
Abstract
Purpose
Hemodialysis (HD) patients are known to have high cardiovascular mortality rate. Sudden cardiac death (SCD) due to arrhythmias causes most of the cardiac deaths. HD per se may lead to ECG abnormalities and ventricular arrhythmias. Monitoring ECG parameters such as corrected QT interval, QT dispersion (QTd), Tpe interval may be useful to stratify the patients with high risk of arrhythmia and SCD. Herein we aimed to investigate the effects of changes in serum electrolyte levels and pH on ECG parameters before and after the HD.
Methods
A total of 50 chronic HD patients (mean age 58 ± 19; male 27) were enrolled. Patients with unmeasurable T waves; atrial fibrillation; bundle branch block; use of class I or class III antiarrhythmic drugs were excluded. Serum potassium, magnesium, calcium, urea, creatinine and pH were measured before and after HD treatment. Standard surface 12-lead ECGs were recorded before and after HD. QTc, QTd, Tpe, JT interval, P-wave-duration, P-wave dispersion were determined.
Results
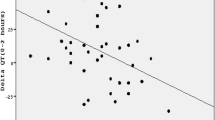
Serum potassium and magnesium decreased, and calcium, pH and bicarbonate levels increased; QRS and Tpe interval were increased after HD. Basal Tpe was correlated with urea (r = 0.31, p = 0.02). Tpe interval was higher in hypocalcemic compared to normocalcemic patients (77 ± 11 vs 70 ± 9 ms, p = 0.02). ∆Tpe was correlated with ∆calcium (r = −0.32, p = 0.02). Basal QTc was correlated with calcium (r = −0.62, p < 0.001). ∆QTc was correlated with basal calcium (r = 0.39, p = 0.005) and ∆calcium (r = −0.46, p < 0.001). Basal JT was correlated with calcium (r = −0.55, p < 0.001). ∆JT was correlated with pH (r = 0.35, p = 0.01), ∆calcium (r = −0.53, p < 0.001) and ∆magnesium (r = −0.30, p = 0.03). Before HD, 12 patients (12%) were hypermagnesemic of whom JT intervals were lower (314 ± 20 vs 332 ± 23 ms, p = 0.02). Ultrafiltration per body weight was associated with ∆QTc (r = −0.40, p = 0.007) and ∆JT (r = −0.36, p = 0.01).
Conclusion
QRS and Tpe intervals were increased after HD. Tpe interval was longer in hypocalcemic patients. Change in Tpe was negatively associated with the change in calcium. Ultrafiltration was associated with ∆QTc and ∆JT. Calcium and ultrafiltration seem to be the most important determinants of ECG parameters of HD-induced repolarization abnormalities.




Similar content being viewed by others


References
Herzog CA, Mangrum M, Passman R (2008) Sudden cardiac death in dialysis patients. Semin Dial 21:300–307
Secemsky EA, Verrier RL, Cooke G, Ghossein C, Subacius H, Manuchehry A, Herzog CA, Passman R (2011) High prevalence of cardiac autonomic dysfunction and T-wave alternans in dialysis patients. Heart Rhythm 8(4):592–598
Levin A, Singer J, Thompson CR, Ross H, Lewis M (1996) Prevalent left ventricular hypertrophy in the predialysis population: identifying opportunities for intervention. Am J Kidney Dis 27:347–354
Abe S, Yoshizawa M, Naganishi N et al (1996) Electrocardiographic abnormalities in patients receiving hemodialysis. Am Heart J 131:1137–1144
Istvan L, Janos M, Zsolt Z et al (1999) QT dispersion in patients with end-stage renal failure and during hemodialysis. J Am Soc Nephrol 10:1297–1302
Kors JA, van Eck HJR, van Herpen G (2008) The meaning of the Tp-Te interval and its diagnostic value. J Electrocardiol 41:575–580
Jaroszyński AJ, Załuska WT, Ksiazek A (2005) Effect of haemodialysis on regional and transmural inhomogeneities of the ventricular repolarisation phase. Nephron Clin Pract 99(1):c24–c30
Tang WH, Wang CP, Chung FM, Huang LL, Yu TH, Hung WC, Lu LF, Chen PY, Luo CH, Lee KT, Lee YJ, Lai WT (2015) Uremic retention solute indoxyl sulfate level is associated with prolonged QTc interval in early CKD patients. PLoS ONE 10(3):e0119545
Algra A, Tijssen JGP, Roelandt JRTC, Pool J, Lubsen J (1991) QTc prolongation measured by standard 12-lead electrocardiography is an independent risk factor for sudden death due to cardiac arrest. Circulation 83:1888–1894
Lörincz I, Ma´tyus J, Zilahi Z, Kun C, Kara´ny Z, Kakuk G (1999) QT dispersion in patients with end-stage renal failure and during haemodialysis. J Am Soc Nephrol 10:1297–1302
Covic A, Diaconita M, Gusbeth-Tatomir P, Covic M, Botezan A, Ungureanu G, Goldsmith DJ (2002) Haemodialysis increases QT(c) interval but not QT(c) dispersion in ESRD patients without manifest cardiac disease. Nephrol Dial Transplant 17(12):2170–2177
Floccari F, Aloisi E, Nostro L, Caccamo C, Crisafulli A, Barillà A, Aloisi C, Romeo A, Corica F, Ientile R, Frisina N, Buemi M (2004) QTc interval and QTc dispersion during haemodiafiltration. Nephrology (Carlton) 9(6):335–340
Severi S, Ciandrini A, Grandi E, Cavalcanti S, Bini S, Badiali F, Gattiani A, Cagnoli L (2006) Cardiac response to hemodialysis with different cardiovascular tolerance: heart rate variability and QT interval analysis. Hemodial Int 10(3):287–293
Drighil A, Madias JE, Benjelloun M, Kamoum H, Bennis A, Azzouzi L, Yazidi A, Ramdani B (2007) Changes in the QT intervals, QT dispersion, and amplitude of T waves after hemodialysis. Ann Noninvasive Electrocardiol 12(2):137–144
Afshinnia F, Doshi H, Rao PS (2012) The effect of different dialysate magnesium concentrations on QTc dispersion in hemodialysis patients. Ren Fail 34(4):408–412
Yetkin E, Ileri M, Tandoğan I, Boran M, Yanik A, Hisar I, Kutlu M, Cehreli S, Korkmaz S, Göksel S (2000) Increased QT interval dispersion after hemodialysis: role of peridialytic electrolyte gradients. Angiology 51(6):499–504
Yildiz A, Akkaya V, Sahin S et al (2001) QT dispersion and signal-averaged electrocardiogram in haemodialysis and CAPD patients. Perit Dial Int 21:186–192
Howse M, Sastry S, Bell GM (2002) Changes in the corrected QT interval and corrected QT dispersion during haemodialysis. Postgrad J Med 78:273–275
Zulqarnain MA, Qureshi WT, O’Neal WT, Shah AJ, Soliman EZ (2015) Risk of mortality associated with QT and JT intervals at different levels of QRS duration (from the third national health and nutrition examination survey). Am J Cardiol 116(1):74–78
Dilaveris PE, Gialafos EJ, Sideris SK et al (1998) Simple electrocardiographic markers to the prediction of paroxysmal idiopathic atrial fibrillation. Am Heart J 135:733–736
Ozmen N, Cebeci BS, Kardesoglu E, Atasoyu EM, Unver S, Celik T, Aparci M, Dincturk M (2007) Relationship between P-wave dispersion and effective hemodialysis in chronic hemodialysis patients. Med Princ Pract 16(2):147–150
Páll A, Czifra Á, Sebestyén V, Becs G, Kun C, Balla J, Paragh G, Lőrincz I, Páll D, Padra TJ, Agarwal A, Zarjou A, Szabó Z (2016) Hemodiafiltration and hemodialysis differently affect P wave duration and dispersion on the surface electrocardiogram. Int Urol Nephrol 48(2):271–277
Tezcan UK, Amasyali B, Can I et al (2004) Increased P wave dispersion and maximum P wave duration after hemodialysis. Ann Noninvasive Electrocardiol 9:34–38
Szabo Z, Kakuk G, Fulop T et al (2002) Effects of haemodialysis on maximum P wave duration and P wave dispersion. Nephrol Dial Transplant 17:1634–1638
Acknowledgements
We appreciate and thank our hemodialysis staff especially Gulden Bosgelmez, Ayse Ersoy Aydin and Semra Canpolat for their great efforts and contributions to this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Authors HO, AO, OA, ASB, MB, MI, GA, ARO declare that they have no conflict of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Ozportakal, H., Ozkok, A., Alkan, O. et al. Hemodialysis-induced repolarization abnormalities on ECG are influenced by serum calcium levels and ultrafiltration volumes. Int Urol Nephrol 49, 509–515 (2017). https://doi.org/10.1007/s11255-016-1472-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11255-016-1472-z