
Abstract
This paper investigates the impact of socioeconomic (SES) disparities on anthropometrics, receptive vocabulary skills, and socio-emotional skills in Chilean children 31–83 months old (n = 7744). Longitudinal data allow for the estimation of dynamic models of child growth and skill formation while adjusting for mother's schooling and cognitive ability. The results show small length differences at birth with the better-off being shorter, but these differences are reversed during the first 10 months of life, at which age SES disparities in height-for-age z scores (HAZ) favored the better-off. Disparities in receptive vocabulary skills found at 30 months continue until the child is at least 6 years old. For socio-emotional skills, we found SES disparities before 72 months, but not after. Our results indicate that—even after controlling for factors that are not usually considered in the literature, such as mother's cognitive ability and lagged skills—SES remains significantly associated with child development outcomes within a dynamic context.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
The importance of early human capital in economic and social well-being over the life cycle has received substantial and increasing attention in the literature including studies on in-utero conditions (Almond, 2006; Barker, 1990; Majid, 2015) to early childhood (Behrman et al., 2009; Gertler et al., 2014; Hoddinott et al., 2008, 2013a, 2013b; Maluccio et al., 2009; Martorell et al., 2010) and into adolescence (Black et al., 2021; Heckman et al., 2006; Schott et al., 2017; Stein et al., 2016). There is a general consensus that birth outcomes, especially birth weight, can impact schooling achievement, employment, and earnings (Behrman & Rosenzweig, 2004; Conley & Bennett, 2000; Currie & Almond, 2011; Torche & Echevarría, 2011). There is also agreement that early life nutrition and cognitive and socio-emotional stimulation can have multiple impacts over the life cycle and across generations (Black et al., 2017; Crookston et al., 2013; Stein et al., 2010, 2013; Victora et al., 2008; Walker et al., 2011a, 2011b). Additionally, there is a growing literature relating early cognitive and socio-emotional skills to adulthood outcomes (Cunha & Heckman, 2008), finding that both types of skills have long-term effects.
In this context, it is relevant to study how early human capital varies by household SES. We examine SES disparities in anthropometric and skill outcomes using longitudinal data within a dynamic framework for both preschool and early elementary school students in Chile, a country that exhibits high-income inequality but generally very good average-health outcomes. Chile has one of the most unequal income distributions in the Latin American and the Caribbean (LAC) region, which in turn has the greatest inequality among the world’s major regions. According to the World Bank, in 2016, Chilean inequality was only surpassed in the LAC region by Honduras, Colombia, Brazil, Guatemala, and Panama. In addition, Chile is the most unequal economy of OECD countries with a Gini index of 0.465, followed by Mexico and the United States with 0.459 and 0.394, respectively (OECD, 2016). Perhaps paradoxically, Chile however has relatively good and egalitarian health indicators in early years; the mortality rate for children under 5 years of age in 2015 was 8.1 per 1000 live births, which is much lower than the LAC average of 17.9, and only slightly higher than the OECD average of 6.9. Furthermore, health outcomes are similar across socioeconomic (SES) status; according to Contreras and Puentes (2017), there are no differences across the SES distribution in either weight or length at birth. The high inequality along with the relatively good and equally distributed health outcomes raise the question of what happens in Chile between birth and adulthood that transforms relatively similar newborns in terms of human capital into adults with extremely different opportunities.
We make several contributions to the literature. First, we use longitudinal data, which represent an advantage over the cross-sectional data previously used in this literature (Bando et al., 2016; Fernald et al., 2011, 2012; Paxson & Schady, 2007). While other papers have used longitudinal data, particularly from the Young Lives project [see for example Lopez Boo (2016) and Aurino et al., (2019)], we are one of the few papers that uses longitudinal data to test the cumulative impact of SES on skills when controlling for lagged skill levels. Galasso et al. (2019) is an example of this approach which allows us to study the cumulative and current impact of SES on children’s outcomes. Second, we use a nationally representative survey where most of the existing literature focuses on sub-populations (Fernald et al., 2011; Galasso et al., 2019; Schady, 2011). Third, we make a comprehensive assessment of child development by analyzing physical, cognitive, and socio-emotional development instead of focusing on just one of these areas (like Lopez Boo (2016) and Schady (2011)). Fourth, it is regularly acknowledged in the literature that mother’s cognitive ability is one factor that is often missing in the analysis, but the richness of our data allows us to include it. The paper by Schady (2011) controls for mother´s ability, which allows for better identification of the extent of the persistence of SES disparities. Fifth, we provide a correction for multiple testing, which is important since we are analyzing several outcomes for different age groups.
Our results indicate there are no statistically significant differences in weight at birth across SES quintiles. There are differences in height at birth, with newborns in the top SES quintile unexpectedly tending to be shorter. However, these gaps are soon reversed and disparities favoring the better-off in height (length)-for-age z scores (HAZ) and in cognitive and socio-emotional skills emerge early in the postnatal period and become prominent by 30 months old. Since we use a dynamic approach controlling for lagged outcomes, SES status has a baseline and a dynamic association through the lagged outcome. Before preschool there are already SES differences in HAZ, and socio-emotional and receptive vocabulary skills even after adjusting for lagged measures of these outcomes and for mother’s cognitive skills. While socioeconomic disparities have important predictive power on receptive vocabulary scores until children are 83 months old, SES differences for socio-emotional skills and anthropometrics gaps are not statistically significant for children over the age of 72 months. All the results hold when we correct for multiple testing.
In summary, our study sheds new light on the relationship between SES and children’s outcomes by controlling for several variables that are often not used in previous studies. Our findings show that lagged outcomes and mother’s cognitive ability are important factors that mediate SES disparities in children’s outcomes. However, even after accounting for these variables, we still find disparities by SES in several outcomes. Interestingly, the magnitude of these disparities is lower than what is typically reported in the literature (Galasso et al., 2019), which could suggest that some public policies implemented in Chile may have had some success in mitigating SES disparities. Nevertheless, further research is needed to fully understand the impact of these policies. Our results also highlight the important role that schools can play in narrowing SES gaps, particularly in the areas of socio-emotional skills and anthropometrics, where we found no disparities by SES after the age of 72 months.
The remaining sections in the paper describe the relevant literature, context, and methods; present the results; and conclude with a discussion.
Literature Review
The study of household socioeconomic status is relevant for policy because prenatal and early life disadvantages may prevent children from achieving their developmental potential (Black et al., 2017; Grantham-McGregor et al., 2007; Walker et al., 2011a, 2011b) with long-term consequences. Conditions as early as in-utero matter, since disadvantaged prenatal conditions are associated with reduced schooling attainment, increased rates of physical disability and poor health, lower income, and lower socioeconomic status (Almond, 2006; Almond & Currie, 2011; Almond et al., 2018). Furthermore, low SES is related to poor nutritional status and low levels of cognitive development and vocabulary in early childhood in both high-income (Aughinbaugh & Gittleman, 2003; Currie, 2009) and low- and middle-income countries (Behrman et al., 2009; Gertler et al., 2014; Hoddinott et al., 2008; Maluccio et al., 2009; Martorell et al., 2010).
Poor nutritional status and low levels of cognitive development and vocabulary in early childhood are in turn associated with negative outcomes later in life: worse birth outcomes, especially low birth weight, can impact schooling achievement, employment, and earnings, with profound adverse consequences over the life cycle on human, social, and economic capital (Behrman & Rosenzweig, 2004; Conley & Bennett, 2000; Currie & Almond, 2011; Hoddinott et al., 2008; Schott et al., 2017; Stein et al., 2016; Torche & Echevarría, 2011). Similarly, worse cognitive outcomes early in life are associated with lower schooling attainment (Currie, 2009; Walker et al., 2011a, 2011b), worse adult health (Campbell et al., 2014), lower probability of employment, lower future earnings (Gertler et al., 2014; Heckman et al., 2006), and higher probabilities of participating in criminal activity (Heckman et al., 2010). Additionally, worse socio-emotional skills early in life are linked to worse adulthood outcomes (Cunha & Heckman, 2008), influencing schooling decisions and through them potentially affecting wages (Heckman et al., 2006). All of this evidence points to the fact that early life nutrition and cognitive and socio-emotional stimulation can have multiple impacts over the life cycle and even across generations (Crookston et al., 2013; Stein et al., 2010, 2013; Victora et al., 2008; Walker et al., 2011a, 2011b).
Focusing on SES is relevant for policy not only on the individual level, as disadvantages found at an early age may result in the intergenerational transmission of poverty and income inequalities if they are not addressed by policymakers before children reach primary school age (Lopez Boo, 2016). Several papers—Bando et al. (2016), Fernald et al., (2011, 2012), Lopez Boo (2016), Paxson and Schady (2007), Reynolds et al. (2017), and Schady et al. (2014)—among others have studied how early human capital varies by household SES. They have consistently found strong associations between indicators of SES and child development.
The existing literature has proposed a variety of potential mechanisms linking SES and children’s abilities. The parental investment perspective (Becker & Tomes, 1979; Behrman et al., 1982) suggests that income allows families to invest in their children, providing better food, education, books, and toys among other inputs in the skill formation process. Another relevant mechanism is that children from poorer households less frequently attend preschool or school, usually because they are contributing to household work. Meanwhile, bullying also has a negative relationship with SES (Laith & Vaillancourt, 2022). Other mechanisms could be that high-income households face lower stress, which could benefit children’s development or emotional state (Blair & Raver, 2016). Finally, mothers with lower SES could have lower-quality interactions with their children, leading to lower skill accumulation (Lugo-Gil & Tamis-LeMonda, 2008).
Chilean Context
This section briefly describes the characteristics of Chilean early childhood policies to provide context and thus allow for a clearer interpretation of the results.
Both health and education provision are organized through a combination of public and private sector initiatives. The public sector is responsible for providing universal access to healthcare through a network of primary-care centers, specialized-care centers, and hospitals along with a public health insurance system. The private sector also plays a significant role in healthcare delivery, with some families opting to purchase private insurance or pay out-of-pocket for additional services. In education, the public sector is responsible for providing free, universal preschool education for children between the ages of 3 and 5 through a program that aims to provide children with a foundation in language, literacy, mathematics, and social skills, which is based on a play-based approach to learning. Private sector preschool is also available and may offer a range of additional services and resources such as extended hours, specialized curricula, and extracurricular activities.
Chile has recently significantly increased the access to early childhood education, with the enrollment rate in early childhood education (for children aged 3–5) increasing from 44% in 2005 to 79% in 2017 (OECD, 2019). However, there are still significant disparities in access to quality early childhood education for children from disadvantaged backgrounds, with children from lower-income households being more likely to attend lower-quality schools and having less access to resources such as trained teachers and educational materials (Bainbridge et al., 2005; Magnuson & Waldfogel, 2016; Meyers et al., 2004; UNICEF, 2015).
The Chilean health system is characterized by a high level of coverage and access to care (Missoni & Solimano, 2010), which has caused significant improvements in the overall health of its population. For example, the infant mortality rate in Chile has decreased significantly in recent decades, from 16.1 deaths per 1000 live births in 1990 to 6.1 deaths per 1000 live births in 2019Footnote 1. However, there are still significant disparities in health outcomes for children from different socioeconomic backgrounds. For example, children from lower-income households are more likely to experience malnutrition and other health problems and may have less access to preventive and curative health services (UNICEF, 2019).
One of the key Chilean policies aimed at addressing these remaining inequalities is Chile Crece Contigo. This policy is managed by the Ministry of Social Development but includes participation from the Ministry of Education and the Ministry of Health. The program was fully implemented in 2009. Initially the policy aimed to address children from conception to age 4, but currently it includes older children. The policy combines universal and targeted benefits, and includes educational programs, special access to social protection programs such as access to free childcare, and health check-ups for all children enrolled in the public health sector. Evaluations of the different aspects of this policy have shown positive effects on social development, and high satisfaction ratings (Torres et al., 2018).
Materials and Methods
This study uses data from the first (2010) and second (2012) rounds of the Early Childhood Longitudinal Survey (Encuesta Longitudinal de la Primera Infancia, ELPI for its Spanish acronym). The survey was commissioned by the Chilean Ministries of Labor and Education to inform the design of and assess public-policy programs and is representative of the sex, ethnic, and SES breakdowns of the Chilean population under 5 years old in 2010.
The information was gathered through two visits: in the first one, a socio-demographic household survey was conducted. In the second visit, the child’s physical, cognitive, and socio-emotional characteristics were measured. The survey was administered by psychologists with experience in infant evaluations and/or psychological tests who were selected after written and practical examinations and were trained specifically for the administration of these tests. The final decision regarding the topics covered in the questionnaire, as well as the choice of the instruments was made jointly between researchers from Northwestern University: the University of Pennsylvania; the University of California, Berkeley; and the Centre for Microdata at the University of Chile.
Child Development Assessments
For a comprehensive assessment of children’s development, we assessed their anthropometric, cognitive, and socio-emotional development using height-for-age z scores (HAZ), Peabody Picture Vocabulary Test (PPVT), and Child Behavior Checklist (CBCL), respectively. In what follows, we briefly describe each of these measures and how they were collected by the ELPI. Detailed descriptions of each test can be found in Online Appendix 1.
Anthropometric Development Measures
In 2010 and 2012, all children’s current height was measured on site using certified measurement tools and following age-specific procedures for children under and over 2 years old. We used World Health Organization standards to transform heights into HAZ to measure anthropometric development (Onis et al., 2007; World Health Organization, 2006). HAZ has been widely used in the literature as an indicator of long-term nutritional status (Arimond & Ruel, 2004; Black et al., 2017; Foster et al., 2005; Hoddinott et al., 2013a, 2013b; Hoddinott et al., 2013a, 2013b).
Receptive Vocabulary Measures
Receptive vocabulary was measured using an adaptation of the PPVT designed for Spanish-speaking children (Dunn et al., 1986). PPVT is an internally valid and consistent measure of auditory vocabulary extensively used both in Latin America and worldwide (Coddington et al., 2014; Contreras & González, 2015; Crookston et al., 2013; Lopez Boo, 2016; Schady et al., 2014), and has been validated with Mexican and Puerto Rican populations (Reynolds et al., 2017). Higher PPVT scores indicate higher receptive vocabulary skills.
In ELPI, PPVT was administered to children between 30 and 60 months old in 2010 and to children between 30 and 83 months old in 2012. Following Galasso et al. (2019), Schady et al. (2014), and many others, the PPVT was internally normalized using means and standard deviations from children of the same age.
Socio-emotional Development Measures
To assess socio-emotional development, we use the Spanish version of the CBCL. The CBCL measures children’s behavioral and socio-emotional abilities and helps identify problems such as anxiety, autism, violent behaviors, and attention deficit disorder (Achenbach & Edelbrock, 1991). It has been validated in Argentina and Uruguay (Samaniego, 2008; Viola et al., 2011) and has been used in several international studies (Anselmi et al., 2008; Weisz et al., 1993) as well as studies in Chile (Reynolds et al., 2017). Note that higher CBCL scores indicate lower socio-emotional skills.
The CBCL was administered to children between 18 and 60 months old in 2010 and between 18 and 83 months old in 2012. During that round, a slightly different version was administered to children between 72 and 83 months old. That version included many of the questions given to younger children, while adding some items covering socialization problems and ability to follow instructions, among others, which are more pertinent for children aged 72 months plus given the new challenges and situations they face. Following (Reynolds et al., 2017), the CBCL was internally normalized using means and standard deviations from children of the same age.
It is important to be aware of the potential socioeconomic biases in psychometric measures; there is evidence that CBCL may be influenced by factors that are correlated with SES (Gross et al., 2006; Schneiders, 2003). For example, Gross et al. (2006) argues that low scores from children from low-income families could be the result of parents being anxious or stressed when answering the questionaries or that parents from minority ethnic groups or low-income groups could interpret behavioral problems differently than their peers.
Household SES Measure
To measure household SES status, we follow Pollitt et al. (1993), Filmer and Pritchett (2001), and Galasso et al. (2019), among others and use the ELPI questions on household assets, dwelling ownership, and number of bathrooms and sleeping-only rooms to create our SES proxy. This index was derived through principal component analysis based on the first component (eigenvalue = 3.89), consistent with 30% of the variance in the data. We then ranked it and divided it into quintiles, with the first quintile being the lowest SES and the fifth quintile the highest SES. This SES proxy has been widely used to analyze gradients in child outcomes in both high- and low-and middle-income countries (Fernald et al., 2011; Galasso et al., 2019; Schady et al., 2015).
The assets included in the index are having a refrigerator, washing machine, VCR or DVD player, microwave, water heater, video camera, paid internet connection, desktop computer, laptop computer, paid TV service, and house ownership. In our data, the index differentiates household’s SES as proxied by assets, presented in Table 1. For example, while 16% of households in the lowest quintile have paid internet access and 47% own their home, 63% of households in the highest quintile have internet access and 67% own their home. Although this SES index is preferred over income variables since it is less likely to be affected by measurement errors and seasonal volatility, we also perform robustness analysis using per capita household income and the sum of assets; our results are unchanged. Measurement errors in income or the SES index would lead to attenuation bias, e.g., we would be observing a lower bound of the relationship of income or SES gradients on our outcomes.
Covariates
Early Child Conditions
Early child conditions were assessed using birth order, household size, and height and weight at birth. Height and weight were collected retrospectively in 2010. To minimize the risk of measurement errors, mothers were asked to show the birth registrations or certificates provided by the hospitals where the children were born. Those who did not have such documents self-reported.
Parental Endowments
To assess the role of parental endowments, we include the maternal schooling level and the maternal numerical and verbal Wechsler Adult Intelligence Scale (WAIS) test scores (Wechsler, 1955). The latter were taken by a trained psychologist during the same household visit when the child was evaluated. Further details on this test can be found in Online Appendix 1.
Household Determined Inputs
Household inputs are measured using two variables: a dummy indicating whether the child attended preschool (nursery school or pre-kindergarten) in 2010 or 2012, and a household-environment scale that combines mother-reported variables and interviewer-reported variables from the Home Observational for the Measurement of the Environment (HOME) inventory. Those variables range from 0 to 10 and captures learning environments fostering growth and education or active child stimulation, which can help children thrive in spite of poverty (Blair & Raver, 2012; Bradley & Corwyn, 2002; Evans, 2004; Galasso et al., 2019). The list of included items in the household-environment scale and its sources is given in Table 2.
Sample
To evaluate anthropometric, receptive vocabulary, and socio-emotional development, we use three different samples according to the age range covered by each test. The first sample consists only of children with anthropometric data for 2010 and 2012 (Anthropometric Longitudinal Sample), the second sample is those with PPVT data for 2010 and 2012 (PPVT Longitudinal Sample), and the third sample includes children with CBCL data for 2010 and 2012 (CBCL Longitudinal Sample). In Table 3, we show descriptive statistics of the covariates for the three samples. As already mentioned, the three samples are different sizes since the tests cover different age ranges: the anthropometric longitudinal sample is children from 31 to 83 months old in 2012, the PPVT and CBCL longitudinal samples are children 52–83 and 39–83 months, respectively. In general, the three samples have similar observed characteristics, and the main differences are due to age differences among the samples. For example, in all samples around 45% are first-born children, mother’s and father’s average grades of schooling attainment around 11.5, and length at birth is almost 50 cm.
The attrition rate between rounds was 13.4%, and in Table A3 in the Online Appendix we show the attrition analysis for HAZ, CBCL, and PPVT. Children from the second and fourth SES quintiles are less likely to attrit, and children with more educated fathers are more likely to attrit. To control for attrition, we use longitudinal sampling weights for the entire sample. Our sample also has some additional restrictions. To start with, we only included interviews with biological mothers (98.9% of the sample). Then, we required children in our sample to have dependent variable measurements for both years (93.67% of the sample for anthropometrics, 99.35% for cognitive, and 99.11% for socio-emotional development) and no missing values in the covariates (79.96% for anthropometrics, 66.02% for cognitive, and 70.29% for socio-emotional development). Despite these restrictions, the samples remain similar in terms of covariates (Online Appendix Table A4).
Statistical Analysis
Following the standard approach in the literature (Fernald et al., 2011; Lopez Boo, 2016; Schady et al., 2015), we use regression models to study SES disparities in anthropometric measures and skills. We begin with the following parametric base model:
where \({Y}_{i}\) is the standardized outcome (anthropometric or skill measure) of child \(i\), \({A}_{i,j}\) is a dummy variable that takes the value 1 if the family of child \(i\) belongs to SES quintile \(j\) and 0 if not, with the first quintile as the reference (excluded) quintile. \({X}_{i}\) stands for child demographics such as sex (male = 1), region of residence (one dummy for each of the 15 regions), monthly age in 2012, and mothers’ schooling in 2010, among other variables. The error term \({\upepsilon }_{i}\) is clustered at the regional level.
Equation (1) allows us to study gross SES disparities, and the coefficients show us the raw SES disparities among the children. As is usual in the literature, these parameters cannot be interpreted as causal since there could be bias arising from omitted variables or measurement errors.
To assess the robustness of the results, we control for a vector of observed variables that might be confounding or mediating the relationship between SES gradients and each of the outcomes. We also exploit the survey’s longitudinal dimension and include early child characteristics (\({C}_{i})\) and lagged child development outcomes\({(Y}_{i, 2010 })\). The inclusion of lagged scores allows us to control for past investments and evaluate if SES gaps accumulate over childhood or if they occur only at certain ages, providing information on the dynamics of SES disparities.Footnote 2
These changes lead to the following specification:
where \({P}_{i,}\) stands for maternal endowments (schooling and cognitive tests) and \({H}_{i}\) for household inputs (household-environment index and preschool attendance).
In Eq. (2), SES disparities are captured by the parameters \({\beta }_{j}\) that show the baseline SES association and \({\delta }_{3}\) that shows the dynamic SES association. Even if \({\beta }_{j}\) is not statistically significant, SES might still play a role through \({\delta }_{3}\) and SES disparities for \({Y}_{i, 2010}\). \({\delta }_{3}\) shows convergence: if \({\delta }_{3}\) is not significantly different from one there is no convergence, if \({\delta }_{3}\) is not significantly different from zero there is complete convergence, and if \({\delta }_{3}\) is significantly greater than zero and less than one there is partial convergence.Footnote 3
Including the additional variables in Eq. (2) and comparing it with Eq. (1) allow us to go beyond much of the previous literature by investigating to what extent the disparities estimated in Eq. (1) are attenuated by allowing for dynamics. Note that because the dependent variables are defined as z scores, the right-side coefficient estimates can be compared across child outcomes since they all represent the impact of a one-unit change in the relevant right-side variable on standard deviations in child outcomes in the reference populations.
To study SES disparities using age groups that allow for comparability among the outcomes, we use two different samples divided by age: younger than 72 months old and 72 months old or older. We use this threshold since most children start primary school at that age, which could impact skill formation and the role of SES.
Results
Raw SES Gaps
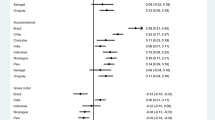
In Fig. 1, we present the variation of anthropometrics at birth by the SES (wealth) index. It shows that, while there are no statistically significant differences in birth weight-for-height z scores (WHZ) by SES, children from the lowest SES households are slightly taller than those from the highest families. This is somewhat surprising but may reflect three potential factors. First, there is a higher prevalence of cesarean births and shorter gestation periods for the fifth quintile: while in the first quintile about one third of births are Cesareans, this percentage is above 50% for the highest quintile (see Online Appendix 5 for an analysis of birth type and gestation period). Second, in Chile, there are differences in mortality rates by mother’s schooling, with larger mortality rates for mothers with lower education (Aguilera et al., 2020), that could also explain the differences on length at birth. However, the relatively low mortality rate in Chile suggests that this mechanism probably has a small effect. Third, there may be measurement error by SES status, as data on height and weight at birth are collected retrospectively. In Online Appendix 2, we analyze this issue in more detail, finding that this does not seem to differ by SES. Specifically, we focus on the information that households have about health status of their children, specifically their vaccine record cards. We find that poorer households have vaccine cards more often than richer households (74% vs 64%, respectively). This is not consistent with the lowest SES households having less information and therefore being more prone to measurement error.

Length- and weight-for-length z scores (HAZ, WHZ) at birth across SES index score
Despite the initial advantage in HAZ for children in the bottom SES quintile, by 10 months of age, differences in HAZ between the lowest and highest quintiles reverse and favor higher quintiles (see the first panel in Fig. 2). These differences reach a peak around 20 months of age and then decrease until there are no statistically significant differences at around 80 months.

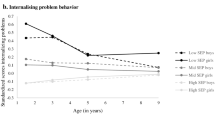
HAZ, PPVT, and CBCL gaps between first and fifth SES quintiles by age
From the second panel in Fig. 2, we observe that by 30 months of age there are some significant differences in receptive vocabulary skills between the lowest and highest quintile, which increase for children in the 30–50-month age range. The third panel shows the case of socio-emotional skill: differences in social behavior by SES already exist at 20 months of age but decrease with age.
Statistical Analysis of SES Gradients
Table 4 presents the estimated SES coefficients for the top quintile relative to the bottom quintile across four specifications for HAZ, PPVT, and CBCL. Full-model results are included in Tables A6–A8 in the Online Appendix. The first specification includes SES index quintiles and demographic variables such as age and sex. In the following specifications, covariates are included sequentially. All outcomes were corrected for multiple testing and the results hold, which is shown in Online Appendix Table A9. The number of observations remains almost constant by model; any differences are less than ten observations and are due to some missing mediators.
Anthropometric Results
For children between 33 and 71 months of age, the gross SES coefficient estimate gap between the lowest and highest quintile is 0.26 favoring the latter. This gap diminishes to 0.13 when adjusting for lagged HAZ and early child conditions. When further adjusting for parental endowments and household inputs, the gap remains stable at 0.12 and is statistically significant. For children between 72 and 83 months of age, the gross SES coefficient estimate gap is 0.28. When adjusting for the lagged HAZ, early child characteristics, and parental endowment, the coefficient estimate gap is still positive but loses its statistical significance. No differences are observed in the SES gradient when also adjusting for household inputs.
In terms of the other covariates, the lagged HAZ is significantly non-zero indicating there is some persistence, but it is also significantly different from one so there is also some partial convergence (test results available upon request). The coefficient estimate for lagged HAZ is larger for the older age range, suggesting greater persistence with age.
Receptive Vocabulary Development Results
For children under 72 months of age, there are relatively larger differences by SES quintile for PPVT: children from the highest quintile have on average, 0.65 higher PPVT z scores than those from the lowest quintile. When including lagged PPVT and early child conditions as covariates, the coefficient estimate decreases to 0.39. When further adjusting for parental endowments and home inputs, the coefficient estimate declines to 0.18. Despite the inclusion of covariates, the coefficient estimate remains strongly statistically significant, meaning children in the fifth quintile have 0.18 SD higher scores on the PPVT test compared to those in the lowest quintile.
In the second panel of Table 4, we observe that for older children there are still large differences by quintile when only demographics are included (baseline model): children in the fifth quintile have 0.80 higher scores than those in the first quintile. When all covariates are included, the differences remain significant at 0.26.
The coefficient estimates of the lagged test scores are significantly non 0 and different than 1.0 (test results available upon request) indicating some persistence in SES disparities with partial convergence. They also increase with age, as do the lagged effects of anthropometrics, from 0.45 for the youngest children to 0.63 for the oldest. This increase might explain in part the lower SES differences by quintiles for older compared to younger children. Note that the lagged coefficient estimates are smaller for the PPVT scores than for HAZ, indicating greater convergence for these test scores than for anthropometrics.
Socio-emotional Development Results
For socio-emotional skills (CBCL), we find smaller gross SES coefficient estimate disparities than for PPVT. In the base model (Table 4, column (i)), for children under 72 months old, the SES coefficient estimate gap is − 0.53 and almost halves in magnitude when including lagged tests and early child conditions (note again that a lower CBCL score means that the child has higher socio-emotional skills). Further adjustment for household inputs makes the SES gradient even smaller but still significant. Children from the highest quintile have on average 0.09 lower scores than children from the lowest one.Footnote 4
For children between 72 and 83 months old, the SES disparities start lower in the base model (0.28), and there are no significant SES associations when including covariates. The SES gap is not statistically significant when adjusting for maternal endowments and even changes sign. This pattern indicates that mediators are playing a role in the initial gap, and each time we include a new group of mediators, they are significant and impactful (see Table A5). In terms of dynamics of socio-emotional skills, there is less persistence as children became older, the opposite of what occurs for receptive vocabulary skills. The coefficient for the lag of the CBCL scores goes from 0.37 for children younger than 72 months to 0.32 for children older than 72 months.
Mediation Analysis
To test if and how the adjustment for family characteristics attenuates the associations between SES and child development, we perform mediation analysis for the following mediators: mother’s schooling attainment, mother’s numeric WAIS test scores, mother’s vocabulary WAIS test scores, household environment, and preschool attendance. Most of these mediators are included in the literature, but we improve on the literature by adding a new mediator: mother’s cognitive test scores. Starting from the baseline specification that includes SES quintile dummies, lagged child HAZ, PPVT or CBCL, and early childhood conditions, we include one mediator at a time and calculate the percentage change in the SES gap between the fifth and first quintiles. Finally, we include all mediators to account for the overall reduction in the gap in coefficient estimates. Results are seen in Table 5 and Online Appendix Tables A11–A13.
First, we analyze mediators for HAZ. We find that length at birth and household size mediators remain statistically significant after including previous HAZ measures (See Online Appendix Table A11). However, there are interesting changes when adding mediators to our models, which differ by child age; there is a SES coefficient estimate gap of 0.13 for children younger than 72 months after including demographics, the lagged test, and birth variables (see column (i) in Online Appendix Table A11), which is stable to the inclusion of all mediators (see column (vii) in Online Appendix Table A11). Therefore, all mediators together account for 12.1% of the coefficient estimate gap (See Table 5). For children 72 months old and older, the coefficient estimate gap including demographics, the lagged test, and birth variables is 0.278 and is statistically significant (see column (viii) in Online Appendix Table A11). The SES coefficient estimate gap shrinks significantly and loses statistical significance when including parental endowments such as the mother’s education, vocabulary test scores, and household inputs. The most striking result is that the mother’s vocabulary test is negatively related to HAZ, and its inclusion results in a larger coefficient estimate gap for HAZ. These results could be explained by a third variable such as employment, hours worked, or marital sorting, that is correlated with mother’s ability and SES. There is also a dynamic relationship of maternal skills through the lagged HAZ, which could be counterbalancing the negative baseline SES relationship. Finally, as discussed before, Chile presents relative similar birth anthropometrics across SES so that this negative sign could be capturing a negative relationship between initial health conditions and mother´s WAIS.
For PPVT, we find several mediators that seem to explain large portions of the SES coefficient estimate gap, which can be seen in Tables 5 and A12. The most important mediator is mother’s schooling, which explains 40.2% of the SES coefficient estimate gap. Mother’s vocabulary test score explains around 18% of the coefficient estimate gap for children of all ages. In terms of household inputs, preschool attendance is only relevant for older children, and the household-environment index decreases in importance as children age, going from 21.2 to 7%. These results suggest that parents could be compensating for preschool attendance with activities at home when children are younger, but that preschool pays off at older ages. Overall, mediators are consistent with large part of the coefficient estimate gap, 54.7% for children younger than 72 months, and 43.8% for children 72 months old or older. Despite this reduction, the SES coefficient estimate gap remains for children’s vocabulary skills even after all of the mediators are included.
In terms of the role of mother’s schooling, our results for PPVT show that the inclusion of household inputs and mother’s cognitive ability decreases the relevance of her schooling. In the case of children younger than 72 months, the coefficient estimate on mother’s schooling changes from 0.04 when only that variable is included to 0.027 when all variables are included (a 32% drop), while from children 72 months of age or older, the drop is from 0.035 to 0.022 (a 34% drop). These results suggest that the gross mediation between mothers’ schooling and SES gaps is partly related to different household inputs proxied by our home index and partly related to mother’s vocabulary test.
In the case of socio-emotional skills (third panel in Table 5), we again find that mother’s schooling is the most relevant mediator. For younger children, half of the SES coefficient estimate gap is mediated by mother’s schooling. The second most relevant mediator is household environment, which accounts for 31.4% of the coefficient estimate gap. Among the remaining mediators, father’s schooling and mother’s ability are the most relevant. For older children, there is no significant SES coefficient estimate gap to start with, nonetheless, again mother’s cognitive abilities and the household-environment index apparently are the most relevant mediators in this context.
For SES skills, we also find that the inclusion of mother’s ability and household inputs reduce the mediating role of mothers’ schooling. For children younger than 72 months of age, including all mediators decrease the coefficient estimate of mother’s schooling from − 0.031 to − 0.021 (32% drop), while for children 72 months of age and older, the change is from − 0.036 to − 0.026 (28% drop), indicating again that household inputs and mother’s cognitive ability are related to the role of mother’s schooling on skill formation.
Sensitivity Analysis
To assess the robustness of our results to changes in the measure of SES, we re-estimated all our models using quintiles of per capita household income instead of the asset index. We found that income gradients are smaller and less stable to the inclusion of covariates (Online Appendix Table A14). This may be related to the fact the income is much more volatile than the SES index and has a smaller association with test scores. Additionally, income might have a higher degree of measurement error, which leads to a larger attenuation bias.
We also re-estimated using the sum of owned assets as a SES index, and results hold (see Online Appendix Table A15). The measure using our PCA is preferred since it allows different weights for different assets and is also the standard in the literature (Fernald et al., 2011; Galasso et al., 2019; Rubio-Codina et al., 2015, among others).
Furthermore, since in our sample girls systematically do better than boys on PPVT and CBCL, we also explored whether there are systematic differences in SES coefficient estimate disparities by sex and found no significant consistent differences (Tables A16 and A17).
Finally, to study whether early disparities in HAZ are associated with SES coefficient estimate disparities in cognitive or socio-emotional skills, we included lagged HAZ as an additional regressor in the specifications for PPVT and CBCL. We find that the lagged anthropometrics have statistically significant coefficient estimates, but the changes in estimated SES coefficient estimate disparities are very small, which indicates disparities in anthropometrics are not associated with disparities in either receptive vocabulary or socio-emotional skills (Online Appendix Table A18).
Discussion
We contribute to the literature by using a nationally representative longitudinal survey, simultaneously studying several outcomes: anthropometrics, receptive vocabulary skills, and socio-emotional skills. Our longitudinal data allow us to test the cumulative impact of SES on skills by controlling for lagged outcome levels and to identify the extent to which SES coefficient estimate disparities persist when controlling for parental endowments and abilities, child characteristics, and household inputs. Our data also allow us to perform mediation analysis to evaluate whether family practices and characteristics are attenuating or strengthening the associations between SES and our outcome variables.
Our study is particularly relevant in a country like Chile that has both high-income inequality and good average-health outcomes at the same time, since it allows us to investigate what happens in Chile between birth and mid childhood that transforms newborns who are relatively similar in terms of length and weight at birth into adults with extremely different outcomes.
Our results align with previous literature finding strong relationships between indicators of socioeconomic status and early life human capital. We found that SES disparities have important predictive power on receptive vocabulary scores even after controlling for several relevant variables. These differences start as early as in the second year of life and continue at least until children are 83 months old, with children in the highest quintile obtaining 0.14–0.19 higher scores on the PPVT test compared to children in the lowest quintile.
SES is less associated with anthropometrics and socio-emotional skills for children starting in their second year and continuing through 72 months of age. Moreover, for older children, we do not find any SES coefficient estimate gaps for anthropometrics and socio-emotional skills. One potential reason for more tenuous anthropometric differences is the widespread access to nutritional support and health provisions through a massive milk program that has been in place for over 50 years and includes mothers and children up to 6 years of age, and the availability of food at school for all children, which may have helped to reduce socioeconomic anthropometric disparities.
Small differences at birth but larger and persistent cognitive disparities shortly after are consistent with the history of Chile’s health care system: a relatively developed health system that dates back to at least the mid-1950s and provides good prenatal care, but poorer postnatal growth and health care (Contreras & Puentes, 2017). To evaluate if family characteristics or practices strengthen or attenuate the associations between SES and child outcomes, we performed mediation analysis. In this analysis, an index of household environment tends to be significant; we find that home inputs are particularly important before entering school, mediating between 21 and 31% of children vocabulary and socio-emotional skills, respectively. This is higher than what is usually found in the literature (Galasso et al., 2019). This finding provides potential scope for policy action in equalizing child outcomes through, for example, properly evaluated child stimulation programs.
Another key result is that initial conditions, measured as length- and weight at birth, do not affect skill formation. This may be because there are no significant differences at birth favoring the highest quintile. Surprisingly for length at birth, differences favor the lowest over the highest quintile. The reason for this could be twofold: while it could be related to the Chilean ante-natal care system doing well in avoiding discrepancies in birth outcomes, we cannot rule out the possibility of mortality selection bias, in which most frail children would be lost to mortality for lower SES households, but may be able to survive in wealthier households. Regardless, this does not continue into the second year of life, and SES disparities start to emerge.
Our results also show that mother's schooling and cognitive ability are important correlates for skill formation. That both variables are significant and that including maternal cognitive ability decreases the apparent mediating role of her schooling might reflect there is some genetic transmission of abilities and/or that increased schooling provided mothers with tools to raise their children. We find that one additional grade of mother’s schooling attainment is associated with a 0.025 SD increase in receptive vocabulary skills for both younger and older children and an increase in socio-emotional skills of 0.017 SD and 0.019 SD for younger and older children, respectively. These results suggest that the disparity between the top and bottom quintiles is equal to the impact of about 5–6 years of maternal schooling in receptive vocabulary skills, and more than 3 grades in socio-emotional skills.
Mother’s cognitive ability only has significant associations with cognitive skills for children with less than 72 months of age. Maternal vocabulary WAIS is positively associated with socio-emotional skills for children of all ages. To offset the SES gap in cognitive and socio-emotional skills, an increase of 1–2 SD would be needed in maternal vocabulary WAIS scores and around 7 grades in maternal education.
We also look at the impact of preschool attendance and household environment, which are variables that public policy could address in order to narrow impacts of SES gaps. Preschool attendance is positively and significantly associated with vocabulary skills only for older children, but it appears to mediate 4% of the gap between the gap in receptive vocabulary skills between children in the first and fifth quintiles. Despite its relative importance for cognitive skills, preschool attendance is not statistically related to either HAZ or CBCL.
Our household-environment index is positively associated with both vocabulary and socio-emotional skills; a one-point increase in our household index is associated with 0.038 SD and 0.022 SD improvements in receptive vocabulary skills and 0.038 SD and 0.051 SD improvements in socio-emotional skills for children under and over 72 months of age, respectively. The SES coefficient estimate gap in children’s socio-emotional skills between the first and fifth quintile is about the same as an increase of 1.5 points in the household index. This is equivalent to the gap between the household index of an average household in the first quintile and the fourth. On the other hand, using household environment to offset SES gradients in receptive vocabulary is similar to an increase of 3.5 and 8.7 points in the household index (for younger and older children, respectively), which are higher than the household index differences between the first and fifth quintiles.
That the lags of the skills tests are significantly greater than zero and different from one (test results available upon request) highlights the dynamic nature of skill formation. This persists but there is also partial convergence. SES disparities persist but became smaller over time, with a greater convergence for skills than for anthropometrics.
There are several limitations to our analysis. First we do not have access to data on important mediators such as iron-deficiency anemia, food, preschool quality, and health care access (Lopez Boo, 2016). Second, the mediation analysis does not provide causal relationships. For example, we find that a positive correlation between the home environment Index but there could be another factor explaining both the index and outcomes (such as the mother’s or father’s socio-emotional skills). Finally, the attrition rate is relatively large (13.4%), and while we attempt to control for it, unobserved factors (such as health or income shocks) could be explaining the attrition and biasing our analysis.
Conclusion
Our results show gaps in anthropometrics, receptive vocabulary, and socio-emotional skills favoring the better-off arise early in life, are large and persistent, and remain stable until at least 6 years of age. The analysis of covariates, together with the mediation analysis, allowed us to further investigate what happens in Chile between birth and mid childhood that transforms newborns who are relatively similar in terms of weight and height at birth into adults with extremely different outcomes.
Similarly to Contreras and Puentes (2017), we conclude these results are consistent with a system in which good prenatal care does well in avoiding SES discrepancies in birth outcomes. However, this does not continue past the first year of life, when SES disparities start to emerge and widen.
With respect to other Latin American countries, we find that in Chile gaps tend to be smaller with respect to cognitive development as shown in (Schady et al., 2015). For example, for Peru, Lopez Boo (2016), finds larger differences even after controlling for several mediators, 0.5 standard deviations in PPVT for children 5 years old, and 0.59 standard deviations for children 8 years old. Results for Bogotá (Rubio-Codina et al., 2016), although for a younger sample, show that after controlling for several mediators, only the SES gaps for cognition remain, while SES gaps are not significant for socio-emotional skills. For Madagascar, (Galasso et al., 2019) using a methodology similar to ours find that the SES gradients range from 0.29 to 0.53. At the same time, household inputs in Chile are more relevant as mediators, which in turn might explain why the gap is lower in Chile. This suggests that some of the public policies implemented in Chile might have reduced the SES disparities.
Our results reinforce the importance of investing in early childhood development for children in poorer households especially the household learning environment in order to improve socio-emotional gaps. At the same time, they suggest it would be harder to close gaps for receptive vocabulary skills. Therefore, policies such as “Chile Crece Contigo” that start at gestation and continue until the age of 9 and do not only monitor a child’s health and nutritional status but also give age-specific learning materials are a good public policy to reduce these gaps or, even better, to prevent their emergence.
Data Availability
The data used in this study are publicly available and can be accessed through the following link: http://observatorio.ministeriodesarrollosocial.gob.cl/elpi/elpi_bd.php
Notes
Retrieved from https://urldefense.com/v3/__https://data.worldbank.org/indicator/SP.DYN.IMRT.IN?locations=CL__;!!NLFGqXoFfo8MMQq71YXunZaMDwegdtuxDTcUn4TU8kikv_OTM1qmi94r7TUUYvB383LxlT3qyN0nMjf2tBzncY0kBiGPq1-yZa8mSy918k$
A similar strategy was followed by Schady, (2011).
These definitions are not mutually exclusive, but they provide insight about the level of convergence (or lack thereof) that can be derived from the results. We perform a test for significance in each case, and also a test of the coefficient being equal to one.
In Table A10 in the Appendix, we present the results using the subsample that has data for three outcomes, thus for the CBCL, we are including only children who are over 52 months old. We observe that there are no significant SES coefficient estimate differences for children between 52 and 72 months old. Therefore, there are significant differences by SES for socio-emotional skills only for children younger than 52 months.
References
Achenbach, T. M., & Edelbrock, C. (1991). Child behavior checklist. Burlington (Vt), 7, 371–392.
Aguilera, X., Delgado, I., Icaza, G., Apablaza, M., Villanueva, L., & Castillo-Laborde, C. (2020). Under five and infant mortality in Chile (1990–2016): Trends, disparities, and causes of death. PLoS ONE, 15(9), e0239974. https://doi.org/10.1371/journal.pone.0239974
Almond, D. (2006). Is the 1918 influenza pandemic over? Long-term effects of in utero influenza exposure in the post-1940 US population. Journal of Political Economy, 114(4), 672–712. https://doi.org/10.1086/507154
Almond, D., & Currie, J. (2011). Killing me softly: The fetal origins hypothesis. Journal of Economic Perspectives, 25(3), 153–172. https://doi.org/10.1257/jep.25.3.153
Almond, D., Currie, J., & Duque, V. (2018). Childhood circumstances and adult outcomes: Act II. Journal of Economic Literature, 56(4), 1360–1446. https://doi.org/10.1257/jel.20171164
Anselmi, L., Barros, F. C., Teodoro, M. L., Piccinini, C. A., Menezes, A. M. B., Araujo, C. L., & Rohde, L. A. (2008). Continuity of behavioral and emotional problems from pre-school years to pre-adolescence in a developing country. Journal of Child Psychology and Psychiatry, 49(5), 499–507. https://doi.org/10.1111/j.1469-7610.2007.01865.x
Arimond, M., & Ruel, M. T. (2004). Dietary diversity is associated with child nutritional status: Evidence from 11 demographic and health surveys. The Journal of Nutrition, 134(10), 2579–2585.
Aughinbaugh, A., & Gittleman, M. (2003). Does money matter? A comparison of the effect of income on child development in the United States and Great Britain. The Journal of Human Resources, 38(2), 416–440. https://doi.org/10.2307/1558750
Aurino, E., Schott, W., Behrman, J. R., & Penny, M. (2019). Nutritional status from 1 to 15 years and adolescent learning for boys and girls in Ethiopia, India, Peru, and Vietnam. Population Research and Policy Review, 38(6), 899–931. https://doi.org/10.1007/s11113-019-09557-8
Bainbridge, J., Meyers, M. K., Tanaka, S., & Waldfogel, J. (2005). Who gets an early education? Family income and the enrollment of three-to five-year-olds from 1968 to 2000. Social Science Quarterly, 86(3), 724–745.
Bando, R., López-Boo, F., & Li, X. (2016). Sex-differences in language and socio-emotional skills in early childhood. Inter-American Development Bank.https://doi.org/10.18235/0000500
Barker, D. J. (1990). The fetal and infant origins of adult disease. BMJ (clinical Research Ed.), 301(6761), 1111. https://doi.org/10.1136/bmj.301.6761.1111
Becker, G. S., & Tomes, N. (1979). An equilibrium theory of the distribution of income and intergenerational mobility. Journal of Political Economy, 87(6), 1153–1189. https://doi.org/10.1086/260831
Behrman, J. R., Calderon, M. C., Preston, S. H., Hoddinott, J., Martorell, R., & Stein, A. D. (2009). Nutritional supplementation in girls influences the growth of their children: Prospective study in Guatemala. The American Journal of Clinical Nutrition, 90(5), 1372–1379. https://doi.org/10.3945/ajcn.2009.27524
Behrman, J. R., Pollak, R. A., & Taubman, P. (1982). Parental preferences and provision for progeny. Journal of Political Economy, 90(1), 52–73. https://doi.org/10.1086/261039
Behrman, J. R., & Rosenzweig, M. R. (2004). Returns to birthweight. Review of Economics and Statistics, 86(2), 586–601. https://doi.org/10.1162/003465304323031139
Black, M. M., Behrman, J. R., Daelmans, B., Prado, E. L., Richter, L., Tomlinson, M., Trude, A. C. B., Wertlieb, D., Wuermli, A. J., & Yoshikawa, H. (2021). The principles of Nurturing Care promote human capital and mitigate adversities from preconception through adolescence. BMJ Global Health, 6(4), e004436. https://doi.org/10.1136/bmjgh-2020-004436
Black, M. M., Walker, S. P., Fernald, L. C. H., Andersen, C. T., DiGirolamo, A. M., Lu, C., McCoy, D. C., Fink, G., Shawar, Y. R., Shiffman, J., Devercelli, A. E., Wodon, Q. T., Vargas-Barón, E., & Grantham-McGregor, S. (2017). Early childhood development coming of age: Science through the life course. The Lancet, 389(10064), 77–90. https://doi.org/10.1016/S0140-6736(16)31389-7
Blair, C., & Raver, C. C. (2012). Child development in the context of adversity: Experiential canalization of brain and behavior. American Psychologist, 67(4), 309.
Blair, C., & Raver, C. C. (2016). Poverty, stress, and brain development: New directions for prevention and intervention. Academic Pediatrics, 16(3 Suppl), S30-36. https://doi.org/10.1016/j.acap.2016.01.010
Bradley, R. H., & Corwyn, R. F. (2002). Socioeconomic status and child development. Annual Review of Psychology, 53(1), 371–399.
Campbell, F., Conti, G., Heckman, J. J., Moon, S. H., Pinto, R., Pungello, E., & Pan, Y. (2014). Early childhood investments substantially boost adult health. Science (new York, NY), 343(6178), 1478–1485. https://doi.org/10.1126/science.1248429
Coddington, C. H., Mistry, R. S., & Bailey, A. L. (2014). Socioeconomic status and receptive vocabulary development: Replication of the parental investment model with Chilean preschoolers and their families. Early Childhood Research Quarterly, 29(4), 538–549. https://doi.org/10.1016/j.ecresq.2014.06.004
Conley, D., & Bennett, N. G. (2000). Is biology destiny? Birth weight and life chances. American Sociological Review. https://doi.org/10.2307/2657467
Contreras, D., & González, S. (2015). Determinants of early child development in Chile: Health, cognitive and demographic factors. International Journal of Educational Development, 40, 217–230. https://doi.org/10.1016/j.ijedudev.2014.06.010
Contreras, D., & Puentes, E. (2017). Inequality of opportunities at early ages: Evidence from Chile. The Journal of Development Studies, 53(10), 1748–1764. https://doi.org/10.1080/00220388.2016.1262025
Crookston, B. T., Schott, W., Cueto, S., Dearden, K. A., Engle, P., Georgiadis, A., Lundeen, E. A., Penny, M. E., Stein, A. D., & Behrman, J. R. (2013). Postinfancy growth, schooling, and cognitive achievement: Young Lives. The American Journal of Clinical Nutrition, 98(6), 1555–1563. https://doi.org/10.3945/ajcn.113.067561
Cunha, F., & Heckman, J. J. (2008). Formulating, identifying and estimating the technology of cognitive and noncognitive skill formation. Journal of Human Resources, 43(4), 738–782. https://doi.org/10.3368/jhr.43.4.738
Currie, J. (2009). Healthy, wealthy, and wise: Socioeconomic status, poor health in childhood, and human capital development. Journal of Economic Literature, 47(1), 87–122. https://doi.org/10.1257/jel.47.1.87
Currie, J., & Almond, D. (2011). Human capital development before age five. In Handbook of labor economics (Vol. 4, pp. 1315–1486). Elsevier. https://doi.org/10.3386/w15827
de Onis, M., Onyango, A. W., Borghi, E., Siyam, A., Nishida, C., & Siekmann, J. (2007). Development of a WHO growth reference for school-aged children and adolescents. Bulletin of the World Health Organization, 85, 660–667. https://doi.org/10.2471/blt.07.043497
Dunn, L. M., Padilla, E. R., Lugo, D. E., & Dunn, L. M. (1986). Manual del examinador para el Test de Vocabulario en Imágenes Peabody. American Guidance Service.
Evans, G. W. (2004). The environment of childhood poverty. American Psychologist, 59(2), 77.
Fernald, L. C., Kariger, P., Hidrobo, M., & Gertler, P. J. (2012). Socioeconomic gradients in child development in very young children: Evidence from India, Indonesia, Peru, and Senegal. Proceedings of the National Academy of Sciences, 109(Supplement 2), 17273–17280. https://doi.org/10.1073/pnas.1121241109
Fernald, L. C., Weber, A., Galasso, E., & Ratsifandrihamanana, L. (2011). Socioeconomic gradients and child development in a very low income population: Evidence from Madagascar. Developmental Science, 14(4), 832–847. https://doi.org/10.1111/j.1467-7687.2010.01032.x
Filmer, D., & Pritchett, L. H. (2001). Estimating wealth effects without expenditure data-or tears: An application to educational enrollments in states of India. Demography, 38(1), 115–132. https://doi.org/10.2307/3088292
Foster, Z., Byron, E., Reyes-García, V., Huanca, T., Vadez, V., Apaza, L., Pérez, E., Tanner, S., Gutierrez, Y., & Sandstrom, B. (2005). Physical growth and nutritional status of Tsimane’ Amerindian children of lowland Bolivia. American Journal of Physical Anthropology: THe Official Publication of the American Association of Physical Anthropologists, 126(3), 343–351.
Galasso, E. W., Fernald, A., & Lia, C. H. (2019). Dynamics of child development: Analysis of a longitudinal cohort in a very low income country. World Bank Economic Review, 33(1), 140–159. https://doi.org/10.1093/wber/lhw065
Gertler, P., Heckman, J., Pinto, R., Zanolini, A., Vermeersch, C., Walker, S., Chang, S. M., & Grantham-McGregor, S. (2014). Labor market returns to an early childhood stimulation intervention in Jamaica. Science, 344(6187), 998–1001. https://doi.org/10.1126/science.1251178
Grantham-McGregor, S., Cheung, Y. B., Cueto, S., Glewwe, P., Richter, L., & Strupp, B. (2007). Developmental potential in the first 5 years for children in developing countries. The Lancet, 369(9555), 60–70. https://doi.org/10.1016/S0140-6736(07)60032-4
Gross, D., Fogg, L., Young, M., Ridge, A., Cowell, J. M., Richardson, R., & Sivan, A. (2006). The equivalence of the child behavior checklist/1 1/2-5 across parent race/ethnicity, income level, and language. Psychological Assessment, 18(3), 313–323. https://doi.org/10.1037/1040-3590.18.3.313
Heckman, J. J., Moon, S. H., Pinto, R., Savelyev, P., & Yavitz, A. (2010). A new cost-benefit and rate of return analysis for the Perry preschool program: A summary (No. w16180). National Bureau of Economic Research. https://doi.org/10.3386/w16180
Heckman, J. J., Stixrud, J., & Urzua, S. (2006). The effects of cognitive and noncognitive abilities on labor market outcomes and social behavior. Journal of Labor Economics, 24(3), 411–482. https://doi.org/10.3386/w12006
Hoddinott, J., Alderman, H., Behrman, J. R., Haddad, L., & Horton, S. (2013a). The economic rationale for investing in stunting reduction. Maternal & Child Nutrition, 9(S2), 69–82. https://doi.org/10.1111/mcn.12080
Hoddinott, J., Behrman, J. R., Maluccio, J. A., Melgar, P., Quisumbing, A. R., Ramirez-Zea, M., Stein, A. D., Yount, K. M., & Martorell, R. (2013b). Adult consequences of growth failure in early childhood. The American Journal of Clinical Nutrition, 98(5), 1170–1178. https://doi.org/10.3945/ajcn.113.064584
Hoddinott, J., Maluccio, J. A., Behrman, J. R., Flores, R., & Martorell, R. (2008). Effect of a nutrition intervention during early childhood on economic productivity in Guatemalan adults. The Lancet, 371(9610), 411–416. https://doi.org/10.1016/s0140-6736(08)60205-6
Laith, R., & Vaillancourt, T. (2022). The temporal sequence of bullying victimization, academic achievement, and school attendance: A review of the literature. Aggression and Violent Behavior, 64, 101722. https://doi.org/10.1016/j.avb.2022.101722
Lopez Boo, F. (2016). Socio-economic status and early childhood cognitive skills: A mediation analysis using the Young Lives panel. International Journal of Behavioral Development. https://doi.org/10.1177/0165025416644689
Lugo-Gil, J., & Tamis-LeMonda, C. S. (2008). Family resources and parenting quality: Links to children’s cognitive development across the first 3 years. Child Development, 79(4), 1065–1085.
Magnuson, K., & Waldfogel, J. (2016). Trends in income-related gaps in enrollment in early childhood education: 1968 to 2013. AERA Open, 2(2), 2332858416648933.
Majid, M. F. (2015). The persistent effects of in utero nutrition shocks over the life cycle: Evidence from Ramadan fasting. Journal of Development Economics, 117, 48–57. https://doi.org/10.1016/j.jdeveco.2015.06.006
Maluccio, J. A., Hoddinott, J., Behrman, J. R., Martorell, R., Quisumbing, A. R., & Stein, A. D. (2009). The impact of improving nutrition during early childhood on education among Guatemalan adults. The Economic Journal, 119(537), 734–763. https://doi.org/10.2139/ssrn.946107
Martorell, H., Adair, S., Richter, F., & Bhargava, & Biswas. (2010). Weight gain in the first two years of life is an important predictor of schooling outcomes in pooled analyses from five birth cohorts from low- and middle-income countries. The Journal of Nutrition, 140(2), 348–354. https://doi.org/10.3945/jn.109.112300
Meyers, M. K., Rosenbaum, D., Ruhm, C., & Waldfogel, J. (2004). Inequality in early childhood education and care: What do we know. In K. Neckerman (Ed.), Social inequality. (Vol. 223). New York: Russell Sage College.
Missoni, E., & Solimano, G. (2010). Towards universal health coverage: The Chilean experience. World Health Report.
OECD. (2016). OECD Income Distribution Database (IDD): Gini, poverty, income, methods and concepts. http://www.oecd.org/social/income-distribution-database.htm
OECD. (2019). Education at a glance 2019: OECD indicators. OECD. https://doi.org/10.1787/f8d7880d-en
Paxson, C., & Schady, N. (2007). Cognitive development among young children in Ecuador the roles of wealth, health, and parenting. Journal of Human Resources, 42(1), 49–84. https://doi.org/10.3368/jhr.xlii.1.49
Pollitt, E., Gorman, K. S., Engle, P. L., Martorell, R., Rivera, J., Wachs, T. D., & Scrimshaw, N. S. (1993). Early supplementary feeding and cognition: Effects over two decades. Monographs of the Society for Research in Child Development, 58(7), i–118. https://doi.org/10.2307/1166162
Reynolds, S. A., Andersen, C., Behrman, J., Singh, A., Stein, A. D., Benny, L., Crookston, B. T., Cueto, S., Dearden, K., & Georgiadis, A. (2017). Disparities in children’s vocabulary and height in relation to household wealth and parental schooling: A longitudinal study in four low-and middle-income countries. SSM-Population Health, 3, 767–786. https://doi.org/10.1016/j.ssmph.2017.08.008
Rubio-Codina, M., Attanasio, O., & Grantham-McGregor, S. (2016). Mediating pathways in the socio-economic gradient of child development: Evidence from children 6–42 months in Bogota. International Journal of Behavioral Development, 40(6), 483–491. https://doi.org/10.1177/0165025415626515
Rubio-Codina, M., Attanasio, O., Meghir, C., Varela, N., & Grantham-McGregor, S. (2015). The socioeconomic gradient of child development: Cross-sectional evidence from children 6–42 months in Bogota. Journal of Human Resources, 50(2), 464–483. https://doi.org/10.1920/wp.ifs.2014.1411
Samaniego, V. C. (2008). El Child Behavior Checklist: Su estandarización en población urbana argentina. Revista De Psicología, 4(8), 2008.
Schady, N. (2011). Parents’ education, mothers’ vocabulary, and cognitive development in early childhood: Longitudinal evidence from Ecuador. American Journal of Public Health, 101(12), 2299–2307. https://doi.org/10.2105/ajph.2011.300253
Schady, N., Behrman, J., Araujo, M. C., Azuero, R., Bernal, R., Bravo, D., Lopez-Boo, F., Macours, K., Marshall, D., & Paxson, C. (2014). Wealth gradients in early childhood cognitive development in five Latin American countries. The World Bank. https://doi.org/10.1596/1813-9450-6779
Schady, N., Behrman, J., Araujo, M. C., Azuero, R., Bernal, R., Bravo, D., Lopez-Boo, F., Macours, K., Marshall, D., Paxson, C., & Vakis, R. (2015). Wealth gradients in early childhood cognitive development in five Latin American countries. Journal of Human Resources, 50(2), 446–463. https://doi.org/10.3368/jhr.50.2.446
Schneiders, J. (2003). Neighbourhood socioeconomic disadvantage and behavioural problems from late childhood into early adolescence. Journal of Epidemiology & Community Health, 57(9), 699–703. https://doi.org/10.1136/jech.57.9.699
Schott, W., Aurino, E., Penny, M. E., & Behrman, J. R. (2017). Adolescent mothers’ anthropometrics and grandmothers’ schooling predict infant anthropometrics in Ethiopia. Annals of the New York Academy of Sciences. https://doi.org/10.1111/nyas.13455
Stein, A. D., Barros, F. C., Bhargava, S. K., Hao, W., Horta, B. L., Lee, N., Kuzawa, C. W., Martorell, R., Ramji, S., & Stein, A. (2013). Birth status, child growth, and adult outcomes in low-and middle-income countries. The Journal of Pediatrics, 163(6), 1740–1746. https://doi.org/10.1016/j.jpeds.2013.08.012
Stein, A. D., Lundeen, E. A., Martorell, R., Suchdev, P. S., Mehta, N. K., Richter, L. M., & Norris, S. A. (2016). Pubertal development and prepubertal height and weight jointly predict young adult height and body mass index in a prospective study in South Africa. The Journal of Nutrition, 146(7), 1394–1401. https://doi.org/10.3945/jn.116.231076
Stein, A. D., Wang, M., Martorell, R., Norris, S. A., Adair, L. S., Bas, I., Sachdev, H. S., Bhargava, S. K., Fall, C. H., & Gigante, D. P. (2010). Growth patterns in early childhood and final attained stature: Data from five birth cohorts from low-and middle-income countries. American Journal of Human Biology, 22(3), 353–359. https://doi.org/10.1002/ajhb.20998
Torche, F., & Echevarría, G. (2011). The effect of birthweight on childhood cognitive development in a middle-income country. International Journal of Epidemiology, 40(4), 1008–1018. https://doi.org/10.1093/ije/dyr030
Torres, A., Lopez Boo, F., Parra, V., Vazquez, C., Segura-Pérez, S., Cetin, Z., & Pérez-Escamilla, R. (2018). Chile Crece Contigo: Implementation, results, and scaling-up lessons. Child: Care, Health and Development, 44(1), 4–11. https://doi.org/10.1111/cch.12519
UNICEF. (2015). The Investment Case for Education and Equity. https://www.unicef.org/reports/investment-case-education-and-equity
UNICEF. (2019). The changing face of malnutrition. http://features.unicef.org/state-of-the-worlds-children-2019-nutrition/
Victora, C. G., Adair, L., Fall, C., Hallal, P. C., Martorell, R., Richter, L., Sachdev, H. S., & Group, M. and C. U. S. (2008). Maternal and child undernutrition: Consequences for adult health and human capital. The Lancet, 371(9609), 340–357. https://doi.org/10.1016/s0140-6736(07)61692-4
Viola, L., Garrido, G., & Rescorla, L. (2011). Testing multicultural robustness of the child behavior checklist in a national epidemiological sample in Uruguay. Journal of Abnormal Child Psychology, 39(6), 897. https://doi.org/10.1007/s10802-011-9500-z
Walker, S. P., Chang, S. M., Vera-Hernández, M., & Grantham-McGregor, S. (2011a). Early childhood stimulation benefits adult competence and reduces violent behavior. Pediatrics, 127(5), 849–857. https://doi.org/10.1542/peds.2010-2231
Walker, S. P., Wachs, T. D., Grantham-McGregor, S., Black, M. M., Nelson, C. A., Huffman, S. L., Baker-Henningham, H., Chang, S. M., Hamadani, J. D., & Lozoff, B. (2011b). Inequality in early childhood: Risk and protective factors for early child development. The Lancet, 378(9799), 1325–1338. https://doi.org/10.1016/s0140-6736(11)60555-2
Wechsler, D. (1955). Wechsler adult intelligence scale—. Archives of Clinical Neuropsychology
Weisz, J. R., Sigman, M., Weiss, B., & Mosk, J. (1993). Parent reports of behavioral and emotional problems among children in Kenya, Thailand, and the United States. Child Development, 64(1), 98–109. https://doi.org/10.1111/j.1467-8624.1993.tb02897.x
World Health Organization. (2006). WHO child growth standards: Length/height-for-age, weight-for-age, weight-for-length, weight-for-height and body mass index-for-age: Methods and development. World Health Organization. https://doi.org/10.1111/j.1651-2227.2006.tb02378.x
Funding
Dr. Behrman acknowledges funding provided by the Eunice Kennedy Shriver National Institute of Child Health and Human Development Grant NICHD R01HD065436 on "Early Child Development Programs: Effective Interventions for Human Development." Dr. Contreras thanks funding provided by the Center for Studies of Conflict and Social Cohesion (CONICYT/FONDAP/15130009) and the ANID – Millennium Science Initiative Program – Code: NCS17_015. Dr. Puentes thanks the funding of the ANID – Millennium Science Initiative Program – Code: NCS17_015.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors declare no conflict of interests or competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Behrman, J.R., Contreras, D., Palma, M.I. et al. Socioeconomic Disparities for Early Childhood Anthropometrics and Vocabulary and Socio-emotional Skills: Dynamic Evidence from Chilean Longitudinal Data. Popul Res Policy Rev 43, 3 (2024). https://doi.org/10.1007/s11113-023-09832-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1007/s11113-023-09832-9