
Abstract
Previous studies have observed heterogeneous changes in domestic violence-related 911 calls, police incident reports, and arrests at the onset of the COVID-19 pandemic. In this study, we use a large-scale medical claims database with coverage of over 100 million patients to examine the impact on domestic violence victims’ use of emergency department care for their injuries in the early weeks of the pandemic compared to the corresponding weeks in previous years. We find a 23–35% decrease in utilization of emergency medical services by domestic violence victims between March and June of 2020. Based on this finding, it is essential to use caution when using medical claims to measure domestic violence in future research covering this time period. Decreases in care utilization also have important implications for the detection, screening, and treatment of domestic violence injuries during future public health crises.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
At the onset of the COVID-19 pandemic, news reports and victim advocacy organizations raised concerns about potential increases in domestic violence due to increased time at home, widespread job losses and furloughs, and increased stress - all known risk factors for violence in the home. Furthermore, concerns about COVID-19 infection risk and strain on the healthcare system reduced overall healthcare utilization in the early weeks of the pandemic. The combination of these factors suggests that domestic violence victims may have been less willing and able to access medical care and other supportive services in the early weeks of the pandemic. In this paper, we use a medical claims database covering over 100 million patients in 48 states to investigate the ways that the onset of the pandemic and its associated behavioral and policy responses affected victims’ access to emergency medical care for domestic violence injuries as well as any additional services that may result from emergency department domestic violence screening.
Much of the existing economic literature on domestic violence during the COVID-19 pandemic (Bullinger et al. 2021; Hsu and Henke 2021; Leslie and Wilson 2020; McCrary and Sanga 2021; Miller et al. 2020, 2022) measures incidence of domestic violence by using police data measures, such as 911 calls for service or police incident reports for domestic violence offenses. These studies find that domestic violence 911 calls increased, while arrests and recorded criminal incidents decreased. Miller et al. (2020) find that reports of severe domestic violence offenses like aggravated assaults and homicides decreased while 911 calls increased. Ivandic et al. (2020) link the rise in calls to increased reporting by both victims and third parties such as neighbors and note increases in violence by current partners and decreases in violence by ex-partners. Bullinger et al. (2021) find a similar pattern of rising calls for service, noting that the drop in arrests and incident reports for domestic violence offenses mimics that of other crimes, suggesting that the decline in reports may be driven not by declines in domestic violence but by changes in police behavior. In fact, some police agencies issued explicit directives to alter or reduce public contact (Jennings and Perez 2020). Taken together, simultaneously changing victim and police behavior result in heterogeneous effects depending on the police data measures used.
In addition to the substantial work focused on assessing domestic violence using law enforcement data, economic literature has examined incidence of domestic violence using alternative data sources which may be less subject to shifts in both victim reporting and police behavior. A survey undertaken by Arenas-Arroyo et al. (2021) in Spain finds that the pandemic increased verbal and emotional abuse rather than physical abuse, a result that is consistent among other studies employing survey measures of verbal and emotional abuse (Drotning et al. 2023). Research using calls to domestic violence hotlines (Perez-Vincent and Carreras 2022; Silverio-Murillo et al. 2023) and internet search intensity for domestic violence (Berniell and Facchini 2021) find significant increases during the initial period of lockdowns. These findings are consistent with the observed increases in 911 calls coupled with decreasing police reports or arrests observed in the U.S. and international contexts (Hoehn-Velasco et al. 2021; Ravindran and Shah 2020).
While these studies provide important evidence about changing incidence and reporting of domestic violence, we focus on the substantial impacts on medical treatment for domestic violence injuries during the COVID-19 pandemic. To this end, we use detailed medical claims data spanning over 100 million patients in 48 states with tens of millions of visits to healthcare providers. Existing studies have used medical records to study domestic violence during the pandemic within a single medical facility or geographic area and find a range of differing impacts. Several studies focused often on single trauma centers find increases in domestic violence medical visits (Pallansch et al. 2022; Rahman et al. 2022; Rhodes et al. 2020; Smith et al. 2022). In contrast, other single-hospital analyses find decreases in domestic violence and abuse-related medical visits (Muldoon et al. 2021). These studies employ comparable measures of domestic violence medical visits, but differ according to provider settings, geographies, and observed effects. This study fills an important research gap by analyzing domestic violence medical visits with extensive coverage across varied providers and geographies.
Overall, we find that emergency department visits for domestic violence injuries declined considerably in the early phase of the pandemic from March to June of 2020. Visits recovered in the later months of the year but remained lower than prior years. However, this decline was smaller in percentage terms than the corresponding decline in accidental injury visits, which suggests that it is likely driven by the broader decline in healthcare utilization rather than declines in the actual incidence of domestic violence injuries. Reinforcing this conclusion, the decline is driven almost entirely by less severe injuries; visits for severe or life-threatening injuries make up a small portion of the decline in assault injury visits. This pattern is consistent with forgoing or delaying care as victims face tradeoffs between untreated domestic violence injuries and COVID-19 infection risk.
To ensure our results are not driven by increased unemployment and insurance loss related to the pandemic (Albanesi and Kim 2021; Bundorf et al. 2021; Cajner et al. 2020), we examine trends in domestic violence visits separately among public and private insurance payers. It is unlikely that our results are driven by insurance loss, as trends in assault claims are similar across both private insurance payers administering group plans that would be more affected by pandemic-related job loss and government and exchange payers that primarily administer individual plans that are less tied to specific jobs. Furthermore, we find a 23–35% decline in female assault visits at the onset of the pandemic (depending on the specification) and compare this with only a 3–4% decrease in reported domestic violence incidents to police departments using data from the Federal Bureau of Investigation’s National Incident Based Reporting System (NIBRS), despite existing evidence that police were less likely to record a domestic violence incident when responding to a 911 call during this time period (Bullinger et al. 2021). The totality of these results leads us to conclude that while domestic violence injuries were likely increasing or stable in the early weeks of social distancing behavior, victims were less likely to receive emergency medical care for their injuries.
Our main finding – that victims were less likely to access emergency medical care for domestic violence during the most acute phase of the pandemic – has implications for measurement of domestic violence in future empirical work. Aizer (2010) used emergency department visits by women for assault injuries as a measure of domestic violence that is unaffected by victims’ self-selection into reporting their abuse to law enforcement. This is a sensible proxy, as victims often do not report their abuse to law enforcement, due to shame, fear of retaliatory violence, or a desire to keep their families intact (Felson et al. 2002; Felson and Paré 2005; Griffing et al. 2002). While those that require medical care often seek it, many do not admit to the cause of their injuries or hesitate to seek additional services for victims (Kothari and Rhodes 2006). However, our results imply that future analyses whose time horizons cover the COVID-19 pandemic (or other public health crises that reduce medical care utilization) should not rely solely on medical visits as a measure of domestic violence.
Our findings also have implications for service provision for domestic violence victims during times of widespread distress. Healthcare providers have increasingly adopted screening to identify social determinants of health. Since 2012, the American College of Obstetricians and Gynecologists has recommended regular intimate partner violence screening during pregnancy and postpartum and in 2018, the U.S. Preventive Services Task Force adopted a recommendation for universal violence screening among reproductive-aged individuals (US Preventive Services Task Force 2018). In a large sample of healthcare providers, nearly 60% of physician practices and U.S. hospitals report screening for interpersonal violence (Fraze et al. 2019). Although research examining the effectiveness of both hospital-based screening and resulting domestic violence interventions is limited (Ghidei et al. 2023; Seff et al. 2021), recent evidence suggests that access to digital safety planning tools (Ford-Gilboe et al. 2020; Hegarty et al. 2019; Bloom et al. 2014) and virtual therapies (Ragavan et al. 2020; Gray et al. 2015) may result in improved safety-seeking behaviors and mental health outcomes for survivors of domestic violence. Evaluations of similar programs implemented by police agencies have shown that the use of screening tools such as lethality assessments increase victims’ use of safety planning strategies (Messing et al. 2015) and results in reduced risk of future homicide victimization (Koppa 2022). In light of this, policy responses to any future public health crises that may reduce in-person medical care utilization should account for reduced ability to screen for domestic violence.
2 Data
2.1 Medical claims: COVID-19 research database
We use data from the COVID-19 Research Database, a collaboration between industry leaders and researchers with the objective of providing medical data for pandemic-related research.Footnote 1 The COVID-19 Research Database is a collection of health databases including multiple medical claims data sources. We use de-identified medical claims data from a claims data aggregator that facilitates reimbursement for submitted claims between payers and billing providers. This aggregator spans over 100 million patients in 48 states with tens of millions of visits to healthcare providers. We construct a balanced panel of emergency department visits to healthcare providers that consistently appear in the dataset from 2017 to 2020.Footnote 2
Figure 1 shows the geographic coverage of our sample. The finest geographic designation available in our dataset is the three-digit zip code, which is often roughly city-sized in urban and suburban areas and often roughly county-sized in rural areas. The sample is not nationally representative, as coverage differs across states, and we do not observe uninsured patients. However, even after dropping zip codes with apparent reporting issues that are difficult to resolve at the billing provider level (described below) and areas in which no emergency department billing providers report any assault visits during the panel, our sample contains billing providers from emergency departments in 449 different three-digit zip codes, resulting in at least partial coverage of about 50% of regular residential three-digit zips in the United States.Footnote 3 This large coverage area should provide sufficient information to identify impacts on medical treatment in emergency department claims for domestic violence injuries at the onset of the pandemic compared to the usual seasonal pattern.

Sample coverage map. Map shading represents the portion of a county’s population residing in a three-digit-ZIP area in our sample. Three-digit ZIP areas included in the sample are not fully covered, and their counts represent only the billing providers who (1) consistently appear in the dataset and (2) report at least one emergency department assault visit during our sample period
2.2 Panel construction
We construct a balanced panel of billing providers that consistently submit claims for reimbursement to the COVID-19 Research Database claims data aggregator. We construct a sample of “good reporters” from billing provider unique identifiers to consistently track weekly emergency department visit volume without bias from idiosyncratic data reporting behavior at the provider level as billing providers may enter or exit the full sample.Footnote 4 We require that each billing provider, which generally serve physician or physicians’ network, to submit at least one claim in a given state in at least 50 weeks of each year in our sample period. Any billing provider that does not meet this condition is dropped entirely in order to ensure that results are not driven by changes in sample composition over time. This approach is especially important to appropriately use the COVID-19 Research Database. Payers may change claims clearinghouse services, triggering changes to where billing providers submit claims. Billing provider inclusion in the research database varies in terms of how far back in time records are included. Our approach avoids false zeros in the panel, or instances where a provider does not report claims despite actually seeing patients for assault injuries because it does not appear in the dataset that week.
We compare seasonal patterns in 2017–2018, before the pandemic, to those in 2020. We exclude 2019 from our sample due to a known data reporting issue identified by the data provider that results in an artificial dip in claims in April through July of 2019.Footnote 5 After filtering out billing providers with irregular reporting behavior, claims are aggregated to the zip-week level.
Despite filtering out individual billing providers based on inconsistent reporting behavior, some reporting anomalies remain at the three-digit zip level. Specifically, areas that report very few assault or accidental injury claims will infrequently report disproportionately high visit counts. To mitigate this concern, each three-digit zip area a is assigned a percentile Percentileay of assault claims and accidental injury claims reported in the first ten weeks of each year y of the panel. Each zip area’s percentile range PctRangea is calculated as:
Areas above the 95th percentile of PctRangea in either assault claims or accidental injury claims are dropped from the panel, as their extreme movement in percentiles across years in the weeks of the year prior to the onset of the pandemic is likely to be the result of changes in reporting behavior rather than a measure of true changes in injury visit rates.
The final panel includes professional claims for assault and abuse injuries across 449 three-digit zip areas over three years. Many of these areas rarely report assaults in our sample, and may not report assaults every year. We discuss the implications of this sparseness and implement mitigating strategies in the robustness section.
2.3 Outcomes and benchmark measures
We construct counts of emergency department claims for visits to treat domestic violence injuries as outcomes. We create narrow and broad definitions of domestic violence, constructed from medical billing record use of International Classification of Disease (ICD-10) coding. We use a feature of ICD coding known as external cause of injury codes, or “E-Codes.” E-codes track injuries by intent and mechanism of injury, and include designations for assault injuries generally as well as injuries believed to be caused by domestic abuse specifically. While E-codes are not a billable medical code, their use is standard practice in medical coding such that over ninety percent of emergency department injury visits include an E-code (Barret 2016). We use claims submitted for reimbursement for professional servicesFootnote 6, identifying emergency department services from the place of service listed on the professional claim.Footnote 7 We identify a visit as a unique patient treated by physicians in an emergency department on a single day of service and we classify each visit according to the associated E-codes. We de-duplicate claims that are likely to reflect billing errors or changes by excluding duplicate claims for the same patient for the same diagnosis codes, billing provider NPI and service dates. We use E-codes to classify visits in accordance with the Health Resources and Services Administration Uniform Data System (UDS) Reporting Requirements (Rebbe et al. 2023; Uniform Data System 2021 Health Center Data Reporting Requirements 2021).
Our first outcome is emergency department visits for actual or suspected abuse, as defined by ICD-10 codes T74 or T76, denoting suspected or confirmed adult and child abuse, neglect and other maltreatment. This measure includes few false positives, where a visit for assault injuries caused by a party outside the household is erroneously counted as domestic violence (Brown et al. 2023; Rasooly et al. 2023). However, this outcome severely undercounts the number of domestic violence cases, since victims often do not share with medical providers the source of their assault injuries (Rhodes et al. 2011). For this outcome, we include both female and male patients.
We also include a broader outcome of “female assault” to capture female victims who are not identified by their provider as abuse victims but are nonetheless victims of domestic violence. This outcome includes all visits with E-codes denoting intentional assault by another person. About 75% of assaults of women are domestic violence (Tjaden and Thoennes 1998), and an influential paper by Aizer (2010) studying the effect of the gender wage gap on domestic violence uses the same proxy. We cannot measure visits for male victims of domestic violence using this particular outcome because the majority of assaults of men are not related to domestic violence (Lauritsen and Heimer 2012). This outcome measure does introduce some false positives, as female assault visits will include assaults perpetrated by outside parties as well as those perpetrated by partners. However, it omits fewer true domestic violence cases than the more strictly defined “abuse” outcome because it includes domestic violence victims who do not tell their medical providers the source of their injuries. Because most assaults against women are by intimate partners and our results are similar across abuse and female assault visits, it is unlikely that the estimated changes in female assault visits are driven by perpetrators outside the home.
In addition to the measures of domestic violence, we also include outcome variables for accidental injuries (falls, cuts, strikes) and firearm assaults in order to more fully characterize care-seeking behaviors during the COVID-19 pandemic. Accidental injuries are a useful benchmark outcome for which the underlying incidence of injuries does not depend on police reporting or interactions. We employ accidental injuries as an important comparison to characterize changes in emergency department utilization for external injuries, as increases in violence, decreases in the likelihood of seeking emergency medical care due to perceived risk or strain on the healthcare system, and decreases in claims due to changes in insurance status may have offsetting effects. We omit injuries resulting from motor vehicle accidents to avoid measuring decreases in injury driven by decreasing vehicle use. We also limit the analysis to adults, which prevents this benchmark from being biased by the increase in children’s accidental injury visits due to supervisory neglect during the pandemic (Bullinger et al. 2021).
Finally we also explore domestic violence visits unlikely to be deterred by COVID-19 risk by examining severe types of injuries likely to require medical attention. For this, we focus on firearm assaults - including rifles, handguns, and unknown firearm types.Footnote 8 Firearm assaults are the rarest outcome in the data and analyses of firearm assaults disaggregated by gender are underpowered. Nonetheless, firearm assaults are a measure of extremely severe instances of assault in which patients are very unlikely to forgo medical care due to other concerns. Patients treated in emergency departments for assault by gunshot wound suffer injuries so severe that the majority are admitted for further treatment in an inpatient setting (Fowler et al. 2015). Even with inpatient treatment, about one in six firearm assaults are fatal (Barber et al. 2022; Braga and Cook 2018). Furthermore, firearms are used in the majority of intimate partner homicides (Gold 2020), so female firearm assault visits are likely to primarily reflect extremely severe domestic violence incidents.
Table 1 presents summary statistics for main outcome variables. Female assault visits are about ten times as common as abuse visits in the sample.
Because each outcome - assault, accidental injury, or firearm assault visits - is the number of patient visits submitted to the claims aggregator for a given injury type in three-digit zip area a at time t, it is reflective of several factors including patients’ decisions to seek medical care if injured \(P{\left({Care|Injury}\right)}_{{at}}\), the insurance status of injured patients \(P{\left({Insurance|Injury}\right)}_{{at}}\), and injury status of persons in the area \({\left({TotalInjuries}\right)}_{{at}}\). Visits counts can therefore be conceptualized as the following composite of the three latent variables:
For domestic violence injuries, all three latent variables are likely to be affected by the pandemic. Total injuries likely increased or remained stable given the documented increases in domestic violence 911 calls discussed in Section “Introduction”. However, many victims may have foregone or delayed emergency medical care due to COVID-19 risk, strain on the healthcare system, or increased partner control. Finally, some victims may have become uninsured due pandemic-related job loss, causing their visits to be excluded from the sample, which we discuss in Section 4.2.
We benchmark our estimates of changes in emergency department domestic violence injury visits against emergency department visits for accidental injuries, excluding car accidents due to changes in driving behavior. Because we find that accidental injury visits decreased by roughly the same percentage as the decrease in preventative care visits estimated by previous studies (Cantor et al. 2022; Law et al. 2022), we use these estimates as a benchmark for the likely change in emergency department utilization for physical injuries in the absence of large expected changes in the underlying need for care.
Table 2 summarizes the advantages and disadvantages of each outcome or benchmark measure we construct and relates them to the latent variables they measure in our interpretation of outcomes.
To capture differences in seriousness of injury, we calculate an Injury Severity Score (ISS) for all assault injuries.Footnote 9 The ISS score classifies injury severity according to risk of injury mortality, morbidity, and inpatient hospital admission (Petridou and Antonopoulos 2017), enabling us to differentiate between severe injuries likely to require immediate medical attention and more minor physical injury. To calculate the ISS score, each of a patient’s affected anatomical injury area is scored from 1 to 6 where a score of 1 constitutes a “minor” injury while 6 denotes an “untreatable” injury (Clark et al. 2018). Each anatomical injury area is aggregated to a total score, which is binned into four final severity categories ranging from category 1 for minor injuries to category 4 for severe life-threatening injuries. We therefore interpret scores in category 1 to reflect injuries that are not life threatening, and scores in categories 2–4 to reflect injuries that could result in threats to the patient’s life or long-term health if not treated. Table 2 in Appendix A presents descriptive statistics for visits by injury severity score; we see on average 1.18 assault visits and 22.52 accident visits per zip-week in category 1, and 0.11 assault visits and 1.84 visits per zip-week in categories 2–4 combined, suggesting that the vast majority of visits of both types are for injuries that are not life-threatening.
3 Methodology
To investigate whether the pandemic and associated behavioral and policy responses changed emergency room visits for abuse and assault, we use a strategy akin to a difference-in-differences design. We contrast emergency room visits in 2020 to the usual seasonal pattern of visits in 2017 and 2018 before and after the onset of the pandemic in March.Footnote 10 Prior year comparison groups are essential to capture the true effect of pandemic behavior change, as many in areas and time periods not under stay-at-home orders nonetheless significantly reduced their mobility (Goolsbee and Syverson 2021) and past work documents significant seasonal variation in domestic violence (Einiö and Elina 2019; Farrell and Pease 1994). This design is similar to that used by Leslie and Wilson (2020), the first to document the increase in domestic violence 911 calls at the beginning of the pandemic. Although this is not a canonical difference-in-differences design with a cross-sectional comparison group, it still identifies the causal effect of the pandemic on domestic violence-related emergency department visits provided that seasonal trends in visits would have been similar in 2020 to those in 2017 and 2018 if the pandemic had not happened.
3.1 Event study
To assess how domestic violence-related visits differed in 2020 from the usual seasonal pattern, we use an event study regression comparing a given two-week period t in 2020 to the same period in 2017 and 2018. Each observation AssaultClaimsawy is at the week level but coefficients are pooled at the two-week period beginning in week τ of the year, or in other words where
as assaults are a relatively rare outcome in some zips and are somewhat noisy at the weekly level.
We estimate:
with the two-week period τ beginning week 9 of the year as the reference period. βt is interpreted as the year-over-year change in assault injury visits in period t of 2020 over the average in the same period in 2017 and 2018. θt is a two-week period fixed effect, and θa is a three-digit zip area fixed effect. Standard errors are clustered at the three-digit zip area level. Results from a similar specification omitting these fixed effects to allow for pandemic-induced migration are presented in Fig. 16 and are similar to the main estimates.
3.2 Pooled difference-in-differences
We pool different phases of the pandemic together based on mobility patterns: the first phase will be the early weeks of the pandemic in which mobility patterns were changing rapidly, and the second phase will be the later weeks of 2020 in which mobility, though lower than before the pandemic, had stabilized considerably. In analyses where several weeks are pooled together, we designate the beginning of the “first phase” of the pandemic from March to June beginning in Week 10, the week mobility patterns began to significantly change (Elarde et al. 2021; Kellermann et al. 2022; Lee et al. 2020). We designate Week 26 at the beginning of the “second phase” from July to December, where some social distancing behavior remained but mobility patterns were more stable, with the exception of holidays (Kim and Kwan 2021 and Elarde et al. 2021).
We estimate the following pooled difference-in-differences specification to obtain an overall estimate of how the number of assault and abuse claims in each phase of the pandemic differed from the usual seasonal average:
where (Mar–Jun) and (Jul–Dec) are indicators for the first and second phase of the pandemic, and the coefficients on the interaction terms β4 and β5 can be interpreted as the change in visits in each phase of the pandemic in 2020 compared to the usual seasonal pattern of claims in those weeks in 2017 and 2018. θa is a three-digit-zip fixed effect and standard errors are clustered at the three-digit-zip level. It should be noted that, based on the pattern of effects in the event studies, the effect appears to be concentrated in the early months of the pandemic. Splitting the pandemic into these two phases in the pooled regression allows us to capture the possibility that some patients who were injured in the first phase of the pandemic may have delayed care or faced different factors determining the decision to seek medical care than in later weeks of the year.
4 Results
4.1 Main results
Our first main finding is that the pandemic and associated shutdowns social distancing measures are associated with decreases in abuse, accident, and female assault visits treated in emergency departments. Figure 2 shows event studies in the number of visits per zip-week, with event study coefficients pooled into two week periods (see Eq. 3) and overall difference-in-difference coefficients pooled into the early and later phases of the pandemic (see Eq. 4). The top left panel contains results for abuse visits, where the provider knows or suspects that the injuries are a result of domestic violence, showing an average decrease of about 0.02 visits per zip-week which translates to a 35% reduction relative to the prior years’ average, between March and June of 2020. The largest decrease, about 0.04 visits per zip-week (68% reduction), occurs in weeks 13–18. Likewise, the top right panel shows results for all female assault visits, showing an average decrease of 0.2 visits per zip-week (30% decrease) over the same period, with the largest decrease (about 0.35 visits per zip-week or about 52%) also occurring in weeks 13–18. Accident visits decreased by 4.48 visits per zip-week (38%) in the early phase, with even larger decreases of about 7 visits per zip-week (roughly 58% decrease) occurring in weeks 13–16. The magnitudes of the declines in accidental visits are in line with those estimated by Cantor et al. (2022) for decreases in preventive care visits for colonoscopies (34% relative reduction) and mammograms (38% relative reduction) immediately after the implementation of shelter-in-place policies, suggesting that the change is likely to be driven by care utilization rather than the number of injuries for which patients would normally seek emergency care.Footnote 11 Lastly, unlike accidental injury and overall assault visits, firearm assault visits increased in the early (March–June) phase of the pandemic by about 0.02 visits per zip-week (45%). This contrasting result would be consistent with some victims forgoing care unless they believe their injuries will be more dangerous than any COVID-19 infection risk or retaliatory violence that may result from accessing emergency medical care.Footnote 12

Main results, all outcomes All event studies include three-digit zip and week-of-year fixed effects and compare zip-week visit counts in 2020 to the same zip-weeks in 2017 and 2018. All outcomes are visit counts at the zip-week level. Event study estimates are results from the specification in Eq. 3 with dotted lines denoting 95% confidence intervals. Pooled difference-in-differences estimates reported below each event study are results from the specification in Eq. 4. ***,**,*,+ denote p < 0.001, p < 0.01, p < 0.05, and p < 0.1, respectively
In the later phase (July to December), accident visits treated in emergency departments reverted towards baseline levels but remained approximately 25% below prior-year averages. In contrast, female assault visits recovered to 16% below prior-year averages. Abuse visits remained 10% lower than prior-year averages, but this difference was not statistically significant as these visits are relatively rare compared to the other visit categories. Gun assault visits remained 47% higher than prior years during this later phase.
The differences between the estimated changes in accidental injury (largest relative decline), abuse and assault (smaller relative decline), and firearm assault (increase) visits are consistent with decreases in care utilization rather than decreases in underlying victimization.Footnote 13 This accords with other studies about domestic violence during the pandemic: Erten et al. (2022) find that 911 calls increased in the early weeks of the pandemic and decreased after the CARES Act economic impact payments were disbursed to eligible households. Miller et al. (2022) show that increases in 911 calls were concentrated prior to the implementation of stay-at-home orders. Because we find more pronounced decreases in assault compared to accident visits during the early period when 911 calls were increasing, it is unlikely that these decreases in visits coincide with decreases in the underlying number of domestic violence injuries that would normally cause victims to seek emergency medical care. Rather, victims likely declined to seek care for other reasons such as COVID-19 risk or increased partner control, which we will explore in Section 4.2. We also compare our main results to those limiting the sample to geographic areas included in Leslie and Wilson (2020), Erten et al. (2022), and Miller et. al. (2022), in Figs. 21 and 22 in Appendix B; our main results, while underpowered, are qualitatively similar in those samples, suggesting that the estimated decrease in emergency department utilization for domestic violence injuries during the early period of increasing 911 calls is unlikely to be driven by geographic differences in sample coverage.
4.2 Mechanisms
We explore the severity of victim injuries to examine how victims with severe injuries sought medical care for their injuries. Figure 3 illustrates that decreases in female assault visits are concentrated in minor injuries (Injury Severity Score Category 1) while severe or life-threatening emergency department visits for female assaults (Injury Severity Score Categories 2–4) remained more stable. Female assault visits for minor injuries declined by 0.50 visits per zip-week (a 32% decrease relative to prior year averages) in the early phase of the pandemic and 0.28 visits per zip-week (18% decrease) in the later phase compared to prior years. By contrast, visits for severe assaults (Injury Severity Score Categories 2–4) were not statistically different from prior years across early and late periods.Footnote 14

Accident, female assault visits by injury severity. All event studies include three-digit zip and week-of-year fixed effects and compare zip-week visit counts in 2020 to the same zip-weeks in 2017 and 2018. All outcomes are visit counts at the zip-week level. Left panel includes accident visits by Injury Severity Score Category. The right panel includes female assault visits by Injury Severity Score Category. Category 1 denotes injuries that are not life threatening. Injury Severity Score Categories 2–4 denote injuries that could severely threaten the life or long-term health of the patient if not treated. These visits are the subset of the female assault visits in Fig. 2 for which injury coding was sufficiently well-populated to calculate the injury severity score. As a result, a few sparse zips have been removed from this sample as providers in those zips did not enter this data. Results showing comparable event studies for all accidental injury and female assault visits with a valid ISS and all accidental injury and female assault visits without a valid ISS are reported in Fig. 15 in Appendix B. Event study estimates are results from the specification in Eq. 3 with dotted lines denoting 95% confidence intervals. Pooled difference-in-differences estimates reported below each event study are results from the specification in Eq. 4. ***,**,*,+ denote p < 0.001, p < 0.01, p < 0.05, and p < 0.1, respectively
The left panel of Fig. 3 shows accident visits by injury severity, indicating that minor injury visits declined by 12.25 visits per zip-week, or 42% of the past years’ average, in the early pandemic months (May–June). Late pandemic minor accidental injury visits declined less relative to prior years, decreasing by 8.61 visits per zip-week in July to December (30% relative decrease). Contrary to severe female assaults which remained stable relative to prior-year averages, severe accidental injuries decreased by almost one visit per zip-week (32% decrease) in the early pandemic months, followed by a decrease of 0.25 visits, or 11%, in later pandemic months.
We supplement this analysis using reports of domestic and intimate partner assaults reported to police during the same timeframe (see Section 4.4, Fig. 4 and Appendix C, Fig. 24) and find similar heterogeneity across injury severity stemming from reported crimes. Domestic violence assaults resulting in major injuries declined by at most 3–4%, suggesting that the large declines in emergency department visits that we find in our sample are unlikely to be driven by decreases in the incidence of domestic violence injuries. Furthermore, changes in reported domestic violence crimes resulting in major injuries are similar whether 2019 is included in or excluded from the comparison time period, suggesting that our choice to exclude it due to poor medical claims data reporting is unlikely to affect our results.

Domestic violence by injury severity in NIBRS, 2020 vs. 2017–2018. All event studies include agency and week-of-year fixed effects and compare agency-week visit counts in 2020 to the same agency-weeks in 2017–2019. All outcomes are incident counts at the agency-week level. Analogous results including 2019 in the comparison period are reported in Appendix Fig. 25. Event study estimates are results from the specification in Eq. 3 with dotted lines denoting 95% confidence intervals. Pooled difference-in-differences estimates reported below each event study are results from the specification in Eq. 4. ***,**,*, and + denote p < 0.001, p < 0.01, p < 0.05, and p < 0.1, respectively
Taken together, heterogeneity by injury severity is suggestive of a decrease in care utilization rather than a decrease in the incidence of domestic violence injuries. Severe female assault visits to the emergency department declined alongside severe accidental injury visits in the early months of the pandemic. However, relative to severe accidents and abuse, severe female assaults returned to prior-year levels in the later phase (July-December) of the pandemic. These estimates would be consistent with either severe injuries increasing during the early phase of the pandemic and victims delaying or forgoing care, or severe injuries remaining stable during the early phase and becoming more likely during the later phase. Either scenario is plausible given that victims’ response to the COVID-19 pandemic may have softened over time leading them to eventually seek care, or victims experiencing domestic violence incidents during the early phase that did not result in significant outside intervention (crime incident report, arrest, or medical care) may have experienced subsequent escalations in violence within the relationship resulting in more severe injuries later in the year.
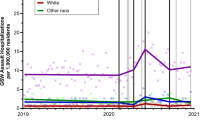
Because the underlying dataset we use to construct our panel consists of insurance claims, a primary concern is that pandemic-related job loss resulted in artificial decreases in claims in our data if patients were no longer eligible to appear in the sample due to loss of insurance but were still visiting emergency departments. To mitigate this concern, we show trends in abuse and female assault visits by insurance payer type in Fig. 5. As described in Section “Data”, “low loss” payers are those associated with government-sponsored insurance programs such as Medicaid, Medicare, and ACA exchange plans, so patients on these plans are less likely to lose their health insurance after a pandemic-related job loss. “Regular commercial” payers are other payers that are likely to contain primarily employer-based plans.Footnote 15

Abuse, female assault visits among low insurance loss groups. All event studies include three-digit zip and week-of-year fixed effects and compare zip-week visit counts in 2020 to the same zip-weeks in 2017 and 2018. All outcomes are visit counts at the zip-week level. Event study estimates are results from the specification in Eq. 3 with dotted lines denoting 95% confidence intervals. Pooled difference-in-differences estimates reported below each event study are results from the specification in Eq. 4. ***,**,*,+ denote p < 0.001, p < 0.01, p < 0.05, and p < 0.1, respectively
Figure 5 displays similar trends in female assault visits across low-loss payers and regular commercial payers, suggesting that pandemic-induced decreases in visits are unlikely to be driven by patients’ exit from the sample due to insurance loss and likely reflect actual decreases in emergency medical care utilization by domestic violence victims. Relative to the full sample (Fig. 2), where abuse visits fell in the early stages of the pandemic by approximately 31%, visits from patients insured by “low-loss” payers declined by 40% and commercial payers declined by 31%. Similarly, relative to the 30% reduction in assault visits during the early stage of the pandemic, among “low-loss” payers, assault visits dropped by 30% and visits from patients with commercial insurance decreased by 28%.
We also explore additional heterogeneity in care-seeking behavior; how victims may have elected to forgo care for pandemic-related reasons such as increased partner control due to increased time at home together. We examine the timing of domestic violence visits to examine if changes in time spent at home during lockdowns altered medical care timing. Prior to the pandemic, victims may have been more able to seek care on weekdays while their partners were at work. Detailed in Fig. 18 in Appendix B, we do not find strong evidence that the pandemic shifted the timing of visits within the week in response to changes in victims’ or abusive partners’ work schedules or likelihood of working from home versus outside the home, but cannot fully rule out a partner control mechanism given the nature of our data. We also document that victims in areas with lower care utilization early in the pandemic, who were more likely to forgo care during those early weeks, remained less likely to seek care later in the year (see Appendix C, Fig. 19).
4.3 Robustness
Figure 6 shows the robustness of the main results to an alternative sample in which we drop “sparse zips” – those where assault and abuse visits are the most rare due to having few billing providers in our sample. We classify a zip as sparse if there is at least one year in the panel where providers in that three-digit zip do not report any assault or abuse visits. This sample drops the majority of the main sample (270 out of 449 zips, or 60%), as the sample inclusion criterion for this check is quite strict and assault visits are a relatively rare outcome. This sample likely reflects an estimate of declines in care utilization for the subset of billing providers who have particularly good coverage in our sample and are located in populous areas. The top left panel shows results for abuse visits; in the early phase of the pandemic, abuse visits decline by about 32% of the zip-week mean in the main sample and about 70% of the zip-week mean in this sample where sparse zips are dropped; this is unsurprising, as the three-digit zips with more assault visits provide most of the variation. We see a similar pattern for female assault visits in the top right panel: in the early phase, female assault visits in the sample dropping sparse zips decline by about 67% (compared to 30% in the main sample) and by about 37% in the later phase (compared to 17% in the main sample).

Main outcome visits (abuse, female assault, accident, firearm assaults) without sparse three-digit zips All event studies include three-digit zip and week-of-year fixed effects and compare zip-week visit counts in 2020 to the same zip-weeks in 2017 and 2018. All outcomes are visit counts at the zip-week level. Event study estimates are results from the specification in Eq. 3 with dotted lines denoting 95% confidence intervals. Pooled difference-in-differences estimates reported below each event study are results from the specification in Eq. 4. ***,**,*,+ denote p < 0.001, p < 0.01, p < 0.05, and p < 0.1, respectively
We also show an alternative specification that removes three-digit zip fixed effects to allow for the possibility of pandemic-induced migration in Appendix B, Fig. 16. Results from this specification are also similar to the main results, suggesting that the main results are not affected by pandemic-induced migration across zips in our sample.
Figure 7 presents results from a placebo test comparing results in 2018 to those in 2017, to ensure that the main results are not simply a product of secular decreasing trends in emergency department use for injuries. We do find some changes in visits across the two comparison years. For example, in the placebo test for our most frequent domestic violence outcome of female assault visits, we find no statistically significant change in weeks 10–25, and a small but statistically significant decrease in weeks 26–52, resulting in about 0.05 fewer visits per zip-week (−7%) in 2018 than in 2017. These estimated changes are small compared to the estimated 30% decline in the first phase of the pandemic and the 16% decline in the second phase of the pandemic in the main results (Fig. 2), suggesting that the decline in care utilization for domestic violence injuries cannot be driven only by this secular trend. Results for accidental injury visits are similar; we estimate a statistically significant decline in visits, albeit smaller than that estimated in the main results in Fig. 2. Figure 17 in Appendix B also presents results comparing visits in 2020 to 2018, excluding 2017 as a comparison year. Results are similar to the main results in Fig. 2.

2017–2018 Placebo tests All event studies include three-digit zip and week-of-year fixed effects. Event studies compare zip-week visit counts in 2018 to 2017 as a placebo test. All outcomes are visit counts at the zip-week level. Event study estimates are results from the specification in Eq. 3 with dotted lines denoting 95% confidence intervals. Pooled difference-in-differences estimates reported below each event study are results from the specification in Eq. 4. ***,**,*,+ denote p < 0.001, p < 0.01, p < 0.05, and p < 0.1, respectively
To mitigate the influence of any potential secular declines in emergency department utilization, we estimate two additional specifications. Figure 8 presents results from the following first-differences event study specification,

Robustness to secular trends All event studies include three-digit zip and week-of-year fixed effects and compare year-over-year changes in visit counts at the three-digit zip level from 2018–2020 to those from 2017–2018. All outcomes are year-over-year changes in visit counts at the zip-week level. Event study estimates are results from the specification in Eq. 3 with dotted lines denoting 95% confidence intervals. Pooled difference-in-differences estimates reported below each event study are results from the specification in Eq. 4. ***,**,*,+ denote p < 0.001, p < 0.01, p < 0.05, and p < 0.1, respectively
as well as the following difference-in-first-differences specification,
in which ∆AssaultClaimsawy is the change in the number of visits in week w of the current year compared to week w of the previous year in the sample (2020 vs. 2018 or 2018 vs. 2017). This specification should eliminate the influence of any secular declining trends in visits. We are unable to detect any statistically significant changes in abuse or firearm assault visits when using this specification to control for secular trends; these outcomes are the most rare, and appear to experience the largest relative changes from 2017 to 2018 in Fig. 7, although the absolute changes are small. This warrants caution in interpreting the main results for these two outcomes, and we do not recommend relying on results for these outcomes in isolation. We do find, however, a decline in female assault visits of 0.16 visits per zip-week (−23%) in the early phase of the pandemic. As in the main results, the corresponding change in accidental injury visits is larger in percentage terms (−33%) than that for female assault visits. The totality of these results suggests that the decline in female assault visits, which are likely to primarily consist of domestic violence visits, cannot be driven only by secular declining trends in emergency department use and is likely to be driven by declines in care utilization rather than decreases in violence.
Lastly, Table 3 presents results from the pooled difference-in-differences specification (Eq. 4) manipulating the threshold between the “first phase” and the “second phase” of the pandemic. Results do not appear sensitive to this choice, as they are nearly identical if this threshold is moved either two weeks earlier or two weeks later.
4.4 Comparisons with reported domestic violence
To compare our injury visit results to a concurrent measure of domestic violence injuries not affected by medical care utilization, we explore changes in domestic violence using data reported by police to the (FBI through the nation’s crime surveillance system), NIBRS. NIBRS records granular data from police agencies documenting the nature of the crime, victim, and perpetrator relationships, as well as whether the crime resulted in an injury. While NIBRS data is detailed, currently the sample covers only approximately 60% of the U.S. population as police agencies have slowly adopted the crime reporting system.
We create a panel of agencies who reliably report data to NIBRS in each month from 2017–2020. We include only those agencies who report at least one crime per month in each month during our sample period.Footnote 16 We identify intimate partner and domestic violence crimes using information about the victim-perpetrator relationship.Footnote 17 For all analyses using the NIBRS data, we compare results across two samples: (1) including panel data observations of crimes that occurred in 2019 in the comparison period and (2) excluding crimes that occurred in 2019 as we did in the main analysis due to the data reporting anomaly in the medical claims data. Because all NIBRS results are similar whether 2019 is included or excluded, we can reasonably assume our main results are unaffected by the exclusion of 2019 in the claims data.
Figure 9 presents trends in reported nonfatal domestic violence incidents in NIBRS for each sample. Non-fatal domestic violence incidents recorded by police declined by about 3.5% in the early phase of the pandemic in 2020 compared to the same weeks of the year in 2017–2019, or by about 3.8% compared to the same weeks in 2017–2018, the years used as our comparison period in the medical claims data.Footnote 18 Importantly, the percentage decline in reported domestic violence incidents is much smaller than that in emergency department visits, providing further evidence that the changes in emergency department visits are driven primarily by decreased healthcare utilization rather than by decreases in domestic violence.

Nonfatal domestic violence incidents in NIBRS. All event studies include agency and week-of-year fixed effects and compare agency-week visit counts in 2020 to the same agency-weeks in 2017–2019. All outcomes are incident counts at the agency-week level. Event study estimates are results from the specification in Eq. 3 with dotted lines denoting 95% confidence intervals. Pooled difference-in-differences estimates reported below each event study are results from the specification in Eq. 4. ***,**,*, and + denote p < 0.001, p < 0.01, p < 0.05, and p < 0.1, respectively
Figure 10 presents results for reported domestic violence incidents involving guns. Consistent with the increases in emergency department visits for firearm assaults reported in the main results in Fig. 3, police departments in the NIBRS sample recorded more domestic violence incidents involving guns after the onset of the pandemic than in prior years. These incidents increased by about 28% in the early phase of the pandemic and about 36% in the later part of 2020. However, because the results for firearm assault visits in the medical claims analysis are not robust to the adjustments in Figs. 7 and 8 (Section 4.3), we caution against over-interpretation of comparisons between the two data sources. Figure 13 in Appendix B disaggregates firearm assault visits by gender and presents results showing increases in firearm assault visits among both men and women as well as increases in accidental firearm injuries among men, suggesting that increases in gun purchasing at the onset of the pandemic (Crifasi et al. 2021) may play a role in the increase in domestic violence incidents using firearms.

Domestic violence incidents involving firearms in NIBRS. All event studies include agency and week-of-year fixed effects and compare agency-week visit counts in 2020 to the same agency-weeks in 2017–2019. All outcomes are incident counts at the agency-week level. Event study estimates are results from the specification in Eq. 3 with dotted lines denoting 95% confidence intervals. Pooled difference-in-differences estimates reported below each event study are results from the specification in Eq. 4. ***,**,*, and + denote p < 0.001, p < 0.01, p < 0.05, and p < 0.1, respectively
Figure 5 presents results for reported domestic violence incidents by severity of injuries recorded by police. Minor injuries are defined as all injuries recorded in NIBRS as “apparent minor injuries,” and no further detail is available regarding the nature of these injuries. We create a pooled major injury category that includes injuries that are categorized as apparent broken bones, other possible internal injury, severe laceration, unconsciousness, and “other major injury.” No further detail is reported for the “other major injury” category.Footnote 19
It is important to note that it is not possible to standardize injury severity measures across our two data sources; police may subjectively classify injuries as “apparent minor injuries” or “other major injury,” and these two categories make up a large proportion of injuries recorded in NIBRS. As a result of this, there is not a 1:1 mapping between severe injuries in NIBRS and severe injuries in the injury severity analysis in the emergency department data reported in Fig. 4. Additionally, the total universe of injuries is different. Recall that all injuries in the medical claims analysis must be severe enough to warrant an emergency department visit in the first place; while most of the specific injuries recorded in our “major injury” category in NIBRS would seem to warrant emergency medical attention, it is unclear whether all of the injuries recorded as “other major injury” or “apparent minor injuries” would be likely to result in an emergency department visit, either before or during the pandemic. Despite this limitation, the results presented in Fig. 5 are consistent with the medical visits by injury severity in Fig. 4 in the sense that, within each dataset, victims are more likely to be selected into either receiving medical attention or having their victimization recorded by police if their injuries are more severe.
While results using NIBRS data are unlikely to be affected by medical care utilization, they reflect a different combination of latent variables that could be changing as a result of the pandemic. Just as Eq. 2 indicates that any changes in domestic violence-related medical visits in the COVID-19 research database reflect a combination of total incidence of domestic violence injuries and other factors, changes in NIBRS incidents may reflect changes in rates of domestic violence victimization, the likelihood that a victim or witness calls the police, and the likelihood that police responding to the call determine and report that a crime has occurred. The existing literature finds that domestic violence 911 calls increased during the weeks when we find large decreases in emergency department use (Erten et al. 2022; Leslie and Wilson 2020; Miller et al. 2022). In contrast, police propensity to record a criminal incident or make an arrest decreased during the same time period, both for domestic violence and for other crimes (Bullinger et al. 2021; Miller et al. 2022). Our findings suggest that both police reporting and emergency department use are selected on severity. Fig. 26 in Appendix C shows that we detect no significant change in domestic violence homicides within the NIBRS sample, which are the least likely to be affected by reporting.
5 Conclusion
Overall, we find that visits for domestic violence injuries declined considerably in the early phase of the pandemic from March to June of 2020. Visits recovered in the later months of the year but remained lower than prior years. We find that the decline is driven almost entirely by less severe injuries; visits for severe or life-threatening injuries remain stable in the early phase of the pandemic and increase in the later phase. The decline in assault visits is also smaller in magnitude than both our estimated decrease in accidental injury visits and previously documented decreases in preventative care visits, suggesting that decreases in visits are driven by declines in emergency department use rather than declines in actual injuries; if anything, this difference in percentage changes between female assault visits and accidental injury visits suggests an increase in the incidence of domestic violence injuries. Evidence from domestic violence crimes recorded by police show small declines in incidence of domestic violence, suggesting further that changes in emergency department visits are due to declining healthcare utilization rather than decreased violence. Furthermore, trends in assault claims are similar across insurance types, confirming that the decline in claim counts is likely to be driven by actual declines in the number of visits rather than a mechanical effect of patients exiting the sample due to insurance loss.
The totality of our results, in combination with the findings in the literature documenting an increase in domestic violence 911 calls and a decrease in medical visits at the onset of the pandemic, leads us to conclude that while domestic violence injuries were likely increasing in the early weeks of social distancing behavior, victims were less likely to receive emergency medical care for their injuries, particularly those injuries that were not life-threatening. This finding reconciles several studies focused on single-site trauma centers reporting increases in domestic violence injuries, which may reflect treatment of more severe injuries than emergency departments without trauma centers and several other single-site studies finding decreases in victims’ emergency department use. Our larger sample spanning diverse providers and settings suggests that focuses on single sites may mask broader trends in domestic violence, namely a substantial decline in treatment in the majority of care settings.
Our findings have obvious implications for future studies of domestic violence that encompass the time period of the COVID-19 pandemic; medical visits are often an excellent proxy for domestic violence that may go unreported, but changes in care utilization during this time period warrant the use of alternative measures. However, our results throughout the paper highlight that both medical care utilization and domestic violence reporting in police data are selected on severity. This finding has implications for the measurement of domestic violence more generally; researchers studying domestic violence may be able to use similar heterogeneity analysis to evaluate the extent to which they are detecting changes in domestic violence incidence or domestic violence reporting and detection.
Our findings also raise questions about victims’ access to other preventative services in times of crisis. Medical providers often screen for domestic violence and sometimes provide referrals to safety planning, mental health services, and victim advocacy groups when abuse is confirmed or suspected (Fraze et al. 2019; Ford-Gilboe et al. 2020; Hegarty et al. 2019; Bloom et al. 2014; Ragavan et al. 2020; Gray et al. 2015), resulting in changes in victims’ efforts to keep themselves safe from re-victimization. While more work is needed on the effects of hospital-based assessments and referrals on re-victimization morbidity and lethality, our findings imply that policy responses to future public health crises or other shocks that reduce emergency medical care utilization may benefit from alternative outreach strategies to identify and support victims of domestic violence that increase take-up of preventative services otherwise offered by medical providers.
Notes
We considered including urgent care providers, but they comprised only 4% of billing providers who (1) consistently appeared in our dataset and (2) reported at least one assault in the data, so we elected to drop them.
Our data use agreement does not permit us to disclose the name of the claims aggregator that provides the data to the COVID-19 Research Database. Several aggregators provide datasets to the database, and researchers are discouraged from requesting access to multiple datasets, so we limit our analysis to a single claims dataset.
We define “regular residential” three-digit zips as those that are still in use and are not designated for a special purpose such as government, IRS, military, and parcel return. By this definition there are 895 regular residential three-digit zips.
The claims aggregator informed us that claims are reported to the dataset by billing providers, not by insurance payers, which informed this choice. They were unable to provide further information about how claims are selected into the dataset, which led us to develop this approach to ensure a consistent sample.
Appendix C reports results using this same strategy to estimate changes in police reports for domestic violence using NIBRS data, and these results suggest that trends in domestic violence in 2019 were not meaningfully different from those in 2017–2018 and the choice to exclude 2019 from the comparison period should not meaningfully affect any estimated changes at the onset of the pandemic.
While institutional or hospital bills have valuable information and may capture a somewhat larger proportion of the universe of emergency department claims than a provider-based definition of emergency department services (Venkatesh et al. 2016), in practice, the claims data aggregator masks fields that would enable identification of inpatient vs. outpatient visits on institutional claims.
We considered including urgent care providers, but they comprised only 4% of billing providers who (1) consistently appeared in our dataset and (2) reported at least one assault in the data, so we elected to drop them.
BB guns, paintball guns, and air guns are the only types of firearms excluded from firearm assaults.
We use the open source ICDpicr package for Injury Categorization in R.
We omit 2019 from the comparison group, as the claims aggregator has informed us that there was a claims reporting issue in the summer of 2019 that caused claim counts to be artificially lower during that time.
Cantor et al. (2022) present various estimates controlling for differential COVID-19 risk conditions leading jurisdictions to implement shelter-in-place policies at different times. We focus on estimating the overall effect of the pandemic and associated behavior changes, so we opt to compare to the usual seasonal pattern from prior years and designate all areas as treated at the same time. Furthermore, in estimating the accidental injury visit changes as a care utilization benchmark, we include visits by all adult patients. Changes in accidental injury visits by gender are presented in Appendix B, Fig. 14, and show that the decline in visits was similar across men and women.
Due to limited statistical power, we present firearm assault visits for all adult patients in the main results. Results disaggregated by gender are presented in Appendix B, Fig. 13.
In some robustness checks in Section 4.3, we find no change in abuse or firearm assault visits; we still find decreases in both female assault and accidental injury visits, where the decline in accidental injury visits is larger in percentage terms than that for assault visits. This pattern is still consistent with changes being driven by care utilization rather than domestic violence incidence.
Some visits (and therefore some zips) are excluded from the ISS analysis because they did not report sufficient diagnosis code information to estimate the ISS. Figure 15 in Appendix B shows that results are similar across visits with any valid ISS and visits with a missing ISS, suggesting that ISS missingness is not selected on likelihood of seeking care.
Appendix B Fig. 20 presents analogous results comparing Medicaid payers to non-Medicaid payers, but non-parallel pre-trends and limited statistical power among Medicaid payers warrant caution in interpreting these results.
This is standard practice when using NIBRS data, as there is no reliable way to differentiate between no crimes occurring and no crimes reported. For details, see guidance on appropriate use of NIBRS data from Kaplan (2021).
Family relationships to the victim included in domestic violence are: victim was parent, victim was sibling, victim was spouse, victim was step-child, victim was step-parent, victim was step-sibling, victim was other family member, victim was child, victim was child of boyfriend/girlfriend, victim was grandchild,victim was grandparent, victim was in-law. Intimate partner relationships included are: victim was boyfriend/girlfriend, victim was in a homosexual relationship with the offender, victim was common-law spouse, victim was ex-spouse, victim was spouse. All incidents with an intimate partner relationship are included as a subset of domestic violence incidents.
Changes in reported intimate partner violence incidents and in domestic violence homicides are reported in Appendix C. Declines in IPV incidents are similar to those for all DV incidents, and we detect no change in DV homicides.
Figure 25 in Appendix C shows that, like the other NIBRS estimates, these results are similar when including 2019 as a comparison year.
References
Aizer, A. (2010). The gender wage gap and domestic violence. American Economic Review, 100, 1847–1859.
Albanesi, S., & Kim, J. (2021). Effects of the COVID-19 recession on the US labor market: Occupation, family, and gender. Journal of Economic Perspectives, 35(3), 3–24.
Arenas-Arroyo, E., Fernandez-Kranz, D., & Nollenberger, N. (2021). Intimate partner violence under forced cohabitation and economic stress: Evidence from the COVID-19 pandemic. Journal of Public Economics, 194, 104350.
Barber, C., Cook, P. J., & Parker, S. T. (2022). The emerging infrastructure of US firearms injury data. Preventive Medicine, 165, 107129.
Barret, M. (2016). HCUP External Cause of Injury (E-Code) Evaluation Report. US Department of Health and Human Services Agency for Healthcare Research and Quality. Report #2016-03. https://hcup-us.ahrq.gov/reports/methods/2016-03.pdf.
Berniell, I., & Facchini, G. (2021). COVID-19 lockdown and domestic violence: Evidence from internet-search behavior in 11 countries. European Economic Review, 136, 103775.
Bloom, T. L. et al. (2014). Feasibility of an online safety planning intervention for rural and urban pregnant abused women. Nursing Research, 63, 243–251.
Braga, A. A., & Cook, P. J. (2018). The association of firearm caliber with likelihood of death from gunshot injury in criminal assaults. JAMA Network Open, 1(3), e180833–e180833.
Brown, E. C. B. et al. (2023). ICD-10-CM codes for the identification of abusive head trauma in administrative datasets. Academic Pediatrics, 23(2), 410–15.
US Preventive Services Task Force. (2018). Screening for intimate partner violence, elder abuse, and abuse of vulnerable adults: US Preventive Services Task Force final recommendation statement. JAMA, 320(16), 1678–87.
Bullinger, L. R., Carr, J. B., & Packham, A. (2021). COVID-19 and crime: effects of stay-at-home orders on domestic violence. American Journal of Health Economics, 7(3), 249–80.
Bullinger, L. R., Boy, A., Messner, S., & Self-Brown, S. (2021). Pediatric emergency department visits due to child abuse and neglect following COVID-19 public health emergency declaration in the southeastern United States. BMC Pediatrics, 21(1), 401.
Bundorf, M. K., Gupta, S., & Kim, C. (2021). Trends in US health insurance coverage during the COVID-19 pandemic. JAMA Health Forum, 2(9), e212487.
Cajner, T. et al. (2020). The U.S. labor market during the beginning of the pandemic recession. https://www.nber.org/papers/w27159 (December 23, 2022).
Cantor, J. et al. (2022). The impact of the COVID-19 pandemic and policy response on health care utilization: evidence from county-level medical claims and cellphone data. Journal of Health Economics, 82, 102581.
Clark, D. E., Black, A. W., Skavdahl, D. H., & Hallagan, L. D. (2018). Open-access programs for injury categorization using ICD-9 or ICD-10. Injury Epidemiology, 5(1), 11.
Crifasi, C. K., Ward, J. A., McGinty, E. E., Webster, D. W., & Barry, C. L. (2021). Gun purchasing behaviours during the initial phase of the COVID-19 pandemic, March to mid-July 2020. International Review of Psychiatry, 33(7), 593–597.
Drotning, K. J. et al. (2023). Not all homes are safe: family violence following the onset of the Covid-19 pandemic. Journal of Family Violence, 38(2), 189–201.
Einiö, M. K. & Elina, E. (2019). Seasonal variation in seeking help for domestic violence based on Google search data and Finnish police calls in 2017 - Eeva M. Koutaniemi, Elina Einiö. Scandinavian Journal of Public Health. https://doi.org/10.1177/1403494819834098 (April 13, 2020).
Elarde, J. et al. (2021). Change of human mobility during COVID-19: A United States case study. PLoS ONE, 16(11), e0259031.
Erten, B., Keskin, P., & Prina, S. (2022). Social distancing, stimulus payments, and domestic violence: Evidence from the US during COVID-19. AEA Papers and Proceedings, 112, 262–266.
Farrell, G., & Pease, P. (1994). CRIM SEASONALITY: Domestic disputes and residential burglary in merseyside 1988–90. The British Journal of Criminology, 34(4), 487–98.
Felson, R. B., & Paré, P.-P. (2005). The reporting of domestic violence and sexual assault by nonstrangers to the police. Journal of Marriage and Family, 67(3), 597–610.
Felson, R. B., Messner, S. F., Hoskin, A. W., & Deane, G. (2002). Reasons for reporting and not reporting domestic violence to the police*. Criminology, 40(3), 617–48.
Ford-Gilboe, M. et al. (2020). Longitudinal impacts of an online safety and health intervention for women experiencing intimate partner violence: randomized controlled trial. BMC Public Health, 20, 260.
Fowler, K. A., Dahlberg, L. L., Haileyesus, T., & Annest, J. L. (2015). Firearm Injuries in the United States. Preventive Medicine, 79, 5–14.
Fraze, T. K. et al. (2019). “Prevalence of screening for food insecurity, housing instability, utility needs, transportation needs, and interpersonal violence by US physician practices and hospitals.” JAMA Network Open, 2(9), e1911514.
Ghidei, W. et al. (2023). Examining the effectiveness, acceptability, and feasibility of virtually delivered trauma-focused domestic violence and sexual violence interventions: A rapid evidence assessment. Trauma Violence Abuse, 24, 1427–1442.
Gold, L. H. (2020). Domestic violence, firearms, and mass shootings. The Journal of the American Academy of Psychiatry and the Law, 48(1), 35–42.
Goolsbee, A., & Syverson, C. (2021). Fear, lockdown, and diversion: comparing drivers of pandemic economic decline 2020. Journal of Public Economics, 193, 104311.
Gray, M. J. et al. (2015). Provision of evidence-based therapies to rural survivors of domestic violence and sexual assault via telehealth: Treatment outcomes and clinical training benefits. Training and Education in Professional Psychology, 9, 235–241.
Griffing, S., et al. (2002). Domestic violence survivors’ self-identified reasons for returning to abusive relationships. Journal of Interpersonal Violence, 17(3), 306–19.
Hegarty, K. et al. (2019). An online healthy relationship tool and safety decision aid for women experiencing intimate partner violence (I-DECIDE): a randomised controlled trial. Lancet Public Health, 4, e301–e310.
Hoehn-Velasco, L., Silverio-Murillo, A., & de la Miyar, J. R. B. (2021). The Great Crime Recovery: Crimes against Women during, and after, the COVID-19 Lockdown in Mexico. Economics & Human Biology, 41, 100991.
Hsu, L.-C., & Henke, A. (2021). COVID-19, staying at home, and domestic violence. Review of Economics of the Household, 19(1), 145–55.
Ivandic, R., Kirchmaier, T. & Linton, B. (2020) Changing patterns of domestic abuse during Covid-19 lockdown. https://econpapers.repec.org/paper/ehllserod/108483.htm.
Jennings, W. G., & Perez, N. M. (2020). The immediate impact of COVID-19 on law enforcement in the United States. American Journal of Criminal Justice, 45(4), 690–701.
Junghwan, K., & Kwan, M. P. (2021). The impact of the COVID-19 pandemic on people’s mobility: A longitudinal study of the U.S. from March to September of 2020. Journal of Transport Geography, 93, 103039.
Kaplan, J. (2021). National incident-based reporting system (NIBRS) data: A practitioner’s guide. Computer Software Manual. Retrieved January 2, 2021. https://nibrsbook.com/.
Kellermann, R. et al. (2022). Mobility in pandemic times: Exploring changes and long-term effects of COVID-19 on urban mobility behavior. Transportation Research Interdisciplinary Perspectives, 15, 100668.
Kim, J., & Kwan, M. P. (2021). The impact of the COVID-19 pandemic on people’s mobility: A longitudinal study of the US from March to September of 2020. Journal of Transport Geography, 93, 103039.
Koppa, V. (2022). Can information save lives? effect of a victim-focused police intervention on intimate partner homicides. Effect of a Victim-focused Police Intervention on Intimate Partner Homicides (August 1, 2022). Forthcoming at Journal of Economic Behavior and Organization.
Kothari, C. L., & Rhodes, K. V. (2006). Missed opportunities: Emergency department visits by police-identified victims of intimate partner violence. Annals of Emergency Medicine, 47(2), 190–99.
Lauritsen, J., & Heimer, K. (2012). Gender and violent victimization, 1973–2005 [United States]: Archival Version. http://www.icpsr.umich.edu/icpsrweb/NACJD/studies/27082 (April 5, 2023).
Law, R. K. et al. (2022). Injury-related emergency department visits during the COVID-19 pandemic. American Journal of Preventive Medicine, 63(1), 43–50.
Lee, M. et al. (2020). Human mobility trends during the early stage of the COVID-19 pandemic in the United States. PLoS ONE, 15(11), e0241468.
Leslie, E., & Wilson, R. (2020). Sheltering in place and domestic violence: Evidence from calls for service during COVID-19. Journal of Public Economics, 189, 104241.
McCrary, J., & Sanga, S. (2021). The impact of the coronavirus lockdown on domestic violence.”. American Law and Economics Review, 23(1), 137–63.
Messing, J. T., Campbell, J., Webster, D. W., Brown, S., Patchell, B., & Wilson, J. S. (2015). The Oklahoma lethality assessment study: A quasi-experimental evaluation of the lethality assessment program. Social Service Review, 89(3), 499–530.
Miller, A. R., Segal, C., & Spencer, M. K. (2022). Effects of COVID‐19 shutdowns on domestic violence in US Cities. Journal of Urban Economics, 131, 103476.
Miller, A. R., Segal, C. & Spencer, M. K. (2020). Effects of the COVID-19 pandemic on domestic violence in Los Angeles. https://papers.ssrn.com/abstract=3727143 (December 23, 2022).
Muldoon, K. A. et al. (2021). COVID-19 Pandemic and violence: Rising risks and decreasing urgent care-seeking for sexual assault and domestic violence survivors. BMC Medicine, 19(1), 20.
Pallansch, J. et al. (2022). Intimate partner violence, sexual assault, and child abuse resource utilization during COVID-19. Western Journal of Emergency Medicine, 23(4), 589–96.
Perez-Vincent, S. M., & Carreras, E. (2022). Domestic violence reporting during the COVID-19 pandemic: Evidence from Latin America. Review of Economics of the Household, 20(3), 799–830.
Petridou, E. T. H. & Antonopoulos, C. N. (2017) Injury epidemiology. In S. R. Quah (Eds.), International encyclopedia of public health. (2nd ed., pp. 258–74). Oxford: Academic Press. https://www.sciencedirect.com/science/article/pii/B9780128036785002332.
Ragavan, M. I., Ferre, V., & Bair-Merritt, M. (2020). Thrive: A novel health education mobile application for mothers who have experienced intimate partner violence. Health Promotion Practice, 21, 160–164.
Rahman, R., Huysman, C., Ross, A. M., & Boskey, E. R. (2022). Intimate partner violence and the COVID-19 pandemic. Pediatrics, 149(6), e2021055792.
Rasooly, I. R. et al. (2023). Validating use of ICD-10 diagnosis codes in identifying physical abuse among young children. Academic Pediatrics, 23(2), 396–401.
Ravindran, S., & Shah M. (2020). Unintended Consequences of Lockdowns: COVID-19 and the Shadow Pandemic. https://www.nber.org/papers/w27562 (June 16, 2023).
Rebbe, R. et al. (2023). The measurement of intimate partner violence using international classification of diseases diagnostic codes: a systematic review. Trauma, Violence, & Abuse, 24(4), 2165–80. https://doi.org/10.1177/15248380221090977.
Rhodes, K. V. et al. (2011). Intimate partner violence identification and response: Time for a change in strategy. Journal of General Internal Medicine, 26(8), 894–99.
Rhodes, H. X. et al. (2020). COVID-19 Resilience for Survival: Occurrence of domestic violence during lockdown at a rural American College of Surgeons verified level one trauma center. Cureus, 12(8). https://www.cureus.com/articles/37222-covid-19-resilience-for-survival-occurrence-of-domestic-violence-during-lockdown-at-a-rural-american-college-of-surgeons-verified-level-one-trauma-center (June 16, 2023).
Seff, I., Vahedi, L., McNelly, S., Kormawa, E., & Stark, L. (2021). Remote evaluations of violence against women and girls interventions: a rapid scoping review of tools, ethics and safety. BMJ Global Health, 6, e006780
Silverio-Murillo, A., de la Miyar J. B., & Lauren H. V. (2023). Families under confinement: COVID-19 and domestic violence. In crime and social control in pandemic times, sociology of crime, Law and deviance, Mathieu deflem ed. Emerald Publishing Limited, 23–41. https://doi.org/10.1108/S1521-613620230000028003 (June 9, 2023).
Smith, R. N. et al. (2022). Intimate partner violence at a level-1 trauma center during the COVID-19 pandemic: An interrupted time series analysis. The American Surgeon, 88(7), 1551–53.
Tjaden, P., & Thoennes, N. (1998). Prevalence, incidence, and consequences of violence against women: Findings From the National Violence Against Women Survey, Research in Brief National Institute of Justice. https://nij.ojp.gov/library/publications/prevalence-incidence-and-consequences-violence-against-women-findings-national (December 23, 2022).
Uniform Data System. (2021) Health Center Data Reporting Requirements. 2021. Health Resources and Services Administration -Bureau of Primary Health Care. https://bphc.hrsa.gov/sites/default/files/bphc/data-reporting/2021-uds-manual.pdf.
Venkatesh, A. K., Mei, H., Kocher, K., Spatz, E., Granovsky, M., Eichenfeld, J., ... & Lin, Z. (2016). 143 Improving the Identification of Emergency Department Visits in Medicare Administrative Claims. Annals of Emergency Medicine, 68(4), S57–S58.
Acknowledgements
We thank the COVID-19 Research Database for invaluable resources and platforms and we thank the COVID-19 Research Accelerator Program (administered by the Health Care Cost Institute and funded by the Bill and Melinda Gates Foundation Grant #INV-031351) and the Walter J. McInerney Award at the University of Michigan for funding enabling our work.
Author information
Authors and Affiliations
Contributions
L.G. contributed to research design, literature review, and manuscript drafting. S.P. prepared all datasets for analysis and contributed to research design and manuscript drafting. L.S. conducted analyses and prepared all tables and figures, and contributed to research design and manuscript drafting. All authors reviewed the manuscript before submission.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Gilbert, L., Parker, S. & Schechter, L. The impact of the COVID-19 pandemic on treatment for domestic violence injuries: evidence from medical claims. Rev Econ Household 22, 535–562 (2024). https://doi.org/10.1007/s11150-024-09696-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11150-024-09696-8