
Abstract
Objective
To quantificationally illustrate the impact of ischemia time (IT) on renal function decline after partial nephrectomy (PN), especially for patients with compromised baseline renal function (estimated glomerular filtration rate [eGFR] < 90 mL/min/1.73 m2).
Methods
Patients undergoing PN during 2014–2021 from a prospectively maintained database were reviewed. Propensity score matching (PSM) was employed to balance the possible covariates between patients with or without baseline compromised renal function. Specifically, the relationship of IT with postoperative renal function was illustrated. Two machine learning methods (logistic least absolute shrinkage and selection operator [LASSO] logistic regression and random forest) were applied to quantify the relative impact of each covariables.
Results
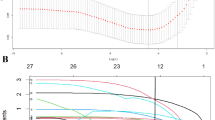
The average drop percent of eGFR was -10.9% (− 12.2%, − 9.0%). Multivariable Cox proportional regression and linear regression analyses identified five risk factors for renal function decline, namely RENAL Nephrometry Score (RNS), age, baseline eGFR, diabetes and IT (all p < 0.05). Specifically, the relationship of IT with postoperative functional decline emerged as non-linear, with an increase from 10–30 min and a plateau afterwards among patients with normal function (eGFR ≥ 90 mL/min/1.73 m2), whereas with an increase from 10 to 20 min and a plateau afterwards among patients with compromised function (eGFR < 90 mL/min/1.73 m2). Furthermore, the coefficient’s path and random forest analysis revealed that the top two most important features were RNS and age.
Conclusion
IT exhibits the secondarily non-linear relationship with postoperative renal function decline. Patients with compromised baseline renal function are less tolerant to ischemia damage. The use of a single cut-off interval of IT in the setting of PN is flawed.



Similar content being viewed by others


Data availability
Request from corresponding author with proper reasons.
References
Campbell SC et al (2021) Renal mass and localized renal cancer: evaluation, management, and follow-up: AUA guideline: part I. J Urol 206(2):199–208
Antonelli A et al (2018) Role of clinical and surgical factors for the prediction of immediate, early and late functional results, and its relationship with cardiovascular outcome after partial nephrectomy: results from the prospective multicenter RECORd 1 project. J Urol 199(4):927–932
Antonelli A et al (2022) Prediction of significant renal function decline after open, laparoscopic, and robotic partial nephrectomy: external validation of the Martini’s nomogram on the RECORD2 project cohort. Int J Urol 29(6):525–532
Jin D et al (2022) Development and validation of an integrated nomogram to predict personalized new baseline functional outcomes after partial nephrectomy. Transl Androl Urol 11(1):9–19
Crocerossa F et al (2022) Estimated glomerular filtration rate decline at 1 year after minimally invasive partial nephrectomy: a multimodel comparison of predictors. Eur Urol Open Sci 38:52–59
Pecoraro A et al (2023) Estimating postoperative renal function after surgery for nonmetastatic renal masses: a systematic review of available prediction models. Eur Urol Oncol. https://doi.org/10.1016/S0302-2838(23)01046-1
Carrion DM, Aguilera Bazán A, Martínez-Piñeiro L (2020) Re: do patients with stage 3–5 chronic kidney disease benefit from ischaemia-sparing techniques during partial nephrectomy? Eur Urol 78(4):629–630
Abdel Raheem A et al (2022) Warm ischemia time length during on-clamp partial nephrectomy: does it really matter? Minerva Urol Nephrol 74(2):194–202
Antonelli A et al (2022) Is off-clamp robot-assisted partial nephrectomy beneficial for renal function? Data from the CLOCK trial. BJU Int 129(2):217–224
Bessede T et al (2015) Are warm ischemia and ischemia time still predictive factors of poor renal function after partial nephrectomy in the setting of elective indication? World J Urol 33(1):11–15
Lee H et al (2018) Impact of warm ischaemia time on postoperative renal function after partial nephrectomy for clinical T1 renal cell carcinoma: a propensity score-matched study. BJU Int 121(1):46–52
Xiong L et al (2022) What happens to the preserved renal parenchyma after clamped partial nephrectomy? Eur Urol 81(5):492–500
Campbell SC et al (2023) Every decade counts: a narrative review of functional recovery after partial nephrectomy. BJU Int 131(2):165–172
Anderson BG et al (2019) comparing off-clamp and on-clamp robot-assisted partial nephrectomy: a prospective randomized trial. Urology 126:102–109
Campbell SC, Yasuda Y (2022) Off-clamp partial nephrectomy: level 1 data regarding real-world utility (or futility). BJU Int 129(2):131–132
Bravi CA et al (2021) Toward individualized approaches to partial nephrectomy: assessing the correlation between ischemia time and patient health status (RECORD2 project). Eur Urol Oncol 4(4):645–650
Abushamma F et al (2021) Global analysis of research trends on kidney function after nephron-sparing surgery: a bibliometric and visualised study. Cancer Manag Res 13:7479–7487
Chung JS et al (2021) Impact of short warm ischemic time on longitudinal kidney function and survival rate after partial nephrectomy for renal cell carcinoma in patients with pre-existing chronic kidney disease stage III: a multi-institutional propensity score-matched study. Eur J Surg Oncol 47(2):470–476
Dagenais J et al (2019) “At-risk” kidney: how surgical factors influence renal functional preservation after partial nephrectomy. Int J Urol 26(5):565–570
Ebbing J et al (2019) Outcome of kidney function after ischaemic and zero-ischaemic laparoscopic and open nephron-sparing surgery for renal cell cancer. BMC Nephrol 20(1):40
Ishiyama Y et al (2021) Limited impact of warm ischemic threshold for partial nephrectomy in the robotic surgery era: a propensity score matching study. Int J Urol 28(12):1219–1225
Ma YC et al (2006) Modified glomerular filtration rate estimating equation for Chinese patients with chronic kidney disease. J Am Soc Nephrol 17(10):2937–2944
Zargar H et al (2015) The impact of extended warm ischemia time on late renal function after robotic partial nephrectomy. J Endourol 29(4):444–448
Nahar B, Bhat A, Parekh DJ (2019) Does every minute of renal ischemia still count in 2019? Unlocking the chains of a flawed thought process over five decades. Eur Urol Focus 5(6):939–942
Volpe A et al (2015) Renal ischemia and function after partial nephrectomy: a collaborative review of the literature. Eur Urol 68(1):61–74
Dong W et al (2018) Ischemia and functional recovery from partial nephrectomy: refined perspectives. Eur Urol Focus 4(4):572–578
Campi R et al (2022) Impact of frailty on perioperative and oncologic outcomes in patients undergoing surgery or ablation for renal cancer: a systematic review. Minerva Urol Nephrol 74(2):146–160
Choi JD et al (2010) Renal damage caused by warm ischaemia during laparoscopic and robot-assisted partial nephrectomy: an assessment using Tc 99m-DTPA glomerular filtration rate. Eur Urol 58(6):900–905
Choi JD et al (2012) Does prolonged warm ischemia after partial nephrectomy under pneumoperitoneum cause irreversible damage to the affected kidney? J Urol 187(3):802–806
Kumar RK et al (2014) Robot-assisted partial nephrectomy in patients with baseline chronic kidney disease: a multi-institutional propensity score-matched analysis. Eur Urol 65(6):1205–1210
Lane BR et al (2010) Performance of the chronic kidney disease-epidemiology study equations for estimating glomerular filtration rate before and after nephrectomy. J Urol 183(3):896–901
Karabay E et al (2021) Identifying the predictors of estimated glomerular filtration rate after partial nephrectomy with a nonlinear regression model. Int J Clin Pract 75(3):e13763
Author information
Authors and Affiliations
Contributions
Data acquisition: XL, DJ. Statistical analysis: DJ and SZ. Data analysis and interpretation: DJ, YZ. Drafting of the manuscript: DJ, YZ. Critical revision of the manuscript: YZ and XL. Administrative, technical, or material support: YZ and DJ. Supervision: SZ and YZ. Approval of the final manuscript: SZ.
Corresponding author
Ethics declarations
Conflict of interest
All authors have completed the ICMJE uniform disclosure form. The authors have no conflicts of interest to declare.
Ethical approval
The authors are accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. The study was conducted in accordance with the Declaration of Helsinki (as revised in 2013). This study was approved by the Institutional Review Board of the Army Medical Center Ethical Committee and registered on Chinese Clinical Trial Registry (ChiCTR2300069180).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
11255_2023_3630_MOESM2_ESM.jpg
Supplementary file2 a. Propensity score test demonstrating standardized bias before and after PSM. b. Propensity score graph demonstrating distribution of on- or off-support patients. RNS: RENAL nephrometry score; CVD: cardiovascular disease. (JPG 374 KB)
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

{kind=link}
Cite this article
Liu, X., Jin, D., Zhang, Y. et al. Limited non-linear impact of warm ischemia time on renal functional decline after partial nephrectomy: a propensity score-matched study. Int Urol Nephrol 55, 1699–1708 (2023). https://doi.org/10.1007/s11255-023-03630-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-023-03630-0