
Abstract
The relationship between altitude of residence and child linear growth is studied using data for 630,499 children below age 5 years born between 1992 and 2016, as recorded in 47 countries at elevations ranging from − 377 to 4498 m above sea level. Regressions are used to measure the role of household, community, and environmental factors in explaining an observed altitude effect on linear growth. Controlling for birth year and country effects, and a range of factors correlated with altitude and associated with nutrition outcomes, for each 1000 m gain in elevation, height for age z score (HAZ) declines by 0.195 points on average. Country-specific estimates of the association vary and include positive associations. Results highlight the potential links between developmental risks for children and features of their physical environment.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Background and motivation
Despite sustained international efforts to eradicate child undernutrition, it remains the most common health risk among young children (Ahmed et al., 2012). In 2018, 149 million children under the age of 5 years worldwide were stunted and 49 million exhibited low weight for height (UNICEF, WHO, and World Bank Group, 2019). Understanding the importance of the physical environment in shaping a child’s nutrition, growth and development is important for geographically targeting public interventions and for assessing tradeoffs and synergies associated with interventions. Remote, high-altitude environments that are thinly populated by those living on the social and economic margins can present particular challenges for building infrastructure, providing health services, and improving agriculture.
Intriguingly, a number of country-specific studies have identified an apparent disadvantage for children living at high altitudes. The seemingly pernicious effect of altitude is not fully explained by basic agricultural conditions, poverty, or simple remoteness from markets and services. For example, altitude was found to be a significant predictor of linear growth at birth, 6 months, and 1 year for Bolivian children living at 3600 m above sea level (masl) compared to their counterparts living at 400 masl, and similar findings were later reported for a different Bolivian sample, as well as for children in the US mountain west and Tibet (Argnani et al., 2008; Dang et al., 2007; Greksa et al., 1985; Haas et al., 1982; Wang et al., 2016; Zahran et al., 2014). Studies from high-altitude areas in Argentina (Roman et al., 2015), and Ethiopia (Mohammed et al., 2020) have also found negative and statistically significant associations between altitude and linear growth, with children living beyond 2000 masl facing 28 percent greater odds of stunting, and children living at higher altitudes facing even greater risks.
At least three biological pathways could link altitude to growth: (i) chronic hypoxia, (ii) soil-determined mineral deficiencies in diets, and (iii) disease exposure. In the first case, evidence points to slowed growth during pregnancy due to hypoxia (Moore et al., 2011). Hypoxia has been shown to affect growth in models of mice (Farahani et al., 2007), perhaps because chronic constant hypoxia (CCH) and chronic intermittent hypoxia (CIH) produce different body and organ growth patterns. In CCH, changes to liver and kidney size are proportionate to body size, while heart, lungs, and brain are spared or increase in size vis-à-vis the body. Additionally, hypoxia impairs normal development in oxygen delivery tissues (Harrison et al., 2015), which suggests hypoxia-mediated regulation of growth may be an important aspect of development in all animals.
A second possible pathway is the link between the nutritional quality of foods and the nutrient profile of soils in which those foods are grown. For example, Gashu et al. (2021) find spatial variability in the micronutrient composition of staple cereal grains in Ethiopia and Malawi, with nutritionally important sub-national variation in calcium, iron, selenium, and zinc. Iron and zinc deficiencies, in particular, have been shown to be correlated with restricted linear growth (Bevis, 2015; Gibson et al., 2008; Prasad, 1991), and because the zinc content of a plant comes directly from the soil in which it grows, people who rely on their own agricultural production and consume limited amounts of animal protein may face risk of shortfalls (Mayer et al., 2007; Singh, 2009). Bevis et al. (2019) show that low-zinc soils are associated with elevated rates of stunting in Nepal, and Tessema et al. (2019) find that soil zinc is associated with serum zinc in children in Ethiopia. There is also a growing body of evidence that zinc deficiencies can hinder the absorption of iron, so that a zinc deficiency can contribute to an iron deficiency, which can also contribute to restricted linear growth (Graham et al., 2012). Some soils at high altitudes have been found to be deficient in zinc and iron (Andersen, 2007). If soils at lower altitudes have more iron and zinc than those at higher altitudes, children residing in subsistence households at higher elevations may exhibit higher rates of stunting due to lack of iron and zinc in their diets compared with those at lower elevations. To the extent soils at lower altitudes have higher concentrations of iron and zinc, access to market-provided food could reduce the risk of stunting and partly explain why wealth and income are commonly associated with reduced risk of stunting. If soils in areas isolated from markets are disproportionately prone to zinc deficiencies in ways that are systematically associated with elevation, this mechanism could drive outcomes. Furthermore, mineral soil deficiencies could be important at lower elevations. For example, a recent review placed zinc atop the list of micronutrients that are deficient in arable soils in sub-Saharan Africa, with boron, iron, molybdenum, and copper deficiencies also common (Kihara et al., 2020).
Drawing a connection between altitude and growth in the context of disease risk presents a challenge. Malaria has long-been associated with child stunting (Sharp & Harvey, 1980), and some characteristics of cropping systems are known to exacerbate malarial risk among highland populations (Lindsay & Martens, 1998). However, malaria prevalence and transmission tend to decrease seasonally at high altitudes due to lower temperatures and humidity (Attenborough et al., 1997; Bødker et al., 2003). Evidence regarding potential pathways connecting elevation, other vector-borne diseases, and stunting remains even less clear.
For each of the pathways identified above, potential confounders with the altitude-growth relationship clearly arise. At the most basic level, Stinson (1982) found no growth differences between affluent high-altitude Bolivian children and affluent low-altitude Guatemalan children, which suggest that socioeconomic factors can mediate the altitude-stunting relationship. Mortality rates have been shown to be higher in high-altitude ecological zones of Nepal than at lower elevations, but considerably higher among low-wealth populations (Chin et al., 2011). Similarly, increased mortality rates in high-altitude populations have been measured in Peru (Mazess, 1965), Bolivia (Keyes et al., 2003), and India (Wiley, 1994). Better access to maternal and health services and food markets among the better-off may contribute to these patterns (Chikhungu et al., 2014; Hotchkiss, 2001). Among household-level factors that strongly vary with altitude, maternal education stands out as a particularly important predictor of linear growth (Bicego & Boerma, 1993; Boyle et al., 2006; Semba et al., 2008). Community-level economic status modifies the role of household-level socioeconomic status, which suggests improvements in access to basic community resources may contribute to individual child health (Fotso & Kuate-Defo, 2005; Stinson, 1982). Work from Nepal supports this conjecture. A number of studies find that height for age z scores (HAZ) and stunting rates have improved for children below age 5 since 2000, but gains have been largest for children from wealthier and more educated households (Budhathoki et al., 2020; Dorsey et al., 2018; Hanley-Cook et al., 2020; Nepali et al., 2019; Shively, et al., 2020). Characteristics of children and households explain most of the variance in HAZ and weight for height z scores (WHZ) in Nepal, with relatively smaller but statistically significant contributions from community-level factors (Smith & Shively, 2019).
Informed by these past findings, our goals in this article are to (1) test the hypothesis that altitude (elevation) of residence is, on average, negatively associated with child linear growth; (2) measure the extent to which various child-, household-, and community-level characteristics mitigate this relationship; and (3) report the extent to which the altitude-HAZ relationship varies across countries. We study altitude and linear growth in as large a sample as is currently available, controlling for as many potential confounders as possible. Although our results do not establish a causal link between altitude, biological drivers, and early child growth, they do provide the strongest evidence to date of a link and underscore the need for additional research and policy attention on hidden biological and environmental drivers of stunting.
Methods
We use regression models to study patterns of long-term linear growth attainment in children age 5 years and below, as measured by height for age z score (HAZ). We combine data from multiple sources, starting with Demographic and Health Surveys, and isolate the correlation between altitude and HAZ by controlling for observable factors that are themselves likely to be correlated with altitude and child growth. Conceptually, HAZ is reflective of numerous factors, some of which (e.g., agronomic potential, household wealth, economic conditions, access to markets) may be fixed throughout early life and some of which (e.g., temperature, rainfall, disease exposure) may vary over time (Brown et al., 2014). For both short-term and long-term nutrition indicators, timing of exposure to shocks may matter. For example, in a study of 30 countries in sub-Saharan Africa, Baker and Anttila-Hughes (2020) find that lifetime-scale effects largely explain observed negative relationships between child weight and temperature. Using DHS data from Ethiopia, Randell et al. (2020) find that greater rainfall during rainy seasons in early life is associated with greater HAZ, and that higher temperatures during the first and third trimesters of pregnancy are positively associated with subsequent stunting. Similarly, using DHS data from 16 countries in sub-Saharan Africa, Thiede and Strube (2020) find high temperatures and low precipitation are associated with low child weight, and that high temperatures increase risk of wasting. Omiat and Shively (2020) focus on agriculture and disease as potential causal pathways for such effects, finding positive and significant associations between crop yields and WHZ in Uganda, as well as strong correlations between excess rainfall and contemporaneous diarrhea incidence. Below, we attempt to minimize the influence of such possible time-varying effects by focusing on HAZ as an outcome, rather than WHZ, and by accounting for temporal markers including child age, birth year and month, and household time in residence.
Data sources and key measurements
Demographic and health surveys
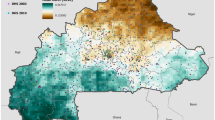
Data used in the analysis come from public sources. The primary source is a series of Demographic and Health Surveys (DHS; www.measuredhs.com) conducted between 2003 and 2016 across 47 countries in Africa, Southeast Asia, Eastern Europe, and Latin America. Figure 1 maps geographic coverage of the surveys, which constitute the current subset of available DHS surveys for which reliable measures of altitude are available. All country-year combinations included in the dataset are listed in Appendix Table 5. Descriptive statistics for all variables are reported for the full sample in Table 1 and by continent in Appendix Table 6.

Map of world indicating data coverage (n = 630,499; 47 countries)
Each country provides between one and three survey years in the timespan covered. Each DHS is a nationally representative household survey and includes anthropometric data, information on household health, sanitation, and demographic conditions, and a community-level measure of altitude. The DHS surveys provide the primary data on child growth and child and household characteristics. DHS data are typically collected by trained enumerators under the supervision of a relevant government ministry, such as the Ministry of Health or Bureau of Statistics. Surveys are comprehensive and nationally representative household surveys focusing on men aged 15–59, women aged 15–59, and children under age 5. Most DHS samples are selected using a stratified two-stage cluster design and provide key health measurements and indicators across relevant geographic and political zones. DHS data are georeferenced, but to protect confidentiality of respondents, data from the same enumeration area are aggregated to a single point and the coordinate is masked using a displacement process. Urban clusters are displaced up to 2 km, and rural clusters are displaced up to 5 km, with a randomly selected 1% of rural clusters displaced up to 10 km (Burgert, et al., 2013).
DHS surveys do not define urban–rural locations. Instead, they adopt designations made by national governments and their statistical agencies. For this reason, the way the urban indicator is assigned to households in the DHS varies somewhat across countries. In some cases, the designation is population based, and in some cases, it is based on political or other criteria. The International Labor Office maintains a database (ILO, 2015) describing how various countries define urban areas.
Our observations constitute a pooled cross-section of 630,499 children under 5 years of age born between 1992 and 2016 and measured in a specific survey at a specific point in time. Our outcome variable is height for age z score (HAZ), a standard measure of long-term nutritional status in children, calculated by comparing a child’s linear growth attainment at a particular age to the median for that age-sex cohort in the WHO reference population (WHO, 1995, 2006), normalizing by the standard deviation of the reference population. We use as our dependent variable the continuous measure of HAZ, rather than a binary, below-threshold, indicator, because we expect the relationship between altitude and linear growth to be potentially nonlinear and mediated through other continuous variables.
We account for birth year and several individual- and household-level factors reported in the DHS, including duration of residence at the household’s location, the sex of the head of the household, and several variables capturing aspects of healthcare utilization. The DHS provides measures of maternal education and mother’s BMI. Maternal education can affect childhood health and nutrition directly. It also reflects parental background and earning potential. Similarly, a mother’s BMI is a direct measure of her health, and to the extent BMI reflects household food availability, dietary diversity, sanitation, or disease burden, including her BMI in a child-level regression controls for these factors that we cannot observe directly. We also include an indicator of household electrification and a household wealth quintile index constructed for each DHS survey by matching observed household assets to an imputed wealth level (Filmer & Prichett, 2001). Although the underlying wealth index cannot be reliably compared across countries, since each is constructed within a specific country sample, its inclusion in regressions in the form of a relative quintile ranking does allow us to account for relative differences in economic status. Additional child-specific variables used in the regressions include age (in months), binary indicators of vitamin A supplementation, recent vaccinations, current breastfeeding status, recent fever and recent diarrhea (both within the past 14 days), mother’s height, and—in a sub-sample of observations—indicators for a child’s dietary diversity based on 7-day food recall and fuel source as a proxy for indoor air quality.
We rely on the DHS-reported measurement of altitude (elevation in masl), which is available for each survey cluster. This provides a reliable estimate of the altitude a child experiences because these clusters (i.e., small enumeration units roughly comparable to a community) are sufficiently small that it is unlikely that a household’s altitude would deviate markedly from the community value. The average altitude of residence in the sample is 549 masl (std. dev. = 644; min = − 377; max = 4498). Approximately 4% of observations are at elevations above 2000 masl and 1% are above 3000 masl.
Although a large body of published research has established the reliability of the DHS data, a few anomalies were detected at altitude extremes (greater than 4500 masl). Some of these high-altitude observations correspond to latitude and longitude pairs that mapped to uninhabitable locations during the initial inspection of the data and were therefore removed (236 observations in total). Reported altitude was also checked against the highest recorded elevation in each country (CIA, 2020); recorded altitude for 24 observations from the same cluster in Nigeria exceeded Nigeria’s maximum elevation, and these were therefore dropped from the sample.
Geographic Information Systems data
To separate the influence of altitude from that of other potentially confounding location-and environment-specific variables, we include non-DHS data corresponding to rainfall, temperature, the normalized difference vegetation index (NDVI), length of growing period, local population density, household electrification, and average intensity of nighttime light radiation and its square. Temperature, rainfall, NDVI, and length of growing period all account for important aspects of agricultural growing conditions and, hence, potential food security of the household. These variables are taken from Geographic Information System’s (GIS) sources and compiled as part of the Advancing Research on Nutrition and Agriculture (ARENA) project (https://www.ifpri.org/project/advancing-research-nutrition-and-agriculture-arena) conducted at the International Food Policy Research Institute (IFPRI). GIS data were merged with the DHS datasets in a way that assures the closest possible spatial and temporal overlap with the DHS.
Nighttime light radiation images are collected by the US Air Force Weather Agency and processed at the National Geophysical Data Centre (NGDC) of the National Ocean and Atmosphere Administration (NOAA) using Defense Meteorological Satellite Program (DMSP) Operational Linescan System (OLS). Version 4 DMSP/OLS night-time image products from 1992 to 2013 (30 arc seconds spatial resolution; available at http://www.ngdc.noaa.gov/dmsp/downloadV4composites.html) were used. DMSP operates satellites in sun-synchronous orbits with nighttime overpasses at 8–10 p.m. local time. Each OLS instrument generates a complete coverage of nighttime light data in a 24-h period (Elvidge et al., 2001, 2009). Data were merged by country, DHS cluster number, and child birth year. Available GIS data do not contain data for 2014 to 2016; the value from 2013 was used for missing years. More than half of all observations from 2014 to 2016 are found in 2014, and the year-to-year changes in values are sufficiently small that inaccuracies arising from the matching procedure are likely to be extremely minor.
Length of growing period is collected by the Agro-Ecological Zones project by the Food and Agriculture Organization (FAO, 2002). The variable is defined as the period (in days) during a year when precipitation exceeds half the potential evapotranspiration (FAO, 1978). Values corresponding to individual 5 arc-minute grid cells were merged with the DHS data by country, cluster number, and the year corresponding to the end of the DHS survey period.
Normalized Difference Vegetation Index (NDVI) is referred to as the continuity index to the existing National Oceanic and Atmospheric Administration-Advanced Very High Resolution Radiometer (NOAA-AVHRR) derived NDVI (Didan, 2015). NDVI effectively characterizes the global range of vegetation states and processes, i.e., “greenness” at the Earth’s surface as observed from space. Higher values of the index observed for a location indicate more intense vegetative cover than lower values. The spatial resolution of AVHRR on NOAA satellites is effectively 3 × 5 km for most global locations. NDVI values were merged with the DHS data by country, cluster number, and the year corresponding to the end of the DHS survey period.
Average rainfall comes from the Climatic Research Unit Time Series (CRU TS) of data sets (NCARS, 2017). The rainfall variable used is the average of annual totals from 1901 to 2015 for each DHS cluster. Temperature comes from the WorldClim version 2 data sets (Fick & Hijmans, 2017). Temperature is calculated as the average over all days from 1970 to 2000 for the DHS cluster. Rainfall and temperature were merged with the DHS data by country, cluster number, and the year corresponding to the end of the corresponding DHS survey period.
Nighttime lights, population density, and electrification are useful proxies for a constellation of features associated with isolation and the built environment (Doll et al., 2000; Elvidge et al., 1997; Zhao et al., 2016). Accounting for isolation separate from altitude may be particularly important because infrastructure development supports food security and other factors important for child health and growth. For example, Shively (2017) finds that infrastructure reduces children’s vulnerability to negative rainfall shocks, and Shively and Thapa (2016) find that transportation linkages moderate both the level and volatility of food prices, which matter for food security and dietary quality. To the extent altitude’s role might operate through restrictions on agricultural potential, controlling for these variables in our regressions should increase the accuracy of the estimate of altitude’s association with child growth independent of the negative influence of altitude on food production.
Study limitations
Some factors considered fixed by location could vary by time if, for example, short-term factors such as environmental shocks cause households to migrate. To the extent migration decisions systematically coincide with birth timing, HAZ data could reflect spatial sorting of children. In some countries, internal migration tends to flow from high to low altitudes. As a result, our estimates regarding altitude could depend on factors other than those we observe if children born at high altitudes to non-migrating mothers are systematically advantaged or disadvantaged compared to children born at lower altitudes. Available data do not allow us to directly control for household migration decisions or test for correlations. However, as a check we present results for an auxiliary regression that accounts for household duration in residence.
Another potential confounding factor in the chain connecting altitude to HAZ is indoor air quality. Evidence from Bangladesh (Hong et al., 2006) and India (Mishra & Retherford, 2007) shows that use of low-quality heating and cooking fuels is strongly associated with stunting risk and that children living at higher altitudes face greater exposure to smoke and respiratory illness (due to both greater heating needs and poverty-induced use of lower-quality fuels). Although an insufficient proportion of our sample includes information on cooking fuel to allow inclusion of proxies for indoor air quality in all reported regressions, we do report results for a sub-sample as a check of the impact of this measure on our estimates of altitude effects.
Finally, although we account for several drivers of agricultural production and health, we cannot fully eliminate transitory environmental shocks (e.g., rainfall, temperature), crop diversity, or diet patterns as explanations of differences in HAZ across altitudes. We believe the inclusion of rainfall, NDVI, and length of growing period account for a large proportion of the variance in underlying agricultural potential and crop diversity. Including maternal BMI in our models also captures a substantial component of underlying household food access and health, since mother’s BMI and child HAZ are likely to be sensitive to food entitlements and health shocks in similar ways. To test for the possible relationship between agricultural or dietary diversity, we estimate regressions with a sub-set of our data for which indicators of dietary diversity were reported. This does not rule out potential dietary differences as an unobserved confounder in our full sample, but it is not obvious that diets should matter more at some altitudes than others, or that unobserved variation in diets could fully account for patterns observed.
Results
Descriptive statistics
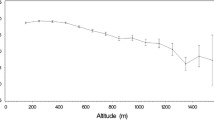
We use a pooled dataset combining children from all 47 countries and all 25 birth years. Each survey reflects substantial variation in HAZ values (Fig. 2) and in altitude (Fig. 3). We summarize the bivariate relationship between altitude and HAZ in Figs. 4 and 5. In Fig. 4, average values of HAZ, grouped by ten values of altitude, are plotted against a local polynomial regression of HAZ on altitude. In Fig. 5, the solid line also represents a local polynomial regression of HAZ on altitude, but to illustrate the basic relationship between altitude and HAZ for specific countries, as well as the highest altitudes recorded in each country, the scatter points in Fig. 5 plot the median HAZ for each country against the maximum altitude recorded in each country. Figures 4 and 5 illustrate the unconditional relationship between altitude and HAZ. They clearly suggest a negative relationship, but show that HAZ is by no means determined by altitude. Regressions reported below are designed to isolate as much as possible the independent contribution of altitude to HAZ by controlling for factors associated with place of residence.

Distribution of height for age z score, by country. Figure 2 graphically depicts HAZ quartile values in each country (n = 47). Open circles indicate median HAZ values for each country. Ticks represent the lower (left) and upper (right) adjacent values; the edges of the shaded boxes represent the 25th (left) and 75th (right) percentiles. Outside values excluded from the figure

Distribution of altitude, by country. Figure 3 graphically depicts altitude quartile values in each country (n = 47). Open circles indicate median altitude for each country. Ticks represent the lower (left) and upper (right) adjacent values; the edges of the shaded boxes represent the 25th (left) and 75th (right) percentiles. Outside values excluded from the figure

Altitude and height for age z scores (by altitude groupings). Figure 4 illustrates the bivariate relationship between altitude and HAZ in the sample. The solid line represents a local polynomial regression of HAZ on altitude, constructed with Epanechnikov kernel and bandwidth of 750 (n = 630,499). The shaded area represents the 95% confidence band for the estimate. Scatter points display the mean HAZ for each of ten groupings of altitude values

Altitude and height for age z scores (country medians scatter plot). Figure 5 illustrates the bivariate relationship between altitude and HAZ in the sample. The solid line represents a local polynomial regression of HAZ on altitude, constructed with Epanechnikov kernel and bandwidth of 750 (n = 630,499). The shaded area represents the 95% confidence band for the estimate. Scatter points display the median HAZ for each country plotted against the maximum altitude recorded in each country (n = 47). For convenience when generating the scatter plot, markers for eight countries with a comparatively high median HAZ have been suppressed. These are Albania (median HAZ = − 0.65), Armenia (− 0.30), Colombia (− 0.85), the Dominican Republic (− 0.50), Jordan (− 0.61), Kyrgyz Republic (− 0.87), Moldova (− 0.33), and Morocco (− 0.89)
Regression results
We begin by fitting a baseline model of HAZ as a function of altitude, which enters linearly. We then sequentially add sets of variables that could be expected to account for the HAZ-altitude relationship (Table 2). All main regressions employ fixed effects for country, the child’s birth year, and country crossed with birth year. Regressions are unweighted. To adjust for the possibility that the HAZ residuals may be correlated within sampled locations, all standard errors are clustered at the level of the DHS sample unit. Model 1 includes altitude only. This establishes the basic finding of interest, namely, a negative association between altitude and HAZ. Adding child-level variables in Model 2 does not impact the negative relationship.
Model 3 adds to Model 2 a set of maternal and household-level variables. Key variables of the mother (height, female headship, education, breastfeeding, and BMI) display strong individual and joint significance (F[5,71202] = 3869.70; p = 0.0000). Children who have taller mothers with more education and higher BMI are likely to have higher HAZ. Rural children have significantly lower HAZ than urban children, although the difference (0.02 z score) is negligible. Relative wealth rankings are strongly associated with HAZ in the sample, with each step up to a higher quintile associated with a 0.07- to 0.13-point increase in HAZ. The largest incremental increase comes from moving from the 4th to 5th (top) quintiles, and the overall HAZ gap between children in the top and bottom quintiles is nearly half a standard deviation. In Model 3, coefficients for vitamin A and vaccinations are reversed from Model 2, and negative. One interpretation is that the indicators are collinear with mother’s education (excluded from Model 2) and their negative associations with HAZ reflect a pattern in which low HAZ children are more likely to visit clinics due to illness and receive supplementation and vaccination as a result.
Model 4 adds to Model 3 location-specific variables that drive or account for economic development (nighttime light radiation, population density) or agricultural conditions (NDVI, temperature, rainfall, length of growing period). Most are correlated with HAZ at standard significance levels. HAZ increases with nighttime lights, suggesting the overall intensity of local economic activity is positively associated with HAZ, albeit at a diminishing rate. The positive coefficients for rainfall and length of growing period suggest beneficial conditions for crops are likely beneficial for child growth via agricultural production and food security. Higher temperatures and higher NDVI values, in contrast, are negatively associated with HAZ. After accounting for these additional variables, the estimated coefficient for altitude strengthens in magnitude and retains its statistical significance. In terms of magnitude, a 1000-m increase in altitude more than offsets the HAZ gain associated with belonging in the fourth wealth quintile rather than the lowest (for example, the coefficient on altitude is − 0.195 in Model 4, whereas the coefficient for the fourth wealth quintile relative to the lowest quintile is 0.209).
The insensitivity of the altitude coefficient to inclusion of household variables (Model 3) and location-specific economic and environmental variables (Model 4) is the key finding in this series of models, but leaves open whether the relationship might be accounted for by additional child or environmental factors. To address this conjecture, three auxiliary regressions (models 5–7) are reported in Table 3. These provide robustness checks for the main regression results. In addition, the possibility of non-linear altitude effects is explored via Model 8 in Table 4.
Model 5 reports results for a regression that accounts for child dietary diversity via a dietary diversity score. This score is available for a subset of the sample (360,396 observations, 57% of the full sample). Results for dietary diversity are as expected: more diverse diets are associated with better linear growth outcomes. However, the inclusion of this variable does not alter the HAZ-altitude relationship or diminish the magnitude of the estimated correlation.
Model 6 reports results for a regression that includes an indicator for the source of household cooking fuel. This variable is available for a sub-sample of 340,732 observations (54% of the full sample). The type of cooking fuel is a proxy for smoke exposure, since improved cooking fuels (gas or electric) are associated with less smoke exposure than biomass-based fuels. Improved fuels are less widely used at higher altitudes and are at the same time associated with fewer negative child health effects, such as upper respiratory infections. Results for indoor air quality are as expected: use of an improved fuel source is associated with better linear growth outcomes. At the same time, inclusion of fuel source does not account for the altitude relationship or diminish the magnitude or significance of the HAZ-altitude correlation.
The last auxiliary regression reported, Model 7, includes time (duration) in residence at the household’s current location. This regression uses 460,892 observations (roughly three-quarters of the full sample) and aims to account for possible unobserved time-varying factors, including cumulative environmental shocks. The full dataset does not support the inclusion of both the duration variable and country-year fixed effects and Model 7 excludes country × year effects. Patterns of results from this auxiliary regression are consistent with the other reported models in terms of signs, magnitudes, and statistical significance of estimated coefficients.
In Table 4, results from Model 4 are compared with those from Model 8, in which we allow the strength of the HAZ-altitude relationship to vary across altitude levels. In this specification, we interact altitude with binary variables taking the value of 1 if altitude falls below 1000 masl, between 1000 and 2000 masl, between 2000 and 3000 masl, or above 3000 masl. This allows the altitude slope to differ across these ranges, picking up any potential non-linearities in the altitude-HAZ relationship. Results from this regression show that each step up to a higher altitude category is associated with a comparatively lower HAZ value—up through 3000 masl, with a slight moderation in the impact beyond 3000 masl. The slopes in the highest altitude categories are more strongly negative compared with both lower altitudes and the average linear effect imposed in earlier models. A Wald test confirms that point estimates on altitude are jointly significant (F[4,71202] = 103.86; p = 0.0000). In paired tests, altitude estimates for sub-samples above 2000 masl are significantly different from those for sub-samples below 2000 masl, suggesting a stronger association with altitude for children at the highest elevations.
Discussion
To put into context our finding of an overall average negative relationship between altitude and linear growth, it is important to note that many factors beyond environment and location influence nutrition and health. The 2008 and 2013 Lancet reviews on maternal and child nutrition underscore the importance of breastfeeding and adequate vitamin intake (Horton, 2008; Horton & Lo, 2013). Access to safe water, sanitation, and health information and facilities is important (Lavy et al., 1996), especially because immature gut biota and subclinical enteropathy may be causal factors in undernutrition (Blanton, 2016; Humphrey, 2009). Other contributing exposures to impaired growth and mortality include poor indoor air quality and maternal tobacco smoking (Fullerton et al., 2008; Gani, 2015; Kyu et al., 2009), aflatoxin exposure (Khlangwiset et al., 2011), and war, civil unrest, and drought (Alderman et al., 2006). Agricultural capacity, diversity, and performance may be especially important to nutrition where households pursue self-provisioning strategies or are poorly integrated into markets (IFAD, 2014). Positive associations have been found between nutrition outcomes and both crop diversity and specific farm practices, such as production of animal protein or fruits and vegetables (Arimond & Ruel, 2004; Shively & Sununtnasuk, 2015). In addition, because agricultural production is highly sensitive to rainfall and temperature, nutrition outcomes often track environmental variability (Brown et al., 2009; Grace et al., 2014), as demonstrated by mortality effects associated with season of birth. These have been found in The Gambia (Moore et al., 1997), India (Lokshin & Radyakin, 2012), Indonesia (Cornwell & Inder, 2015; Maccini & Yang, 2009), Mexico (Skoufias & Vinha, 2011), Nigeria (Rabassa et al., 2012), and Vietnam (Thai & Falaris, 2014). Environmental conditions potentially influence nutrition via multiple indirect pathways, including food prices (Anriquez et al., 2013; Bouis, 2008; Grace et al., 2014; Thomas & Strauss, 1992) and market access (Gómez & Ricketts, 2013; Minten, 1999), which have only been partially or indirectly accounted for in this study.
In our pooled sample of 630,499 children from 47 countries, altitude maintains a significant and negative relationship with HAZ, on average, that is consistent in magnitude across all specifications and robustness checks. Notably, our sample excludes children from Argentina, Bolivia, the USA, and Tibet—locations where previous research has demonstrated a negative altitude-growth association. Considering the findings, a reasonable conjecture might be that the local intensity of economic activity drives these patterns. The level of nighttime light radiation—an imperfect but widely used proxy for local economic activity (Doll et al., 2000)—is strongly and negatively correlated with altitude in our sample. On average, a one percent increase in altitude is associated with a 0.7% reduction in the nighttime light value and, as the results of Model 4 demonstrate, nighttime lights are positively correlated with child linear growth. Figure 6 demonstrates that gains in linear growth associated with higher rates of economic activity are especially pronounced at low nighttime light levels and flatten out at high levels, exhibiting a pattern similar to Preston’s curves for per capita income and life expectancy (Preston, 1975) and curves for district-level indices of human development and HAZ reported for Uganda (Shively, 2017). Whether altitude independently contributes to child growth or simply serves as a proxy for differences in underlying patterns of economic development has obvious relevance for targeting policy and project interventions. For example, using data from Nepal, a country with a substantial number of children living at high altitudes, Shively et al. (2020) find that household wealth and maternal BMI mitigate the altitude-HAZ relationship. Our confidence that altitude signals underlying drivers in a child’s linear growth is buttressed by our large sample and ability to control for various location-specific confounders that might explain away the observed correlation. The negative association holds both in the set of high-altitude countries (i.e. those with children observed at elevations in excess of 3000 masl, namely, Colombia, Ethiopia, Guatemala, India, Kenya, Kyrgyz Republic, Lesotho, Nepal, and Peru) and in a large sub-set of low-altitude (primarily West African) countries (i.e., those with samples containing only children observed at elevations below 1000 masl, among them Cote d’Ivoire, Ghana, Mali, Senegal, and Togo). This points to the possibility that hypoxia could be a driver at extremely high altitudes, with other pathways, including disease exposure or soil mineral deficiencies, operating at lower altitudes.

Nighttime light radiation index and height for age (HAZ) z scores. Figure 6 displays the bivariate relationship between initial development conditions in the sample, measured as the level of nighttime light radiation observed in the year of the child’s birth, and subsequent linear growth, measured as the height for age z score (HAZ). The solid line represents a local polynomial regression of HAZ on nighttime light radiation, constructed with an Epanechnikov kernel (n = 630,499). The shaded area represents the 95% confidence band for the regression estimate. Circles indicate country-level, unweighted means. Circle sizes are proportional to the country’s population of children below age 5 years in the most recent year of the DHS survey included in the sample. For convenience in building the figure, three countries have been omitted from the scatter plot. These are Moldova (mean light value = 11.81; mean HAZ = − 0.19), Dominican Republic (21.01; − 0.35), and Jordan (30.72; − 0.53). Data for these countries are included when constructing the local polynomial regression
On average, after controlling for potential confounders, for each 1000 m gain in altitude, HAZ falls by approximately 0.195 points. In the context of our sample, this represents roughly a 0.80-point difference in HAZ between children residing at sea level and those at 4000 m (of which there are more than 1000 in the sample). However, as alluded to above, this average effect masks some important differences across countries. In order to compare countries, and thereby aid in the interpretation of these results, Fig. 7 displays the regression-adjusted estimated altitude coefficients for each country. These were obtained via 47 country-specific regressions, using the variable specification of Model 4 but omitting (by necessity) country and country × birth year fixed effects. For 20 countries, the altitude coefficient is positive, although significantly different from zero in only 2 instances. In contrast, for 27 countries, the measured association is negative, ranging from − 1.38 (Moldova) to − 0.04 (Namibia). For 15 of these countries, the negative coefficient is significantly different from zero.
In part, the patterns observed could be driven by disease exposure. Malaria, which has long-been associated with child stunting (Sharp & Harvey, 1980), could help to explain some of the country-specific associations between altitude and HAZ shown in Fig. 7. Unobserved factors could include disease prevalence, limited access to healthcare resources, and low immunity in isolated communities. More fundamentally, modest gains in altitude in some low-altitude settings may reduce exposure risk to malaria and other easily communicable diseases, and may contribute to the observed positive altitude-HAZ relationship exhibited in low-altitude countries with high malarial risk (e.g., Bangladesh, Benin, Burkina Faso, Gabon, and Sierra Leone). However, it is important to note that the regressions included controls for presence of fever and diarrhea (for the 14 days preceding anthropometric measurement). Inclusion of a control for household fuel source also helps to account for smoke-exacerbated upper respiratory infections. That unobserved aspects of disease could account for the entire negative correlation between altitude and HAZ seems unlikely. Of the factors unexplored directly in this analysis, soil mineral content seems especially important as a topic for further study.

Adjusted country-specific altitude coefficient estimates. Figure 7 displays the regression-adjusted estimated altitude coefficients for each country (n = 47). Estimated coefficient values (open circles) were obtained via 47 country-specific regressions, using the variable specification of Model 4 (Table 4), omitting country- and country-year fixed effects. Gray bands represent the 95% confidence intervals for the estimated coefficients
Conclusion
The relationship between altitude and child growth was investigated using data from 47 countries, evaluating the extent to which other factors, particularly health attributes of child and mother, household resources, and location-specific characteristics mediate or explain away the observed negative relationship. The finding regarding negative effects of altitude on child growth appears to be highly robust to the inclusion of potential confounding variables that are themselves correlated with poverty and economic isolation. Altitude effects are robust to the inclusion of controls for relative wealth and the characteristics of mothers, including her height, BMI, and education. A range of place-based factors, including nighttime lights, length of growing periods, population density, normalized difference of vegetation, average rainfall, and average temperature, are positively associated with child linear growth, underscoring the importance of general patterns of economic development, rural electrification, and agricultural capacity for health and nutrition outcomes.
When running the most comprehensive country-specific regression models, we observe that among the 17 altitude coefficient estimates that are statistically different from zero, only 2 are positive and 15 are negative. These negative associations are observed across three continents, suggesting the HAZ-altitude relationship is not restricted to particular global regions. Results also suggest the pernicious effect of altitude may intensify above 2000 masl. The robustness of this HAZ-altitude relationship suggests a need for deeper investigation into the sources of the observed associations, whether arising from the connection between altitude, soil minerals, and dietary deficiencies, or other hidden health pathways. Keeping in mind the formidable economic and logistical challenges associated with reaching remote populations, nutrition interventions targeted at those living at high altitudes nevertheless may be warranted, as these children appear to exhibit more restricted linear growth than those at lower altitudes.
Availability of data and material
All data used in the analysis come from public sources. Data for replication are permanently archived in the Interuniversity Consortium for Political and Social Research (ICPSR) data repository (https://doi.org/10.3886/E144841V1).
Code availability
All Stata code necessary to replicate the results of this paper is available upon request and also permanently archived along with the data in the Interuniversity Consortium for Political and Social Research (ICPSR) data repository (https://doi.org/10.3886/E144841V1).
References
Ahmed, T., Hossain, T., & Sanin, K. I. (2012). Global burden of maternal and child undernutrition and micronutrient deficiencies. Annals of Nutrition and Metabolism, 61(1), 8–17.
Alderman, H., Hoddinott, J., & Kinsey, B. (2006). Long term consequences of early childhood malnutrition. Oxford Economic Papers, 58(3), 450–474.
Andersen, P. (2007). A review of micronutrient problems in the cultivated soil of Nepal. Mountain Research and Development, 27, 331–335.
Anriquez, G., Daidone, S., & Mane, E. (2013). Rising food prices and undernourishment: A cross-country inquiry. Food Policy, 38, 190–202.
Arimond, M., & Ruel, M. T. (2004). Dietary diversity is associated with child nutritional status: Evidence from 11 demographic and health surveys. Journal of Nutrition, 134(1), 2579–2585.
Argnani, L., Cogo, A., & Gualdi-Russo, E. (2008). Growth and nutritional status of Tibetan children at high altitude. Collegium Anthropologicum, 32, 807–812.
Attenborough, R. D., Burkot, T. R., & Gardner, D. S. (1997). Altitude and the risk of bites from mosquitoes infected with malaria and filariasis among the Mianmin people of Papua New Guinea. Transactions of the Royal Society of Tropical Medicine and Hygiene, 91, 8–10.
Baker, R. E., & Anttila-Hughes, J. (2020). Characterizing the contribution of high temperatures to child undernourishment in Sub-Saharan Africa. Scientific Reports, 10, 18796. https://doi.org/10.1038/s41598-020-74942-9
Bevis, L., Kim, K., Guerena, D. (2019). Soils and South Asian stunting: Low soil zinc availability drives child stunting in Nepal. Working Paper.
Bevis, L. (2015). Soil-to-human mineral transmission with an emphasis on zinc, selenium, and iodine. Springer Science Reviews, 3, 77–96.
Bicego, G. T., & Boerma, J. T. (1993). Maternal education and child survival: A comparative study of survey data from 17 countries. Social Science and Medicine, 36, 1207–1227.
Blanton, L. V., et al. (2016). Gut bacteria that prevent growth impairments transmitted by microbiota from malnourished children. Science, 351(6275), 3311–3317.
Bødker, R., Akida, J., Shayo, D., Kisinza, W., Msangeni, H. A., Pedersen, E. M., & Lindsay, S. W. (2003). Relationship between altitude and intensity of malaria transmission in the Usambara Mountains, Tanzania. Journal of Medical Entomology, 40, 706–717.
Bouis, H. (2008). Rising food prices will result in severe declines in mineral and vitamin intakes of the poor. Harvest Plus.
Boyle, M. H., Racine, Y., Georgiades, K., et al. (2006). The influence of economic development level, household wealth and maternal education on child health in developing world. Social Science and Medicine, 63, 2242–2254.
Brown, M., Grace, K., Shively, G., Johnson, K., & Carroll, M. (2014). Using satellite remote sensing and household survey data to assess human health and nutrition response to environmental change. Population and Environment, 36(1), 48–72.
Brown, M., Hintermann, B., & Higgins, N. (2009). Markets, climate change and food security in West Africa. Environment, Science and Technology, 43, 8016–8020.
Budhathoki, S. S., Bhandari, A., Gurung, R., et al. (2020). Stunting among under 5-year-olds in Nepal: Trends and risk factors. Maternal and Child Health Journal, 24, 39–47.
Burgert, C.R., Colston, J., Roy, T., Zachary, B. (2013). Geographic displacement procedure and georeferenced data release policy for the demographic and health surveys. DHS Spatial Analysis Report No. 7 (ICF International, Calverton, MD).
Chikhungu, L. C., Madise, N. J., & Padmada, S. S. (2014). How important are community characteristics in influencing children’s nutritional status? Evidence from Malawi population–based household and community surveys. Health and Place, 30, 187–195.
Chin, B., Montana, L., & Basagana, X. (2011). Spatial modeling of geographic inequalities in child mortality across Nepal. Health and Place, 17, 929–936.
Cornwell, K., & Inder, B. (2015). Child health and rainfall in early life. Journal of Development Studies, 51, 865–880.
CIA. (2020). The World Factbook 2020. Central Intelligence Agency.
Dang, S., Yan, H., & Yamamoto, S. (2007). High altitude and early childhood growth retardation: New evidence from Tibet. European Journal of Clinical Nutrition, 62, 342–348.
Didan, K. (2015). MOD13C2 MODIS/Terra Vegetation Indices Monthly L3 Global 0.05Deg CMG V006. NASA EOSDIS Land Processes DAAC. Accessed 2021-03-05 from https://doi.org/10.5067/MODIS/MOD13C2.006.
Doll, C., Muller, J. P., & Elvidge, C. D. (2000). Night-time imagery as a tool for global mapping of socioeconomic parameters and greenhouse gas emissions. Ambio, 29(3), 157–162.
Dorsey, J.L., Manohar, S., Neupane, S., Shrestha, B., Klemm, R.D.W., West, K.P. (2018). Individual, household, and community level risk factors of stunting in children younger than 5 years: Findings from a national surveillance system in Nepal. Maternal and Child Nutrition, 14:e12434.
Elvidge, C. D., Baugh, K. E., Kihn, E. A., et al. (1997). Relation between satellite observed visible-near infrared emissions, population, economic activity and electric power consumption. International Journal of Remote Sensing, 18(6), 1373–1379.
Elvidge, C. D., Imhoff, M. L., Baugh, K. E., et al. (2001). Night-time lights of the world: 1994–1995. ISPRS Journal of Photogrammetry and Remote Sensing, 56(2), 81–99.
Elvidge, C. D., Sutton, P. C., Ghosh, T., et al. (2009). A global poverty map derived from satellite data. Computers & Geosciences, 35(8), 1652–1660.
FAO. (1978). Report on the agro-ecological zones project. Vol 1: Results for Africa. World Soil Resources Report. Rome: FAO.
FAO. (2002). Global Agro-ecological Assessment for Agriculture in the 21st Century (GAEZ v 2.0). Rome: FAO/IIASA.
Farahani, R., Kanaan, A., Gavrialov, O., et al. (2007). Differential effects of chronic intermittent and chronic constant hypoxia on postnatal growth and development. Pediatric Pulmonology, 43, 20–28.
Fick, S. E., & Hijmans, R. J. (2017). Worldclim 2: New 1-km spatial resolution climate surfaces for global land areas. International Journal of Climatology, 37(2), 4302–4315.
Filmer, D., & Prichett, L. (2001). Estimating wealth effects without expenditure data–or tears: An application to educational enrollments in states of India. Demography, 38, 115–132.
Fotso, J. C., & Kuate-Defo, B. (2005). Socioeconomic inequalities in early childhood malnutrition and morbidity: Modification of the household–level effects by the community SES. Health and Place, 11, 205–225.
Fullerton, D., Bruce, N., & Gordon, S. (2008). Indoor air pollution from biomass fuel smoke is a major health concern in the developing world. Transactions of the Royal Society for Tropical Medicine and Hygiene, 102, 843–851.
Gani, A. (2015). Air quality and under-five mortality rates in the low-income countries. Journal of Development Studies, 51(7), 851–864.
Gashu, D., Nalivata, P. C., Amede, T., et al. (2021). The nutritional quality of cereals varies geospatially in Ethiopia and Malawi. Nature, 594, 71–76. https://doi.org/10.1038/s41586-021-03559-3
Gibson, R. S., Hess, S. Y., Hotz, C., & Brown, K. H. (2008). Indicators of zinc status at the population level: A review of the evidence. British Journal of Nutrition, 99(S3), S14–S23.
Gómez, M. I., & Ricketts, K. D. (2013). Food value chain transformations in developing countries: Selected hypotheses on nutritional implications. Food Policy, 42(1), 139–150.
Grace, K., Brown, M., & McNally, A. (2014). Examining the link between food prices and food insecurity: A multi-level analysis of maize price and birth-weight in Kenya. Food Policy, 46, 56–65.
Graham, R. D., Knez, M., & Welch, R. M. (2012). How much nutritional iron deficiency in humans globally is due to an underlying zinc deficiency? Advances in Agronomy, 115, 1–40.
Greksa, L. P., Spielvogel, H., & Caceres, E. (1985). Effect of altitude on the physical growth of upper-class children of European ancestry. Annals of Human Biology, 12, 225–232.
Haas, J. D., Moreno-Black, G., Frongillo, E. A., et al. (1982). Altitude and infant growth in Bolivia: A longitudinal study. American Journal of Physical Anthropology, 59, 251–262.
Hanley-Cook, G., Alemayehu, A., Dahal, P., Chitekwe, S., Rijal, S., Bichha, R.P., et al. (2020). Elucidating the sustained decline in under-three child linear growth faltering in Nepal, 1996–2016. Maternal and Child Nutrition, e12982.
Harrison, J. F., Shingleton, A. W., & Callier, V. (2015). Stunted by developing in hypoxia: Linking comparative and model organism studies. Physiological and Biochemical Zoology, 88, 455–470.
Hong, R., Banta, J. E., & Betancourt, J. A. (2006). Relationship between household wealth inequality and chronic childhood under-nutrition in Bangladesh. International Journal of Equity in Health, 5, 15.
Horton, R. (2008). Maternal and child undernutrition: An urgent opportunity. Lancet, 371, 179.
Horton, R., & Lo, S. (2013). Nutrition: A quintessential sustainable development goal. Lancet, 382(9890), 371–372.
Hotchkiss, D. R. (2001). Expansion of rural health care and the use of maternal services in Nepal. Health and Place, 7, 39–45.
Humphrey, J. H. (2009). Child undernutrition, tropical enteropathy, toilets, and handwashing. Lancet, 374, 1032–1035.
IFAD. (2014). Improving nutrition through agriculture. International Fund for Agricultural Development.
International Labor Organization (ILO). (2015). Inventory of official national-level statistical definitions for rural/urban areas. Available at www.ilo.org/wcmsp5/groups/public/—dgreports/—stat/documents/genericdocument/wcms_389373.pdf.
Keyes, L., Armaza, F., Niermeyer, S., et al. (2003). Intrauterine growth restriction, preeclampsia, and intrauterine mortality at high altitude in Bolivia. Pediatric Research, 54, 20–25.
Khlangwiset, P., Shephard, G. S., & Wu, F. (2011). Aflatoxins and growth impairment: A review. Critical Reviews in Toxicology, 41(9), 740–755.
Kihara, J., Bolo, P., Kinyua, M., et al. (2020). Micronutrient deficiencies in African soils and the human nutritional nexus: Opportunities with staple crops. Environmental Geochemistry and Health, 42, 3015–3033.
Kyu, H. H., Georgiades, K., & Boyle, M. H. (2009). Maternal smoking, biofuel smoke exposure and child height-for-age in seven developing countries. International Journal of Epidemiology, 38(5), 1342–1350.
Lavy, V., Strauss, J., Thomas, D., & Vreyer, P. D. (1996). Quality of health care, survival and health outcomes in Ghana. Journal of Health Economics, 15(3), 333–357.
Lindsay, S. W., & Martens, W. J. (1998). Malaria in the African highlands: Past, present and future. Bulletin of the World Health Organization, 76(1), 33–45.
Lokshin, M., & Radyakin, S. (2012). Month of birth and children’s health in India. Journal of Human Resources, 47, 174–203.
Maccini, S. L., & Yang, D. (2009). Under the weather: Health, schooling, and economic consequences of early-life rainfall. American Economic Review, 99, 1006–1026.
Mayer, A.-M., Latham, M., Duxbury, J., Hassan, N., & Frongillo, E. (2007). A food-based approach to improving zinc nutrition through increasing the zinc content of rice in Bangladesh. Journal of Hunger and Environmental Nutrition, 2(1), 19–39.
Mazess, R. B. (1965). Neonatal mortality and altitude in Peru. American Journal of Physical Anthropology, 23, 209–213.
Minten, B. (1999). Infrastructure, market access and agricultural prices: Evidence from Madagascar. Markets and Structural Studies Division Discussion Paper 26. Washington, DC: International Food Policy Research Institute.
Mishra, V., & Retherford, R. (2007). Does biofuel smoke contribute to anaemia and stunting in early childhood? International Journal of Epidemiology, 36, 117–129.
Mohammed, S. H., Habtewold, T. D., Abdi, D. D., Alizadeh, S., Larijani, B., & Esmaillzadeh, A. (2020). The relationship between residential altitude and stunting: Evidence from >26,000 children living in highlands and lowlands of Ethiopia. British Journal of Nutrition, 123(8), 934–941.
Moore, L. G., Charles, S. M., & Julian, C. G. (2011). Humans at high altitude: Hypoxia and fetal growth. Respiratory Physiology and Neurobiology, 178, 181–190.
Moore, S. E., Cole, T. J., Poskitt, E. M. E., Sonko, B. J., Whitehead, R. G., McGregor, I. A., & Prentice, A. M. (1997). Season of birth predicts mortality in rural Gambia. Nature, 388, 434.
National Center for Atmospheric Research Staff (NCARS). (2017). The Climate Data Guide: CRU TS Gridded precipitation and other meteorological variables since 1901. Retrieved from https://climatedataguide.ucar.edu/climate-data/cru-ts-gridded-precipitation-and-other-meteorological-variables-1901.
Nepali, S., Simkhada, P., & Davies, I. (2019). Trends and inequalities in stunting in Nepal: A secondary data analysis of four Nepal demographic health surveys from 2001 to 2016. BMC Nutrition, 5(19), 1–10.
Omiat, G., & Shively, G. (2020). Rainfall and Child Weight in Uganda. Economics and Human Biology 38. https://doi.org/10.1016/j.ehb.2020.100877
Prasad, A. (1991). Discovery of human zinc deficiency and studies in an experimental human model. American Journal of Clinical Nutrition, 53, 403–412.
Preston, S. H. (1975). The changing relation between mortality and level of economic development. Population Studies, 29(2), 321–248.
Rabassa, M., Skoufias, E., & Jaboby, H. (2012). Weather and child health in rural Nigeria. Journal of African Economies, 23(4), 464–492.
Randell, H., Gray, C., & Grace, K. (2020). Stunted from the start: Early life weather conditions and child undernutrition in Ethiopia. Social Science & Medicine, 261, 113234. https://doi.org/10.1016/j.socscimed.2020.113234
Roman, E. M., Bejarano, I. F., Alfaro, E. L., et al. (2015). Geographical altitude, size, mass and body surface area in children (1–4 years) in the Province of Jujuy (Argentina). Annals of Human Biology, 42, 431–438.
Semba, R. D., de Pee, S., Sun, K., et al. (2008). Effect of parental formal education on risk of child stunting in Indonesia and Bangladesh: A cross–sectional study. Lancet, 371, 322–328.
Sharp, P. T., & Harvey, P. (1980). Malaria and growth stunting in young children of the highlands of Papua New Guinea. Papua and New Guinea Medical Journal, 23(3), 132–140.
Shively, G., & Sununtnasuk, C. (2015). Agricultural diversity and child stunting in Nepal. Journal of Development Studies, 51(8), 1078–1096.
Shively, G., & Thapa, G. (2016). Markets, transportation infrastructure and food prices in Nepal. American Journal of Agricultural Economics, 99, 660–682.
Shively, G. (2017). Infrastructure mitigates the sensitivity of child growth to local agriculture and rainfall in Nepal and Uganda. Proceedings of the National Academy of Sciences, 114, 903–908.
Shively, G., Smith, T., & Paskey, M. (2020). Elevation and child linear growth in Nepal. Mountain Research and Development, 40, R11–R20.
Singh, M. V. (2009). Micronutrient nutritional problems in soils of India and improvement for human and animal health. Indian Journal of Fertility, 5(4), 11–16.
Skoufias, E., & Vinha, K. (2011). Climate variability and child height in rural Mexico. Economics and Human Biology, 10, 54–73.
Smith, T., & Shively, G. (2019). Multilevel analysis of individual, household, and community factors influencing child growth in Nepal. BMC Pediatrics, 19, 91–105.
Stinson, S. (1982). The effect of high altitude on the growth of children of high socioeconomic status in Bolivia. American Journal of Physical Anthropology, 59, 61–71.
Tessema, M., De Groote, H., Brouwer, I. D., Feskens, E. J. M., Belachew, T., Zerfu, D., Belay, A., Demelash, Y., & Gunaratna, N. S. (2019). Soil zinc is associated with serum zinc but not with linear growth of children in Ethiopia. Nutrients, 11(2), 221.
Thai, T. Q., & Falaris, E. M. (2014). Child schooling, child health, and rainfall shocks: Evidence from rural Vietnam. Journal of Development Studies, 50(7), 1025–1037.
Thiede, B. C., & Strube, J. (2020). Climate variability and child nutrition: Findings from sub-Saharan Africa. Global Environmental Change, 65, 102192. https://doi.org/10.1016/j.gloenvcha.2020.102192
Thomas, D., & Strauss, J. (1992). Prices, infrastructure, household characteristics and child height. Journal of Development Economics, 39(2), 139–331.
UNICEF, WHO, and World Bank Group. (2019). Levels and trends in child malnutrition. UNICEF/WHO/World Bank Group Joint Child Malnutrition Estimates Key findings of the 2019 edition. Accessed 04/19/20 at https://www.who.int/nutgrowthdb/jme-2019-key-findings.pdf?ua=1
Wang, W., Liu, F., Zhang, Z., et al. (2016). The growth pattern of Tibetan infants at high altitudes: A cohort study in rural Tibet region. Nature Scientific Reports, 6, 1–8.
Wiley, A. S. (1994). Neonatal size and infant mortality at high altitude in the western Himalaya. American Journal of Physical Anthropology, 94, 289–305.
WHO in de Onis M. (2006). Weltgesundheitsorganisation WHO Child Growth Standards: Length/Height-for-Age, Weight-for-Age, Weight-for-Length. WHO Press Geneva.
WHO. (1995). Physical status: the use and interpretation of anthropometry. Report of a WHO Expert Committee. Technical Report Series No. 854. Geneva: World Health Organization.
Zahran, S., Breunig, I., Link, B., Snodgrass, J., & Wiler, S. (2014). A quasi-experimental analysis of maternal altitude exposure and infant birth weight. American Journal of Public Health, 104, S166–S174.
Zhao, N., Currit, N., & Samson, E. (2016). Net primary production and gross domestic product in China derived from satellite imagery. Ecological Economics, 70(5), 921–928.
Funding
Financial support for this research was provided in part by the Feed the Future Innovation Lab for Nutrition, which is funded by the US Agency for International Development (USAID). USAID provides financial support for the DHS Program. DHS and GIS data sets were compiled as part of the Advancing Research on Nutrition and Agriculture (ARENA) project (https://www.ifpri.org/project/advancing-research-nutrition-and-agriculture-arena) which is funded by the Bill and Melinda Gates Foundation.
Author information
Authors and Affiliations
Contributions
The authors’ responsibilities were as follows: GS was responsible for the overall design and planning of the study; JS contributed to the analysis, construction of the tables and figures, and writing of the manuscript; GS had primary responsibility for the final content; and both GS and JS reviewed the manuscript for accuracy and read and approved the final manuscript.
Corresponding author
Ethics declarations
Conflict of interest
Gerald Shively declares a relationship with the International Food Policy Research Institute but no conflict of interest. Jacob Schmiess declares no conflict of interest.
Disclaimer
USAID had no role in the collection, analysis, or interpretation of the data, and played no role in the decision to submit the paper for publication. The opinions expressed herein are those of the authors and do not necessarily reflect the views of the sponsoring agencies.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix
Appendix
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Shively, G., Schmiess, J. Altitude and early child growth in 47 countries. Popul Environ 43, 257–288 (2021). https://doi.org/10.1007/s11111-021-00390-w
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11111-021-00390-w