
Abstract
Objective
This study aims to investigate the effect of physical violence and serious injury on health-related quality of life in the Australian adult population.
Methods
This study utilised panel data from the Household, Income and Labour Dynamics in Australia (HILDA) Survey. HRQoL was measured through the physical component summary (PCS), mental component summary (MCS), and short-form six-dimension utility index (SF-6D) of the 36-item Short-Form Health Survey (SF-36). Longitudinal fixed-effect regression models were fitted using 19 waves of the HILDA Survey spanning from 2002 to 2020.
Results
This study found a negative effect of physical violence and serious injury on health-related quality of life. More specifically, Australian adults exposed to physical violence and serious injury exhibited lower levels of health-related quality of life. Who experienced physical violence only had lower MCS (β = −2.786, 95% CI: −3.091, −2.481) and SF-6D (β = −0.0214, 95% CI: −0.0248, −0.0181) scores if switches from not experiencing physical violence and serious injury. Exposed to serious injury had lower PCS (β = −5.103, 95% CI: −5.203, −5.004), MCS (β = −2.363, 95% CI: −2.480, −2.247), and SF-6D (β = −0.0585, 95% CI: −0.0598, −0.0572) score if the adults not experiencing physical violence and serious injury. Further, individuals exposed to both violence and injury had substantially lower PCS (β = -3.60, 95% CI: -4.086, -3.114), MCS (β = −6.027, 95% CI: −6.596, −5.459), and SF-6D (β = −0.0716, 95% CI: −0.0779, −0.0652) scores relative to when the individuals exposed to none.
Conclusion
Our findings indicate that interventions to improve Australian adults’ quality of life should pay particular attention to those who have experienced physical violence and serious injury. Our findings suggest unmet mental health needs for victims of physical violence and serious injuries, which calls for proactive policy interventions that provide psychological and emotional therapy.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Globally, physical violence remains one of the major causes of injuries that result in deaths and disabilities [1, 2]. Despite the adoption of the World Health Organisation’s Resolution WHA49.25 in 1996, which called for the implementation of programmes to prevent the occurrence of violence [3, 4], the global burden of physical violence remains high [2]. In 2016, for instance, interpersonal physical violence resulted in approximately 390,800 deaths across the world [2]. It is currently ranked the 26th cause of disability-adjusted life years (DALYs) worldwide, having declined marginally from the 24th position over the past three decades [2]. Physical violence-related injuries and associated deaths and disabilities are mostly preventable and occur mainly among youth and young adults aged 15–44 years [3, 4]. In Australia, approximately 3.7 million men (4 in 10 men) and 2.9 million women (3 in 10 women) aged 18 years and over have experienced physical violence since age 15 [5]. Additionally, injuries, including interpersonal physical violence-related injuries, are among the top five contributors to DALYs and the national burden of diseases in Australia (Australian Institute of Health and Welfare, 2020). For example, in 2015–2016, injuries accounted for 7.6% (8.9 billion dollars) of the Australian healthcare system’s total healthcare expenditure [6].
Physical violence involves the intentional use of physically aggressive acts such as beating, kicking, and strangling another person or group that could result in injury or have a high tendency to cause injury or death [4, 7]. It is often perpetrated by close acquaintances (e.g. intimate partners, friends, and parents) and is mostly triggered by easy access to weapons and the use of psychotropic drugs and alcohol [8]. Victims of physical violence may suffer serious injuries such as fractures of extremities [9], spinal cord and head injuries [10], which could affect their physical functioning and daily-life activities [11]. Although serious injuries predict poor HRQoL [9, 10], how their severity affects HRQoL remains unclear. An earlier cross-sectional study of severely injured trauma patients found that poor HRQoL was associated with psychosocial factors such as pre-injury co-morbidity, inability to return to work and living alone, but not with the severity of injury [12]. Similarly, a 5-year longitudinal study found that the severity of injuries did not determine the victims’ HRQoL [13]. However, a recent study claimed that poor HRQoL of trauma victims was primarily predicted by factors such as the severity of injury (having more than three days’ intensive care unit stay), type, and location of injury [11].
The available literature on the relationship between injuries and HRQoL has mainly focussed on accidental or unintentional causes such as work-related injuries [14], sports-related injuries [15], and road traffic accidents and falls [9]. Additionally, a few studies have investigated HRQoL among injured domestic violence victims or intimate partner violence [16]. There is limited research examining how serious injuries caused by interpersonal physical violence influence HRQoL. Thus, understanding the relationships between interpersonal physical violence-related serious injuries and HRQoL could help develop tailored interventions at the initial stages of treatment and prioritisation of resources for victims. To fill this gap in research evidence, the present study examined the relationships between physical violence and serious injury with HRQoL in the Australian adult population, using panel data from the Household, Income and Labour Dynamics in Australia (HILDA) Survey. Our results can generate novel and useful insights for policymakers to develop interventions that target the population at risk of physical violence, serious injuries, and poor HRQoL outcomes.
Methodology
Data source and sample selection
This study utilised de-identified person data of the Household, Income and Labour Dynamics in Australia (HILDA) Survey. HILDA is Australia’s biggest household-based longitudinal survey and one of the largest in the world [17]. The survey commenced in 2001 following the design of the German Socio-Economic Panel (SOEP), the British Household Panel Survey (BHPS), and the US Panel Study of Income Dynamics (PSID) to establish a nationally representative sample [18]. HILDA collects annual information on diverse domains from more than 13,000 individuals living in over 7,000 households in Australia. Data were collected from individuals aged 15 years or older in each household through personalised interviews (self-completion questionnaires and face-to-face interviews by trained interviewers). Details about the HILDA survey design and procedures have been published elsewhere [18].
This study utilised the last 19 waves (waves 2 through 20) of the HILDA Survey, spanning the period 2002 to 2020. The main reason for using these waves is that information on key variables of interest (physical violence, serious injury, and markers of HRQoL) was collected in these waves. Observations were excluded if there was missing data on the outcome variable (eight dimensions of the SF-36) and physical violence and serious injury. The final analytic sample consists of 245,070 person-year observations from 29,884 unique participants. Figure 1 shows the step-by-step selection of study participants.

Participants flow into the analytic sample, and missing data
Outcomes variables
The outcome variable, health-related quality of life (HRQoL), is operationalised through the 36-item Short-Form Health Survey (SF-36). The SF-36 is a broadly used generic, coherent, and easily accomplished questionnaire form to measure an individual’s physical and mental health status [19]. It measures eight health dimensions: physical functioning (PF), role physical (RP), role emotional (RE), social functioning (SF), mental health (MH), vitality (VT), bodily pain (BP), and general health (GH) through 36 questions. The score scale for each dimension of the SF-36 is transformed to a 0–100 range, where 0 indicates the worst health state and 100 indicates the best health state.
The eight dimensions of the SF-36 were further used to derive two distinct higher-ordered composite summary measures: the physical component summary (PCS) and mental component summary (MCS). The PCS is based on four subscales of the SF-36: PF, RP, BP, and GH. The MCS is based on the other four subscales: RE, SF, MH, and VT. Both the PCS and MCS scores were standardised to have a mean of 50 and a standard deviation of 10, respectively. The PCS scores ranged from 4.54 to 76.09 and the MCS scores from −1.21 to 76.19, with higher scores reflecting better quality of life.
The SF-6D is a global index derived from the SF-36 to capture respondents’ health state utility (Norman et al., 2014). This utility index is often used for economic evaluation (to estimate QALY and DALY). The SF-6D score is derived from responses from six dimensions of the SF-36, including PF, RP, RE, SF, VT, and BP. Each of the six dimensions has a level between 2 to 6 that can predict 18,000 health states [20]. The SF-6D score ranges from 0.29 (worst health) to 1 (full health state).
Exposure variables
Physical violence and serious injury are the primary variables of interest for the current study. Information on both variables was collected in every HILDA Survey wave, except for Wave 1. Data on physical violence were collected by asking respondents whether they had been a victim of physical violence in the past twelve months. Similarly, respondents were asked whether they had experienced any serious injury or illness to self in the previous twelve months. Responses to both questions were taken in binary form (0 = ‘no’; 1 = ‘yes’). The authors utilised these two variables to construct a new variable, ‘physical violence and serious injury’. The main exposure was categorised as ‘none’, ‘no violence, but injury’, ‘violence, but no injury’, and ‘both violence and injury’.
Control variables
A number of control variables were included in the statistical analyses to account for potential confounding. Following existing studies on HRQoL [19, 21, 22], this study included a compassing set of factors known to be correlated with HRQoL. These are age, gender, relationship status, highest education level completed, household annual disposable income, labour force status, Indigenous status, region of residence, smoking status, alcohol consumption, and physical activity. Descriptions of all covariates used in the analysis are provided in Table 1.
Estimation strategy
An unbalanced longitudinal dataset consisting of 245,070 person-year observations was constructed by linking 29,884 de-identified records from individuals who participated in at least one survey wave (from waves 2 through 20). To summarise the characteristics of the study participants, descriptive statistics in the form of frequency (n) and percentage (%) were reported for categorical variables. The mean along with the standard deviation (SD) was reported for continuous variables.
Our main analyses involve multivariate regression models estimating the relationships between physical violence and injury and HRQoL. We fitted three different models for continuous dependent variables: PCS, MCS, and SF-6D. This study utilised fixed-effects longitudinal regression model to estimate the effect of physical violence and serious injury on HRQoL. The model estimates how switches from individuals’ exposure to physical violence and serious injury are associated with deviations from their usual outcomes (captured by the individual mean scores in HRQoL over time). It takes the following form:
In Eq. 1, \({HRQoL}_{it}\) refers to the summary measures (PCS and MCS), and the health utility index (SF-6D). PVSA is the main variable of interest that captures physical violence and serious injury experienced by the respondents. X is a vector of control variables, \({\varepsilon }_{it}\) is the error term, subscripts i refer to individual and t indicates time.
Fixed-effects model captures the underlying reasons for variations in outcomes within a person across different periods. In the current study, the fixed-effects models estimate how within-person variations in a person’s HRQoL differ in those observation periods in which they were exposed to physical violence and injury compared to those in which they were not exposed to physical violence and serious injury. All models were adjusted for the socio-demographic and lifestyle characteristics described before. This study considers statistical significance for the exposure variables at p < 0.05. All analyses were conducted using Stata version 16.0 (Stata SE 16, Stata Corp, College Station, TX, USA).
Results
Descriptive statistics
A summary of socio-economic and health-related characteristics of the study sample at baseline, final, and all waves pooled is presented in Table 2. Among the study participants, over one-third (41%) were aged 46–64 years, more than half (53%) were female, and approximately 60% were coupled, one-fourth (25%) have university degrees, two-thirds (65%) are employed, are non-Indigenous (97%), and nearly two-third (65.73%) lives in major cities. Variations also existed concerning the study participants’ health-related characteristics. More than half (54%) of the study participants never smoked, a vast proportion (82%) consumed alcohol, and two-thirds (66%) did not engage in the recommended level of physical activity (pooled sample).
Summary statistics of the subjective health scores of the analytic sample as well as the status of physical violence and serious injury are shown in Table 3. Mean scores on each of the eight SF-36 domains are PF (83.84 ± 23.00), RP (79.00 ± 36.02), RE (82.44 ± 33.37), SF (82.30 ± 23.50), MH (73.78 ± 17.38), VT (59.45 ± 19.96), BP (73.01 ± 23.92), and GH (68.04 ± 20.91). The mean SF-36 component summary measures (PCS and MCS) and health utility index (SF-6D) are 49.45 ± 10.38, 48.38 ± 10.64, 0.76 ± 0.12, respectively (pooled in all waves). Table 3 also shows that 90% of the sample did not experience physical violence or serious injury. Concerning the key exposure variable, 8.4% of adults had no injury but serious illness, 1.15% had experienced violence but no injury, and 0.34% had experienced both (pooled sample).
The distribution of the outcome variables (PCS, MCS and SF-6D utility score) is shown in Fig. 2. The figure reveals that most respondents had PCS and MCS scores between 50 and 60. The SF-6D score is skewed to the right, with a lot of observations having a score greater than 0.7. There are a relatively small number of observations with a score of 0.4 to 0.6.

Distribution of PCS and MCS scores and SF-6D utility values
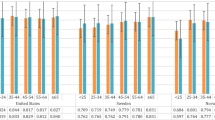
Figure 3 displays the mean PCS, MCS, and SF-6D scores by physical violence and serious injury. The figure demonstrates that mean PCS, MCS, and SF-6D scores decline for participants exposed to either physical violence, serious injury, or both. Participants who had been exposed to both physical violence and serious injury had lower mean PCS, MCS, and SF-6D scores. For example, mean PCS, MCS, and SF-6D scores in Wave 20 were much lower among the respondents exposed to both physical violence and serious injury (41.24, 39.95, and 0.58, respectively) compared to participants exposed to none (50.86, 46.65, and 0.76, respectively).

Mean SF-36 component summary scores and SF-6D utility score by physical violence and serious injury, waves 2–20
Regression modelling
Table 4 presents the result from the fixed-effects regression models examining the combined effects of physical violence and serious injury on HRQoL measured through PCS, MCS, and SF-6D. Model 1 indicates that participants reported lower PCS scores in those observations in which they had been exposed to serious injury (β = −5.103) or both physical violence and injury (β = −3.60) than in those observations in which they had been exposed to neither of these stressors. However, a statistically positive significant difference in PCS score has been found in terms of experiencing physical violence (0.376). Model 2 also shows that adults exposed to only injury (−2.363), only physical violence (−2.786) and both (−6.027) had lower MCS scores if switched from not experiencing physical violence and serious injury.
Statistically significant lower scores in SF-6D score are also observed among adults exposed to physical violence and serious injury compared with those exposed to none. Adults exposed to physical violence (−0.0585), serious injury (−0.0214), and both (−0.0716) had lower SF-6D scores if the adults were exposed to none (Model 3).
Discussion
This study aimed to examine the association between physical violence, serious injuries, and HRQoL in the Australian adult population. The analysis was based on 19 consecutive waves of longitudinal data from the HILDA Survey spanning the 2002 to 2020 period. The results showed that 1.15% and 8.44% of the respondents had experienced physical violence and serious injury, respectively. The main findings suggest that exposure to physical violence and serious injury were associated with a reduction in HRQoL as measured by the SF-36. Specifically, of the summary measures and health utility index of SF-36 (PCS, MCS and SF-6D), victims of only physical violence have reduced MCS and SF-6D utility scores. Similarly, individuals exposed to only serious injuries and both physical violence and serious injuries scored substantially lower for PCS, MCS, and SF-6D. These associations were statistically significant even after controlling for age, gender, relationship status, highest education level completed, household annual disposable, labour force status, Indigenous status, region of residence, smoking status, alcohol consumption, and physical activity.
The negative associations between MCS and SF-6D with physical violence found in the present study were consistent with those reported in the previous literature [23, 24]. The emotional problems associated with experiencing physical violence could plausibly account for the poor mental health outcomes (low MCS scores) among the victims compared to other adults. For instance, an earlier study reported that victims of physical violence experience long-term adverse mental health consequences that negatively impact their quality of life [25]. This might have probably also contributed to the worst possible health state (low SF-6D) recorded among victims of physical violence compared to non-victims.
We found a positive association between physical violence and PCS, which contradicts previous studies [23, 24, 26]. Arguably, victims of physical violence may recover from any related physical health consequences within a relatively shorter duration than the emotional health consequences. However, they may still suffer emotionally, which could negatively affect their mental health, as manifested in the low MCS scores recorded among the victims. This calls for increased psychosocial interventions such as social support for victims of physical violence [27], given that social support improves mental health outcomes among victims of physical violence [25].
The findings from this study also suggest that victims of serious injuries have lower scores for PCS, MCS and SF-6D compared to their peers without serious injuries. Similarly, previous studies had reported a negative association between serious injuries and the PCS [28] and MCS [29]. To the best of our knowledge, the present study is the first that reports an association between serious injury and the SF-6D utility score. Thus, the present study finding is important because it could serve as a reference for future studies on the association between serious injuries and HRQoL as measured by the SF-6D utility score.
The significant negative association between serious injuries and lower PCS and MCS scores, as found in this study, suggests that injured victims may have a worse physical and mental health-related quality of life than those without injuries. Contrary to the findings from the present study, a recent study reported no association between serious injuries and PCS scores, even though the researchers found a significant negative association between serious injuries and MCS scores [29]. Perhaps, the duration of their study (data were collected from road traffic accident victims at 6, 12, and 24 months) might not have been long enough to elicit a significant perception of a decrease in quality of life [29]. Besides, the method, focal population, and type of likely injury (traffic-related) are plausible reasons. Relatedly, another study reported that injury severity was not significantly associated with both PCS and MCS scores [30]. However, the researchers noted that persons with traumatic injuries generally had low PCS and MCS scores. In their prospective study, data were collected at one month and six months post injury, a duration that might be too short to produce any significant association between injury and HRQoL. However, corroborating the findings from the current study, a recent study found a significant association between serious injuries and low PCS among victims of the 9/11 World Trade Center attack in the US, fifteen years after the incident [27].
This study’s findings add to increasing evidence indicating that physical violence and serious injuries are associated with reduced HRQoL. Given that most previous studies used the SF-36 (a general measure of HRQoL) in examining the relationship between HRQoL and physical violence [31, 32] or serious injuries [10, 33], the current study innovates with respect to the existing literature by using the SF-6D utility score, a generic preference-based measure of HRQoL, which is highly generalisable and can be used to estimate quality-adjusted life years [QALYs] [34, 35]. Additionally, the utilisation of a large sample size helps to get more precise estimates when investigating the relationships between HRQoL and physical violence and serious injuries in the Australian population. Further, to minimise the risk of omitted variable bias, this study employed fixed-effects analytical approach. For example, it is possible that individuals who have certain unobserved characteristics (e.g. housing instability, certain personality types, etc.) tend to attract both violence and poor HRQoL. Fixed-effect models would minimise the possibility of this type of omitted variable bias that affects results.
The present study findings highlight a significant impact of physical violence and serious injuries on HRQoL, especially concerning the mental health states of victims, even in the absence of any form of physical health issues. Thus, there is a possibility of unmet mental health needs for victims of physical violence and serious injuries, which calls for proactive policy interventions that provide psychological and emotional therapy for victims. Therefore, this study recommends that victims of physical violence and serious injuries be screened for mental health problems by healthcare professionals during their first hospital visits with follow-up mental health assessments. Hence, all healthcare professionals in acute care settings should be given regular training on primary mental health screening or assessment skills. All screened patients should be referred to a clinical psychologist for follow-up assessments and management when appropriate. This approach could minimise the long-term mental health impact of physical violence and serious injuries on the Australian population.
This study’s major strength is using a large and nationally representative longitudinal dataset with numerous observations over prolonged periods (19 waves spanning from 2002–2020). Thus, the study findings could be generalisable to victims of physical violence and serious injuries in Australia.
Despite the importance of our findings, it is worthy to note some of the limitations of this study. First, even though the study used longitudinal data, we cannot make causal inferences due to the study’s observational nature. A second limitation of this study is that the sources and type of injuries were not identified in the data. Different sources and types of injuries may impact victims’ quality of life differently, pointing to the need to replicate our analyses using data containing more granular information [9]. Finally, this study—as well as earlier studies—has not considered the longitudinal persistence of the negative impacts of physical violence and serious injuries on HRQoL. Understanding the duration of these negative effects would be helpful in designing remedial interventions, and may also contribute to reconciling the mixed findings from earlier studies described before. Therefore, future research adopting a life-course approach to examine the duration of the negative effects of physical violence and serious injuries on HRQoL is warranted.
Conclusion
This study has provided novel empirical evidence on the associations between physical violence and serious injuries on HRQoL among adults in Australia. Physical violence and serious injuries were associated with decreased mental health (MCS) and worse health states (SF-6D), while serious injuries were related to decreased physical health (PCS). Thus, there is a possibility of unmet mental health needs for victims of physical violence and serious injuries. This calls for proactive policy interventions that provide psychological and emotional therapy.
Data availability
The data used for the study were collected from the Melbourne Institute of Applied Economic and Social Research. There are some restrictions on these data and are not available to the public. Those interested in accessing these data should contact the Melbourne Institute of Applied Economic and Social Research, The University of Melbourne, VIC 3010, Australia.
Abbreviations
- BMI:
-
Body Mass Index
- HILDA:
-
Household, Income and Labour Dynamics in Australia Survey
- HRQoL:
-
Health-related Quality of Life
- PCS:
-
Physical Component Summary
- MCS:
-
Mental Component Summary
- SF-6D:
-
Short-Form Six-Dimension
- SF-36:
-
36-Item Short-Form Health Survey
References
Naghavi, M., Abajobir, A. A., Abbafati, C., Abbas, K. M., Abd-Allah, F., Abera, S. F., & Murray, C. J. L. (2017). Global, regional, and national age-sex specific mortality for 264 causes of death, 1980–2016: A systematic analysis for the global burden of disease study 2016. The Lancet, 390(10100), 1151–1210. https://doi.org/10.1016/S0140-6736(17)32152-9
Vos, T., Lim, S. S., Abbafati, C., Abbas, K. M., Abbasi, M., Abbasifard, M., & Murray, C. J. L. (2020). Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the global burden of disease study 2019. The Lancet, 396(10258), 1204–1222. https://doi.org/10.1016/S0140-6736(20)30925-9
Dahlberg, L. L., & Krug, E. G. (2006). Violence a global public health problem. Ciência & Saúde Coletiva, 11(2), 277–292. https://doi.org/10.1590/S1413-81232006000200007
Zwi, A. B., Krug, E. G., Mercy, J. A., & Dahlberg, L. L. (2002). World report on violence and health—exploring Australian responses. Australian and New Zealand Journal of Public Health, 26(5), 405–408. https://doi.org/10.1111/j.1467-842X.2002.tb00334.x
Australian Bureau of Statistics. (2017). Personal Safety, Australia: Statistics for family, domestic, sexual violence, physical assault, partner emotional abuse, child abuse, sexual harassment, stalking and safety. Retrieved January 31, 2021, from https://www.abs.gov.au/statistics/people/crime-and-justice/personal-safety-australia/latest-release
Australian Institute of Health and Welfare. (2020). Australia’s health snapshots 2020. Canberra: AIHW.
Gunilla Krantz; Claudia Garcia-Moreno. (2005). Violence against women. Journal of Epidemiology & Community Health, 59(10), 818–821. https://doi.org/10.1136/jech.2004.022756
Wang, H., Naghavi, M., Allen, C., Barber, R. M., Bhutta, Z. A., Carter, A., & Murray, C. J. L. (2016). Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: A systematic analysis for the global burden of disease study 2015. The Lancet, 388(10053), 1459–1544. https://doi.org/10.1016/S0140-6736(16)31012-1
Borg, T., Berg, P., Fugl-Meyer, K., & Larsson, S. (2010). Health-related quality of life and life satisfaction in patients following surgically treated pelvic ring fractures. A prospective observational study with two years follow-up. Injury, 41(4), 400–404. https://doi.org/10.1016/j.injury.2009.11.006
Tøien, K., Bredal, I. S., Skogstad, L., Myhren, H., & Ekeberg, Ø. (2011). Health related quality of life in trauma patients data from a one-year follow up study compared with the general population. Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine. https://doi.org/10.1186/1757-7241-19-22
Christensen, M. C., Banner, C., Lefering, R., Vallejo-Torres, L., & Morris, S. (2011). Quality of life after severe trauma: Results from the global trauma trial with recombinant factor VII. The Journal of Trauma: Injury, Infection, and Critical Care, 70(6), 1524–1531. https://doi.org/10.1097/TA.0b013e3181f053c2
van Delft-Schreurs, C. C. H. M., van Bergen, J. J. M., de Jongh, M. A. C., van de Sande, P., Verhofstad, M. H. J., & de Vries, J. (2014). Quality of life in severely injured patients depends on psychosocial factors rather than on severity or type of injury. Injury, 45(1), 320–326. https://doi.org/10.1016/j.injury.2013.02.025
Sluys, K., Hggmark, T., & Iselius, L. (2005). Outcome and quality of life 5 years after major Trauma. The Journal of Trauma: Injury, Infection, and Critical Care, 59(1), 223–232. https://doi.org/10.1097/01.TA.0000173832.01547.CB
Salah Eldin, W., Hirshon, J. M., Smith, G. S., Kamal, A.-A.M., Abou-El-Fetouh, A., & El-Setouhy, M. (2012). Health-related quality of life after serious occupational injury in Egyptian workers: A cross-sectional study. British Medical Journal Open, 2(6), e000413. https://doi.org/10.1136/bmjopen-2011-000413
Simon, J. E., & Docherty, C. L. (2016). Current health-related quality of life in former national collegiate athletic association division i collision athletes compared with contact and limited-contact athletes. Journal of Athletic Training, 51(3), 205–212. https://doi.org/10.4085/1062-6050-51.4.05
Wittenberg, E., Joshi, M., Thomas, K. A., & McCloskey, L. A. (2007). Measuring the effect of intimate partner violence on health-related quality of life: A qualitative focus group study. Health and Quality of Life Outcomes, 5(1), 67. https://doi.org/10.1186/1477-7525-5-67
Department of Social Services. (2016). Review of Australia’s Longitudinal Data System. Canberra: DSS.
Watson, N. (2021). Finding your way around the HILDA survey data. Australian Economic Review, 54(4), 554–564. https://doi.org/10.1111/1467-8462.12437
Perales, F., del Pozo-Cruz, J., del Pozo-Cruz, J., & del Pozo-Cruz, B. (2014). On the associations between physical activity and quality of life: Findings from an Australian nationally representative panel survey. Quality of Life Research, 23(7), 1921–1933. https://doi.org/10.1007/s11136-014-0645-4
Kortt, M. A., & Dollery, B. (2011). Association between body mass index and health-related quality of life among an Australian sample. Clinical Therapeutics, 33(10), 1466–1474. https://doi.org/10.1016/j.clinthera.2011.08.009
Sahle, B. W., Slewa-Younan, S., Melaku, Y. A., Ling, L., & Renzaho, A. M. N. (2020). A bi-directional association between weight change and health-related quality of life: Evidence from the 11-year follow-up of 9916 community-dwelling adults. Quality of Life Research, 29(6), 1697–1706. https://doi.org/10.1007/s11136-020-02423-7
Renzaho, A., Wooden, M., & Houng, B. (2010). Associations between body mass index and health-related quality of life among Australian adults. Quality of Life Research, 19(4), 515–520. https://doi.org/10.1007/s11136-010-9610-z
Costa, D., Hatzidimitriadou, E., Ioannidi-Kapolou, E., Lindert, J., Soares, J., Sundin, Ö., & Barros, H. (2015). Intimate partner violence and health-related quality of life in European men and women: Findings from the DOVE study. Quality of Life Research, 24(2), 463–471. https://doi.org/10.1007/s11136-014-0766-9
Sørensen, J., Kruse, M., Gudex, C., Helweg-Larsen, K., & Brønnum-Hansen, H. (2012). Physical violence and health-related quality of life: Danish cross-sectional analyses. Health and Quality of Life Outcomes, 10(1), 113. https://doi.org/10.1186/1477-7525-10-113
Coker, A. L., Smith, P. H., Thompson, M. P., McKeown, R. E., Bethea, L., & Davis, K. E. (2002). Social support protects against the negative effects of partner violence on mental health. Journal of Women’s Health & Gender-Based Medicine, 11(5), 465–476. https://doi.org/10.1089/15246090260137644
Straus, H., Cerulli, C., McNutt, L. A., Rhodes, K. V., Conner, K. R., Kemball, R. S., & Houry, D. (2009). Intimate partner violence and functional health status: associations with severity, danger, and self-advocacy behaviors. Journal of Women’s Health, 18(5), 625–631. https://doi.org/10.1089/jwh.2007.0521
Brackbill, R., Alper, H., Frazier, P., Gargano, L., Jacobson, M., & Solomon, A. (2019). An assessment of long-term physical and emotional quality of life of persons injured on 9/11/2001. International Journal of Environmental Research and Public Health, 16(6), 1054. https://doi.org/10.3390/ijerph16061054
Rivers, C. S., Fallah, N., Noonan, V. K., Whitehurst, D. G., Schwartz, C. E., Finkelstein, J. A., & Noreau, L. (2018). Health conditions: Effect on function, health-related quality of life, and life satisfaction after Traumatic spinal cord injury a prospective observational registry cohort study. Archives of Physical Medicine and Rehabilitation. https://doi.org/10.1016/j.apmr.2017.06.012
Kenardy, J., Heron-Delaney, M., Warren, J., & Brown, E. (2015). The effect of mental health on long-term health-related quality of life following a road traffic crash: Results from the UQ SuPPORT study. Injury, 46(5), 883–890. https://doi.org/10.1016/j.injury.2014.11.006
Kiely, J. M., Brasel, K. J., Weidner, K. L., Guse, C. E., & Weigelt, J. A. (2006). Predicting quality of life six months after Traumatic injury. The Journal of Trauma: Injury, Infection, and Critical Care, 61(4), 791–798. https://doi.org/10.1097/01.ta.0000239360.29852.1d
Bonomi, A. E., Anderson, M. L., Rivara, F. P., & Thompson, R. S. (2007). Health outcomes in women with physical and sexual intimate partner violence exposure. Journal of Women’s Health, 16(7), 987–997. https://doi.org/10.1089/jwh.2006.0239
Tavoli, Z., Tavoli, A., Amirpour, R., Hosseini, R., & Montazeri, A. (2016). Quality of life in women who were exposed to domestic violence during pregnancy. BMC Pregnancy and Childbirth, 16(1), 19. https://doi.org/10.1186/s12884-016-0810-6
Jacobsson, L. J., Westerberg, M., & Lexell, J. (2010). Health-related quality-of-life and life satisfaction 6–15 years after traumatic brain injuries in northern Sweden. Brain Injury, 24(9), 1075–1086. https://doi.org/10.3109/02699052.2010.494590
Dritsaki, M., Petrou, S., Williams, M., & Lamb, S. E. (2017). An empirical evaluation of the SF-12, SF-6D, EQ-5D and michigan hand outcome questionnaire in patients with rheumatoid arthritis of the hand. Health and Quality of Life Outcomes, 15(1), 20. https://doi.org/10.1186/s12955-016-0584-6
Fu, S., Dao, M.-C., Wong, C.K.-H., & Yu, W. (2019). SF-6D utility scores of smokers and ex-smokers with or without respiratory symptoms attending primary care clinics. Health and Quality of Life Outcomes, 17(1), 48. https://doi.org/10.1186/s12955-019-1115-z
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions. This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
SAK initiated the study, conducted the data analysis. SAK, AS, AM, and BOA drafted the manuscript. FP, KN, and TC offered advice, critical comments, and edited the draft manuscript. All the authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflicts of interest.
Ethics approval
This paper uses unit record data from Household, Income and Labour Dynamics in Australia Survey (HILDA) conducted by the Australian Government Department of Social Services (DSS). However, the findings and views reported in this paper are those of the authors and should not be attributed to the Australian Government, DSS, or any of DSS contractors or partners. https://doi.org/10.26193/OFRKRH, ADA Dataverse, V2”.
This study did not require ethical approval as the analysis used only de-identified existing unit record data from the HILDA Survey. However, the authors completed and signed the Confidentiality Deed Poll and sent it to NCLD (ncldresearch@dss.gov.au) and ADA (ada@anu.edu.au) before the data applications’ approval. Therefore, the datasets analysed and/or generated during the current study are subject to the signed confidentiality deed.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Keramat, S.A., Nguyen, KH., Perales, F. et al. Estimating the effects of physical violence and serious injury on health-related quality of life: Evidence from 19 waves of the Household, Income and Labour Dynamics in Australia Survey. Qual Life Res 31, 3153–3164 (2022). https://doi.org/10.1007/s11136-022-03190-3
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11136-022-03190-3