examination of the Baujat plot (Appendix C, Figure C2) identified Shachar et al. as adding substantially to the heterogeneity as well as highly influencing effect size, possible due to the large N. A second sensitivity analysis was performed removing only Shachar et al., see Table 3. This reduced the effect size slightly (g = − 0.23) with a prediction interval ranging from g − 1.17 to 0.70. A forest plot was created excluding all outliers (Harvey et al., 2018; Phung & Goldberg, 2021; and Shachar et al., 2016), see Appendix C, Figure C3.

Forest plot of main analysis weighed by study n and ordered by effect size
Due to the expected small sample size, we included studies where physical activity was the main treatment, but a significantly smaller part included non-physical activity treatment. Specifically, Hilyer et al. (1982) included 10–15 min counseling mostly related to fitness and health, Phung and Goldberg (2021) included a 5-min bowing and mindfulness exercise, and Wade et al. (2018) included 3 × 20 min interactive seminars on screen time. To examine if this influenced our effect size, a third sensitivity analysis was performed excluding these three studies. Removing these studies did not result in large deviations, as shown in Table 3 (g = − 0.22 with a prediction interval ranging from g − 1.08 to 0.64).
Lastly, because three studies only reported on post-treatment means, we ran a supplementary analysis using post-treatment scores without correction for pre-treatment scores. Results are similar, with k = 23, g = − 0.27, p = 0.02, and a prediction interval ranging from g − 1.18 to 0.66 (see Appendix C, Table C2).
Moderator analysis
Nine moderator analyses were performed (Table 4). Due to small subgroups and overlapping constructs, we combined problem behavior with externalizing behavior and anger expression with hostility. Significant moderating effects were found for type of control group, type of physical activity intervention, and type of antisocial outcome. Specifically, we found a larger effect of physical activity interventions (g = − 0.31, k = 18) compared to control groups that did not receive any intervention, but no significant effect (g = 0.25, k = 2) compared to sedentary attention or other types of interventions not containing elements of physical activity (e.g., psychosocial treatment). Furthermore, we found a significant moderating effect of type of physical activity, with larger effects for interventions containing walking, jogging, or running (g = − 0.87, k = 3) but non-significant effects for aerobic exercise (g = 0.05, k = 5), sports (g = − 0.04, k = 6), martial arts (g = − 0.713, k = 3), or other types of physical activity (e.g., weightlifting or dancing; g = − 0.33, k = 3). Lastly, we found a larger effect size on anger and/or hostility as an antisocial outcome (g = − 0.42, k = 5), but no significant effect on other types of antisocial behavior, i.e., aggressive behavior (g = − 0.21, k = 7), problem and/or externalizing behavior (g = − 0.48, k = 6), and disruptive classroom behavior (g = 0.45, k = 2). Study design, sample characteristics (age, proportion male, sample type), intervention frequency (in weeks), and intervention duration (in weeks) did not significantly moderate the effect of physical activity on antisocial behavior. Caution is advised interpreting these results, due to the limited amount of studies in some of the comparison groups (i.e., active control groups and interventions containing walking, jogging, and/or running).
Risk of bias
The Cochrane risk of bias tool was used to assess the risk of bias in several domains (Sterne et al., 2019). Table 1 summarizes the results. As this tool is designed for RCTs, studies with a quasi-experimental design will always be classified as having at least some concerns. The current meta included 5 studies with a quasi-experimental design, of which 2 studies were judged as having a high risk of bias as it was unclear if they adopted adequate matching procedures in an attempt to decrease the risk of bias. Regarding deviations from intended interventions, the lack of published trial protocols hampered assessment and introduced bias in most studies. Missing outcome data was a problem for 11 studies, of which 1 study raised some concerns and 10 studies were assessed as having a high risk of bias. This was due to an unclear description of handling the missing data (e.g., controlling for possible bias, sensitivity analysis). All studies were judged to have some concerns related to the measurement of the outcome. This was the result of questionnaires with mostly non-blinded outcome assessors (i.e., self-report (n = 9), parents (n = 6), teachers (n = 3), or outcome assessors with unclear blinding (i.e., trained researchers (n = 1)). Knowledge of the intervention could have influenced their answers on the questionnaires, although this risk was assessed as unlikely (as the assessors would not gain any benefit from this). Information on analysis intentions was judged as not available in all studies, resulting in some concerns related to the selection of the reported result for all included studies.
Discussion
The current meta-analytic review assessed the effects of physical activity interventions on several measures of antisocial behavior (i.e., aggression, externalizing behavior, delinquency, hostility, and anger) in children and adults. Overall, we found a significant effect size (g = − 0.26) in favor of physical activity, indicating physical activity interventions can improve antisocial behavior. More specifically, the negative effect size implies on average antisocial behavior is decreased in participants receiving physical activity compared to participants not receiving this intervention (e.g., waitlist or sedentary attention controls). A note of caution is due here since the estimated range of effect sizes of future studies includes both positive and negative effect sizes (prediction interval ranging from g = − 1.18 to 0.66). Thus, although our current results suggest a beneficial intervention effect, future studies might find less positive or even detrimental effects. In addition, the substantial heterogeneity indicates the need for more univariate measures of antisocial behavior, although removing three possible outliers resulted in moderate-substantial heterogeneity.
Our findings are partially consistent with previous meta-analyses in youth. Physical activity has previously been shown to be similarly effective (d = 0.32) in reducing antisocial behavior (i.e., aggression, delinquency, or other conduct problems) in adolescents (Spruit et al., 2016). In contrast, larger effect sizes (d = 0.65) were found in a review only including martial arts as a physical activity, indicating a significant reduction in aggression in youth (Harwood et al., 2017). This may be due to the mindfulness components common to martial arts (Miyata et al., 2020), as mindfulness can effectively reduce antisocial behavior (Gillions et al., 2019; Tao et al., 2021), possibly through decreased rumination (Borders et al., 2010) and increased compassion (Lim et al., 2015). In our study, we did not find martial arts to be a significant moderator, yet caution is advised as we only included three studies with this type of activity (Delva-Tauiliili, 1995; Greco & de Ronzi, 2020; Phung & Goldberg, 2021). Thus, it is possible that interventions containing martial arts may result in larger reductions in antisocial behavior, but further research is needed to test this.
To the authors’ knowledge, in adults, no meta-analytic review exists on the effect of physical activity on antisocial behavior, yet related externalizing behavior (i.e., substance abuse (Wang et al., 2014)) has been investigated. Physical activity interventions including mindfulness (e.g., martial arts or yoga) significantly reduced withdrawal symptoms (d = − 1.24) and increased abstinent rate (odds ratio = 1.69) in adult substance abusers (Wang et al., 2014). As in our meta-analysis, the authors did not find a moderating effect of the type of activity (aerobic versus mind–body). However, it should be noted that even though 30% of the included studies had mindfulness components, their comparisons contained only 3 and 2 studies in the mind–body subgroup for withdrawal symptoms and abstinence rate, respectively. Therefore, it is not possible to completely rule out the effects of mindfulness (Auty et al., 2017). In sum, there is evidence indicating that physical activity interventions (possibly with mindfulness) can be effective in the reduction of substance abuse in adults, yet comparison with our current results is complicated due to the possible interfering effect of mindfulness.
Similar to our findings, a recent meta-review found a moderate positive effect of sports programs (excluding martial arts programs and outdoor or adventure activities, but including yoga) on criminal behavior (e.g., reconviction, drug use, anger, self-control, and impulsivity) in favor of the sports programs (d = 0.36) in a sample containing both children and adults (Jugl et al., 2021). In line with our results, the authors could not find significant moderating effects for study design or sample characteristics. To our current knowledge, they did not examine any possible moderating effect for the type of control group or intervention duration and frequency. Jugl and colleagues could not find an effect of the type of physical activity but only looked at teams sports versus individual versus combined sports, complicating the comparison with our categorization. Somewhat surprisingly (due to the heterogeneous nature of their outcome measures), they also did not include the type of outcome measure as a possible moderator. Despite these discrepancies, their results taken together with our findings indicate physical activity including sports programs can be beneficial (with a moderate effect) for both children and adults in the treatment and/or prevention of several measures of antisocial behavior.
In addition, we explored if the effect of physical activity on antisocial behavior was moderated by study design, sample characteristics, intervention characteristics, or outcome. Larger effect sizes were found for comparisons with controls not receiving any treatment compared to controls receiving a sedentary-attention treatment. This could indicate that the effect of physical activity may be partially explained by the attention received and interpersonal interactions (LaFave et al., 2019), but due to the small number of studies using a sedentary-attention control condition (k = 2), it is not possible to further interpret these results. Larger effects were also found for interventions containing walking, jogging, or running, yet no significant effects were found for other types of physical activity such as aerobic exercises or sports. Speculatively, this may be related to how difficult it is to master certain activities. It can be argued that compared to other types of activity (such as basketball or martial arts), walking, jogging, and running are easy to master, requiring no additional skill set or high cognitive control. As previous studies show robust associations between antisocial behavior and cognitive control deficits (Ogilvie et al., 2011) including high impulsivity (Gordon & Egan, 2011) and low self-control (DeLisi & Vaughn, 2011), it is possible that other types of activity are too demanding for participants to benefit from the positive behavioral effects. Lastly, we found a larger effect on anger and hostility as a measure of antisocial outcome versus other types of antisocial behavior (e.g., externalizing behavior or aggression). Hostility and anger may be classified as more emotion-driven behavior (Tsikandilakis et al., 2020) compared to other antisocial constructs (which may be expressions of more learned behavior (Bandura, 1973)). The effect of physical activity on anger and hostility might be the result of enhanced emotion regulation. This hypothesis is supported by (limited) existing research in clinical populations such as those suffering from multiple sclerosis (Bahmani et al., 2020) or children diagnosed with autism spectrum disorder (Tse, 2020). Although preliminary, these results indicate several important factors to address in future research to optimize the potential positive effects of physical activity interventions. To further examine their potential moderating effects, future research should include different types of control groups, measurements related to motivation, and differentiate between emotion-driven and acquired antisocial behavior.
Several limitations need to be acknowledged. First, none of the studies controlled for recreational physical activity during the intervention, which may have influenced treatment effects. However, these effects may be minimal due to the random assignment of treatments and comparison groups in 15 studies, and the instructions to continue normal physical activity during the intervention period in the other studies. Second, as only three studies reported on an adult sample, the generalizability to adults is limited, indicating the need for more (quasi-) experimental studies on adults. Third, antisocial outcomes were measured with a wide variety of instruments, which likely contributes to the high heterogeneity in the analysis. Lastly, the included studies were generally assessed as having a high risk of bias, complicating interpretations.
To summarize, these results demonstrate a negative effect size in favor of physical activity interventions in the reduction of several types of antisocial behavior. As physical activity is inexpensive and easy to administer, it may serve as a cost-effective treatment to improve multiple antisocial behaviors. However, due to the overall high risk of bias in the included studies and the level of variation in estimated future treatment effects, more sound evaluation research is needed to better understand the functioning and to improve the possible implementation of physical activity interventions. Future studies should differentiate between the types of the control group, types of physical activity, and underlying causes of antisocial behavior, as these may significantly affect treatment outcome.
Data availability
The datasets generated during and analyzed during the current study are available from the corresponding author on reasonable request and with the permission of VU Amsterdam.
References
References marked with an asterisk indicate studies included in the meta-analysis
American Psychiatric Association. (2022). Diagnostic and statistical manual of medical disorders (DSM-5) (5th ed.). Boom uitgevers Amsterdam. https://doi.org/10.1176/appi.books.9780890425787
Auty, K. M., Cope, A., & Liebling, A. (2017). A systematic review and meta-analysis of yoga and mindfulness meditation in prison: Effects on psychological well-being and behavioral functioning. International Journal of Offender Therapy and Comparative Criminology, 61(6), 689–710. https://doi.org/10.1177/0306624X15602514
Bahmani, D. S., Razazian, N., Motl, R. W., Farnia, V., Alikhani, M., Pühse, U., ... & Brand, S. (2020). Physical activity interventions can improve emotion regulation and dimensions of empathy in persons with multiple sclerosis: An exploratory study. Multiple sclerosis and related disorders, 37, 101380.
Balduzzi, S., Rücker, G., & Schwarzer, G. (2019). How to perform a meta-analysis with R: A practical tutorial. Evidence-Based Mental Health, 22(4), 153–160.
Bandura, A. (1973). Aggression: A social learning analysis. prentice-hall
Basile, V. C., Motta, R. W., & Allison, D. B. (1995). Antecedent exercise as a treatment for disruptive behavior: Testing hypothesized mechanisms of action. Behavioral Interventions, 10(3), 119–140.
Battaglia, C., Di Cagno, A., Fiorilli, G., Giombini, A., Borrione, P., Baralla, F., Marchetti, M., & Pigozzi, F. (2015). Participation in a 9-month selected physical exercise programme enhances psychological well-being in a prison population. Criminal Behaviour and Mental Health, 25(5), 343–354. https://doi.org/10.1002/cbm.1922
Baujat, B., Mahé, C., Pignon, J. P., & Hill, C. (2002). A graphical method for exploring heterogeneity in meta-analyses: Application to a meta-analysis of 65 trials. Statistics in Medicine, 21(18), 2641–2652. https://doi.org/10.1002/sim.1221
Bennett, D. S., & Gibbons, T. A. (2000). Efficacy of child cognitive-behavioral interventions for antisocial behavior: A meta-analysis. Child & Family Behavior Therapy, 22(1), 1–15.
Boat, R., & Cooper, S. B. (2019). Self-control and exercise: A review of the bi-directional relationship. Brain Plasticity, 5(1), 97–104. https://doi.org/10.3233/bpl-190082
Borders, A., Earleywine, M., & Jajodia, A. (2010). Could mindfulness decrease anger, hostility, and aggression by decreasing rumination? AGGRESSIVE BEHAVIOR, 36, 28–44. https://doi.org/10.1002/ab.20327
Borenstein, M., Higgins, J. P. T., Hedges, L. V., & Rothstein, H. R. (2017). Basics of meta-analysis: I2 is not an absolute measure of heterogeneity. Research Synthesis Methods, 8(1), 5–18. https://doi.org/10.1002/jrsm.1230
Bowker, A. (2006). The relationship between sports participation and self-esteem during early adolescence. Canadian Journal of Behavioural Science, 38(3), 214–229. https://doi.org/10.1037/cjbs2006009
Bramer, W. M., Giustini, D., de Jong, G. B., Holland, L., & Bekhuis, T. (2016). De-duplication of database search results for systematic reviews in EndNote. Journal of the Medical Library Association : JMLA, 104(3), 240. https://doi.org/10.3163/1536-5050.104.3.014
Bunketorp Käll, L., Malmgren, H., Olsson, E., Lindén, T., & Nilsson, M. (2015). Effects of a curricular physical activity intervention on children’s school performance, wellness, and brain development. Journal of school health, 85(10), 704–713.
*Bustamante, E. E., Davis, C. L., Frazier, S. L., Rusch, D., Fogg, L. F., Atkins, M. S., & Marquez, D. X. (2016). Randomized controlled trial of exercise for ADHD and disruptive behavior disorders. Medicine and science in sports and exercise, 48(7), 1397
Carter, J. S., Karczewski, S., Decator, D. D., & Hollowell, A. A. M. (2017). Ethnic differences in impact of physical activity program on psychological symptoms in youth. Journal of Physical Activity and Health, 14(4), 283–289. https://doi.org/10.1123/JPAH.2016-0450
Caspersen, C. J., Powell, K. E., & Christenson, G. M. (1985). Physical activity, exercise, and physical fitness: Definitions and distinctions for health-related research. Public Health Reports, 100(2), 126–131.
Chang, Y. K., Labban, J. D., Gapin, J. I., & Etnier, J. L. (2012). The effects of acute exercise on cognitive performance: A meta-analysis. In Brain Research, 1453, 87–101. https://doi.org/10.1016/j.brainres.2012.02.068
Cohen, J. (1988). Statistical power analysis for the behavioral sciences (2nd ed.). Lawrence Erlbaum Associates.
Cohen, M. A., & Piquero, A. R. (2009). New evidence on the monetary value of saving a high risk youth. Journal of Quantitative Criminology, 25(1), 25–49. https://doi.org/10.1007/s10940-008-9057-3
Cuijpers, P., Weitz, E., Cristea, I. A., & Twisk, J. (2017). Pre-post effect sizes should be avoided in meta-analyses. Epidemiology and Psychiatric Sciences, 26(4), 364–368. https://doi.org/10.1017/S2045796016000809
Daskalopoulou, C., Stubbs, B., Kralj, C., Koukounari, A., Prince, M., & Prina, A. M. (2017). Physical activity and healthy ageing: A systematic review and meta-analysis of longitudinal cohort studies. Ageing Research Reviews, 38, 6–17. https://doi.org/10.1016/j.arr.2017.06.003
DeLisi, M., & Vaughn, M. G. (2011). The importance of neuropsychological deficits relating to self-control and temperament to the prevention of serious antisocial behavior. International Journal of Child, Youth and Family Studies, 2(1/2), 12–35. https://doi.org/10.18357/ijcyfs21/220115425
*Delva-Tauiliili, J. (1995). Does brief Aikido training reduce aggression of youth? Perceptual and Motor Skills, 80(1), 297–298. https://doi.org/10.2466/pms.1995.80.1.297
Dickson, K., Emerson, E., & Hatton, C. (2005). Self-reported anti-social behaviour: Prevalence and risk factors amongst adolescents with and without intellectual disability. Journal of Intellectual Disability Research, 49(11), 820–826.
Dodge, K. A. N., & McCourt, S. (2010). Translating models of antisocial behavioral development into efficacious intervention policy to prevent adolescent violence. Developmental Psychobiology: The Journal of the International Society for Developmental Psychobiology, 52(3), 277–285.
Duval, S., & Tweedie, R. (2000). Trim and fill: A simple funnel-plot-based method of testing and adjusting for publication bias in meta-analysis. Biometrics, 56(2), 455–463. https://doi.org/10.1111/j.0006-341X.2000.00455.x
Egger, M., Smith, G. D., Schneider, M., & Minder, C. (1997). Bias in meta-analysis detected by a simple, graphical test. British Medical Journal, 315(7109), 629–634. https://doi.org/10.1136/bmj.315.7109.629
Ekholm, D., Nygren, L., Michailakis, D., Dahlstedt, M., & Sjöblom, Y. (2013). Research on sport as a means of crime prevention in a Swedish welfare context : A literature review. Scandinavian Sport Studies Forum, 4(4), 91–120.
Fazel, S., & Wolf, A. (2015). A systematic review of criminal recidivism rates worldwide: Current difficulties and recommendations for best practice. PLOS ONE, 10(6), e0130390. https://doi.org/10.1371/journal.pone.0130390
Fredricks, J. A., & Eccles, J. S. (2008). Participation in extracurricular activities in the middle school years: Are there developmental benefits for African American and European American Youth? Journal of Youth and Adolescence, 37(9), 1029–1043. https://doi.org/10.1007/s10964-008-9309-4
Frick, P. J. (2016). Early identification and treatment of antisocial behavior. In Pediatric Clinics of North America, 63(5), 861–871. https://doi.org/10.1016/j.pcl.2016.06.008
Gillions, A., Cheang, R., & Duarte, R. (2019). The effect of mindfulness practice on aggression and violence levels in adults: A systematic review. In Aggression and Violent Behavior, 48, 104–115. https://doi.org/10.1016/j.avb.2019.08.012
Goldshtrom, Y., Korman, D., Goldshtrom, I., & Bendavid, J. (2011). The effect of rhythmic exercises on cognition and behaviour of maltreated children: A pilot study. Journal of bodywork and movement therapies, 15(3), 326–334.
Gordon, V., & Egan, V. (2011). What self-report impulsivity measure best postdicts criminal convictions and prison breaches of discipline? Psychology, Crime & Law, 17(4), 305–318. https://doi.org/10.1080/10683160903203946
*Greco, G., & de Ronzi, R. (2020). Effect of karate training on social, emotional, and executive functioning in children with autism spectrum disorder. Journal of Physical Education and Sport ® (JPES), 20(4), 1637–1645. https://doi.org/10.7752/jpes.2020.04223
Guiney, H., & Machado, L. (2013). Benefits of regular aerobic exercise for executive functioning in healthy populations. Psychonomic Bulletin and Review, 20(1), 73–86. https://doi.org/10.3758/s13423-012-0345-4
Harrer, M., Cuijpers, P., Furukawa, T. & Ebert, D. D. (2019). dmetar: Companion R package for the guide ‘doing meta-analysis in R’. R package version 0.0.9000. URL http://dmetar.protectlab.org/
Harrer, M., Cuijpers, P., Furukawa, T. A., & Ebert, D. D. (2021). Doing meta-analysis with R. Chapman and Hall/CRC. https://doi.org/10.1201/9781003107347
Hartmann, D., & Depro, D. (2006). Rethinking sports-based community crime prevention: A preliminary analysis of the relationship between midnight basketball and urban crime rates. Journal of Sport and Social Issues, 30(2), 180–196. https://doi.org/10.1177/0193723506286863
*Harvey, S. P., Lambourne, K., Greene, J. L., Gibson, C. A., Lee, J., & Donnelly, J. E. (2018). The effects of physical activity on learning behaviors in elementary school children: A randomized controlled trial. Contemporary School Psychology, 22(3), 303-312
Harwood, A., Lavidor, M., & Rassovsky, Y. (2017). Reducing aggression with martial arts: A meta-analysis of child and youth studies. Aggression and Violent Behavior, 34, 96–101. https://doi.org/10.1016/j.avb.2017.03.001
Hasler, G., Pine, D. S., Gamma, A., Milos, G., Ajdacic, V., Eich, D., ... & Angst, J. (2004). The associations between psychopathology and being overweight: A 20-year prospective study. Psychological medicine, 34(6), 1047-1057
Heap, V. (2021). Exploring the effects of long-term anti-social behavior victimization. International Review of Victimology, 27(2), 227–242. https://doi.org/10.1177/0269758020961979
Hedges, L. V. (1981). Distribution theory for Glass’s estimator of effect size and related estimators. Journal of Educational Statistics, 6, 107–128.
Higgins, J. P. T., & Thompson, S. G. (2002). Quantifying heterogeneity in a meta-analysis. Statistics in Medicine, 21(11), 1539–1558. https://doi.org/10.1002/sim.1186
*Hilyer, J. C., Wilson, D. G., Dillon, C., Caro, L., Jenkins, C., Spencer, W. A., ... & Booker, W. (1982). Physical fitness training and counseling as treatment for youthful offenders. Journal of Counseling Psychology, 29(3), 292
Hofer, S. M., & Piccinin, A. M. (2009). Integrative data analysis through coordination of measurement and analysis protocol across independent longitudinal studies. Psychological Methods, 14(2), 150–164. https://doi.org/10.1037/a0015566
*Hughes, J. R., Casal, D. C., & Leon, A. S. (1986). Psychological effects of exercise: A randomized cross-over trial. Journal of Psychosomatic Research, 30(3), 355-360
IntHout, J., Ioannidis, J. P. A., Rovers, M. M., & Goeman, J. J. (2016). Plea for routinely presenting prediction intervals in meta-analysis. British Medical Journal Open, 6(7), e010247. https://doi.org/10.1136/BMJOPEN-2015-010247
Inthout, J., Ioannidis, J. P., & Borm, G. F. (2014). The Hartung-Knapp-Sidik-Jonkman method for random effects meta-analysis is straightforward and considerably outperforms the standard DerSimonian-Laird method. BMC Medical Research Methodology, 14(1), 1–12. https://doi.org/10.1186/1471-2288-14-25
Jones-Palm, D. H., & Palm, J. (2005). Physical activity and its impact on behavior among youth. World Health Organization, 1–5
Jugl, I., Bender, D., & Lösel, F. (2021). Do sports programs prevent crime and reduce reoffending? A systematic review and meta-analysis on the effectiveness of sports programs. Journal of Quantitative Criminology, 1–52. https://doi.org/10.1007/s10940-021-09536-3
Kelly, L. (2013). Sports-based interventions and the local governance of youth crime and antisocial behavior. Journal of Sport and Social Issues, 37(3), 261–283. https://doi.org/10.1177/0193723512467193
Knapp, G., & Hartung, J. (2003). Improved tests for a random effects meta-regression with a single covariate. Statistics in Medicine, 22(17), 2693–2710. https://doi.org/10.1002/sim.1482
LaFave, S. E., Granbom, M., Cudjoe, T. K. M., Gottsch, A., Shorb, G., & Szanton, S. L. (2019). Attention control group activities and perceived benefit in a trial of a behavioral intervention for older adults. Research in Nursing and Health, 42(6), 476–482. https://doi.org/10.1002/NUR.21992
Langan, D., Higgins, J. P. T., Jackson, D., Bowden, J., Veroniki, A. A., Kontopantelis, E., Viechtbauer, W., & Simmonds, M. (2019). A comparison of heterogeneity variance estimators in simulated random-effects meta-analyses. Research Synthesis Methods, 10(1), 83–98. https://doi.org/10.1002/jrsm.1316
Lim, D., Condon, P., & de Steno, D. (2015). Mindfulness and compassion: An examination of mechanism and scalability. PLoS ONE, 10(2), e0118221. https://doi.org/10.1371/JOURNAL.PONE.0118221
Lipsey, M. W., & Wilson, D. B. (2001). Practical meta-analysis. Sage Publications.
Lipsey, M. W., & Cullen, F. T. (2007). The effectiveness of correctional rehabilitation: A review of systematic reviews. Annual Review of Law and Social Science, 3(1), 297–320. https://doi.org/10.1146/annurev.lawsocsci.3.081806.112833
Liu, M., Wu, L., & Ming, Q. (2015). How does physical activity intervention improve self-esteem and self-concept in children and adolescents? Evidence from a Meta-Analysis. PlOS ONE, 10(8), e0134804. https://doi.org/10.1371/journal.pone.0134804
Lubans, D. R., Plotnikoff, R. C., & Lubans, N. J. (2012). Review: A systematic review of the impact of physical activity programmes on social and emotional well-being in at-risk youth. In Child and Adolescent Mental Health, 17(1), 2–13. https://doi.org/10.1111/j.1475-3588.2011.00623.x
Lüdecke, D. (2019). esc: Effect size computation for Meta Analysis (Version 0.5.1).10.5281/zenodo.1249218, https://CRAN.R-project.org/package=esc
MacLehose, R. R., Reeves, B. C., Harvey, I. M., Sheldon, T. A., Russell, I. T., & Black, A. M. S. (2000). A systematic review of comparisons of effect sizes derived from randomized and non-randomized studies. Health Technology Assessment (Winchester, England), 4(34), 1–154. https://doi.org/10.3310/hta4340
Morris, L., Sallybanks, J., Willis, K., & Makkai, T. (2004). Sport, physical activity and antisocial behaviour in youth. Youth Studies Australia, 23(1), 47–52.
Malmir, R., & Nedaee, T. (2019). The relationship between anger control and physical activity. Health, 21(4), 284–291.
Meek, R. (2018). A sporting chance. An independent review of sport in youth and adult prisons. In Ministry of Justice (Issue 333)
Miyata, H., Kobayashi, D., Sonoda, A., Motoike, H., & Akatsuka, S. (2020). Mindfulness and psychological health in practitioners of Japanese martial arts: A cross-sectional study. BMC Sports Science, Medicine and Rehabilitation, 12(1), 1–10. https://doi.org/10.1186/s13102-020-00225-5
Moffitt, T. E. (2013). Adolescence-limited and life-course-persistent antisocial behavior: A developmental taxonomy. The Science of Mental Health, 7, 90–117. https://doi.org/10.4324/9781315096278-3
Nelson, M., Specian, V. L., Tracy, N. C., & Demello, J. J. (2006). The effects of moderate physical activity on offenders in a rehabilitative program. The Journal of Correctional Education, 57(4), 276–285.
Nichols, G. (2010). Sport and crime reduction. Routledge. https://doi.org/10.4324/9780203089156
*Norris, R., Carroll, D., & Cochrane, R. (1992). The effects of physical activity and exercise training on psychological stress and well-being in an adolescent population. Journal of psychosomatic research, 36(1), 55–65
Ogilvie, J. M., Stewart, A. L., Chan, R. C. K., & Shum, D. H. K. (2011). Neuropsychological measures of executive function and antisocial behavior: A meta-analysis. Criminology, 49(4), 1063–1107. https://doi.org/10.1111/j.1745-9125.2011.00252.x
Otten, R., Vries, R. de, & Schoonmade, L. (2019). Amsterdam Efficient Deduplication (AED) method. https://doi.org/10.5281/ZENODO.3582928
Ouzzani, M., Hammady, H., Fedorowicz, Z., & Elmagarmid, A. (2016). Rayyan-a web and mobile app for systematic reviews. Systematic Reviews, 5(1), 1–10. https://doi.org/10.1186/S13643-016-0384-4/FIGURES/6
*Özer, D., Nalbant, S., Aktop, A., Duman, Ö., Keleş, I., & Toraman, N. F. (2007). Swimming training program for children with cerebral palsy: Body perceptions, problem behaviour, and competence. Perceptual and motor skills, 105(3), 777–787
*Özer, D., Baran, F., Aktop, A., Nalbant, S., Aĝlamiş, E., & Hutzler, Y. (2012). Effects of a Special Olympics Unified Sports soccer program on psycho-social attributes of youth with and without intellectual disability. Research in Developmental Disabilities, 33(1), 229–239. https://doi.org/10.1016/j.ridd.2011.09.011
Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., ... & Moher, D. (2021). The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Systematic reviews, 10(1), 1–11. https://doi.org/10.1136/BMJ.N71
Palermo, M. T., di Luigi, M., Dal Forno, G., Dominici, C., Vicomandi, D., Sambucioni, A., Proietti, L., & Pasqualetti, P. (2006). Externalizing and oppositional behaviors and karate-do: The way of crime prevention A pilot study. International Journal of Offender Therapy and Comparative Criminology, 50(6), 654–660. https://doi.org/10.1177/0306624X06293522
Paluska, S. A., & Schwenk, T. L. (2000). Physical activity and mental health: Current concepts. Sports Medicine, 29(3), 167–180. https://doi.org/10.2165/00007256-200029030-00003
Pan, C. Y. (2010). Effects of water exercise swimming program on aquatic skills and social behaviors in children with autism spectrum disorders. Autism, 14(1), 9–28. https://doi.org/10.1177/1362361309339496
Park, S., Chiu, W., & Won, D. (2017). Effects of physical education, extracurricular sports activities, and leisure satisfaction on adolescent aggressive behavior: A latent growth modeling approach. PLOS ONE, 12(4), e0174674. https://doi.org/10.1371/journal.pone.0174674
Perks, T. (2007). Does sport foster social capital? The contribution of sport to a lifestyle of community participation. Sociology of Sport Journal, 24(4), 378–401. https://doi.org/10.1123/ssj.24.4.378
*Phung, J. N., & Goldberg, W. A. (2021). Mixed martial arts training improves social skills and lessens problem behaviors in boys with Autism Spectrum Disorder. Research in Autism Spectrum Disorders, 83, 101758. https://doi.org/10.1016/J.RASD.2021.101758
Popovici, I., French, M. T., Pacula, R. L., Maclean, J. C., & Antonaccio, O. (2014). Cannabis use and antisocial behavior among youth. Sociological Inquiry, 84(1), 131–162. https://doi.org/10.1111/soin.12027
Reid, W. H., & Gacono, C. (2000). Treatment of antisocial personality, psychopathy, and other characterologic antisocial syndromes. Behavioral Sciences & the Law, 18(5), 647–662.
*Ramer, J. D., Santiago-Rodríguez, M. E., Davis, C. L., Marquez, D. X., Frazier, S. L., & Bustamante, E. E. (2020). Exercise and academic performance among children with attention-deficit hyperactivity disorder and disruptive behavior disorders: A randomized controlled trial. Pediatric exercise science, 32(3), 140–149
Rosenthal, R. (1979). The file drawer problem and tolerance for null results. Psychological Bulletin, 86(3), 638–641. https://doi.org/10.1037/0033-2909.86.3.638
Rosenthal, R. (1986). Meta-Analytic Procedures for Social Science Research. Sage Publications: Beverly Hills, 1984, 148 pp. Educational Researcher, 15(8), 18–20.
Rubin, J., Rabinovich, L., Hallsworth, M., & Nason, E. (2006). Interventions to reduce anti-social behaviour and crime. RAND Corporation.
Shachar, K., Ronen-Rosenbaum, T., Rosenbaum, M., Orkibi, H., & Hamama, L. (2016). Reducing child aggression through sports intervention: The role of self-control skills and emotions. Children and Youth Services Review, 71, 241–249.
Spruit, A., Assink, M., van Vugt, E., van der Put, C., & Stams, G. J. (2016). The effects of physical activity interventions on psychosocial outcomes in adolescents: A meta-analytic review. Clinical Psychology Review, 45, 56–71. https://doi.org/10.1016/j.cpr.2016.03.006
*Spruit, A., Hoffenaar, P., van der Put, C., van Vugt, E., & Stams, G. J. (2018). The effect of a sport-based intervention to prevent juvenile delinquency in at-risk adolescents. Children and Youth Services Review, 94, 689–698.
Sterne, J. A. C., Savović, J., Page, M. J., Elbers, R. G., Blencowe, N. S., Boutron, I., Cates, C. J., Cheng, H. Y., Corbett, M. S., Eldridge, S. M., Emberson, J. R., & Higgins, J. P. T. (2019). R.B 2: A revised tool for assessing risk of bias in randomized trials. British Medical Journal, 366, 14898
Tao, S., Li, J., Zhang, M., Zheng, P., Lau, E. Y. H., Sun, J., & Zhu, Y. (2021). The effects of mindfulness-based interventions on child and adolescent aggression: A systematic review and meta-analysis. Mindfulness, 12(6), 1301–1315. https://doi.org/10.1007/S12671-020-01570-9
*Tkacz, J., Young-Hyman, D., Boyle, C. A., & Davis, C. L. (2008). Aerobic exercise program reduces anger expression among overweight children. Pediatric Exercise Science, 20(4), 390
Taylor, P., Davies, L., Wells, P., Gilbertson, J., Tayleur, W., Christy, E., Cooley, E., Taylor, A., Jones, R., & Dumas, V. (2015). A review of the social impacts of culture and sport.
*Trajković, N., Madić, D., Milanović, Z., Mačak, D., Padulo, J., Krustrup, P., & Chamari, K. (2020a). Eight months of school-based soccer improves physical fitness and reduces aggression in high-school children. Biology of sport, 37(2), 185-193
*Trajkovic, N., Pajek, M., Sporis, G., Petrinovic, L., & Bogataj, S. (2020b). Reducing aggression and improving physical fitness in adolescents through an after-school volleyball program. Frontiers in Psychology, 11, 2081. https://doi.org/10.3389/fpsyg.2020.02081
*Tse, A. C. (2020). Brief report: Impact of a physical exercise intervention on emotion regulation and behavioral functioning in children with autism spectrum disorder. Journal of autism and developmental disorders, 50(11), 4191-4198
Tsikandilakis, M., Bali, P., Derrfuss, J., & Chapman, P. (2020). Anger and hostility: Are they different? An analytical exploration of facial-expressive differences, and physiological and facial-emotional responses. Cognition and Emotion, 34(3), 581–595. https://doi.org/10.1080/02699931.2019.1664415
van der Put, C. E., Asscher, J. J., & Stams, G. J. J. (2016). Differences between juvenile offenders with and without AD(H)D in recidivism rates and risk and protective factors for recidivism. Journal of Attention Disorders, 20(5), 445–457. https://doi.org/10.1177/1087054712466140
Viechtbauer, W. (2010). Conducting meta-analyses in R with the metafor. Journal of Statistical Software, 36(3), 1–48. https://doi.org/10.18637/jss.v036.i03
Wade, L., Smith, J. J., Duncan, M. J., & Lubans, D. R. (2018). Mediators of aggression in a school-based physical activity intervention for low-income adolescent boys. Mental Health and Physical Activity, 14, 39–46.
*Wagner, M., McBride, R. E., & Crouse, S. F. (1999). The effects of weight-training exercise on aggression variables in adult male inmates. The Prison Journal, 79(1), 72-89
Wang, D., Wang, Y., Wang, Y., Li, R., & Zhou, C. (2014). Impact of physical exercise on substance use disorders: A meta-analysis. PLOS ONE, 9(10), e110728. https://doi.org/10.1371/journal.pone.0110728
Welland, S., Duffy, L. J., & Baluch, B. (2020). Rugby as a rehabilitation program in a United Kingdom male young offenders’ institution: Key findings and implications from mixed methods research. Journal of Exercise Rehabilitation, 16(1), 78–87. https://doi.org/10.12965/JER.1938726.363
Williams, D., Collingwood, L., Coles, J. & Schmeer, S. (2015). Evaluating a rugby sport intervention programme for young offenders. Journal of Criminal Psychology, 5(1), 51–64. https://doi.org/10.1108/JCP-05-2014-0008
Wong, T. M. L., Loeber, R., Slotboom, A. M., Bijleveld, C. C. J. H., Hipwell, A. E., Stepp, S. D., & Koot, H. M. (2013). Sex and age differences in the risk threshold for delinquency. Journal of Abnormal Child Psychology, 41(4), 641–652. https://doi.org/10.1007/s10802-012-9695-7
Yılmaz, A., & Soyer, F. (2018). Effect of physical education and play applications on school social behaviors of mild-level intellectually disabled children. Education Sciences, 8(2), 89.
Zivin, G., Hassan, N., DePaula, G., Monti, D., Harlan, C., Hossain, K., & Patterson, K. (2001). An effective approach to violence prevention: Traditional martial arts in middle school. Adolescence, 36(143), 443–459.
Funding
This research project was funded by Reclassering Nederland (the Dutch probation service). They were not involved in the study design, manuscript drafting, or data collection and analysis. Contact information: Vivaldiplantsoen 100, 3533 JE Utrecht, The Netherlands.
Author information
Authors and Affiliations
Contributions
M.E. van der Sluys wrote the review and performed the data analysis in collaboration with J. Zijlmans and P. H. van der Laan. The literature search strategy was devised by J. C. F. Ket. All authors were involved in the revising of the manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher's note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
van der Sluys, M.E., Zijlmans, J., Ket, J.C.F. et al. The efficacy of physical activity interventions in reducing antisocial behavior: a meta-analytic review. J Exp Criminol 20, 347–373 (2024). https://doi.org/10.1007/s11292-022-09536-8
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11292-022-09536-8