
Abstract
To evaluate the potential public health impact of exposure to airborne particulate matter, concentrations of PM10 and PM2.5 were measured at 16 monitoring stations in Pearl River Delta. Epidemiological studies were collected, and meta-analysis method was used to get the exposure-response functions for health effects on mortality of residents in China. Chinese studies reported somewhat lower exposure-response coefficients as compared with studies abroad. Both Poisson model and life-table approach were used to estimate the health effects including acute effects and chronic effects. For short-term exposure, 2,700 (95% confidence interval (CI), 2,200–3,400) premature deaths would be prevented annually if PM10 daily concentrations reduced to below World Health Organization (WHO) guideline value. Much more benefits would be gained for long-term exposure. The annual avoidable deaths would be 42,000 (95% CI, 28,000–55,000) and 40,000 (95% CI, 23,000–54,000) for PM10 and PM2.5, respectively, if the particulate matter annual concentrations were reduced to below WHO guideline values. And the average lifespan of residents would prolong 2.57 years for PM10 and 2.38 years for PM2.5 if reducing the PM annual concentrations. The benefits varied greatly in different areas and different manage strategies should be carried out to protect human health effectively.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
1 Introduction
Compared with other air pollutants, particulate matter measured as either total suspended particle (TSP), PM10 (those less than 10 μm), PM2.5 (those less than 2.5 μm), or black smoke appears to show most consistent association with human health. A recent World Health Organization review (WHO 2003) concluded that ambient particulate matter was considered responsible for the health effects seen in large epidemiological studies relating ambient particulate matter to mortality and morbidity. Epidemiological studies have consistently shown an association between particulate matter pollution and premature deaths in China and other countries (Wong et al. 2001; Kan et al. 2007; Qian et al. 2007a, b; Daniels et al. 2000; Stieb et al. 2002). There was also abundant evidence associating particulate matter pollution with increase in hospital admissions or outpatients for respiratory and cardiovascular diseases (Ware et al. 1986; Burnett et al. 1997; Wong et al. 1999; Peters et al. 1999; Peng et al. 2008).
The public health impact exposure to particulate matter (PM) included both acute (with short-term effects) and chronic (with long-term effects) effects. Time-series studies identified the health impact of PM pollution in the preceding days, whereas cohort studies analyzed the health effects due to long-term exposure to PM. For mortality, whereas time-series approaches captured only cases in which deaths have been triggered by air pollution exposure incurred shortly before deaths, cohort studies captured all air pollution-related categories of deaths, including deaths of persons whose underlying health condition led to premature deaths without being related to the level of pollution shortly before deaths (Kunzli et al. 2001). Compared with time-series studies, the cohort studies provided more complete assessment of the impact from exposure to air pollution (Kunzli et al. 2001) and represented the full effects of air pollution more accurately.
Health impact assessment (HIA) based on epidemiological study evidence was used widely to estimate the health damage due to PM pollution. Similar assessment studies in Japan, America, Europe, and other areas (Aunan et al. 1998; Levy et al. 2001; Leksell and Rabl 2001; Medina et al. 2004; Yorifuji et al. 2005; Boldo et al. 2006; White et al. 2008) showed quantification estimate results of the impact of PM pollution on human health. In those existed estimated studies, mainly focused on PM10, public health impact of short-term or long-term exposure to airborne particulate matter was valued. There were also some assessment studies in China (Zhang et al. 2007a, b, 2008) assessed the acute health impact due to exposure to PM10 in Beijing and other cities and valued the economic loss. Hedley et al. (2006) also valued the acute health effect due to exposure to air pollutants, such as SO2, NO2, O3, and PM10, in Pearl River Delta. Kan and Chen (2002) assessed the impact of long-term exposure to particulate matter (measured as TSP) on life expectancy and survival rate of Shanghai residents. While recent toxicological research suggested potentially important roles for sulfates, particulate acids, metals, and organic compounds in PM toxicity, nevertheless, there was insufficient evidence to identify the independent effects of these correlated compositions. And ambient concentrations of most of the identified particulate constituents would be reduced by control strategies targeting PM10 and PM2.5 mass. Little heath assessment studies on benefits from controlling chemical composition of particulate matter was available in China and other countries.
To our knowledge, assessment studies on public health impact of exposure to PM10 and PM2.5, especially for PM2.5, were much-needed in Pearl River Delta (PRD). PRD is one of the six most important key economic belts in China. It lies in the south of China. PRD consists of nine prefectures in Guangdong Province and two Special Administrative Regions (SARs). Those prefectures include Guangzhou, Shenzhen, Zhuhai, Dongguan, Zhongshan, Foshan, Huizhou, Jiangmen, and Zhaoqing. And the two SARs are Hong Kong (HK) and Macao Special Administrative Region (MSAR). The region, with an area of 41,700 km2 (not including HK and MSAR), had a population of about 45.5 million in 2006. The gross production of this area, without HK and MSAR, was about 2161.8 billion Yuan RMB, which accounted for about 10.3% of GDP of China in 2006. Especially in recent 30 years, PRD had a great progress in economic growth but got more terrible air pollution. Energy production and consumption in Guangdong has increased largely. Evaluating the impact on human health attributable to PM pollution in PRD is regarded as an essential step to assess the effectiveness of air pollution control policies in this region.
The Air Quality Monitoring Network of Guangdong and Hong Kong (AQMNGH) which was consisted of 16 monitoring stations started to work in December, 2005. Thirteen stations were in Guangdong province, and the other three stations were in Hong Kong. The network would provide the government and the public more accurate and overall regional air quality data. For long-term observation, it would provide the policy makers useful information, which was necessary to establish effective management strategies to relieve the regional air pollution level in PRD. Unified guidelines for gathering and analyzing data were used to ensure comparability of the data in different areas. More details about AQMNGH could be found in other published work (Zhang et al. 2005).
In this study, the public health impact of exposure to PM10 and PM2.5 would be assessed, based on the monitoring data of AQMNGH in 2006. The health benefits from reducing the PM concentrations, in terms of number of avoidable deaths and potential gain in life expectancy, would be assessed.
2 Methodology
In this study, HIA provided estimates of avoidable deaths and influence on life expectancy attributable to PM pollution exposure to the target population in PRD, assuming that there was a causal relationship between PM pollution and the observed health effects. The health benefits from reducing PM concentrations in PRD represented the health damage attributed to PM pollution. Both the acute and chronic effects associated with PM exposure were estimated using Poisson model and Life-table method.
The HIA method, similarly used in Japan and Europe (Yorifuji et al. 2005; Boldo et al. 2006), consisted of four steps: specific exposure, health outcomes and exposure response functions, setting HIA scenarios, and calculating the estimated impact in the target population.
2.1 Exposure Measurement
The observation data of PM10 and PM2.5 based on AQMNGH were selected between January 1 and December 31, in 2006. The original data were measured as 1-h average concentrations. And the daily average concentrations and annual average concentrations were exacted from the original data. Concentrations of PM10 were measured at all 16 stations. However, concentrations of PM2.5 were only measured at six stations. PM2.5 annual concentrations were derived from PM10. Conversion factor 0.7, the average annual concentration ratio of PM2.5/PM10 in the six stations, was used. Uncertainties using the factor 0.7 would be discussed later. The observation data were shown in Table 1.
2.2 Health Outcomes and Exposure-Response Functions
The PM-associated health outcomes included mortality, chronic morbidity, hospital admissions and outpatients, and decline in lung function. Among all the health outcomes, death was most notable and contributed largest health damage and economic loss. So, in this study, only the mortality effects due to PM pollution were assessed.
Exposure response functions were used in epidemiologic studies to associate air pollution with adverse health effects. The exposure-response functions in our study were attained from epidemiology studies. Time-series studies identified the short-term health impact of particle pollution, whereas cohort studies analyzed the health effects due to long-term exposure to PM. Time-series studies on mortality from 1990 to 2009 in China were collected, and meta-analysis was used to get the exposure-response functions for short-term exposure. Two major databases, Medline and PubMed, were searched for papers published in international journals. For papers published in local mainland journals, China Academic Journals Full-text Database and Chinese Science Journals Full-text Database were used instead. For long-term exposure, two American cohort studies were used because there were still no published cohort studies on PM10 or PM2.5 in China. The two studies, American Cancer Society (ACS) study (Dockery et al. 1993) and Harvard Six Cities Study (Pope et al. 1995, 2002) were well-illustrated by many assessment studies in other countries (Martuzzi et al. 2003; Sultan 2007; White et al. 2008; Zhang et al. 2008). Table 2 listed all published epidemiology studies of effects of PM10 and PM2.5 in China published in English and Chinese. After a systematic literature search, the exposure-response coefficients were estimated by means of a meta-analysis method (inverse variance method), in which the overall coefficients was a weighted average of the individual study coefficients. The weights used in the calculation were the inverse of the study variance (Aunan and Pan 2004). Homogeneity should be assessed by means of the Q statistic, which was the sum over all studies of the study weight multiplied with the square of the difference between the study coefficients and the weighted average coefficient. After homogeneity test, the fixed-effects model or the random effects model could be chosen (fixed-effects model for homogeneity and random effects model for heterogeneity).The meta-analysis software Revman 4.2.2 was used for statistical integration. More details about the process of meta-analysis could be found in other studies (Schlesselman and Collins 2003; Aunan and Pan 2004; Xie et al. 2009).
2.3 Health Impact Assessment Scenarios
Threshold concentration was defined as the lowest boundary that there was no obvious observed adverse health effect below it. But, there was no such concentration found in existed epidemiological studies. Our aim was to provide useful information for policy decision-makers, the ambient concentration as zero or background concentrations was considered not appropriate as the reference concentration in this study. However, there was no ambient standard of PM2.5 in China yet. So, here, the WHO guideline values were chosen as the reference concentrations. The WHO guideline values included 24 h concentration guideline values (25 μg/m3 for PM2.5 and 50 μg/m3 for PM10) and annual concentrations of PM2.5 and PM10 (10 μg/m3 for PM2.5 and 20 μg/m3 for PM10). WHO guideline values of PM were mainly based on published epidemiological studies all over the world and could well protect human health. In our study, the benefits from reducing annual PM concentrations to WHO guideline values represented the health effects attributed to particulate matter pollution.
2.4 Health Impact Assessment Tools
Both avoidable deaths and potential gain in life expectancy were calculated to assess the public health impact of exposure to PM10 and PM2.5.
-
(a)
Avoidable deaths
Poisson model was often used to quantify the effect of air pollution on morbidity and mortality rates (Zhang et al. 2007a, b). In this study, the simplified linear function was used. The number of avoidable deaths for long-term exposure was calculated as:
Where β is the exposure-response coefficient from cohort studies, C and C 0 are the ambient particle annual concentrations and reference concentrations (here WHO annual guideline values were used). E and E 0 are the health effects at C and C 0, respectively. The ΔH or the health damage caused by increased pollution can be calculated if β, C, C 0, and E are known.
Similarly, for short-term exposure, the calculation formula treated as:
Where β is the exposure-response coefficient from time-series study, C i and C 0 are the ambient particle daily concentrations and reference concentrations (here WHO 24-h guideline values were used).
Health data in PRD, including population and non-accident mortality, was available for 2005 in PRD from the 1% population sampling investigation in Guangdong Province. It was assumed to be applicable to 2006. Health data in Hong Kong were derived from Hong Kong Health Department. Because only adults were included in the two American cohort studies, the estimation of avoidable deaths and the potential gain in life expectancy calculations for long-term exposure were restricted to population older than 30 years. All baseline data were shown in Table 3.
-
(b)
Gain in life expectancy
Because the number of death could not explain the difference between deaths with different ages, so potential gain in life expectancy was also calculated using life table approach in this study. A life table was estimated for a sample population of 100,000 people, who were assumed to be exposed to the current deaths risks in the area of interest for their whole life (Chiang 1968; Nevalainen and Pekkanen 1998). It was constructed with 5-year intervals. For each interval, the number of deaths was estimated for the population alive in the beginning of the interval. The probability of surviving an interval was estimated as the number of people alive at the end of the interval divided by the number of people alive in the beginning of the interval. The calculation of life expectancy was based on these probability estimates (Chiang 1968; Lee 1992).
Comparing the difference of the actual life table based on actual particulate matter levels with the hypothetical life table in the case of baseline scenario, where the concentrations of particulate matter did not exceed the guideline values suggested by WHO, the potential gain in life expectancy was got. The pooled coefficients from meta-analysis results were used, assuming the same proportional hazard reduction for every age group (age ≥ 30 years).
3 Results
3.1 Concentrations of PM in PRD, in 2006
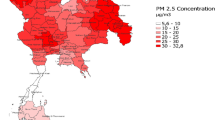
PM exposure concentrations of areas were extracted from the observation data of monitoring stations. For the areas which had over one station, average concentrations of stations were treated as the exposure concentrations. The PM pollution level in PRD was very high and varied greatly in different areas. Throughout the year, higher daily concentrations of PM were observed from October to March.
Table 4 showed the annual concentrations of PM10 and PM2.5 in PRD in 2006. Except for Guangzhou and Hong Kong, annual concentrations of PM2.5 were converted from PM10, and conversion factor 0.7 was used. The annual mean concentrations of PM10 and PM2.5 were 73 and 51 μg/m3, respectively, in PRD, much higher than the guideline values suggested by WHO. In some areas, such as Dongguan, Foshan, and Huizhou, the concentrations of PM10 even exceeded 100 μg/m3 and the concentrations of PM2.5 were higher than 80 μg/m3. Concentrations of PM varied largely in each area. The population in PRD was unevenly distributed, either. In the central and the northeast parts of PRD, such as Foshan, Dongguan, and Huizhou, which were newly developing industrial estates, concentrations of PM10 and PM2.5 were higher than those in the southeast of PRD, such as Zhuhai and Zhongshan. Here, the conception of population-weighted concentration was used to elucidate this variance. The population-weighted concentration was calculated as:
Where Cpw is the population-weighted concentration, Ci and pi are the ambient annual concentration and population in each prefecture. The calculation results showed that the population-weighted concentrations of PM10 and PM2.5 were 77 and 55 μg/m3, respectively, in PRD, a little higher than the annual concentrations. It suggested that a large number of people were exposed to high level of PM pollution. For example, in some areas, such as Guangzhou, Dongguan, and Foshan, the concentration of particulate matter was high while the population was large too.
3.2 Exposure-Response Functions
The selected ERFs finally used in this study were pooled estimate value by the means of meta-analysis, as shown in Table 5. For short-term exposure, while the daily concentrations of PM10 and PM2.5 increased 10 μg/m3, all-course daily mortality of residents increased 0.33% (95% CI, 0.24–0.43%) and 0.42% (95% CI, 0.03–0.81%), respectively. For long-term exposure, all-course annual mortality of adults would increase 5.4% (95% CI, 2.8–7.8%) and 7.6% (95% CI, 3.6–11.6%) for 10 μg/m3 increase in annual concentrations of PM10 and PM2.5. Health effects attributable to PM pollution in terms of avoidable deaths and gain in life expectancy were calculated based on these coefficients.
For short-tem exposure, all published epidemiology studies in China from 1990–2009 were collected, and meta-analysis was used to get the exposure-response coefficients. Chinese studies reported somewhat lower exposure-response coefficients as compared with studies abroad especially in developed countries, shown in Fig. 1. In the APHEA2 project (Air pollution and Health-a European Approach), Katsouyanni et al. 2001, 2003 reported 0.6% (95% CI, 0.4–0.7%) increase in daily mortality rate per 10 μg/m3 increase in PM10 daily concentrations based on data from 29 European countries. A meta-analysis study based on 33 epidemiology studies in Europe (Anderson et al. 2004) also showed 0.6% (95% CI, 0.4–0.8%) increase in mortality while PM10 daily concentrations increased 10 μg/m3. A multi-city study of short-term exposure and mortality based on 20 US large cities (Daniels et al. 2000) reported 0.5% (95% CI, 0.3–0.8%) increase in mortality per 10 μg/m3 increase in PM10. Another NMMAPS (National Morbidity, Mortality, and Air Pollution Study), covering over 90 American cities, indicated a lower increase (0.1–0.4%) in mortality. Burnett et al. (2000) analyzed daily mortality counts and air pollution in nine Canada cities and got the conclusion that daily mortality would increase 0.6% (95% CI, 0.5–0.8%) for 10 μg/m3 increase in PM10 daily concentrations. Meta-analysis studies or multi-city studies on PM2.5 were also compared, shown in Fig. 1. A multi-city study based on 112 American cities (Zanobetti and Schwartz 2009) reported 1.0% (95% CI, 0.8–1.3%) increase in mortality per 10 μg/m3 increase in PM2.5 daily concentrations. The studies done in Canada (Burnett et al. 2000) showed 1.2% (95% CI, 0.5–2.0%) increase for PM2.5.

Percent increase in mortality per 10 μg/m3 increase of the concentrations of PM in different areas. Vertical line means 95% confidence interval. PM 10 China, our study result; Europe, Anderson et al. (2004); USA, Daniels et al. (2000); and Canada, Burnett et al. (2000). PM 2.5 China our study result; Europe, Peters et al. (2002) and Neuberger et al. (2007); USA, Zanobetti and Schwartz (2009); Canada, Burnett et al. (2000)
For long-term exposure, there were still no cohort studies on PM2.5 and PM10 in China. The only published cross-sectional study of long-term exposure and mortality, in Benxi (Jing et al. 1999), indicated 8% increase in mortality while total suspended particles (TSP) concentrations increased 100 μg/m3. It meant 1.3% and 2% increase in mortality per 10 μg/m3 increase in PM10 and PM2.5, while the mass concentration conversion factor 0.65 was used (PM10 = TSP × 0.65, PM2.5 = PM10 × 0.65). The exposure-response coefficients were lower than the two American cohort studies.
3.3 Avoidable Deaths Attributable to PM-Exposure in PRD
As shown in Figs. 1 and 2, in terms of avoidable deaths, 2,700 (95% CI, 2,200–3,400) premature deaths for PM10 would be prevented annually if the daily concentrations were reduced to below WHO 24-h guideline value in PRD. Areas with higher concentrations and larger populations, such as Foshan and Guangzhou had larger benefits from PM10 reductions. Only two areas, Guangzhou and Hong Kong, had the PM2.5 daily concentrations data. The annual number of avoidable deaths would be 710 (95% CI, 340–1,100) in Guangzhou and 240 (95% CI, 110–370) in Hong Kong if the PM2.5 daily concentrations were reduced to below WHO 24-h guideline value.

Number of avoidable deaths reducing PM concentrations below WHO guideline values in PRD (95% confidence limits based on 95% CI of the exposure-response functions). Black solid points meant PM10 and red hollow points meant PM2.5. a For short-term exposure; b For long-term exposure. DG Dongguan, FS Foshan, GZ Guangzhou, HK Hong Kong, HZ Huizhou, JM Jiangmen, SZ Shenzhen, ZH Zhuhai, ZQ Zhaoqing, ZS Zhongshan
The assessment results of chronic effects would be much larger than acute effects. For long-term exposure, 42,000 (95% CI, 28,000–55,000) premature deaths would be prevented annually if the PM10 annual concentrations were reduced to below WHO annual guideline value in PRD. And for PM2.5, the annual number of avoidable deaths became 40,000 (95% CI, 23,000–54,000). The potential benefits of reducing annual PM levels also varied in different areas. In terms of premature deaths, in Guangzhou, Foshan, and Hong Kong, the benefits of reducing annual PM levels were great, whereas Shenzhen, Zhuhai, and Zhongshan showed much smaller benefits. The influence on mortality was mainly influenced by concentrations of PM, while the avoidable deaths were also influenced by the amount and deaths rate of target population. Some areas, like Guangzhou and Hong Kong, showed large numbers of avoidable deaths for a relative larger population, while the changes in mortality were not very huge. Shenzhen showed small benefits in terms of premature deaths for low death rate of population.
3.4 Gain in Life Expectancy Associated with the Reduction of PM Concentration
In Foshan, Huizhou, and Dongguan, where the PM concentrations were higher, influence on life expectancy would be larger. And in Zhuhai and Zhongshan, influence would be much lower than other areas. The average lifespan of adults in Foshan and Dongguan would prolong more than 3 years when the concentrations of PM in these areas were reduced to below WHO guideline values. But, in Zhongshan and Zhuahai, the average lifespan of adults would prolong less than 1 year.
For PM10 and PM2.5, the potential gain in person-years lost would be 68,000,000 person-years in PRD if the concentrations of PM10 were reduced to below the value of WHO guideline. And for PM2.5, the expected gain in person-years lost would be 63,000,000 person-years. The amount of population in PRD was about 26.49 millions, which suggested that the average lifespan in PRD would prolong 2.57 and 2.38 years for PM10 and PM2.5, respectively. As shown in Fig. 3, Guangzhou and Foshan got great benefit from these reductions due to high concentrations of PM and a large population. Zhuhai and Zhongshan were influenced slightly, due to lower PM pollution levels and a smaller population.

Gain in life expectancy reducing PM concentrations below WHO guideline values in PRD (95% confidence limits based on 95% CI of the exposure-response functions). Black solid points meant PM10 and red hollow points meant PM2.5. DG Dongguan, FS: Foshan; GZ: Guangzhou; HK: Hong Kong; HZ: Huizhou; JM: Jiangmen; SZ: Shenzhen; ZH: Zhuhai; ZQ: Zhaoqing; ZS: Zhongshan
4 Discussion
The health impact of exposure to particulate matter in PRD was estimated, in terms of avoidable deaths and gain in life expectancy. Results showed that both PM10 and PM2.5 contributed to the total burden of mortality in PRD in a non-negligible manner. Health effects due to PM might be explained mainly by PM2.5 exposure and coarse particles (PM2.5–10) did not show significant association with mortality. This result was consistent with other studies (Yorifuji et al. 2005). In this study, both the acute effects and chronic effects exposure to PM pollution were assessed. Compared with other HIA estimate findings in PRD (Hedley et al. 2006), this study showed large heath impact attributed to PM10 pollution because long-term air pollution exposure had greater effect on human health than short-term exposure. In China, the only HIA estimate findings of long-term exposure to airborne particulate pollution (measured as TSP) done in Shanghai (Kan and Chen 2002) showed that 1.34–1.69 years reduction of life expectancy could be attributed to air particulate matter exposure. It seemed a little lower than our results. In that study, the natural background level of TSP (127 μg/m3) in Shanghai was chosen as the reference level. Estimated studies done in Europe and America obtained less impact on life expectancy attributed to particulate matter pollution because the pollution level was not as severe as that in PRD (Boldo et al. 2006; Brunekreef 1997).
4.1 Methodological Considerations
In this study, some assumptions about exposure and extrapolation of ERFs and HIA scenarios were set. These assumptions would bring some underlying uncertainties in the assessment of reducing the PM pollution level in PRD.
Regarding exposure data, our HIA findings depended directly on the concentrations of measured particulate matter pollution. As the air pollution in PRD has been paid greater attention in recent several years, there was actually a gentle variation of PM pollution level in PRD, especially from 2004. According to the monitor data promulgated by Guangdong EPA (http://www.gdepb.gov.cn/hjzlyxx/hbzkgb/200906/t20090615_62862.html), the average annual concentrations of PM10 in Guangdong Province from 2005 to 2008 were 61, 62, 63, and 58 μg/m3, respectively. And the average annual concentrations of PM10 in Hong Kong from 2005 to 2008 were 59, 60, 63, and 56 μg/m3, respectively (http://www.epd-asg.gov.hk/english/report/airborne.php). Although, for long-term exposure, available exposure data was just 1 year in this study, our estimate results could elucidate the health impact of long-term exposure attributed to particulate matter in PRD. As the PM2.5 measurement data was not available for each area, the conversion factor 0.7 was used to calculate PM2.5 concentration from PM10. The conversion factor was got from the average ratio of PM2.5/PM10 of the six sites where PM10 and PM2.5 were measured simultaneously. The ratio was consist well with other studies in PRD (Cao et al. 2003, 2004; Niu et al. 2006; Lai et al. 2007; Chen et al. 2008; Liu et al. 2008).
Regarding the exposure-response functions, for short-term exposure, all epidemiology studies from 1990 to 2009 in China were collected, and meta-analysis was used to get the exposure-response coefficients. Our study might be the most systematic review of Chinese epidemiological studies on PM-associated mortality effects especially for fine particles. Results from our study suggested that the exposure response relationship coefficients of PM10 and PM2.5 in China were a little lower than in USA or Europe, which was consisted with other studies (Xie et al. 2009; Aunan and Pan 2004). For long-term exposure, because there were some methods defects in cross-sectional studies (such as ecological fallacy), it was not suitable to use exposure-response functions from cross-sectional studies to quantify the long-term health effects. Estimating the impact on long-term exposure to PM should be based on cohort studies, for cohort studies provide more complete assessment of the impact from exposure to air pollution. But, there were no cohort studies on PM10 or PM2.5 available in China or any other developing countries. Two available and well-accepted cohort studies done in America were applied to our study. The PM pollution level in PRD was very high and in most areas, PM concentrations exceeded the range of the referential cohort studies. Although the association between the mortality and the PM pollution was not significantly different from linear associations, the shape of exposure response relationship in cohort studies (Pope et al. 2002) showed that the relative risk of per 10 μg/m3 increase of PM concentration would decrease slowly when the exposure concentration became too high. The linear assumption about the exposure-response functions would overestimate the health effect. Different internal compositions of PM also existed between PRD and American region. For example, fine particulate mass within the PRD was dominated by organic compounds (24–35%) and sulfate (21–32%). Other important measured constituents included crustal material (7–13%), ammonium (6–8%), elemental carbon (3–8%), and nitrate (1–6%) (Hagler et al. 2006). But, in USA, fine particulate mass was mainly consisted of organic compounds (28%), sulfate (26%), nitrate (12%), and ammonium (11%; Bell et al. 2007), showing higher proportion of nitride and lower proportion of crustal material. Laden et al. (2000) examined PM2.5 data from the Harvard Six-Cities study and got the conclusion that both the motor vehicle and coal factors were associated with mortality, with the strongest effect from the former, but the crustal material in PM2.5 was not associated with mortality. So, the exposure response relationship coefficient applied in PRD might be a little larger than the real effect. The validity of the extrapolation of exposure response functions to our target population was also a concern, and there were few differences in socio-demographic characteristics among the target population. For example, the proportion of elder people and the proportion of smokers, including current and past smokers, were smaller in PRD. Pope et al. (2002) concluded that although differences across age and sex strata were not generally consistent or statistically significant, the relative risk estimates for both cardiopulmonary and lung cancer mortality were higher for nonsmokers. In all, exposure-response functions based on two American cohort studies might overestimate the real effect of exposure to airborne particulate matter and cohort studies on PM in China should be conducted.
The influence of other co-pollutants should be also discussed. The annual concentrations of sulfur dioxide, nitrogen dioxide, and ozone were 18, 24, and 21 ppb in PRD, in 2006. And in ACS study, the concentrations ranges were 6.7–9.7 ppb for sulfur dioxide, 21.4–27.9 ppb for nitrogen dioxide, and 45.5–59.7 ppb for ozone. It seemed that sulfur dioxide pollution was much severer, and ozone pollution was less serious. Krewski et al. (2000) completed an independent validation and reanalysis of both the Six-Cities and the ACS cohort studies and got the conclusion that the PM effects were not confounded by and were independent of effects of other pollutants. Samat et al. (2001) also got the findings that ambient PM2.5 concentrations are suitable surrogates for personal PM2.5 exposures and that ambient gaseous concentrations are surrogates, as opposed to confounders, of PM2.5.Thus, other co-pollutants might not greatly influence the health effects caused by PM.
The reference exposure level was an especially sensitive parameter in our estimate model. Choosing a lower baseline, the impact of the pollution measurements would increase more. Here, the values of WHO guideline were chosen. But, the exposure concentrations of airborne particulate matter in PRD, even in China, were much higher than some other countries, especially those developed countries in Europe and North America. It would be really a hard to reduce the concentrations of particulate matter to the value of WHO guideline in PRD in a short period. In our study, the health benefits from the 10% reduction in particulate matter were also calculated. In terms of avoidable deaths, 6,600 (95% CI, 4,000–9,400) premature deaths for PM10 and 5,900 (95% CI, 3,100–8,800) premature deaths for PM2.5 could be prevented annually if 10% reduction in PM annual concentrations was attained. The potential gain in person-years lost would be 8,800,000 and 8,000,000 for PM10 and PM2.5, respectively, which suggested that the average lifespan of adults in PRD would prolong 0.33 and 0.30 years, respectively. An ambient standard or a guideline of PM2.5 concentration in China would be necessary. And the ambient standard of PM10 needs to be revised, since the current Chinese ambient daily standard and annual standard of PM10 are 150 and 100 μg/m3, which seem too high to protect human health effectively.
The actual impact of exposure to airborne particulate matter on human health in PRD might be a bit greater than the results from our study because the assessed health impact of particulate matter focused only on mortality but morbidity was not included. Although the death was the most important and notable health outcome, the amount of disease due to PM exposure could be considerable in China and other countries (Qian et al. 2004; Kappos et al. 2004; Ranzi et al. 2004). On the other hand, for long-term exposure, the impact due to PM on mortality of those under age 30 years was not estimated, while more or less health damage could be caused to the younger population, especially in the post-neonatal period (Woodruff et al. 1997).
4.2 Manage Strategies Implications
In our study, the avoidable premature deaths were calculated (shown in Figs. 1 and 2). And the expected gain in life expectancy, seen in Fig. 3, was also estimated. The potential benefits were notable if effective controls were carried out in PRD. Even though the 10% reduction in annual particulate matter concentrations was achieved, the health benefits were considerable in PRD. The benefits from reducing PM concentrations varied greatly in different prefectures. Some areas, such as Foshan, Guangzhou, and Dongguan were greatly benefited from the reductions. However, Zhuhai and Zhongshan were influenced slightly.
Note that the potential benefits were mainly influenced by the PM concentrations, the amount of population and the death rate in each prefecture. Areas, with higher concentrations of particulate matter, larger population and higher mortality, showed higher value of potential benefits. The areas like Guangzhou, Foshan, and Dongguan, where the particulate matter concentrations were very high and the amount of population was large, both avoidable deaths and expected gain in life expectancy from reduction in PM concentrations would be remarkable. The kind of areas was suggested as key-controlling areas. In these areas, the PM pollution was severer and great benefits from PM concentration reduction would be gained. Strict management controls should be carried out immediately to reduce the particulate matter levels for protecting human health. In areas like Dongguan, Jiangmen, Zhaoqing, and Huizhou, where the population was relative small, benefits were also considerable owing to high concentrations of particulate matter. Rational and effective control steps should be implemented to improve the air pollution. In areas like Shenzhen and Hong Kong, where the population was large while the particle pollution was not too severe, the impact of exposure to particulate matter was large. The kind of area was suggested as key-monitoring areas. In these areas, little reduction in particulate matter levels would bring in great benefits. Great attention should be paid to the air pollution and some controls should be made out and implemented to prevent damage to human health there. Zhuhai and Zhongshan showed relatively small benefits from the reduction, where the concentration of particulate matter was much lower and the population was smaller than other areas. Different manage strategies in different types of areas should be carried out to protect human health more effectively.
Our study only gave the potential benefits of PM concentration reductions in PRD, and the internal chemical compositions of PM might influence the particles' toxicity. Getting the chemical compositions of PM and identifying which source had the largest contribution to health impact would be also helpful to policy makers.
5 Conclusion
Our assessment led us to get such conclusions: (1) Annual mean concentrations of PM10 and PM2.5 were found to reach 73 and 51 μg/m3, respectively, in PRD. Foshan, Huizhou, and Dongguan had more severe PM pollution. Zhongshan and Zhuhai had a little slighter PM pollution. (2) From the meta-analysis results, Chinese studies reported somewhat lower exposure-response coefficients as compared with internal studies. For short-term exposure, while the daily concentrations of PM10 and PM2.5 increased 10 μg/m3, all-course daily mortality of residents increased 0.33% (95% CI, 0.24–0.43%) and 0.42% (95% CI, 0.03–0.81%), respectively. For long-term exposure, all-course annual mortality of adults would increase 5.4% (95% CI, 2.8–7.8%) and 7.6% (95%CI, 3.6–11.6%) for 10 μg/m3 increase in annual concentrations of PM10 and PM2.5, (3) In terms of avoidable deaths, for short-term exposure, 2,700 (95% CI, 2,200–3,400) premature deaths would be prevented annually if the PM10 daily concentrations were reduced to below WHO 24-h guideline value. Much larger benefits would be gained if the annual concentration did not exceed WHO annual guideline value in PRD. For PM10, 42,000 (95% CI, 28,000–55,000) premature deaths would be prevented annually and for PM2.5, the number of deaths avoidable would be 40,000 (95% CI, 23,000–54,000). (4) In terms of gain in life expectancy, the avoidable person-years lost of adults would be 68,000,000 and the average lifespan would prolong 2.57 years for PM10. And for PM2.5, the avoidable person-years lost would be 63,000,000 and the average lifespan would prolong 2.38 years if the annual concentrations of PM in PRD reduced to below WHO guideline values. (5) The potential benefits of reducing annual PM levels varied in different prefectures. Different manage strategies should be carried out in different types of prefectures in PRD to improve the air quality.
From our study, the reductions in concentrations of both PM10 and PM2.5 would bring in remarkable health benefits, especially for long-term exposure. So, it is obligatory to set up an ambient standard or a guideline of PM2.5, and the ambient standard of PM10 needs to be revised in China to protect human health more effectively.
References
Anderson, H. R., Atkinson, R. W., Peacock, J. L., et al. (2004). Meta-analysis of time series studies and panel studies of particulate matter (PM) and ozone (O3) [R]. Report of a WHO task Group. Copenhagen: WHO.
Aunan, K., & Pan, X. (2004). Exposure-response functions for health effects of ambient air pollution applicable for China: a meta analysis. The Science of the Total Environment, 329(1–3), 3–16.
Aunan, K., Patzay, G., & Asbjorn, A. H. (1998). Health and environmental benefits from air pollution reductions in Hungary. The Science of the Total Environment, 212(2–3), 245–68.
Bell, M. L., Dominici, F., Ebisu, K., Zeger, S. L., & Samet, J. M. (2007). Spatial and temporal variation in PM2.5 chemical composition in the United States for health effects studies. Environmental Health Perspective, 115(7), 989–995.
Boldo, E., Medina, S., Tertre, A., Hurley, F., Muecke, H. G., Ballester, F., et al. (2006). Apheis: health impact assessment of long-term exposure to PM2.5 in 23 European cities. European Journal of Epidemiology. doi:10.1007/s106540069014-0.
Brunekreef, B. (1997). Air pollution and life expectancy: is there a relation? Occupational and Environmental Medicine, 54(11), 781–784.
Burnett, R. T., Brook, J. R., Dann, T., Delocla, C., Philips, O., Cakmak, S., et al. (2000). Association between particulate- and gas-phase components of urban air pollution and daily mortality in eight Canadian cities. Inhalation Toxicology, 12(4), 15–39.
Burnett, R. T., Cakmak, S., Brook, J. R., & Krewski, D. (1997). The role of particulate size and chemistry in the association between summertime ambient air pollution and hospitalization for cardiorespiratory diseases. Environmental Health Perspectives, 105(6), 614–620.
Cao, J., Lee, S., Ho, K. F., Zhang, X., Zou, S., Fung, K., et al. (2003). Characteristics of carbonaceous aerosols in Pearl River Delta region, China in 2001 Winter period. Atmospheric Environment, 37(11), 1451–1460.
Cao, J., Lee, S., Ho, K. F., Zou, S., Fung, K., Li, Y., et al. (2004). Spatial and seasonal variations of atmospheric organic carbon and elemental carbon in Pearl River Delta Region, China. Atmospheric Environment, 38(27), 4447–4456.
Chen, H., Liu, J., Zhang, J., & Song, Z. (2008). Characteristics of mass concentration variations of PM2.5 and PM10 at Guangzhou. Environmental Science & Technology, 31(10), 87–91. In Chinese.
Chiang, C. L. (1968). Introduction to stochastic processes in biostatistics. New York: Wiley.
Dai, H., Song, W., Gao, X., Chen, L., & Hu, M. (2004). Study on relationship between ambient PM10, PM2.5 pollution and daily mortality in a district in Shanghai. Journal of Hygiene Research, 33(3), 293–297. In Chinese.
Daniels, M. J., Dominici, F., Samet, J. M., & Zeger, S. L. (2000). Estimating particulate matter-mortality dose-response curves and threshold levers: an analysis of daily time-series for the 20 largest US cities. American Journal of Epidemiology, 152(5), 397–406.
Dockery, D. W., Pope, C. A., Xu, X., Spengler, J. D., Ware, J. H., Fay, M. E., et al. (1993). An association between air pollution and mortality in six US cities. The New England Journal of Medicine, 329(24), 1753–1759.
Hagler, G. S. W., Bergin, M. H., Salmon, L. G., Yu, J. Z., Wan, E. C. H., Zheng, M., et al. (2006). Source areas and chemical composition of fine particulate matter in the Pearl River Delta region of China. Atmospheric Environment, 40, 3802–3815.
Hedley, A. J., McGhee, S. M., Wong, C. M., Barron, B., Chau, P., Chau, J., et al. (2006). Air pollution: costs and paths to a solution. Resource document. Civic Exchange.(http://www.civic-exchange.org/eng/upload/files/200606_AirPollutionSolution.pdf. Accessed 6 May 2008).
Jia, J., Kan, H., Chen, B., Xu, W., & Xia, D. (2004). Association of air pollution with daily mortality in Zhabei District of Shanghai: a case-crossover analysis. Journal of Environmental Health, 21(5), 279–282. In Chinese.
Jing, L., Qian, Y., Xu, Z., Wang, S., Ren, Z., Ren, L., et al. (1999). Relationship between air pollution and mortality in Benxi. China Public Health, 15(3), 211–212. In Chinese.
Kan, H., & Chen, B. (2003). A case-crossover analysis of air pollution and daily mortality in Shanghai. Journal of Occupational Health, 45(2), 119–124.
Kan, H., London, S. J., Chen, G., Zhang, Y., Song, G., Zhao, N., et al. (2008). Season, sex, age, and education as modifiers of the effects of outdoor air pollution on daily mortality in Shanghai, China: the public health and air pollution in Asia (PAPA) Study. Environmental Health Perspectives, 116(9), 1183–1188.
Kan, H., & Chen, B. (2002). Impact of long-term exposure to air particulate matter on life expectance and survival rate of Shanghai residents. Biomedical and Environmental Sciences, 15(3), 209–214.
Kan, H., London, S., Chen, G., Zhang, Y., Song, G., Zhao, N., et al. (2007). Differentiating the effects of fine and coarse particles on daily mortality in Shanghai, China. Environment International, 33(3), 376–384.
Kappos, A. D., Bruckmann, P., Eikmann, T., Englert, N., Heinrich, U., Hoeppe, P., et al. (2004). Health effects of particles in ambient air. International Journal of Hygiene and Environmental Health, 207(4), 399–407.
Katsouyanni, K., Touloumi, G., Samoli, E., Gryparis, A., Alain, L. T., Monopolis, Y., et al. (2001). Confounding and effect modification in the short-term effects of ambient particles on total mortality: results from 29 European cities within the APHEA2 project. Epidemiology, 12(5), 521–531.
Katsouyanni, K., Touloumi, G., & Samolu, E. (2003). Sensitivity analysis of various models of short-term effects of ambient particles on total mortality in 29 Cities in APHEA2. In revised analyses of time-series of air pollution and health. Special Report (pp. 157–164). Boston: Health Effects Institute.
Krewski, D., Burnett, R., Goldberg, M., Hoover, B. K., Siemiatycki, J., & Jerrett, M. (2000). Reanalysis of the Harvard six cities study and the American Cancer Society study of particulate air pollution and mortality. Cambridge: The Health Effects Institute.
Kunzli, N., Medina, S., Kaiser, R., Quénel, P., Horak, F., & Studnicka, J. M. (2001). Assessment of deaths attributable to air pollution: should we use risk estimate based on time series or on cohort studies? American Journal of Epidemiology, 153(11), 1050–1055.
Laden, F., Neas, L. M., Dockery, D. W., & Schwartz, J. (2000). Association of fine particulate matter from different sources with daily mortality in six U.S. cities. Environmental Health Perspective, 108(10), 941–947.
Lai, S., Zou, S., Cao, J., LEE, S., & HO, K. (2007). Characterizing ionic species in PM2.5 and PM10 in four Pearl River Delta cities, South China. Journal of Environmental Sciences, 19(8), 939–947.
Lee, E. T. (1992). Statistical methods for survival data analysis (2nd ed.). New York: Wiley.
Leksell, I., & Rabl, A. (2001). Air pollution and mortality: quantification and valuation of years of life lost. Risk Analysis, 21(5), 843–857.
Levy, J. I., Carrothers, T. J., Tuomisto, J. T., Hammitt, J. K., & Evans, J. S. (2001). Environmental Health Perspectives, 109(12), 1215–1226.
Liu, S., Hu, M., Slanina, S., He, L., Niu, Y., Bruegemann, E., et al. (2008). Size distribution and source analysis of ionic compositions of aerosols in polluted periods at Xinken in Pearl River Delta (PRD) of China. Atmospheric Environment, 42(25), 6284–6295.
Martuzzi, M., Krzyzanowski, M., & Bertollini, R. (2003). Health impact assessment of air pollution: providing further evidence for public health action. The European Respiratory Journal, 21(40), 86–91.
Medina, S., Plasencia, A., Ballester, F., Mücke, H. G., & Schwartz, J. (2004). APHEIS: public health impact of PM10 in 19 European cities. Journal of Epidemiology and Community Health, 58(10), 831–836.
Neuberger, M., Rabczenko, D., & Moshammer, H. (2007). Extended effects of air pollution on cardiopulmonary mortality in Vienna. Atomospheric Environment, 41(38), 8549–8556.
Nevalainen, J., & Pekkanen, J. (1998). The effect of particulate air pollution on life expectancy. The Science of the Total Environment, 217(11), 137–141.
Niu, Y., He, L., Hu, M., Zhang, J., & Zhao, Y. (2006). Pollution characteristics of atmospheric fine particle and the second component in Winter and Summer at Shenzhen. Science in China Series B-Chemistry, 36(2), 173–180. In Chinese.
Peng, R. D., Chang, H. H., Bell, M. L., McDermott, A., Zeger, S. L., Samet, J. M., et al. (2008). Coarse particulate matter air pollution and hospital admissions for cardiovascular and respiratory diseases among Medicare patients. Journal of the American Medical Association, 299(18), 2172–2179.
Peters, J. M., Avol, E., Navidi, W., London, S. J., Gauderman, J., Lurmann, F., et al. (1999). A study of twelve southern California communities with differing levels and types of air pollution I prevalence of respiratory morbidity. American Journal of Respiratory and Critical Care Medicine, 159(3), 760–767.
Peters, A., Skorkovsky, J., Kotesovec, F., Brynda, J., Spix, C., Wichmann, H. E., et al. (2002). Associations between mortality and air pollution in Center Europe. Environmental Health Perspectives, 108(4), 283–287.
Pope, C. A., Burnett, R. T., Thun, M. J., Calle, E. E., Krewski, D., Ito, K., et al. (2002). Lung cancer, cardiopulmonary mortality, and long-term exposure to fine particulate air pollution. Journal of the American Medical Association, 287(9), 1132–1141.
Pope, C. A., Thun, M. J., Namboodiri, M. M., Dockery, D. W., Evans, J. S., Speizer, F. E., et al. (1995). Particulate air pollution as a predictor of mortality in a prospective study of U.S. adults. American Journal of Respiratory and Critical Care Medicine, 151(3), 669–674.
Qian, Z., He, Q., & Lin, H. (2007a). Association of daily cause-specific mortality with ambient particle air pollution in Wuhan, China. Environmental Research, 105(3), 380–389.
Qian, Z., Chapman, R. S., Hu, W., Wei, F., Korne, L. R., & Zhang, J. (2004). Using air pollution based community clusters to explore air pollution health effects in children. Environment International, 30(5), 611–620.
Qian, Z., He, Q., Lin, H. M., Kong, L., Liao, D., Dan, J., et al. (2007b). Association of daily cause-specific mortality with ambient particle air pollution in Wuhan, China. Environmental Research, 105(3), 380–389.
Ranzi, A., Gambini, M., Spattini, A., Galassi, C., Sesti, D., Bedeschi, M., et al. (2004). Air pollution and respiratory status in asthmatic children: hints for a locally based preventive strategy. AIRE study. European Journal of Epidemiology, 19(6), 567–576.
Samat, J. A., Schwartz, J., Catalano, P. J., & Sub, H. H. (2001). Gaseous pollutants in particulate matter epidemiology: confounders or surrogates? Environmental Health Perspectives, 109(10), 1053–1061.
Schlesselman, J. J., & Collins, J. A. (2003). Evaluating systematic reviews and meta-analysis. Seminars in Reproductive Medicine, 21(1), 95–105.
Stieb, D. M., Judek, S., & Burnett, R. T. (2002). Meta-analysis of time-series studies of air pollution and mortality: effects of gases and particles and the influence of cause of death, age, and season. Journal of the Air & Waste Management Association, 52(4), 470–484.
Sultan, Z. M. (2007). Estimates of associated outdoor particulate matter health risk and costs reductions from alternative building, ventilation and filtration scenarios. The Science of the Total Environment, 377(1), 1–11.
Tang, J., Chen, K., Dong, Y., Zhao, N., & Li, H. (2006). A time-series study on the association of air pollution and mortality in Minhang District, Shanghai. Journal of Environmental and Occupational Medicine, 23(6), 485–487. In Chinese.
Tsai, S. S., Huang, C. H., Goggins, W. B., Wu, T. N., & Yang, C. Y. (2003). Relationship between air pollution and daily mortality in a tropical city: Kaohsiung, Taiwan. Journal of Toxicology and Envrionmental Health, Part A, 66(17), 1341–1349.
Venners, S. A., Wang, B., Peng, Z., Xu, Y., Wang, L., & Xu, X. (2003). Particulate matter, sulfur dioxide, and daily mortality in Chongqing, China. Environmental Health Perspectives, 111(4), 62–567.
Ware, J. H., Ferris, B. G., Dockery, D. W., Spengler, J. D., Stram, D. O., & Speizer, F. E. (1986). Effects of ambient sulfur oxides and suspended particles on respiratory health of preadolescent children. The American Review of Respiratory Disease, 133(5), 834–842.
White, R. H., Stineman, C. H., Symons, J. M., Breysse, P. N., Kim, S. R., Bell, M. L., et al. (2008). Premature mortality in the Kingdom of Saudi Arabia associated with particulate matter air pollution from the 1991 Gulf War. Human and Ecological Risk Assessment, 14(4), 645–664.
Wong, T. W., Lau, T. S., Yu, T. S., Neller, A., Wong, S. L., Tam, W., et al. (1999). Air pollution and hospital admissions for respiratory and cardiovascular diseases in Hong Kong. Occupational and Environmental Medicine, 56(10), 679–683.
Wong, C. M., Ma, S., Hedley, A. J., & Lam, T. H. (2001). Effect of air pollution on daily mortality in Hong Kong. Environmental Health Perspectives, 109(4), 335–340.
Wong, C. M., Vichit-Vadakan, N., Kan, H., & Qian, Z. (2008). Public health and air pollution in Asia (PAPA): a multicity study of short-term effects of air pollution on mortality. Environmental Health Perspectives, 116(9), 1195–1202.
Woodruff, T. J., Grillo, J., & Schoendorf, K. C. (1997). The relationship between selected causes of post-neonatal infant mortality a particulate air pollution in the United States. Environmental Health Perspectives, 105(6), 608–612.
World Health Organization. (2003). Health aspects of air pollution with particulate matter, ozone and nitrogen dioxide. Copenhagen: WHO Regional Office for Europe.
Wu, Y., & Zhang, J. (2009). Interactive effects of particulate matter and temperature on population non-accidental deaths in Being, China. Research of Environmental Science, 22(12), 1403–1410. In Chinese.
Xie, P., Liu, X., Liu, Z., Li, T., & Bai, Y. (2009). Exposure-response functions for health effects of ambient particulate matter pollution applicable for China. China Environmental Science, 29(10), 861–866. In Chinese.
Yorifuji, T., Yamamoto, E., & Tsuda, T. (2005). Health impact assessment of particulate matter in Tokyo, Japan. Archives of Environmental & Occupational Health, 60(4), 179–185.
Yu, B., Lu, H., & Wang, Y. (2006). A time-series study on the association of daily mortality and air pollution in Luwan district, Shanghai, Shanghai. Journal of Preventive Medicine, 18(6), 264–266. In Chinese.
Zanobetti, A., & Schwartz, J. (2009). The effects of fine and coarse particulate air pollution on mortality: a national analysis. Environmental Health Perspectives, 117(6), 898–903.
Zhang, M., Song, Y., & Cai, X. (2007). A health-based assessment of particulate air pollution in urban areas of Beijing in 2000–2004. The Science of the Total Environment, 376(1–3), 100–108.
Zhang, M., Song, Y., Cai, X., & Zhou, J. (2008). Economic assessment of the health effects related to particulate matter pollution in 111 Chinese cities by using economic burden of disease analysis. Journal of Environmental Management, 88(4), 947–954.
Zhang, Y., Zhang, Z., Liu, X., Zhang, X., Feng, B., & Li, H. (2007). Concentration-response relationship between particulate air pollution and daily mortality in Taiyuan. Journal of Peking University Health Science, 39(2), 153–157. In Chinese.
Zhang, Z., Zhong, L., & Xiang, Y. (2005). Regional air monitoring network construction strategy and practice. Environmental Monitoring in China, 21(5), 6–8. In Chinese.
Acknowledgements
This publication supported by the National High Technology Research (863) Program of China (No. 2006AA06A309) and National Basic Research (973) Program of China (No. 2005CB422204). We should give our thanks to the Environmental Monitoring Center of Guangdong Province for providing PM10 and PM2.5 data in PRD. And we also appreciate the health data provided by Hong Kong Health Department.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Xie, P., Liu, X., Liu, Z. et al. Human Health Impact of Exposure to Airborne Particulate Matter in Pearl River Delta, China. Water Air Soil Pollut 215, 349–363 (2011). https://doi.org/10.1007/s11270-010-0483-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11270-010-0483-0