
Abstract
Purpose
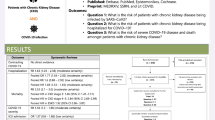
The COVID-19 pandemic may have an impact on the long-term kidney function of survivors. The clinical relevance is not clear.
Methods
This review summarises the currently published data.
Results
There is a bidirectional relationship between chronic kidney disease and COVID-19 disease. Chronic kidney diseases due to primary kidney disease or chronic conditions affecting kidneys increase the susceptibility to COVID-19 infection, the risks for progression and critical COVID-19 disease (with acute or acute-on-chronic kidney damage), and death. Patients who have survived COVID-19 face an increased risk of worse kidney outcomes in the post-acute phase of the disease. Of clinical significance, COVID-19 may predispose surviving patients to chronic kidney disease, independently of clinically apparent acute kidney injury (AKI). The increased risk of post-acute renal dysfunction of COVID-19 patients can be graded according to the severity of the acute infection (non-hospitalised, hospitalised or ICU patients). The burden of chronic kidney disease developing after COVID-19 is currently unknown.
Conclusion
Post-acute COVID-19 care should include close attention to kidney function. Future prospective large-scale studies are needed with long and complete follow-up periods, assessing kidney function using novel markers of kidney function/damage, urinalysis and biopsy studies.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Post-COVID-19 conditions are defined as a heterogeneous clinical syndrome of new onset, returning or ongoing symptoms after COVID-19. According to the WHO definition, they “occur in individuals with a history of a probable or confirmed COVID-19 infection, usually 3 months from the onset, with symptoms lasting at least 2 months, which cannot be explained by an alternative diagnosis” [1]. Post-COVID-19 conditions include a broad spectrum of health problems such as (a) long-COVID-19, which consists of a wide range of symptoms that can last weeks or months; (b) multi-organ effects of COVID-19, affecting predominantly cardiovascular, pulmonary, renal and neuropsychiatric organ systems; and (c) effects of COVID-19 treatment/ hospitalisation (post-intensive care syndrome). Post-COVID-19 conditions are found more often in patients who had critical COVID-19 or in people not vaccinated against COVID-19 [2].
About 10 to 20% of people infected by the COVID-19 virus experience post-COVID-19 conditions. Longitudinal studies indicate that 80–85% of patients with post-COVID-19 report persistence of symptoms after 12 months of follow-up [3, 4]. Given that post-COVID syndrome is relatively new, its natural history and the range of effects are not fully understood.
The objective of this narrative review is to summarise evidence on the interplay between chronic kidney disease (CKD) and COVID-19, both during active COVID-19 infection as well as post-COVID-19. Furthermore, it focusses on potential synergistic effects of the interplay between the two diseases and major common pathways.
Chronic kidney disease and COVID-19
A systematic review and meta-analysis synthesising the incidence and outcomes of COVID-19 patients with CKD from 348 studies suggested that COVID-19 disproportionally affected people with CKD. The incidence of COVID-19 was higher in patients receiving maintenance dialysis than in those with CKD not requiring kidney replacement therapy or those who had received kidney or pancreas/kidney transplants [5]. Patients with CKD were at higher risk than patients with congestive heart failure or type 2 diabetes mellitus [6, 7].
However, reported incidence rates of COVID-19 differ considerably between studies. Some studies included all patients who were diagnosed with COVID-19, whereas others included only those who were hospitalised. Hospitalised patient cohorts had different risk factor profiles than general population cohorts. The criteria used to identify infected patients differed between studies (clinical suspicion vs. PCR test on a nasopharyngeal swab). Finally, there were considerable variations in reporting kidney function parameters and in the methods used for assessing kidney function. Nevertheless, numerous cohort studies found a higher prevalence of CKD in hospitalised COVID-19 patients, compared with the general population.
CKD may increase the risk of COVID-19 both directly (susceptibility) and indirectly (exposure related to receiving medical care outside the home, such as dialysis). Known susceptibility factors include altered immune cell function in the pre-/uremic state, loss of antibodies and complement through damaged glomeruli, systemic inflammation and immunosuppressive medications.
Underlying CKD has been recognised as a risk factor for admission to hospital and severe COVID-19 disease [8,9,10]. Amongst 4.264 critically ill adults with COVID-19 admitted to 68 ICUs across the United States, 143 dialysis patients had a shorter time from symptom onset to ICU admission, compared with 521 non-dialysis dependent CKD patients or 3600 patients without pre-existing CKD [11]. An analysis of the international Health Outcome Predictive Evaluation of COVID-19 (HOPE COVID-19) evaluated the impact of renal function (eGFR) at admission on the clinical course of COVID-19 in 758 patients. Patients with kidney dysfunction (eGFR < 60 ml/min) upon hospital admission had a higher incidence of multi-organ failure, such as sepsis, respiratory failure, and AKI [12]. An early meta-analysis showed that the presence of pre-existing CKD tripled the risk of COVID-19 patients for severe disease [13].
Meta-analyses [5, 14] and nation-wide analyses [7, 15] showed that hospitalised COVID-19 patients with chronic kidney diseases, including CKD stages 3–5, maintenance dialysis and kidney transplantation, had higher mortality rates than COVID patients without CKD. Mohan et al. [16] found that nearly one in six deaths amongst active transplant recipients in the USA in 2020 was attributed to COVID-19, using registry data for waitlisted candidates and kidney transplant recipients. The analyses found high rates of mortality associated with COVID-19 amongst waitlist candidates (24%) and kidney transplant recipients, compared with 2019. The fatality rates of kidney transplant recipients were excessively high (> 30%) in the very early post-transplant period [17, 18]. These observations are corroborated by the OpenSAFELY study, which also emphasised the significance of CKD as an important risk factor for COVID-19 mortality. Estimated hazard ratios from multivariate analysis were 1.33 for CKD with eGFR 30–60, and 2.52 for eGFR < 30 ml/min [7].
COVID-19 and acute kidney damage
COVID-19-associated kidney damage is a heterogeneous syndrome not only regarding exposure and pathophysiology, but also with regard to clinical presentation and the individual patient`s short- and long-term prognosis. Kidney damage in COVID-19 patients is common, and can range from proteinuria, haematuria to acute kidney injury requiring renal replacement therapy (RRT). Low molecular weight proteinuria or haematuria were indicative of subclinical AKI, even in the absence of a concomitant rise in serum creatinine levels or a drop in estimated glomerular filtration rate (eGFR).
Large observational studies from the USA, Europe and Brazil have reported an incidence of COVID-19-associated AKI of 28–34% in all hospitalised patients and 46–77% of patients treated in the intensive care unit. COVID-19 AKI in the intensive care unit (ICU) was generally more severe. [19,20,21,22] The incidence of COVID-19 AKI stages 1, 2 and 3 was 44–66%, 19–20% and 14–34%, respectively, in hospitalised patients, compared with 20–22%. 20–24% and 36–57% in ICU patients. Importantly, patients admitted to the ICU were at risk of AKI onset and progression. An observational study from the UK showed that 36.7% of unwell patients with no AKI or AKI stage 1 progressed to AKI stages 2/3 within 48 h. More than 20 to 30% of the ICU patients required kidney replacement therapy. More severe AKI was associated with high mortality in patients with critical COVID-19 disease [19].
However, ascertaining the true epidemiology of COVID-19 AKI is difficult, owing to differences in health care systems, policies for hospitalisation or assignment levels of ICU admission and case-mix of the populations analysed. Moreover, observational studies are prone to confounding and bias. Many early epidemiological studies of patients with COVID-19 used arbitrary serum creatinine-based definitions of AKI. Urine volume was reported infrequently. The lack of serum creatinine measurements prior to hospital admission often impeded the ability to identify pre-existing chronic kidney disease (CKD) and created challenges for the reliable detection and staging of AKI. Of note, one study in which baseline serum creatinine levels were available reported that 35% of patients with COVID-19 AKI had underlying CKD. The distinction between de novo AKI and AKI superimposed on pre-existing CKD was rarely made. Most observational studies reported the incidence and severity of COVID-19 AKI during the first wave of the pandemic.
Recognised risk factors for COVID-19 AKI were classified into patient demographics (older adults with multiple chronic conditions, male sex, ethnicity), patient characteristics (CKD, diabetes mellitus, hypertension, obesity, cardiac failure), genetic factors (APOL 1 genotype), factors identified at hospitalisation (high respiration rate, hypoxemia, higher inflammatory markers, proteinuria) and factors arising during hospitalisation (sepsis, mechanical ventilation, vasopressor dose, nephrotoxins) [23, 24].
CKD and chronic medical disorders affecting kidney function/structure were identified as most important risk factors for new onset AKI or progressive CKD. In a cohort study from Spain, 21% of COVID-19 patients demonstrated elevated serum creatinine levels at admission, of whom 43.5% had pre-existing CKD [25]. An observational study from Italy found that 22.6% of the hospitalised patients developed AKI, 45% of these showed an acute worsening of CKD [26].
There were significant geographic variations in the reported incidences of AKI. The incidence of AKI in China (5.5%) and in parts of Africa or India was particularly low. [27]. These variations were most likely due to significant differences in patients’ characteristics (less CKD or obesity), hospitalisation rates, access to the ICU, management (traditional Chinese medicine; less mechanical ventilation) and in the assessment of kidney function and definition of AKI.
Currently, most epidemiological studies reported rates of COVID-19-induced AKI during the first wave of the pandemic. However, the incidence of COVID-19-associated AKI has reduced over time, with progressively lower rates of kidney replacement therapy observed in the second and third waves of pandemic [28,29,30,31]. The ISARIC WHO CCP-UK study, a prospective nation-wide cohort study, analysed the rate of AKI and its association with mortality. The study was performed on 85,687 patients admitted to hospitals with COVID-19 between January 2020 and December 2020. The authors reported that peak rates of AKI had fallen from 33.8% but remained at > 20%. [28]. There were several putative reasons for the reduction of AKI rates, including improved recognition of AKI, a move away from restrictive fluid strategies, a reduced rate of invasive mechanical ventilation, introduction of effective therapies and vaccination for COVID-19. However, the relative contribution of different factors has not been studied rigorously.
Histopathology and potential pathophysiological mechanisms of COVID-19-associated kidney damage
Descriptive kidney biopsy studies [32,33,34,35,36] and post-mortem examinations of kidney tissues [34, 35] noted a number of distinct histological findings in COVID-19 patients with kidney damage. This finding underlines the notion that there were multiple causes of AKI. In general, the major pathological, almost universal feature was the presence of acute tubular injury of varying degrees. Acute tubular injury was seen predominantly in critical COVID-19 patients. Case reports and case series individually described glomerular diseases such as collapsing glomerulopathy and focal segmental glomerulosclerosis. Glomerular pathology was associated with proteinuria and restricted to non-ICU patients. The collapsing glomerulopathy had been observed mostly in black patients, and was associated with high-risk APOL1 genotypes. Other examinations of kidney tissue revealed endothelial injury and thrombotic microangiopathy, and pigment nephropathy (rhabdomyolysis) in patients with mild COVID-19-induced kidney damage. Of note, most investigators of injured kidney tissues noted mild chronic changes due to diabetic glomerulosclerosis or hypertensive nephroangiosclerosis.
A detailed discussion of the complex and multifactorial pathophysiology of COVID-19-associated AKI is outside the scope of this clinical review. COVID-19 AKI is often multifactorial in nature and may be due to a variety of interacting mechanisms. The pathophysiology of COVID-19 kidney injury involves both direct effects of COVID-19 on the kidneys as well as mechanisms resulting from a) systemic consequences of the inflammatory response to the viral infection on hemodynamic stability (hypovolemia, sepsis); b) effects of the virus on distant organs (organ crosstalk); and c) therapeutic interventions to manage critical COVID-19 disease (mechanical ventilation, nephrotoxins, inadequate correction of volume depletion).
The COVID-19 virus can directly infect kidney podocytes and proximal tubular cells and via an angiotensin converting enzyme pathway, it can lead to mitochondrial dysfunction, acute tubular necrosis and protein leakage in the Bowman`s capsule. Complement activation, local inflammation and immune cell infiltration have been repeatedly described in patients with COVID-19 AKI. Endothelial dysfunction, microvascular thrombi and pigment nephropathy (rhabdomyolysis) are other potential mechanisms of COVID-19-induced AKI. The pathophysiology of COVID-19-associated AKI resembles—at least in part—AKI due to critical illness (septic AKI).
Currently, the contribution of direct viral infection to the rate of COVID-19 AKI is unknown. High COVID-19 load was found—in most, but not all reports—to be an independent predictor of disease severity and mortality. It may be used to predict the clinical course and prognosis of patients with COVID-19 [37, 38]. Findings of high viral load in patients who had died with AKI suggested a crucial role of virus kidney tissue invasion (renal tropisms) [39]. A retrospective cohort study found that the virus load at admission was associated with AKI stage in a dose-dependent manner in a multivariate logistic regression model adjusted for covariates [40]. Moreover, a higher COVID-19 viral load in urine sediments correlated with an increased incidence of AKI and mortality [41]. The study of Jansen and co-workers [42] aimed to investigate the direct effects of the virus on the kidneys, independently of the systemic effects of COVID-19. The authors studied both COVID-19-infected kidney tissues and a model of infected human-induced pluripotent stem-cell-derived kidney organoids. The results of these investigations suggested that COVID-19 can directly infect kidney cells and induce cell injury with subsequent fibrosis. These data may explain both acute kidney injury and transition to chronic kidney disease in long-COVID-19. Whether or not high COVID-19 virus load is an independent predictor of AKI is uncertain. The data should be interpreted with caution and considered only as trends. There is wide heterogeneity in fluid samples taken at different phases of the COVID-19 virus, and findings concerning the relationship between viral load and disease severity or renal tissue infection are inconclusive.
Transmissibility of the virus, prolonged viability and rapid mutations contributed to the COVID-19 pandemic. Prolonged virus shedding provides the rationale for the strategy to isolate infected patients. In a retrospective cohort study involving adult hospitalised COVID-19 patients, Li and co-workers found that older age was an independent risk factor associated with slow viral decline [43]. However, disease severity (symptomatic disease, need for oxygen replacement) was not significantly associated with slow viral decline.
A small prospective study from Italy focussed on critically ill COVID-19 patients affected by the Delta or Omicron variants of the virus. The authors found a higher incidence of AKI in Omicron ICU patients (38.2%) than in Delta ICU patients (9.7%). However, the study groups were not well matched. The higher number of total comorbidities of Omicron patients may be associated with higher mortality and higher rate of AKI [44].
Population-based studies found that Omicron was associated with less severe COVID-19 disease in the general population despite the high transmissibility and dramatic numbers of infected patients. Vaccination with triple/booster vaccine doses offered additional protection from critical COVID-19 disease [45, 46]. The analyses of the Scottish Renal Registry demonstrated improvements in both hospitalisation and mortality in triple vaccinated patients receiving RRT (dialysis and kidney transplantation) during an era when the Omicron variant was the dominant strain in the general population of Scotland. Whether these changes were due to vaccination, the emergence of the Omicron strain or the administration of antibodies and oral antivirals is unknown [47]. It remains to be seen whether the rate of COVID-19-induced kidney damage can be reduced by vaccination [48].
COVID-19-induced acute kidney damage and outcomes
Systematic reviews have shown that kidney damage remains a common extrapulmonary manifestation of critical COVID-19. AKI was associated with increased severity of illness, prolonged duration of hospitalisation and poor prognosis, irrespective of the severity of the COVID-19 disease and renal function prior to hospital admission. COVID-19-associated AKI was associated with increased mortality even at stage 1 [49]. The burden of CKD following COVID-19-related kidney damage may be substantial [50].
Long-COVID-19 and chronic renal disease
Multiorgan involvement after COVID-19 was detected in 18.5% of low-risk patients (N = 201) discharged from UK NHS hospitals after COVID-19. Impaired function of the lungs (33%), heart (32%) and kidneys (10%) was common. The rates of these multi-organ dysfunctions were significantly raised compared with the expected risk in the general population [51]. Assessment of the cumulative risk of repeated infection showed that the risk and burden increased in a graded fashion according to the number of COVID-19 infections [52].
Epidemiological research has uncovered a significant kidney impairment in the post-acute COVID-19 period. Bowe and co-workers assessed kidney outcomes in 89,216 US veterans who were 30-day survivors of COVID-19 [53]. The risk of post-acute kidney outcomes was graded according to the severity of the acute infection (non-hospitalisation, hospitalisation, admission to the ICU). Beyond the acute illness, survivors of COVID-19 showed a higher risk of AKI, a decline in estimated glomerular filtration rate (– 3.26 (non-hospitalised), – 5.2 (hospitalised) to – 7.69 (ICU) ml/min/1.73m2 per year) and all-cause mortality [53].
Huang et al. described the long-term consequences of COVID-19 in 1733 Chinese patients discharged from hospital [54]. Amongst the participants with an eGFR available both during the acute phase and at follow-up, 35% had decreased eGFR (< 90 ml/min/1.73 m2) at 6 months. 13% of participants with non-acute kidney injury and normal eGFR at the acute phase presented with decreased eGFR at the end of the follow-up.
Gu et al. [55] followed up 1734 COVID-19 patients with AKI (all stages). They found that AKI in the acute phase of COVID-19 was closely related to the longitudinal decline and post-acute kidney function status at nearly 1 year after symptom onset. After adjustment, the percentage of eGFR decline from acute phase to follow-up was 8.3% higher amongst AKI participants than those without AKI at the acute phase. The eGFR decline of patients with AKI stage 1, stage 2 and stage 3 was 6%, 16% and 18% higher than those without AKI.
Stockmann and colleagues analysed retrospectively long-term outcomes in 74 patients with critical COVID-19 disease and AKI requiring RRT [56]. The median baseline eGFR rate was 76.5 ml/min/1.73 m2. After a median follow-up of 151 days post-initiation of RRT, 36 had died during hospitalisation, 1 patient was still hospitalised and 37 patients were discharged. At the end of the follow-up, 34 patients had achieved variable degrees of renal recovery, and 3 patients had non-recovery of renal function.
Nugent et al. conducted a retrospective cohort study at 5 US hospitals to assess the rate of change in eGFR after hospital discharge in 182 patients with COVID-19-associated AKI and 1,430 patients with AKI not associated with COVID-19 [57]. Patients with COVID-19-associated AKI had a greater decrease in eGFR after adjusting for baseline comorbidities (-12.4 ml/min/1.73 m2/year).
The Hamburg City Health Study COVID-19 programme showed that subjects who apparently recovered from mild to moderate COVID-19 infection (mostly non-hospitalised individuals) had signs of subclinical multi-organ damage. The glomerular filtration rate was significantly lower in the post-infection period (9.6 months after the first positive COVID-19 test) [58].
The prospective cohort study by Li et al. observed a persistent decline in kidney function 1 year after discharge in non-severely infected as well as in critical COVID-19 patients [59]. The small prospective cohort study by Al Rumaihi et al. showed that renal involvement with COVID-19 can occur in the absence of AKI even in mildly infected young patients without pre-existing renal disease [60]. The higher serum creatinine concentrations of COVID-19 patients compared to asymptomatic individuals remained within the normal range during follow-up (6 months).
Using the IRoc-GN International Registry, Waldman et al. found in patients with glomerular disease a) that pre-COVID-19 eGFR was the main risk factor for AKI; b) COVID-19 patients with glomerulonephritis had a higher risk of impaired eGFR recovery after COVID-19-associated AKI and c) higher pre-COVID-19 proteinuria. Focal-segmental GN or minimal change diseases were associated with lower post-COVID-19 eGFR (median follow-up 6.4 months after diagnosis of COVID-19) [61].
These results give an indication of long-term renal consequences of an infection that affects a very large population worldwide. However, it must be kept in mind that the limitations of design and methodology may influence the objective interpretation of epidemiological results. Major confounders are the constraints of heterogeneous study populations (non-hospitalised, hospitalised, critically ill patients) with varying renal dysfunction at the end of the active infection period and different timing and numbers of renal function assessments during the post-COVID-19 period.
In all cases, glomerular filtration rate was estimated using the surrogate marker creatinine (eGFR), which is highly influenced by age, sex, muscle mass, body composition, critical disease and other extrarenal factors. This often leads to misclassification of the true renal function. Possible solutions are the use of cystatin C as an alternative endogenous biomarker of renal function or performing direct measurements of GFR using an exogenous marker.
None of the studies documented persistent kidney damage based on repeated assessments of urinalysis or kidney biopsy. The follow-up of patients was short or mid-term, whilst a significant proportion of patients was lost to follow-up. It remains to be seen whether all patients without kidney damage and normal or slightly reduced unadjusted eGFR values will progress to CKD or ESRD or later regain complete renal function after COVID-19 AKI.
However, these epidemiological data illustrate trajectories of kidney function after COVID-19 infection. Patients with pre-existing primary kidney disease or kidney-affecting chronic metabolic or cardiovascular diseases, and immunosenescence are at an increased risk of progressive kidney injury. In patients with normal baseline surrogate markers of GFR, kidney function may decline gradually over time, even in the absence of AKI or COVID-19 necessitating hospitalisation. On the other hand, patients with severe forms of COVID-19 might experience AKI with a rapid loss of renal function. Post-infection trajectories of patients with COVID-19-associated AKI may vary and include complete, partial or non-recovery of renal function. There may be recurrent episodes of AKI and hospitalisation, particularly in reinfected patients.
Loss of renal function in the post-COVID-19 period is likely multifactorial and might be driven by ongoing hyperinflammation, tubular injury, maladaptive repair of AKI or subclinical AKI, resulting in fibrosis, recurrent sepsis and clinical deterioration of metabolic control and onset of cardiac disease [62, 63]. There is no specific treatment for this condition.
Conclusion
The long-term sequelae of COVID-19-associated kidney damage present an unmet clinical need, with no proven interventions to hasten recovery or prevent transition of AKI to CKD. COVID-19 patients often receive no nephrological follow-up after hospital discharge, and often do not realise that they have a decline of kidney function. There are no guidelines regulating the follow-up period for such AKI patients. Given the high morbidity and mortality of chronic kidney disease, it seems vital to pay close attention (at 3-month intervals for at least 12 months) to survivors of COVID-19-associated AKI. Patients with higher stages of AKI and patients with unresolved kidney dysfunction at discharge, irrespective of kidney function prior to COVID-19 infection, should be followed closely.
Availability of data and materials
Data sharing is not applicable to this article as no new datasets were generated or analysed.
References
Soriano JB, Murthy S, Marshall JC, Relan P, Diaz JV (2022) A clinical case definition of post-COVID-19 condition by a Delphi consensus. Lancet Infect Dis 22(4):e102–e107. https://doi.org/10.1016/s1473-3099(21)00703-9
Chippa V, Aleem A, Anjum F (2022) Post Acute Coronavirus (COVID-19) Syndrome. In: StatPearls. StatPearls Publishing Copyright © 2022, StatPearls Publishing LLC., Treasure Island (FL),
Seeßle J, Waterboer T, Hippchen T, Simon J, Kirchner M, Lim A et al (2022) Persistent symptoms in adult patients 1 year after coronavirus disease 2019 (COVID-19): A Prospective Cohort Study. Clin Infect Dis 74(7):1191–1198. https://doi.org/10.1093/cid/ciab611
Tran VT, Porcher R, Pane I, Ravaud P (2022) Course of post COVID-19 disease symptoms over time in the ComPaRe long COVID prospective e-cohort. Nat Commun 13(1):1812. https://doi.org/10.1038/s41467-022-29513-z
Chung EYM, Palmer SC, Natale P, Krishnan A, Cooper TE, Saglimbene VM et al (2021) Incidence and outcomes of COVID-19 in people with CKD: a systematic review and meta-analysis. Am J Kidney Dis 78(6):804–815. https://doi.org/10.1053/j.ajkd.2021.07.003
Oetjens MT, Luo JZ, Chang A, Leader JB, Hartzel DN, Moore BS et al (2020) Electronic health record analysis identifies kidney disease as the leading risk factor for hospitalization in confirmed COVID-19 patients. PLoS ONE 15(11):e0242182. https://doi.org/10.1371/journal.pone.0242182
Williamson EJ, Walker AJ, Bhaskaran K, Bacon S, Bates C, Morton CE et al (2020) Factors associated with COVID-19-related death using OpenSAFELY. Nature 584(7821):430–436. https://doi.org/10.1038/s41586-020-2521-4
Zhou X, Liu J, Ji X, Yang X, Duan M (2018) Predictive value of inflammatory markers for acute kidney injury in sepsis patients: analysis of 753 cases in 7 years. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue 30(4):346–350. https://doi.org/10.3760/cma.j.issn.2095-4352.2018.04.012
Ji W, Huh K, Kang M, Hong J, Bae GH, Lee R et al (2020) Effect of underlying comorbidities on the infection and severity of COVID-19 in Korea: a Nationwide Case-Control Study. J Korean Med Sci 35(25):e237. https://doi.org/10.3346/jkms.2020.35.e237
Petrilli CM, Jones SA, Yang J, Rajagopalan H, O’Donnell L, Chernyak Y et al (2020) Factors associated with hospital admission and critical illness among 5279 people with coronavirus disease 2019 in New York City: prospective cohort study. BMJ 369:m1966. https://doi.org/10.1136/bmj.m1966
Flythe JE, Assimon MM, Tugman MJ, Chang EH, Gupta S, Shah J et al (2021) Characteristics and outcomes of individuals with pre-existing kidney disease and COVID-19 admitted to intensive care units in the United States. Am J Kidney Dis 77(2):190-203.e191. https://doi.org/10.1053/j.ajkd.2020.09.003
Uribarri A, Núñez-Gil IJ, Aparisi A, Becerra-Muñoz VM, Feltes G, Trabattoni D et al (2020) Impact of renal function on admission in COVID-19 patients: an analysis of the international HOPE COVID-19 (Health Outcome Predictive Evaluation for COVID 19) Registry. J Nephrol 33(4):737–745. https://doi.org/10.1007/s40620-020-00790-5
Henry BM, Lippi G (2020) Chronic kidney disease is associated with severe coronavirus disease 2019 (COVID-19) infection. Int Urol Nephrol 52(6):1193–1194. https://doi.org/10.1007/s11255-020-02451-9
Cai R, Zhang J, Zhu Y, Liu L, Liu Y, He Q (2021) Mortality in chronic kidney disease patients with COVID-19: a systematic review and meta-analysis. Int Urol Nephrol 53(8):1623–1629. https://doi.org/10.1007/s11255-020-02740-3
Ozturk S, Turgutalp K, Arici M, Odabas AR, Altiparmak MR, Aydin Z et al (2020) Mortality analysis of COVID-19 infection in chronic kidney disease, haemodialysis and renal transplant patients compared with patients without kidney disease: a nationwide analysis from Turkey. Nephrol Dial Trans 35(12):2083–2095. https://doi.org/10.1093/ndt/gfaa271
Mohan S, King KL, Husain SA, Schold JD (2021) COVID-19-Associated mortality among kidney transplant recipients and candidates in the United States. Clin J Am Soc Nephrol 16(11):1695–1703. https://doi.org/10.2215/cjn.02690221
Akalin E, Azzi Y, Bartash R, Seethamraju H, Parides M, Hemmige V et al (2020) Covid-19 and kidney transplantation. N Engl J Med 382(25):2475–2477. https://doi.org/10.1056/NEJMc2011117
Goffin E, Candellier A, Vart P, Noordzij M, Arnol M, Covic A et al (2021) COVID-19-related mortality in kidney transplant and haemodialysis patients: a comparative, prospective registry-based study. Nephrol Dial Transp 36(11):2094–2105. https://doi.org/10.1093/ndt/gfab200
Hsu CM, Gupta S, Tighiouart H, Goyal N, Faugno AJ, Tariq A et al (2022) Kidney recovery and death in critically Ill patients with COVID-19-associated acute kidney injury treated with dialysis: the STOP-COVID Cohort Study. Am J Kidney Dis 79(3):404-416.e401. https://doi.org/10.1053/j.ajkd.2021.11.004
Silver SA, Beaubien-Souligny W, Shah PS, Harel S, Blum D, Kishibe T et al (2021) The prevalence of acute kidney injury in patients hospitalized with COVID-19 infection: a systematic review and meta-analysis. Kidney Med 3(1):83-98.e81. https://doi.org/10.1016/j.xkme.2020.11.008
Lumlertgul N, Pirondini L, Cooney E, Kok W, Gregson J, Camporota L et al (2021) Acute kidney injury prevalence, progression and long-term outcomes in critically Ill patients with COVID-19: a cohort study. Ann Intensive Care 11(1):123. https://doi.org/10.1186/s13613-021-00914-5
Zamoner W, Santos C, Magalhães LE, de Oliveira PGS, Balbi AL, Ponce D (2021) Acute kidney injury in COVID-19: 90 days of the pandemic in a Brazilian Public Hospital. Front Med (Lausanne) 8:622577. https://doi.org/10.3389/fmed.2021.622577
Legrand M, Bell S, Forni L, Joannidis M, Koyner JL, Liu K et al (2021) Pathophysiology of COVID-19-associated acute kidney injury. Nat Rev Nephrol 17(11):751–764. https://doi.org/10.1038/s41581-021-00452-0
Nadim MK, Forni LG, Mehta RL, Connor MJ Jr, Liu KD, Ostermann M et al (2020) COVID-19-associated acute kidney injury: consensus report of the 25th acute disease quality initiative (ADQI) workgroup. Nat Rev Nephrol 16(12):747–764. https://doi.org/10.1038/s41581-020-00356-5
Portolés J, Marques M, López-Sánchez P, de Valdenebro M, Muñez E, Serrano ML et al (2020) Chronic kidney disease and acute kidney injury in the COVID-19 Spanish outbreak. Nephrol Dial Transp 35(8):1353–1361. https://doi.org/10.1093/ndt/gfaa189
Russo E, Esposito P, Taramasso L, Magnasco L, Saio M, Briano F et al (2021) Kidney disease and all-cause mortality in patients with COVID-19 hospitalized in Genoa. North Italy J Nephrol 34(1):173–183. https://doi.org/10.1007/s40620-020-00875-1
Fu EL, Janse RJ, de Jong Y, van der Endt VHW, Milders J, van der Willik EM et al (2020) Acute kidney injury and kidney replacement therapy in COVID-19: a systematic review and meta-analysis. Clin Kidney J 13(4):550–563. https://doi.org/10.1093/ckj/sfaa160
Sullivan MK, Lees JS, Drake TM, Docherty AB, Oates G, Hardwick HE et al (2022) Acute kidney injury in patients hospitalized with COVID-19 from the ISARIC WHO CCP-UK Study: a prospective, multicentre cohort study. Nephrol Dial Transp 37(2):271–284. https://doi.org/10.1093/ndt/gfab303
Jana KR, Yap E, Janga KC, Greenberg S (2022) Comparison of two waves of COVID-19 in critically Ill patients: a retrospective observational study. Int J Nephrol 2022:3773625. https://doi.org/10.1155/2022/3773625
Masthead YYJ, Wilkins KJ, Alakwaa F, Liu F, Torre-Healy LA et al (2022) COVID-19-associated AKI in hospitalized US patients: incidence, temporal trends, geographical distribution, risk factors and mortality. medrxiv. https://doi.org/10.1101/2022.09.02.22279398
Charytan DM, Parnia S, Khatri M, Petrilli CM, Jones S, Benstein J et al (2021) Decreasing incidence of acute kidney injury in patients with COVID-19 critical illness in New York City. Kidney Int Rep 6(4):916–927. https://doi.org/10.1016/j.ekir.2021.01.036
Kudose S, Batal I, Santoriello D, Xu K, Barasch J, Peleg Y et al (2020) Kidney biopsy findings in patients with COVID-19. J Am Soc Nephrol 31(9):1959–1968. https://doi.org/10.1681/asn.2020060802
May RM, Cassol C, Hannoudi A, Larsen CP, Lerma EV, Haun RS et al (2021) A multi-center retrospective cohort study defines the spectrum of kidney pathology in Coronavirus 2019 Disease (COVID-19). Kidney Int 100(6):1303–1315. https://doi.org/10.1016/j.kint.2021.07.015
Rivero J, Merino-López M, Olmedo R, Garrido-Roldan R, Moguel B, Rojas G et al (2021) Association between postmortem kidney biopsy findings and acute kidney injury from patients with SARS-CoV-2 (COVID-19). Clin J Am Soc Nephrol 16(5):685–693. https://doi.org/10.2215/cjn.16281020
Santoriello D, Khairallah P, Bomback AS, Xu K, Kudose S, Batal I et al (2020) Postmortem kidney pathology findings in patients with COVID-19. J Am Soc Nephrol 31(9):2158–2167. https://doi.org/10.1681/asn.2020050744
Sharma P, Uppal NN, Wanchoo R, Shah HH, Yang Y, Parikh R et al (2020) COVID-19-associated kidney injury: a case series of kidney biopsy findings. J Am Soc Nephrol 31(9):1948–1958. https://doi.org/10.1681/asn.2020050699
Dadras O, Afsahi AM, Pashaei Z, Mojdeganlou H, Karimi A, Habibi P et al (2022) The relationship between COVID-19 viral load and disease severity: a systematic review. Immun Inflamm Dis 10(3):e580. https://doi.org/10.1002/iid3.580
Shenoy S (2021) SARS-CoV-2 (COVID-19), viral load and clinical outcomes; lessons learned one year into the pandemic: a systematic review. World J Crit Care Med 10(4):132–150. https://doi.org/10.5492/wjccm.v10.i4.132
Braun F, Lütgehetmann M, Pfefferle S, Wong MN, Carsten A, Lindenmeyer MT et al (2020) SARS-CoV-2 renal tropism associates with acute kidney injury. Lancet 396(10251):597–598. https://doi.org/10.1016/s0140-6736(20)31759-1
Paranjpe I, Chaudhary K, Johnson KW, Jaladanki SK, Zhao S, De Freitas JK et al (2021) Association of SARS-CoV-2 viral load at admission with in-hospital acute kidney injury: A retrospective cohort study. PLoS ONE 16(2):e0247366. https://doi.org/10.1371/journal.pone.0247366
Caceres PS, Savickas G, Murray SL, Umanath K, Uduman J, Yee J et al (2021) High SARS-CoV-2 viral load in urine sediment correlates with acute kidney injury and poor COVID-19 outcome. J Am Soc Nephrol 32(10):2517–2528. https://doi.org/10.1681/ASN.2021010059
Jansen J, Reimer KC, Nagai JS, Varghese FS, Overheul GJ, de Beer M et al (2022) SARS-CoV-2 infects the human kidney and drives fibrosis in kidney organoids. Cell Stem Cell 29(2):217-231.e218. https://doi.org/10.1016/j.stem.2021.12.010
Li X, Tam AR, Chu WM, Chan WM, Ip JD, Chu AW et al (2022) Risk factors for slow viral decline in COVID-19 patients during the 2022 Omicron wave. Viruses 14(8):1714. https://doi.org/10.3390/v14081714
Corriero A, Ribezzi M, Mele F, Angrisani C, Romaniello F, Daleno A et al (2022) COVID-19 variants in critically Ill patients: a comparison of the delta and omicron variant profiles. Infect Dis Rep 14(3):492–500. https://doi.org/10.3390/idr14030052
Davies MA, Morden E, Rosseau P, Arendse J, Bam JL, Boloko L et al (2022) Outcomes of laboratory-confirmed SARS-CoV-2 infection during resurgence driven by Omicron lineages BA.4 and BA.5 compared with previous waves in the Western Cape Province, South Africa. medRxiv. https://doi.org/10.1101/2022.06.28.22276983
Wolter N, Jassat W, Walaza S, Welch R, Moultrie H, Groome M et al (2022) Early assessment of the clinical severity of the SARS-CoV-2 omicron variant in South Africa: a data linkage study. Lancet 399(10323):437–446. https://doi.org/10.1016/s0140-6736(22)00017-4
Bell S, Campbell J, Watters C, O’Neil M, Almond A, Buck K et al (2023) The impact of Omicron on outcomes following infection with SARS-CoV-2 in patients with kidney failure in Scotland. Clin Kidney J 16(1):197–200. https://doi.org/10.1093/ckj/sfac173
Liakopoulos V, Roumeliotis S, Papachristou S, Papanas N (2022) COVID-19 and the kidney: time to take a closer look. Int Urol Nephrol 54(5):1053–1057. https://doi.org/10.1007/s11255-021-02976-7
Jewell PD, Bramham K, Galloway J, Post F, Norton S, Teo J et al (2021) COVID-19-related acute kidney injury; incidence, risk factors and outcomes in a large UK cohort. BMC Nephrol 22(1):359. https://doi.org/10.1186/s12882-021-02557-x
Sabaghian T, Kharazmi AB, Ansari A, Omidi F, Kazemi SN, Hajikhani B et al (2022) COVID-19 and acute kidney injury: a systematic review. Front Med (Lausanne) 9:705908. https://doi.org/10.3389/fmed.2022.705908
Ayoubkhani D, Khunti K, Nafilyan V, Maddox T, Humberstone B, Diamond I et al (2021) Post-covid syndrome in individuals admitted to hospital with covid-19: retrospective cohort study. BMJ 372:n693. https://doi.org/10.1136/bmj.n693
Bowe B, Xie Y, Al-Aly Z (2022) Acute and postacute sequelae associated with SARS-CoV-2 reinfection. Nat Med 28:2398–2405. https://doi.org/10.1038/s41591-022-02051-3
Bowe B, Xie Y, Xu E, Al-Aly Z (2021) Kidney outcomes in long COVID. J Am Soc Nephrol 32(11):2851–2862. https://doi.org/10.1681/asn.2021060734
Huang C, Huang L, Wang Y, Li X, Ren L, Gu X et al (2021) 6-month consequences of COVID-19 in patients discharged from hospital: a cohort study. Lancet 397(10270):220–232. https://doi.org/10.1016/s0140-6736(20)32656-8
Gu X, Huang L, Cui D, Wang Y, Wang Y, Xu J et al (2022) Association of acute kidney injury with 1-year outcome of kidney function in hospital survivors with COVID-19: A cohort study. EBioMedicine 76:103817. https://doi.org/10.1016/j.ebiom.2022.103817
Stockmann H, Hardenberg JB, Aigner A, Hinze C, Gotthardt I, Stier B et al (2021) High rates of long-term renal recovery in survivors of coronavirus disease 2019-associated acute kidney injury requiring kidney replacement therapy. Kidney Int 99(4):1021–1022. https://doi.org/10.1016/j.kint.2021.01.005
Nugent J, Aklilu A, Yamamoto Y, Simonov M, Li F, Biswas A et al (2021) Assessment of acute kidney injury and longitudinal kidney function after hospital discharge among patients with and without COVID-19. JAMA Netw Open 4(3):e211095. https://doi.org/10.1001/jamanetworkopen.2021.1095
Petersen EL, Goßling A, Adam G, Aepfelbacher M, Behrendt CA, Cavus E et al (2022) Multi-organ assessment in mainly non-hospitalized individuals after SARS-CoV-2 infection: The Hamburg City Health Study COVID programme. Eur Heart J 43(11):1124–1137. https://doi.org/10.1093/eurheartj/ehab914
Li D, Liao X, Ma Z, Zhang L, Dong J, Zheng G et al (2022) Clinical status of patients 1 year after hospital discharge following recovery from COVID-19: a prospective cohort study. Ann Intensive Care 12(1):64. https://doi.org/10.1186/s13613-022-01034-4
Al Rumaihi K, Khalafalla K, Arafa M, Nair A, Al Bishawi A, Fino A et al (2022) COVID-19 and renal involvement: a prospective cohort study assessing the impact of mild SARS-CoV-2 infection on the kidney function of young healthy males. Int Urol Nephrol 55(1):201–209. https://doi.org/10.1007/s11255-022-03301-6
Waldman M, Soler MJ, García-Carro C, Lightstone L, Turner-Stokes T, Griffith M et al (2021) Results from the IRoc-GN international registry of patients with COVID-19 and glomerular disease suggest close monitoring. Kidney Int 99(1):227–237. https://doi.org/10.1016/j.kint.2020.10.032
Yende S, Parikh CR (2021) Long COVID and kidney disease. Nat Rev Nephrol 17(12):792–793. https://doi.org/10.1038/s41581-021-00487-3
Del Rio C, Collins LF, Malani P (2020) Long-term Health Consequences of COVID-19. JAMA 324(17):1723–1724. https://doi.org/10.1001/jama.2020.19719
Funding
There was no funding for the review, preparation and decision of the manuscript.
Author information
Authors and Affiliations
Contributions
All named authors of the article meet the International Committee of Medical Journal Editors’ criteria for authorship for this article, take responsibility for the integrity of the work and have given their approval for the final version of the article to be published.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no non-financial or financial competing interests, or conflicts of interest.
Ethical approval
This narrative review is based on previously conducted studies. It uses publicly accessible documents as evidence. Institutional approval and patient consent were not necessary.
Consent for publication
The manuscript does not contain data from any individual persons.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Schiffl, H., Lang, S.M. Long-term interplay between COVID-19 and chronic kidney disease. Int Urol Nephrol 55, 1977–1984 (2023). https://doi.org/10.1007/s11255-023-03528-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-023-03528-x