
Abstract
The highly pathogenic avian influenza H5N1 viruses usually cause severe diseases and high mortality in infected humans. However, the tissue tropism and underlying pathogenesis of H5N1 virus infection in humans have not been clearly elucidated yet. In this study, an autopsy was conducted to better understand H5N1 virus distributions in tissues of infected humans, and whether H5N1 virus can replicate in extrapulmonary tissues. We found that the lungs had the higher viral load than the spleen, whereas no detectable viruses in tissues of heart, liver, kidney, large intestine, small intestine, or brain. Specifically, the viral load was higher in the left lung (7.1 log10 copies per ml) in relation to the right lung (5.7 log10 copies per ml), resulting in more severe pathological damage in the left lung, and lung tissues contained both positive- and negative-stranded viral RNA. However, there existed a low level of H5N1 viruses in the spleen (3.8 log10 copies per ml), with the absence of positive-stranded viral RNA. Our results indicate that replication of H5N1 viruses mainly occurs in the lungs, and the degree of lung damage is highly correlated with the viral load in the lungs. The low-load viruses in the spleen might be introduced through blood circulation or other ways.
Similar content being viewed by others


Introduction
The highly pathogenic avian influenza H5N1 viruses could replicate systemically in a variety of organs in poultry, such as respiratory tract, intestine, and spleen, affecting these organs, even the central nervous system [1–4]. H5N1 viruses could also cause disseminated infections in either naturally or experimentally infected mammalian species, i.e., tiger, leopard, and ferret [5–10]. However, evidence for extrapulmonary replication of H5N1 viruses in humans, in general, has been lacking at present. Some studies had found H5N1 viruses exclusively in respiratory tract (mainly in lung) [11, 12]. Other studies had found the presence of H5N1 viruses in many extrapulmonary organs, such as intestine, liver, and brain, which indicated that virus dissemination seems to occur in some humans through blood circulation or other ways [13–17]. In March 2006, the first case of avian influenza H5N1 virus infection was identified in Guangdong province of China. An autopsy was then conducted to detect the virus distribution and load, which, we hoped, would provide some insights into H5N1 infection and replication in both pulmonary and extrapulmonary organs.
Materials and methods
Patient and virologic diagnosis
A thirty-six-year-old male patient, who had a 4-day history of discomfort of fever, throat pain, and dry cough, was admitted to hospital on February 26, 2006. A chest radiograph obtained on admission showed evidence of left lower pneumonia. His condition was rapidly deteriorated, featured by consecutive high body temperature and dysfunctions of multiple systems, including respiratory system, circulatory system, central nervous system, liver, kidney, and gastrointestinal system. Chest radiograph revealed a massive consolidation shadow in both lungs on February 28, which, however, was much more severe in the left lung. Despite active treatment, the patient finally died from adult respiratory distress syndrome (ARDS) complicated with multiple organ failure (MOF) on March 2. None of the anti-influenza drugs, such as oseltamivir or amantadine, were used in the treatment.
This patient had been to the market where live chickens were slaughtered for sale 1 week prior to onset of symptoms, so the patient’s tracheal aspirates were detected for H5N1 viral RNA using H5N1 real-time RT-PCR Kit (PG Biotech, China) on March 1. The full-length gene segments of hemagglutinin (HA) and neuraminidase (NA) were amplified by using one-step RT-PCR Kit (Qiagen, Germany) with the specific primer pairs (HA-F 5′-AGCAAAAGCAGGGGTTCAAT-3′, HA-R 5′-AGTAGAAACAAGGGTGTTTT-3′; NA-F 5′-AGCAAAAGCAGGAGTTCAAA-3′, NA-R 5′-AGTAGAAACAAGGAGTTTTTTT-3′), the reaction was subjected to a pre-cycle condition consisting of 30 min at 50°C(for reverse transcription), 15 min at 95°C followed by 25 circles of amplification. Each cycles consisted of 94°C for 30 s, 50°C for 30 s, and 72°C for 1 min 45 s. The amplification ended with a final extension at 72°C for 10 min. The PCR products were purified and cloned into the pGEM-T vector (Promega, USA). The positive clones were sequenced with T7 and SP6 primers by a 3730 automated DNA sequencer (ABI, USA).
Analysis of viral load and replication in autopsy specimens
On March 4, 2006, an autopsy was carried out in Zhongshan School of Medicine, Sun Yat-sen University. Tissues of the left lung, right lung, brain, heart, spleen, liver, kidney, large intestine, and small intestine were obtained, respectively. Some specimens were used for pathological analysis, and the remaining was stored at −80°C in small pieces for future study.
The obtained tissues were minced on ice with presence of culture medium, which were then centrifuged at the speed of 1,500 rpm for 15 min at 4°C. Supernatant was collected and added into lysis buffer of QIAamp Viral RNA Kit (Qiagen, Germany). RNA was then extracted according to the manufacturer protocol. Viral RNA was detected using H5N1 real-time RT-PCR Kit (PG Biotech, China) on ABI 7000 Real-Time PCR System (ABI, USA). Standard curve was used in the quantitative analysis of H5N1 RNA isolated from the autopsy tissues. In our study, the preparation of reagents, nucleic acids extraction, and nucleic acid amplification were performed in three physically separated laboratories.
To analyse viral replication in autopsy tissues, strand-specific RT-PCR was performed with H5 specific primer pairs H5F (5′-GCCATTCCACAACATACACCC-3′, 943–963) and H5R (5′-CTCCCCTGCTCATTGCTATG-3′, 1158–1139). Briefly, two-step reactions were used. First, RT reaction was done in the presence of the primer H5F or H5R. cDNA products then underwent PCR with H5F and H5R. The amplified fragment was about 216 bp and detected by agarose gel electrophoresis.
Results
Real-time RT-PCR had revealed H5N1 viral RNA in the patient’s tracheal aspirates. HA and NA gene sequences amplified were the most related to those of avian influenza H5N1 viruses, Duck/Guangxi/5165/05 and Duck/Hunan/1265/05 (99.5 and 99.1% homologous, respectively). Therefore the patient was identified as avian influenza H5N1 virus infected.
Real-time RT-PCR had detected H5N1 viral RNA in the lungs and spleen, whereas there was no detectable viral RNA in tissues of heart, liver, kidney, large intestine, small intestine, or brain. Specifically, the viral load was higher in the left lung (7.1 log10 copies per ml) in relation to the right lung (5.7 log10 copies per ml); and there existed a lower level of H5N1 viruses in the spleen (3.8 log10 copies per ml) (Fig. 1). To confirm a successful H5N1 viral RNA isolation from the autopsy tissues, GAPDH mRNA amplified using RT-PCR served as the internal reference in our study (data not shown). At the same time negative controls did not produce H5 genes, which suggests there is no cross contamination in RT-PCR amplification.

Interpretation of H5N1 influenza viral RNA in autopsy tissues by single real-time RT-PCR. Different load of H5N1 influenza viral RNA existed in the left lung, right lung, and spleen
To further elucidate whether H5N1 viral RNA in the lungs and spleen was H5N1 genome RNA, or alternatively, was replicated by H5N1 viruses, we performed strand-specific RT-PCR amplification. Our results indicated that negative- and positive-stranded RNA were detectable in both the left and the right lung, but there was only negative-stranded RNA in the spleen (Fig. 2). An independent duplication RT-PCR was performed under the same condition to confirm the result.

Detection of positive- and negative-stranded viral RNA in the lungs and spleen by strand-specific RT-PCR. M DNA mark, − Negative-stranded RNA, + Positive-stranded RNA, Neg Negative control
Discussion
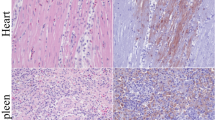
In our study, a high viral load was detected only in the lungs in which both positive- and negative-stranded RNA coexisted, which was consistent with previous findings that replication of H5N1 viruses mainly occurs in the lungs of humans and mammals [18–20]. In line with the finding that the viral load was higher in the left lung in relation to the right lung, a chest radiograph obtained on admission showed evidence of left lower pneumonia, and histopathological analysis of the autopsy specimens had also suggested more severe pathological damage of the left lung, featured by more severe alveolar damage and diffuse exudation [21]. These results had demonstrated that the viral load in the lungs was related to the degree of lung damage. However, whether the observed damage was a direct result of the viral replication or a consequence of the dysfunction of cytokines and chemokines induced by these high-load viruses were still unclear.
Previous studies had shown that avian influenza H5N1 viruses could also target immune organs, in addition to the lung [22, 23]. In our study, a low viral load was detected in the spleen, but with absence of positive-stranded H5N1 viral RNA. Influenza viruses contain negative-stranded RNA, and they first replicate positive-strand RNA, which served as mRNA and the template for genome replication of progeny virus. In our study no positive-stranded viral RNA was detected, which suggested that the H5N1 virus did not replicate in the spleen, or that only little replication occurred [24]. The H5N1 viruses of low load in the spleen might be introduced through blood circulation or other ways.
When compared with that of the human- or swine-derived influenza viruses, NA activity of the avian influenza viruses is more resistant to the low pH environment in the upper digestive tract [25, 26]. Accordingly, the highly pathogenic avian influenza H5N1 viruses can replicate in human intestine, resulting in gastrointestinal symptoms, so that H5N1 viruses were detected in the intestine of infected humans [24, 27, 28]. Clinical data had suggested that the patient presented gastrointestinal symptoms in early stages of disease progression, which finally developed into gastrointestinal dysfunctions. But viral RNA was detected neither in large intestine nor small intestine in our study. Some literature suggested that antiviral drugs can lower the level of viral replication and interfere with the detection of viruses in the examined tissues [24, 29]. However, none of the anti-influenza drugs, such as oseltamivir or amantadine, were used in the treatment.
The HA cleavage site of highly pathogenic H5N1 viruses contains multiple basic amino acids, which could be hydrolyzed by a broader range of cellular proteases, so that the tissue tropism for H5N1 viruses is not restricted to the lungs, but extends to other organs, including the brain [30, 31]. A boy confirmed as H5N1 infected presented with severe diarrhea and acute encephalitis symptoms, and H5N1 virus was isolated from patient’s throat, serum, feces, and the cerebrospinal fluid [32]. In addition to lung tissues, some studies had detected both positive- and negative-stranded RNA in large intestine, small intestine, and liver, suggesting the possibility of viral replication in the intestines and liver [15, 24]. Furthermore, viral gene sequences and antigen were detectable in neurons of the brain, T cells of the lymph node, and Hofbauer cells of the placenta, which was indicative of viral replication in extrapulmonary tissues [29]. The H5N1 virus obtained from the patient has multiple basic amino acids at the HA cleavage site, which has molecular characteristics of the highly pathogenic avian influenza viruses [33]. The viral RNA was detectable in the patient’s lung and spleen in our study. These findings suggested that H5N1 viruses might be transmitted to extrapulmonary tissues, causing disseminate infection. However, viral distribution and replication vary to a certain extent from individual to individual, which might be explained by tissue tropism differences of viral strains, or that viral distribution might differ in different stages of disease progression, or that different individuals reacted differently to H5N1 viruses.
The autopsy tissues of H5N1 infected cases can often not be obtained due to various reasons (e.g. religion), so reports concerning the tissue tropism and distribution of H5N1 viruses are lacking. We studied H5N1 viral load and replication in autopsy tissues, and the relationship between the viral load and tissue damage, which had significant implication for the further investigation of the tissue tropism and pathogenesis of H5N1 viruses.
References
J. Liu, H. Xiao, F. Lei, Q. Zhu, K. Qin, X.W. Zhang, X.L. Zhang, D. Zhao, G. Wang, Y. Feng, J. Ma, W. Liu, J. Wang, G.F. Gao, Science 309, 1206 (2005). doi:https://doi.org/10.1126/science.1115273
J.P. Teifke, R. Klopfleisch, A. Globig, E. Starick, B. Hoffmann, P.U. Wolf, M. Beer, T.C. Mettenleiter, T.C. Harder, Vet. Pathol. 44, 137–143 (2007). doi:https://doi.org/10.1354/vp.44-2-137
C.O. Aiki-Raji, P.V. Aguilar, Y.K. Kwon, S. Goetz, D.L. Suarez, A.I. Jethra, O. Nash, C.A. Adeyefa, F.D. Adu, D. Swayne, C.F. Basler, Emerg. Infect. Dis. 14, 1753–1755 (2008). doi:https://doi.org/10.3201/eid1411.080557
H. Chen, G. Deng, Z. Li, G. Tian, Y. Li, P. Jiao, L. Zhang, Z. Liu, R.G. Webster, K. Yu, Proc. Natl. Acad. Sci. USA 101, 10452–10457 (2004). doi:https://doi.org/10.1073/pnas.0403212101
H. Tanaka, C.H. Park, A. Ninomiya, H. Ozaki, A. Takada, T. Umemura, H. Kida, Vet. Microbiol. 95, 1–13 (2003). doi:https://doi.org/10.1016/S0378-1135(03)00132-9
C.H. Park, M. Ishinaka, A. Takada, H. Kida, T. Kimura, K. Ochiai, T. Umemura, Arch. Virol. 147, 1425–1436 (2002). doi:https://doi.org/10.1007/s00705-001-0750-x
J. Keawcharoen, K. Oraveerakul, T. Kuiken, R.A. Fouchier, A. Amonsin, S. Payungporn, S. Noppornpanth, S. Wattanodorn, A. Theambooniers, R. Tantilertcharoen, R. Pattanarangsan, N. Arya, P. Ratanakorn, D.M. Osterhaus, Y. Poovorawan, Emerg. Infect. Dis. 10, 2189–2191 (2004)
T.R. Maines, X.H. Lu, S.M. Erb, L. Edwards, J. Guarner, P.W. Greer, D.C. Nguyen, K.J. Szretter, L.M. Chen, P. Thawatsupha, M. Chittaganpitch, S. Waicharoen, D.T. Nguyen, T. Nguyen, H.H. Nguyen, J.H. Kim, L.T. Hoang, C. Kang, L.S. Phuong, W. Lim, S. Zaki, R.O. Donis, N.J. Cox, J.M. Katz, T.M. Tumpey, J. Virol. 79, 11788–11800 (2005). doi:https://doi.org/10.1128/JVI.79.18.11788-11800.2005
E.A. Govorkova, J.E. Rehg, S. Krauss, H.L. Yen, Y. Guan, M. Peiris, T.D. Nguyen, T.H. Hanh, P. Puthavathana, H.T. Long, C. Buranathai, W. Lim, R.G. Webster, E. Hoffmann, J. Virol. 79, 2191–2198 (2005)
H.L. Chen, Y.B. Li, Z.J. Li, J.Z. Shi, K. Shinya, G.H. Deng, Q.L. Qi, G.B. Tian, S.F. Fan, H.D. Zhao, Y.X. Sun, Y. Kawaoka, J. Virol. 80, 5976–5983 (2006). doi:https://doi.org/10.1128/JVI.00110-06
J.S. Peiris, W.C. Yu, C.W. Leung, C.Y. Cheung, W.F. Ng, J.M. Nicholls, T.K. Ng, K.H. Chan, S.T. Lai, W.L. Lim, K.Y. Yuen, Y. Guan, Lancet 363, 617–619 (2004). doi:https://doi.org/10.1016/S0140-6736(04)15595-5
K.F. To, P.K. Chan, K.F. Chan, W.K. Lee, W.Y. Lam, K.F. Wong, N.L. Tang, D.N. Tsang, R.Y. Sung, T.A. Buckley, J.S. Tam, A.F. Cheng, J. Med. Virol. 63, 242–246 (2001). doi:https://doi.org/10.1002/1096-9071(200103)63:3<242::AID-JMV1007>3.0.CO;2-N
S. Chutinimitkul, P. Bhattarakosol, S. Srisuratanon, A. Eiamudomkan, K. Kongsomboon, S. Damrongwatanapokin, A. Chaisingh, K. Suwannakarn, T. Chieochansin, A. Theamboonlers, Y. Poovorawan, Emerg. Infect. Dis. 12, 1041–1043 (2006)
J.H. Beigel, J. Farrar, A.M. Han, F.G. Hayden, R. Hyer, M.D. de Jong, S. Lochindarat, T.K. Nguyen, T.H. Nguyen, T.H. Tran, A. Nicoll, S. Touch, K.Y. Yuen, N. Engl. J. Med. 353, 1374–1385 (2005). doi:https://doi.org/10.1056/NEJMra052211
M. Uiprasertkul, R. Kitphati, P. Puthavathana, R. Kriwong, A. Kongchanagul, K. Ungchusak, S. Angkasekwinai, K. Chokephaibulkit, K. Srisook, N. Vanprapar, P. Auewarakul, Emerg. Infect. Dis. 13, 708–712 (2007)
M.D. de Jong, C.P. Simmons, T.T. Thanh, V.M. Hien, G.J. Smith, T.N. Chau, D.M. Hoang, N.V. Chau, T.H. Khanh, V.C. Dong, P.T. Qui, B.V. Cam, Q. Ha do, Y. Guan, J.S. Peiris, N.T. Chinh, T.T. Hien, J. Farrar, Nat. Med. 17, 1203–1207 (2006). doi:https://doi.org/10.1038/nm1477
A.N. Abdel-Ghafar, T. Chotpitayasunondh, Z. Gao, F.G. Hayden, D.H. Nguyen, M.D. de Jong, A. Naghdaliyev, J.S. Peiris, N. Shindo, S. Soeroso, T.M. Uyeki, N. Engl. J. Med. 358, 261–273 (2008). doi:https://doi.org/10.1056/NEJMra0707279
K. Shinya, M. Ebina, S. Yamada, M. Ono, N. Kasai, Y. Kawaoka, Nature 440, 435–436 (2006). doi:https://doi.org/10.1038/440435a
D. van Riel, V.J. Munster, E. de Wit, G.F. Rimmelzwaan, R.A. Fouchier, A.D. Osterhaus, T. Kuiken, Science 312, 399 (2006). doi:https://doi.org/10.1126/science.1125548
D. van Riel, V.J. Munster, E. de Wit, G.F. Rimmelzwaan, R.A. Fouchier, A.D. Osterhaus, T. Kuiken, Am. J. Pathol. 171, 1215–1223 (2007)
H.L. Jing, J.D. Cheng, J.M. Zhang, Chin. J. Forensic Med. 23, 126–127 (2008)
T.M. Tumpey, X. Lu, T. Morken, S.R. Zaki, J.M. Katz, J. Virol. 74, 6105–6116 (2000). doi:https://doi.org/10.1128/JVI.74.13.6105-6116.2000
C. Antarasena, R. Sirimujalin, P. Prommuang, S.D. Blacksell, N. Promkuntod, P. Prommuang, Avian Pathol. 35, 250–253 (2006). doi:https://doi.org/10.1080/03079450600714510
M. Uiprasertkul, P. Puthavathana, K. Sangsiriwut, P. Pooruk, K. Srisook, M. Peiris, J.M. Nicholls, K. Chokephaibulkit, N. Vanprapar, P. Auewarakul, Emerg. Infect. Dis. 11, 1036–1041 (2005)
T. Suzuki, T. Takahashi, C.T. Guo, K.I. Hidari, D. Miyamoto, H. Goto, Y. Kawaoka, Y. Suzuki, J. Virol. 79, 11705–11715 (2005). doi:https://doi.org/10.1128/JVI.79.18.11705-11715.2005
G. Neumann, Y. Kawaoka, Emerg. Infect. Dis. 12, 881–886 (2006)
A. Apisarnthanarak, R. Kitphati, K. Thongphubeth, P. Patoomanunt, P. Anthanont, W. Auwanit, P. Thawatsupha, M. Chittaganpitch, S. Saeng-Aroon, S. Waicharoen, P. Apisarnthanarak, G.A. Storch, L.M. Mundy, V.J. Fraser, Emerg. Infect. Dis. 10, 1321–1324 (2004)
P. Buchy, S. Mardy, S. Vong, T. Toyoda, J.T. Aubin, M. Miller, S. Touch, L. Sovann, J.B. Dufourcq, B. Richner, P.V. Tu, N.T. Tien, W. Lim, J.S. Peiris, W.S. Vander, J. Clin. Virol. 39, 164–168 (2007). doi:https://doi.org/10.1016/j.jcv.2007.04.010
J. Gu, Z. Xie, Z. Gao, J. Liu, C. Korteweg, J. Ye, L.T. Lau, J. Lu, Z. Gao, B. Zhang, M.A. McNutt, M. Lu, V.M. Anderson, E. Gong, A.C. Yu, W.I. Lipkin, Lancet 370, 1137–1145 (2008). doi:https://doi.org/10.1016/S0140-6736(07)61515-3
T. Horimoto, Y. Kawaoka, Clin. Microbiol. Rev. 14, 129–149 (2001). doi:https://doi.org/10.1128/CMR.14.1.129-149.2001
A. Gambotto, S.M. Barratt-Boyes, M.D. de Jong, G. Neumann, Y. Kawaoka, Lancet 371, 1464–1475 (2007). doi:https://doi.org/10.1016/S0140-6736(08)60627-3
M.D. de Jong, V.C. Bach, T.Q. Phan, M.H. Vo, T.T. Tran, B.H. Nguyen, M. Beld, T.P. Le, H.K. Truong, V.V. Nguyen, T.H. Tran, Q.H. Do, J. Farrar, N. Engl. J. Med. 352, 686–691 (2005). doi:https://doi.org/10.1056/NEJMoa044307
J.J. Zhou, J. Fu, D.Y. Fang, H.J. Yan, J. Tian, J.M. Zhou, J.P. Tao, Y. Liang, L.F. Jiang, Arch. Virol. 152, 1515–1521 (2007). doi:https://doi.org/10.1007/s00705-007-0985-2
Acknowledgments
This study was supported by the Science and Technology Project of Guangdong province (grant no 2005A20901005, 2006B21101003), the Natural Science Foundation of Guangdong province (grant no 50111-4203005).
Author information
Authors and Affiliations
Corresponding author
Additional information
Jing-Jiao Zhou and Dan-Yun Fang equally contributed to this work.
Rights and permissions
About this article
Cite this article
Zhou, JJ., Fang, DY., Fu, J. et al. Infection and replication of avian influenza H5N1 virus in an infected human. Virus Genes 39, 76–80 (2009). https://doi.org/10.1007/s11262-009-0365-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11262-009-0365-y