
Abstract
The aim of this study was to analyse the association between season of birth, temperature and neonatal mortality according to socioeconomic status in northern Sweden from 1880 to 1950. The source material for this study comprised digitised parish records combined with local weather data. The association between temperature, seasonality, socioeconomic status and neonatal mortality was modelled using survival analysis. We can summarise our findings according to three time periods. During the first period (1880–1899), temperature and seasonality had the greatest association with high neonatal mortality, and the socioeconomic differences in vulnerability were small. The second period (1900–1929) was associated with a decline in seasonal and temperature-related vulnerabilities among all socioeconomic groups. For the last period (1930–1950), a new regime evolved with rapidly declining neonatal mortality rates involving class-specific temperature vulnerabilities, and there was a particular effect of high temperature among workers. We conclude that the effect of season of birth on neonatal mortality was declining for all socioeconomic groups (1880–1950), whereas weather vulnerability was pronounced either when the socioeconomic disparities in neonatal mortality were large (1880–1899) or during transformations from high to low neonatal rates in the course of industrialisation and urbanisation.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The association between ambient temperature and early infant mortality has been seen in both contemporary and historical populations with risk increasing both due to heat and to cold (Basu & Ostro, 2008; Karlsson et al., 2020; Scalone & Samoggia, 2018; Son et al., 2017; Xu et al., 2012). Neonates are especially vulnerable to heat and cold-related death due to their thermal instability (Basu & Ostro, 2008; Kumar et al., 2009). Another factor highly related to the association between temperature and early infant health is the seasonality of neonatal mortality, where seasonal patterns might vary in different population and at different times (Fellman & Eriksson, 2001). During the nineteenth century, the infant and neonatal mortality rates diverged geographically and socially in northern Sweden, especially between rural areas (Brändström, 1990; Sköld & Axelsson, 2008; Sundin & Willner, 2007). We also know that the seasonality and influence of extreme temperature on neonatal mortality varied over time and differed between indigenous and non-indigenous groups living in the same sub-Artic area (Karlsson, 2017; Karlsson et al., 2019a, b; Schumann et al., 2019). However, we lack knowledge if these differences in temperature and seasonal vulnerabilities found between the ethnic groups also were present between the social classes. This sub-Arctic area constitutes a climatically unique region (long and cold winters, and short and mild summers), which add scientific relevance to previous studies of the association between temperature and neonatal mortality in temperate climates.
High infant and neonatal mortality rates were difficult obstacles to overcome in preindustrial Sweden, and it was not until the twentieth century that the major shift occurred (Kohler, 1991; Sköld et al., 2011). The first half of the twentieth century corresponded to political, social and demographic transformations, where Sweden went from a rural and agrarian to an urban and industrialised society (Stråth, 2012). Compared to many other countries, industrialisation and urbanisation processes began later and at a slower pace in Sweden, especially in the north (Nilsson & Edvinsson, 2000). During the transformation from an agrarian to an industrialised and urbanised society (1880–1950), a new middle class and working class emerged. We do not know, however, if seasonality and weather vulnerability among new-borns differed across classes or how vulnerabilities changed during these societal changes. To fill the gap, we assessed how seasonality and weather were associated with neonatal mortality among different social groups during the socio-economic transformation.
Objective
First, we aimed to study the association between season of birth and neonatal mortality according to socioeconomic status (SES) in northern Sweden between 1880 and 1950. Second, we aimed to study the association between temperature and neonatal mortality and whether the association varied according to socioeconomic status. Our research questions were:
-
1.
Were there socioeconomic differences in seasonal patterns of neonatal mortality? If so, were there socioeconomic differences in turning points in seasonal neonatal mortality?
-
2.
What was the association between temperature exposure and neonatal mortality according to SES? How did climate vulnerability change over time for different SES groups?
Previous research
Socioeconomic status and infant mortality
Socioeconomic differentials in infant mortality have been shown in studies of both historical (Bengtsson, 2004; Burstrom & Bernhardt, 2001; Scalone & Samoggia, 2018) and contemporary populations (for a systematic review, see Blumenshine et al., 2010). During the early twentieth century, an increase in socioeconomic differences in infant mortality occurred in England, Germany and the USA (Preston & Haines, 1991). In some Western countries of today such as England and Wales, the absolute inequality in neonatal mortality according to SES decreased between 1930 and 2000, whereas the relative inequality is still lagging behind (Floud, 2011). This pattern holds true even after taking into account changes in the occupational structure of the population and selection effect (Floud, 2011).
In the five Nordic countries before the twentieth century, there was no evident association between socioeconomic status and infant mortality, but the transition towards lower infant mortality seems to have benefited the higher social strata (Bengtsson, 1999; Edvinsson et al., 2008). As the overall infant mortality declined in Sweden between 1890 and 1910, the socioeconomic differences in mortality increased, mainly due to a sharper mortality decrease among the middle and upper strata (Burstrom & Bernhardt, 2001). The advantage of higher social strata was associated with their improved living conditions and earlier access to knowledge and prevention measures, which were later spread to more resource-poor groups (Sundin & Willner, 2007).
The socioeconomic differences in neonatal and infant mortality rate during the late nineteenth and early twentieth centuries have also been associated with the health and nutritional status of the mother, both before and after birth (Derosas, 2009), and with diverging feeding and weaning practices (Brändström, 1993; Derosas, 2009; Reid, 2001). During the nineteenth century, higher infant mortality was seen among farmers in Sweden, and this was explained by their practice of feeding infants with cow milk (Edvinsson et al., 2008). In some northern areas, a higher infant mortality and a higher prevalence of feeding infants with cow milk were seen among the more affluent groups (Brändström, 1990). Compared to the more affluent groups, alternatives to breastfeeding were limited among the more disadvantaged strata (Brändström, 1993). Thus, the association between socioeconomic status, feeding practices, and infant mortality has not been fully explored, and the results diverge between time periods and locations. In the northern part of Sweden associated with high infant mortality rates, trained midwifes played a major role in improving infant and child health through breastfeeding campaigns, instructions of infant care, and assisted births (Högberg, 2004; Thorvaldsen, 2008).
In Sweden, fertility levels differed between the socioeconomic strata until the 1930s, whereby less affluent groups in general had a greater number of children and shorter interpregnancy period compared to more affluent groups (Ohlander, 1994). Among resource-poor mothers with many children, older siblings often took care of their younger siblings (Ohlander, 1994), which might have risked the supervision of infants. Other factors associated with socioeconomic differentials in neonatal and infant mortality were differences in living conditions, sanitation and dwelling standards between the social strata (Sundin & Willner, 2007). Especially during the late nineteenth and early twentieth centuries when a majority of childbirths occurred at home, poor housing conditions with inferior heating might have had a negative impact on neonatal health and survival. Important factors associated with the declining infant mortality rate in Sweden were health policies and interventions targeted at maternal and child health and the development of obstetrics and neonatal care (Andersson et al., 2000; Burstrom & Bernhardt, 2001; Lazuka et al., 2016). The large-scale preventive efforts that started at the end of the 1930s benefitted the whole population, but particularly the less affluent groups (Kohler, 1991; Sundin & Willner, 2007).
Overall, during the nineteenth and early twentieth centuries, SES in Sweden might have had the greatest impact on health and survival of infants partly due to difficult living conditions for the less affluent groups and partly due to better access to knowledge and prevention measures among the more affluent groups (Sundin & Willner, 2007).
Seasonality, temperature and neonatal mortality
From previous research regarding infant and neonatal mortality in historical populations, we know that season of birth affects the risk of mortality (Breschi & Livi-Bacci, 1997; Hare et al., 1981; Karlsson et al., 2019b; McEniry, 2011). In general, winter-born infants have higher neonatal mortality risk compared to summer-born infants (Dalla-Zuanna & Rosina, 2011; Healy, 2003; Karlsson et al., 2020), but an opposite pattern has also been found (Breschi & Livi-Bacci, 1997). For example, in Poland and Russia during the nineteenth century, the highest neonatal mortality was seen among summer-born infants, a pattern that might be associated with a higher workload among mothers during harvest seasons (Breschi & Livi-Bacci, 1997). A trend toward de-seasonality for neonatal mortality rates was found by Hare, Moran and Macfarlane using data for England and Wales from 1928 to 1978 (Hare et al., 1981).
The seasonal pattern of infectious diseases is well documented (respiratory diseases increase in winter and digestive diseases increase in summer), and this affects the seasonality of neonatal mortality. Further, neonatal mortality and the seasonality of infectious diseases also appear to be associated with exposure to ambient temperature, especially low winter temperatures (Hare et al., 1981) or high summer temperatures (Victora et al., 1985). Also, factors linking weather conditions to seasonal variations in birth outcomes have been observed, such as an increased risk of preterm birth, low birth weight and stillbirths, following temperature extremes (Oris et al., 2004; Strand et al., 2011). For example, in Italy from 1820 to 1900, cold temperatures during the neonatal period increased the risk of cold-related infectious diseases primarily among preterm infants (Scalone & Samoggia, 2018). In the Netherlands from 1850 to 1954, Ekamper et al. (2009, 2010) showed that the effect of temperature was the most significant among infants (< 1 year of age) compared to other age groups, where both extremely high and low temperatures increased the infant mortality risk. Ekamper et al. also showed that infants became less sensitive to temperature fluctuations over time (Ekamper et al., 2010). Studies have shown that seasonal patterns of mortality are amplified by poor living conditions, crises, wars, epidemics and famines (Fellman & Eriksson, 2001).
Taken together, both season and ambient temperature affect neonatal health and mortality among historical populations. In contemporary resource-poor countries, adverse temperature (extreme cold or warm) has a direct effect on neonatal mortality through hypothermia and hyperthermia (Amadi et al., 2015; Kumar et al., 2009; Lunze et al., 2013; Mullany, 2010; Mullany et al., 2010). While hypothermia is a major challenge even in tropical environments, its indirect or direct effects are not fully explored. Hypothermia might be an indirect cause of death associated with mortalities of severe infections (sepsis and pneumonia) (Lunze et al., 2013). Furthermore, hypothermia can also have a direct effect on the cause of death, especially among preterm and extremely low-birth weight neonates (Amadi et al., 2015; Lunze et al., 2013; Mullany et al., 2010).
Socioeconomic differentials in climate vulnerability of neonates
In order to separate causes of death during the neonatal and/or the post-neonatal period, factors are distinguished as endogenous or exogenous. Death in the first week of life is more related to endogenous (biological) factors like preterm birth, congenital malformations and genetic disorders, whereas exogenous (societal, economic, cultural and environmental) factors become more prevalent in neonates at 1–4 weeks of age (Lalou et al., 1997; Reid, 2001). However, studies of historical populations have revealed that endogenous mortality is also influenced by socioeconomic (exogenous) factors (Lalou et al., 1997). The risk of neonatal mortality is especially higher among preterm infants and/or infants of low birth weight (Lawn et al., 2014). In contemporary and historical settings, mothers holding lower SES have higher risk of preterm birth and/or of having infants with low birth weight (Blumenshine et al., 2010; Costa, 1998; Hossin et al., 2020). In their study of neonatal mortality in northern Italy from 1820 to 1900, Scalone and Samoggia (2018) showed that the effect of low temperature at birth varied according to SES, where the infants of landless rural labourers constituted the most vulnerable group (Scalone & Samoggia, 2018).
Derosas (2009) tested the so-called hypothermia hypothesis that women of lower social strata were chronically undernourished, which caused underweight new-borns, which in turn led to higher risk of neonatal death due to hypothermia. Derosas found a higher neonatal mortality risk among infants born during cold periods and among those with lower SES, but no interaction effect between SES and cold temperature. However, evidence for an effect of short-term undernourishment during low temperatures on neonatal mortality was found among infants of lower SES mothers (Derosas, 2009).
Because neonatal mortality is highly related to factors associated with giving birth, midwife-assisted deliveries and the introduction of maternity hospitals were important for the decrease in neonatal mortality during the period 1880–1950. During the last decades of the nineteenth and early twentieth centuries, assisted deliveries increased significantly in rural areas in Sweden, and almost 80% of the home deliveries were assisted by a trained midwife (Högberg, 2004). The use of antiseptic methods and an emphasis on breastfeeding and the importance of warmth might have contributed to decreased neonatal mortality, especially during the winter season (Högberg, 2004).
Following previous research, we expected for northern Sweden during the demographic transition:
-
1.
A peak in winter neonatal mortality and an increased neonatal mortality risk during cold extremes
-
2.
Higher winter mortality and higher climate vulnerability among the more disadvantaged groups (farmers/workers) compared to the middle class
-
3.
A general diminishing trend of seasonality and climate vulnerability in neonatal mortality from 1880 to 1950
Data and methods
Population data
The source material for this study consisted of digitised parish records provided by the Demographic Data Base, Umeå University (DDB, 2019a). The population data contained linked individual data from parish registers and registers of birth, deaths, migration etc., and included every individual who was born or migrated into the parishes (Westberg et al., 2016). In this study, we used date of birth, parish of birth, father’s occupation, birth parity and sex (for a project description, see DDB, 2019b). Our sample size consisted of 122,756 live births, of which 3985 infants died during the neonatal period (Table 2). All of the data on individuals (dead or still alive during the study period) included in the dataset were anonymised.
The study area included the coastal parishes of Umeå and Skellefteå and the inland parishes (Fig. 1), representing varying levels of industrialisation and urbanisation. In the coastal areas of Skellefteå and Umeå, the industrialisation was high during the first decades of the twentieth century, followed by a shift in populations from rural to urban areas during the 1950s and 1960s (especially in the Umeå area). For Umeå, the population data included individuals who were born from 1895 to 1950, whereas the data for Skellefteå and the Inland region included individuals who were born during the entire study period from 1880 to 1950.

Map of the study area, divided by their nearest weather station
Neonatal mortality was defined as death during the first 28 days after birth (stillbirths excluded). In studies of neonatal mortality among historical populations, the accuracy of registration of stillbirths is important, because an under-registration of stillbirths would inflate the neonatal mortality rate and vice versa. In a comparative perspective, Sweden has a high quality of stillbirth registration from 1750 onwards, where the establishment of the governmental agency Statistics Sweden in 1860 further strengthened the accuracy of registrations of stillbirths or early neonatal deaths (Woods, 2009). Since the data for this study included neonatal deaths during the period 1880 to 1950, our results of temperature effect on neonatal mortality are not likely affected by possible bias in stillbirth registrations.
We categorised months of births into extended seasons based upon the day of the year, with a summer season extending from day 91 to 273 (approximately April 1–October 31) and a winter season from day 274 to day 90 (approximately November 1–March 31). This was done to be able to measure the effect of the day of the year within extended seasons as a continuous variable without any gaps.
Regarding parity, previous studies have shown that the mortality risk decreases after the first child and then increases again for four or more children (Knodel, 1988). That first-born infants have higher vulnerability is especially notable for neonatal mortality (Reid, 2001). We therefor controlled for parity, which was categorised as 1, 2–3 and 4 .
Socioeconomic status
Neonatal mortality differences were analysed according to the occupational position of the father at the time of birth based on the historical international standard classification of occupations (HISCO) (Van de Putte & Miles, 2005; Van Leeuwen, 2002). Paternal occupation was categorised into three main groups—farmer, middle-class and worker—using a modification of the Social Power (SOCPO) scheme (Van de Putte & Miles, 2005). SOCPO categorises HISCO codes into six hierarchical groups from ‘elite’ to ‘unskilled worker’. Because of low numbers in some classes, the schema was condensed by combining elite and middle class into one group called ‘Middle class,’ and all workers into one group. Additionally, self-employed farmers were defined as a separate group. The dataset had missing data on socioeconomic status for 13,293 individuals (9.8%). Infants with missing occupational data for the father were excluded from the analyses.
Figure 2 shows the distribution of social classes from 1880 to 1950 according to the fathers’ occupations. At the end of the nineteenth century, farmers constituted the major category followed by workers. During the first decades of the twentieth century, the proportion of middle class increased from previous low levels of 6.2% in 1900 to 23.2% in 1950. The workers increased from 36.9% in 1900 to 54.6% in 1950, whereas the proportion of farmers decreased over time (from 59.9 to 22.2%). At the end of the study period, the occupational structure in northern Sweden was almost the opposite of that at the beginning of the study period. As seen in Fig. 10, Appendix, the social class composition between the regions diverged, where middle class and workers increased in Umeå and Skellefteå, especially from 1930 onwards, whereas the predominantly rural Inland region still had a high proportion of farmers and an increasing proportion of workers.

Socioeconomic distribution of neonates based on father’s occupation, 1880–1950
Temperature data
Temperature data were obtained from the Swedish Meteorological and Hydrological Institute (SMHI) (Swedish Meteorological and Hydrological Institute, 2019) for three weather stations closest to the study area—Umeå, Bjuröklubb and Stensele (Table 1). These data (three daily measurements—morning, noon, evening) were controlled and validated by the SMHI, with the exception of the following years, for which only uncontrolled data were available: Umeå 1940–1944 and 1946–1950 and Bjuröklubb 1919–1948. SMHI gives access to controlled data on an open data website (SMHI, 2021). We obtained non-controlled data from SMHI to fill the gaps in the controlled data. The non-controlled data follow the expected seasonal patterns of daily variations.
We computed mean daily temperature as the mean of the three daily values. If some sub-daily measurement was missing, the daily mean was imputed based on the mean of available measures on the current day, the day before and the day after.
Umeå weather data were used as estimates for infants in Umeå’s rural and urban parishes, Bjuröklubb weather data were used for infants in Skellefteå (Sankt Olof, Bureå, Byske and Lövånger), and the average of Stensele and Bjuröklubb weather data were used for infants born in Norsjö, Jörn and Malå (inland region).
As seen in Table 1, temperature extremes diverged between the two coastal weather stations of Bjuröklubb and Umeå and the inland station of Stensele. Stensele had a much lower minimum temperature (−40.9 °C) compared to the coastal stations (−35.2 °C and −30.8 °C, respectively). For the warmer seasons (April through September), the maximum and minimum temperatures between the stations were more similar. Maximum temperature ranged from 26.7 °C in Stensele to 28.8° C in Umeå, and minimum temperatures ranged from −12.6 °C in Umeå to −15.4 °C in Stensele.
Statistical analysis
Given that season of birth and daily temperature exposures were measured at different time-scales, different statistical models were used to estimate their association with neonatal mortality. Season of birth is fixed for each infant; thus, exposure time can be considered as continuous. Therefore, Cox proportional hazard models were used, which is suitable for the analysis of continuous-time data. Daily temperature exposures vary across the life course of infants, and exposure time can be considered as discrete, occurring at a daily basis. Thus, discrete-time survival analysis was applied, implemented using logistic regression.
Estimation of neonatal mortality and seasonal patterns
In order to produce the yearly neonatal mortality rate by socioeconomic status, we used a LOESS regression using a smoothing parameter of 0.4 (Cleveland et al., 1997). We modelled the association between seasonality of birth, socioeconomic status, and neonatal mortality using Cox proportional hazard analysis, with age in days as the time scale, adjusting for calendar time, sex and parity at birth. The model was specified as:
where the hazard of death λ(t) is a function of the baseline hazard λ0(t) represented by age in days and the exponentiated linear predictors Xtβ. The model matrix X is composed of father’s SES, seasonality, calendar time specified as a cubic spline with three degrees of freedom (De Boor, 1978; Hastie, 1997) parity grouped into parity 1, 2–3 and 4+, sex and region, and β is the corresponding matrix of coefficients. Visual analyses of the proportional hazards and tests of the Schoenfeld residuals supported the proportionality assumption of the Cox models.
In the first step of the analysis, we specified seasonality as a continuous non-linear function based on the day of the year at birth. The day of the year was specified as a cubic spline with six degrees of freedom. To assess how the non-linear effect of seasonality varied across the year, we calculated hazard ratios (HRs) for each day of the year compared to the first of August, which was the month with the lowest mortality rate. To assess how seasonality varied between SES groups, we ran separate models for each group.
Second, we used extended seasons (winter = October through March, and summer = April through September) to assess how SES differences in seasonal mortality varied across the study period, with separate models for each time period (1880–1899, 1900–1929 and 1930–1950). Additionally, we performed sensitivity analyses adjusting for regional differences.
Estimation of temperature effects on neonatal mortality
For the analyses of the association between temperature and neonatal death, we used temperature as a continuous variable from the observed lifetime temperature exposures at each station (Table 1). The mean lifetime temperature exposure was continuously measured, on a daily basis, over the life course of each infant during the neonatal period (up to 28 days unless the infant died). Lifetime temperature exposure has been used in previous studies on the association between heat exposure and infant mortality (Son et al., 2017).
To analyse the effect of daily temperature exposure, the data were transformed into a person-period format with one row for each day in an infant’s life up to 28 days. The association between temperature, SES, and neonatal mortality was modelled using discrete-time survival analysis (Allison, 1982) while adjusting for the baseline hazard age, seasonality, calendar time, sex and parity. Formally, we modelled the log-odds of death P at time t given survival to time t using logistic regression as:
where \(\gamma \left(t\right)\) is the baseline odds hazard function represented by age in days as a cubic spline with knots at age 1.5 and 4 days old. X is a model matrix of time-varying characteristics, and \(\beta\) is the corresponding matrix of coefficients. Within X, seasonality was represented by day of year modelled as a cubic spline with two degrees of freedom, calendar time was modelled as a cubic spline with three degrees of freedom, and a dummy variable, representing the time of day in which temperature measurements were gathered. The timing of noon-temperature measurements varied over the study period, shifting back and forth between 12:00 and 13:00. In addition, X included time-fixed covariates, sex, parity and the region of birth. Because the association between neonatal mortality risk and temperature is nonlinear, the effect of temperature was modelled as a linear threshold function with a cut point at the minimum mortality temperature, around +14.5 °C. To interpret the nonlinear coefficients, we calculated the odds ratios (ORs) over the temperature span where we observed any neonatal deaths, from −32 °C to + 24 °C. To assess variations between SES groups, we specified separate models for each group, and to assess changes over time, we specified separate models for each SES-period combination. Given the possible measurement errors introduced by using the average of Stensele and Bjuröklubb temperatures for the inland temperature estimates, additional sensitivity analyses were performed. In these analyses, we introduced an interaction between season (day of year) and region, in order to assess the impact of seasonal variations in temperature in the inland region on the estimated ORs. We used the statistical software R package dlnm (Gasparrini, 2014, 2019; Gasparrini et al., 2010) for all analyses.
Results
As shown in Table 2, there were large differences in neonatal mortality rates between the locations, where the urban area of Umeå had lower rates (for Umeå 1895–1950) compared to the more rural areas. Children of farmers and workers had the highest neonatal mortality rates (34.6 and 31.4 deaths/1000 live births, respectively), followed by the middle class (26.6). The neonatal mortality rate decreased during the study period, where the major decrease occurred between the two last periods, from 34.7 in 1900–1929 to 23.7 in 1930–1950 (Table 2). Boys had a higher neonatal mortality rate than girls (35.9 and 28.8, respectively), and the rates were higher among children of parity 4 + (35.8) and first-born infants (33.2) compared to parity 2–3 (27.6).
Trends in neonatal mortality by socioeconomic status
The pattern of neonatal mortality differed between the social strata, especially during the last decades of the nineteenth century (Fig. 3). Among the middle class, the neonatal mortality rate declined significantly until the early 1900s, whereas the period 1900–1930 was characterised by rather stable neonatal mortality rates among all social classes. The social classes had different turning points in neonatal mortality rates, and among the middle class, mortality started to decline rapidly during the late nineteenth century, whereas neonatal mortality among the farmers started to decline from the turn of the twentieth century. For the workers, the decrease in neonatal mortality rate was a slower process, with the major downward turn from 1930 onwards. At the end of the study period, the absolute inequalities in neonatal mortality had decreased, whereas the relative inequalities still existed (with workers now having the highest rates).

Neonatal mortality by paternal socioeconomic status, 1880–1950, LOESS fits
Social class and seasonal patterns of neonatal mortality, 1880–1950
Figure 4 shows HRs of neonatal mortality by day of birth within the year compared to the first of August. The lowest neonatal mortality risks were found around August and September, while the highest HR was found during the winter months, December to February. However, a peak in mortality could also be seen around June.

HRs of seasonal variation in neonatal mortality by day of birth, with 95% confidence intervals (grey area), 1880–1950. Reference: 1 August. Estimations from models seen in Table 5
Figure 5 shows the association between the day of birth and neonatal morality risks by social class. The winter months of January and February were found to be the most hazardous for all classes, whereas summer HR showed larger variations. Farmers had a higher HR around June, while the middle class had the lowest HR in the same period.

HRs of neonatal mortality by day of birth with 95% confidence intervals, stratified by SES. Reference: 1th of August. Estimations from models seen in Table 6
The neonatal mortality rate by extended season 1880–1950 (Fig. 6) showed an excess of winter neonatal mortality, except during a couple of years at the beginning of the twentieth century and at the end of the study period. Following the winter neonatal mortality rate, Fig. 6 shows two time points when the mortality rate declined, starting from the end of the nineteenth century to 1910, followed by a plateau 1910–1930, thereafter a sharper decline during the last 20 years to 1950. The summer neonatal mortality showed a similar downward trajectory as the winter neonatal mortality, with decreasing trends around 1910 and 1935.

Neonatal mortality rate by extended season with 95% confidence intervals, 1880–1950
Seasonal differences in neonatal mortality over time
We calculated HRs of neonatal mortality (Fig. 7 and Table 3) from the regression model including an interaction between season of birth and SES stratified by birth period (Table 4 in Appendix). For the first time-period, 1880–1899, the excess in winter neonatal mortality was especially notable for the farmers (HR 1.30, CI 1.12–1.51), followed by the workers (HR 1.20, CI 1.01–1.43). The middle class was too small at that time to detect any effect of seasonality on mortality (Fig. 7). During the second time period, 1900–1929, the differences between winter and summer neonatal mortality decreased for the farmers and workers, whereas the neonatal mortality risk in winter had a substantial effect on the middle class (HR 1.56, CI 1.26–1.93). Overall, there was a de-seasonality of neonatal mortality among the social classes over time from 1880 to 1950.

Seasonal variations in neonatal mortality by SES with 95% confidence intervals, stratified by period. Reference: summer. Estimations from model seen in Table 4
Social class and neonatal mortality, lifetime exposure 1880–1950
Logistic regression models adjusting for sex, parity, age at death, seasonality, region and time trends showed an increased neonatal mortality risk at both low and high temperatures among all social classes (Fig. 8 and Tables 7 and 8 in Appendix). At –25 °C, the OR was about 2.38 (CI 1.15–4.94) for the middle class, and 1.64 (CI 1.22–2.19) for farmers, whereas workers had an OR of 1.66 (CI 1.18–2.34) compared to infants born at temperatures of 14.5 °C. Workers had the largest effect of high temperatures, where a temperature increase from 14.5 °C to 20 °C was associated with an increased mortality risk (OR 1.70, CI 1.32–2.19).

Odds ratios of neonatal mortality by temperature with 95% confidence intervals, stratified by SES, 1880–1950. Reference: 14.5 °C (minimum mortality temperature). Estimations from model seen in Table 7
Temperature effects on neonatal mortality over time
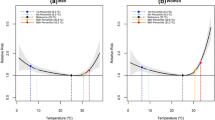
Comparing the temperature vulnerability among the social classes over time, Fig. 9 and Tables 9 and 10 in the Appendix show the effects of low and high temperatures on workers from 1880 to 1899 (at −25 °C, OR 2.3 CI 1.18–4.47, and at + 20 °C, OR 1.90 CI 1.01–3.70). The period 1900–1929 corresponded to a declining effect of both low and high temperatures among all social classes. For the period 1930–1950, the effect of temperature increased, with a large effect of low temperatures for the middle class (−25 °C, OR 4.14, CI 1.24—13.79) and an effect of high temperatures for the workers (+20 °C, OR 1.90 CI 1.28—2.76). For the middle class, temperature vulnerability was noticeable during the last period (1930–1950), whereas the farmers and workers were most vulnerable during the first period (1880–1899). For workers, vulnerability to high temperatures emerged again in the last period.

Odds ratios of neonatal mortality by temperature with 95% confidence intervals, stratified by SES and time period. Reference: 14.5 °C (minimum mortality temperature). Estimated from model seen in Table 9
As we used the average of Stensele and Bjuröklubb temperatures to estimates of inland temperature exposures, there is a possibility for a regional bias in the estimates dependent on differences in seasonal variations in temperature between the observed temperatures and the actual exposures in the inland. We performed sensitivity analysis to assess how this potential bias could affect the estimates, by introducing an interaction between region and season allowing the seasonal effect to vary by region (Fig. 11). These analyses show similar results to the models without the interaction, suggesting that the original models were not biased by an underestimation of seasonal temperature variations in the inland region.
Discussion
During the first decades of the twentieth century, this northern Swedish region underwent industrialisation, resulting in an increased population and a transformation from an agricultural to a socially and economically more diversified society. From the last decades of the nineteenth century to the first decades of the twentieth century, the overall neonatal mortality rate declined in Sweden (Gyllenswärd, 1946). As the overall infant mortality declined, the socioeconomic differences in mortality increased, mainly due to a sharper decrease of mortality among the middle and upper strata (Burstrom & Bernhardt, 2001). In our population in northern Sweden, a similar pattern was found, where the neonatal mortality started to decrease sharply among the middle class, followed only later by farmers and workers.
In this northern area of Sweden in 1880–1950, the differences in neonatal mortality between the social strata were significant up to 1930, and thereafter, the rates converged between the social groups, but the relative inequalities persisted. Among the middle class, the major decrease in neonatal mortality started from the end of the nineteenth century, whereas the decreasing trend among the workers started about 40 years later (in the mid-1930s) implying the advantages of higher classes in the health transformation (Sundin & Willner, 2007; Zetterström & Eriksson, 1987). The results presented here suggest that at the beginning of a health transformation, small-scale interventions (such as information targeted towards parents regarding breastfeeding and infant care) have a significant impact on neonatal health, mainly among the wealthier groups, whereas large-scale interventions (maternal and infant health care, maternity hospitals and neonatal care) and overall living improvement are most important for diminishing health disparities between infants from different socioeconomic groups.
Regarding seasonal differences in neonatal mortality, our findings show a clear pattern of de-seasonality over time (Hare et al., 1981) among all social classes. We can summarise our findings according to the three time-periods. During the first period (1880–1899) associated with high neonatal mortality and major socioeconomic disparities in mortality, we find a pre-transitional regime where temperature and seasonality had the greatest effects, and the socioeconomic differences in vulnerability were small. During the second period (1900–1929), we see a transitional regime, with a decline in seasonal and temperature-related vulnerabilities among all socioeconomic groups. For the last period (1930–1950), a new regime evolves with rapidly declining neonatal mortality rates involving class-specific temperature vulnerabilities of low temperatures (middle class) respective to high temperatures (workers).
According to previous findings regarding the effect of temperature on neonatal health in sub-Arctic areas (Karlsson et al., 2020; Schumann et al., 2019), we expected a strong impact of low temperatures, especially among more resource-poor groups (farmers and workers) that would diminish over time. A declining effect was not clearly discernible in any social group due to the low vulnerability observed in the first decades of the twentieth century. Comparing the first and last periods revealed a diminishing trend of both high and low temperatures among the farmers. The increased effect of high temperature among the working-class in the last period (1930–1950) was an unexpected finding. In Sweden, this period was associated with extensive social, political and demographic changes (Ohlander, 1994; Sundin & Willner, 2007). The fertility rates declined and female labour participation increased, health services improved and the proportion of deliveries at maternity hospitals increased (Gyllenswärd, 1946; Sundin & Willner, 2007). In this northern part of Sweden during the late 1930s, almost 80% of the rural mothers received a need-based maternal subsidy (Ohlander, 1994), implying that the mothers suffered from economic hardship, especially among rural workers.
Different mechanisms are involved in socioeconomic differentials in health and mortality, including living and working conditions, material circumstances and socio-environmental and behavioural factors (Solar & Irwin, 2010). From our findings, we conclude that the living and working conditions and material circumstances have been most important for the differences seen in seasonal and temperature vulnerability among neonates. From 1880 to the first decades of the twentieth century, the middle class and workers differed substantially regarding material resources, their physical environments (housing, central heating, crowding) and working conditions (Sundin & Willner, 2007). The workers, being resource poor and facing higher fertility and shorter interpregnancy periods compared to more affluent families, would have been expected to be more vulnerable to temperature extremes. If breast feeding was uncommon among workers, the neonatal mortality should have peaked during the summer season (Lithell, 1981). Our findings, however, show very small seasonal differences in neonatal mortality rates among the workers. The increased neonatal mortality risk among workers during warm extremes is likely associated with overall disparities in material resources, where unsanitary conditions in particular might have negatively affected the working-class mothers (during pregnancy, delivery and after delivery) and their infants. During the 1930s and 1940s, a significant proportion of births took place in one’s own home, assisted by a midwife, especially in rural areas with long distances to hospitals (Gyllenswärd, 1946). It is possible that the workers to a high extent had home-assisted births and that the neonatal mortality risk therefore increased during warm extremes due to higher indoor temperatures in small houses compared to hospitals. The differences in birth conditions between the socioeconomic groups during the early to mid-twentieth century is an area that needs further research in order to detangle socioeconomic differentials in neonatal health and mortality. In particular, we see the transformation of farm workers to non-farm workers as an important aspect of changing living conditions that would influence the wealth and resilience of the working-class mothers.
Neonatal mortality is related to a combination of physiological, behavioural and environmental factors (Kumar et al., 2009). Therefore, further research is needed regarding vulnerable groups during social, demographic and epidemiological transitions. In this study, we have examined the influence of temperature exposures on neonatal mortality among different socioeconomic strata, and in our previous studies differences between indigenous and non-indigenous populations (Karlsson et al., 2019a; Schumann et al., 2019). The population data used in this study (1880–1950), however, lack ethnic markers, impeding further comparisons between the two populations. Forthcoming research will investigate the association between temperature and deaths prior to birth (stillbirths) and whether the association diverged between socioeconomic groups. From previous research, we know that the stillbirth rate was higher in northern Sweden compared to southern areas and was higher in rural areas compared to larger cities (Gyllenswärd, 1946). It is possible that fragile women to a higher extent suffered the effects of temperature during their last trimester, and that this vulnerability was higher among the less affluent groups.
Strengths and limitations
A major strength of this study is the availability of a large dataset that spans over 70 years, including the entire population during their neonatal period combined with daily local temperatures. Further, by using time-dependent survival analysis comparing neonatal mortality risks of neonates of the same age, and a nonlinear association between temperature and neonatal mortality, we have decreased the risk of confounding by age and captured the risk of both high and low temperatures.
Compared to more contemporary studies of climate vulnerability and neonatal mortality, our study lacked important confounders and effect modifiers. For example, we lacked information about birth weight and gestational age, two important factors that affect the risk of neonatal mortality and that might have varied due to the effect of high or low temperature exposure. Having had information about birth conditions (institution, home deliveries, etc.) would have further strengthened the analysis about the climate vulnerability of different social classes, especially regarding the workers who had a higher risk of neonatal mortality during warm extremes. However, our study brings insights into climate vulnerability of social classes during transitions from high to low neonatal mortality rates and shows that the results from historical studies might be used to improve neonatal health care in contemporary poor socioeconomic settings.
Data availability
The full dataset is available upon request at the Demographic Database, Umeå University. http://dx.doi.org/10.17197/U17004
Code availability
R-codes/scripts can be requested from co-author: Johan Junkka: johan.junkka@umu.se.
References
Allison, P. D. (1982). Discrete-time methods for the analysis of event histories. Sociological Methodology, 13, 61–98. https://doi.org/10.2307/270718
Amadi, H. O., Olateju, E. K., Alabi, P., Kawuwa, M. B., Ibadin, M. O., & Osibogun, A. O. (2015). Neonatal hyperthermia and thermal stress in low- and middle-income countries: a hidden cause of death in extremely low-birthweight neonates. Paediatrics and International Child Health, 35(3), 273–281. https://doi.org/10.1179/2046905515y.0000000030
Andersson, T., Högberg, U., & Bergström, S. (2000). Community-based prevention of perinatal deaths: lessons from nineteenth-century Sweden. International Journal of Epidemiology, 29(3), 542–548.
Basu, R., & Ostro, B. D. (2008). A multicounty analysis identifying the populations vulnerable to mortality associated with high ambient temperature in California. American Journal of Epidemiology, 168(6), 632–637. https://doi.org/10.1093/aje/kwn170
Bengtsson, T. (1999). The Vulnerable Child. Economic Insecurity and Child Mortality in Pre-Industrial Sweden: A Case Study of Västanfors, 1757-1850. European Journal of Population/Revue Européenne de Démographie,15(2), 117-151. https://doi.org/10.1023/A:1006215701608
Bengtsson, T. (2004). Life under pressure : mortality and living standards in Europe and Asia, 1700–1900. MIT.
Blumenshine, P., Egerter, S., Barclay, C. J., Cubbin, C., & Braveman, P. A. (2010). Socioeconomic disparities in adverse birth outcomes: a systematic review. American Journal of Preventive Medicine, 39(3), 263–272. https://doi.org/10.1016/j.amepre.2010.05.012
Breschi, M., & Livi-Bacci, M. (1997). Month of birth as a factor in children’s survival. In B. Desjardins (Ed.), Infant and Child Mortality in the Past Oxford: Clarendon Press.
Brändström, A. (1990). Från förebild till motbild. Spädbarnsvård och spädbarnsdödlighet i Jokkmokk. In S. Åkerman, Lundholm, K. (Ed.), Älvdal i norr. Människor och resurser i Luledalen 1300–1800 (pp. 307–351). Stockholm: Almqvist & Wiksell.
Brändström, A. (1993). Infant mortality in Sweden 1750–1950: Past and present research into its decline. Retrieved from Florence.
Burstrom, B., & Bernhardt, E. (2001). Social differentials in the decline of child mortality in nineteenth century Stockholm. European Journal of Public Health, 11(1), 29–34. https://doi.org/10.1093/eurpub/11.1.29
Cleveland, W. S., Gross, E., & Shyu, W. M. (1997). Local regression models. In J. M. Chambers & T. J. Hastie (Eds.), Statistical Models in S (pp. 309–376): Chapman & Hall.
Costa, D. L. (1998). Unequal at birth: a long-term comparison of income and birth weight. The Journal of Economic History, 58(4), 987–1009. https://doi.org/10.1017/S0022050700021690
Dalla-Zuanna, G., & Rosina, A. (2011). An analysis of extremely high nineteenth-century winter neonatal mortality in a local context of Northeastern Italy. European Journal of Population-Revue Europeenne De Demographie, 27(1), 33–55. https://doi.org/10.1007/s10680-010-9219-5
DDB. (2019a). Demographic Data Base. Retrieved from: https://www.cedar.umu.se/english/ddb/?languageId=1
DDB. (2019b). Project description: whats the weather got to do with it? . Retrieved from: https://doi.org/10.17197/U17004
De Boor, C. (1978). A practical guide to splines. Springer-Verlag.
Derosas, R. (2009). The joint effect of maternal malnutrition and cold weather on neonatal mortality in nineteenth-century Venice: an assessment of the hypothermia hypothesis. Population Studies-a Journal of Demography, 63(3), 233–251.
Edvinsson, S., Garðarsdóttir, Ó., & Thorvaldsen, G. (2008). Infant mortality in the Nordic countries, 1780–1930. Continuity and Change, 23, 457–485. https://doi.org/10.1017/S0268416008006917
Ekamper, P., Van Duin, C., Van Poppel, F., & Mandemakers, K. (2010). Heat waves and cold spells and their effect on mortality: an analysis of micro-data for the Netherlands in the nineteenth and twentieth centuries. [Heat Waves and Cold Spells and their Effect on Mortality: an Analysis of Micro-data for the Netherlands in the Nineteenth and Twentieth Centuries]. Annales de démographie historique, 120(2), 55–104. https://doi.org/10.3917/adh.120.0055
Ekamper, P., Van Poppel, F., Van Duin, C., & Garssen, J. (2009). 150 years of temperature-related excess mortality in the Netherlands. Demographic Research, 21, 385–425. Retrieved from <Go to ISI>://WOS:000270490700001.
Fellman, J., & Eriksson, A. W. (2001). Regional, temporal, and seasonal variations in births and deaths: the effects of famines. Social Biology, 48(1–2), 86–104. https://doi.org/10.1080/19485565.2001.9989029
Floud, R. (2011). The changing body : health, nutrition, and human development in the western world since 1700. . Cambridge University Press.
Gasparrini, A. (2014). Modeling exposure-lag-response associations with distributed lag non-linear models. Statistics in Medicine, 33(5), 881–899. https://doi.org/10.1002/sim.5963
Gasparrini, A. (2019). Extensions of the dlnm package, version 2.3.9. Retrieved from https://cran.r-project.org/web/packages/dlnm/vignettes/dlnmExtended.pdf
Gasparrini, A., Armstrong, B., & Kenward, M. G. (2010). Distributed lag non-linear models. Statistics in Medicine, 29(21), 2224–2234. https://doi.org/10.1002/sim.3940
Gyllenswärd, C. (1946). Dödföddheten och tidigdödligheten i Sverige : dess samband med nativitetsminskningen och dess förhållande vid olika former av förlossningsvård samt dess socialmedicinska och befolkningspolitiska betydelse : en undersökning. Stockholm.
Hare, E. H., Moran, P. A., & Macfarlane, A. (1981). The changing seasonality of infant deaths in England and Wales 1912–78 and its relation to seasonal temperature. Journal of Epidemiology and Community Health, 35(2), 77. https://doi.org/10.1136/jech.35.2.77
Hastie, T. J. (1997). Generalized additive models. In J. M. Chambers & T. J. Hastie (Eds.), Statistical Models in S (pp. 249–307): Chapman & Hall.
Healy, J. D. (2003). Excess winter mortality in Europe: a cross country analysis identifying key risk factors. Journal of Epidemiology & Community Health, 57(10), 784-789. https://doi.org/10.1136/jech.57.10.784
Hossin, M. Z., Björk, J., & Koupil, I. (2020). Early-life social and health determinants of adult socioeconomic position: associations and trends across generations. Journal of Epidemiology and Community Health, 74(5), 412–420. https://doi.org/10.1136/jech-2019-213209
Högberg, U. (2004). The decline in maternal mortality in Sweden: the role of community midwifery. American Journal of Public Health, 94(8), 1312–1320. https://doi.org/10.2105/ajph.94.8.1312
Karlsson, L. (2018). Indigenous infant mortality by age and season of birth, 1800–1899: Did season of birth affect children’s chances for survival?. International Journal of Environmental Research and Public Health, 15(1), 18. https://doi.org/10.3390/ijerph15010018
Karlsson, L., Lundevaller, E., & Schumann, B. (2019a). The association between cold extremes and neonatal mortality in Swedish Sápmi from 1800 to 1895. Global Health Action, 12(1), 1623609. https://doi.org/10.1080/16549716.2019.1623609
Karlsson, L., Lundevaller, E., & Schumann, B. (2019b). Season of birth, stillbirths, and neonatal mortality in Sweden: the Sami and non-Sami population, 1800–1899. International Journal of Circumpolar Health, 78(1), 1629784. https://doi.org/10.1080/22423982.2019.1629784
Karlsson, L., Lundevaller, E., & Schumann, B. (2020). Neonatal mortality and temperature in two Northern Swedish rural parishes, 1860–1899—the significance of ethnicity and gender. International Journal of Environmental Research and Public Health, 17(4). https://doi.org/10.3390/ijerph17041216
Knodel, J. E. (1988). Demographic behavior in the past : a study of fourteen German village populations in the eighteenth and nineteenth centuries. . Cambridge University Press.
Köhler, L. (1991). Infant mortality: the Swedish experience.Annual review of public health, 12(1), 177-193.
Kumar, V., Shearer, J. C., Kumar, A., & Darmstadt, G. L. (2009). Neonatal hypothermia in low resource settings: a review. Journal of Perinatology, 29(6), 401–412. https://doi.org/10.1038/jp.2008.233
Lalou, R., Bideau, A., Desjardins, B., & Brignoli, H. P. (1997). Infant and child mortality in the past.
Lawn, J. E., Blencowe, H., Oza, S., You, D., Lee, A. C. C., Waiswa, P., & Cousens, S. N. (2014). Every Newborn: progress, priorities, and potential beyond survival. The Lancet, 384(9938), 189–205. https://doi.org/10.1016/S0140-6736(14)60496-7
Lazuka, V., Quaranta, L., & Bengtsson, T. (2016). Fighting infectious disease: evidence from Sweden 1870–1940. Population and Development Review, 42(1), 27-52. https://doi.org/10.1111/j.1728-4457.2016.00108
Lithell, U. B. (1981). Breast-feeding and reproduction: Studies in marital fertility and infant mortality in 19th century Finland and Sweden (Doctoral dissertation, Acta Universitatis Upsaliensis).
Lunze, K., Bloom, D. E., Jamison, D. T., & Hamer, D. H. (2013). The global burden of neonatal hypothermia: systematic review of a major challenge for newborn survival. BMC Medicine, 11, 24. https://doi.org/10.1186/1741-7015-11-24
McEniry, M. (2011). Infant mortality, season of birth and the health of older Puerto Rican adults. Social Science and Medicine, 72(6), 1004–1015. https://doi.org/10.1016/j.socscimed.2010.08.026
Mullany, L. C. (2010). Neonatal hypothermia in low-resource settings. Seminars in perinatology, 34(6), 426–433. https://doi.org/10.1053/j.semperi.2010.09.007
Mullany, L. C., Katz, J., Khatry, S. K., LeClerq, S. C., Darmstadt, G. L., & Tielsch, J. M. (2010). Risk of mortality associated with neonatal hypothermia in southern Nepal. Archives of Pediatrics and Adolescent Medicine, 164(7), 650–656. https://doi.org/10.1001/archpediatrics.2010.103
Nilsson, H., & Edvinsson, S. (2000). Swedish towns during industrialization. Annales de démographie historique, 63–96. Retrieved from https://www.persee.fr/doc/adh_0066-2062_2000_num_1999_2_2168
Ohlander, A. S. (1994). Kvinnor, barn och arbete i Sverige 1850–1993: betänkande. Fritze.
Oris, M., Derosas, R., & Breschi, M. (2004). Infant and child mortality. Life Under Pressure: Mortality and Living Standards in Europe and Asia, 1700–1900. (pp. 359–398). MIT Press.
Preston, S. H., & Haines, M. R. (1991). Fatal years : child mortality in late nineteenth-century America. Princeton, N.J. Oxford: Princeton University Press.
Reid, A. (2001). Neonatal mortality and stillbirths in early twentieth century Derbyshire, England. Population Studies, 55(3), 213-232. https://doi.org/10.1080/00324720127696
Scalone, F., & Samoggia, A. (2018). Neonatal mortality, cold weather, and socioeconomic status in two northern Italian rural parishes, 1820–1900. Demographic Research, 39, 525–560. https://doi.org/10.4054/DemRes.2018.39.18
Schumann, B., Häggström Lundevaller, E., & Karlsson, L. (2019). Weather extremes and perinatal mortality - seasonal and ethnic differences in northern Sweden, 1800–1895. PLoS ONE, 14(10), e0223538. https://doi.org/10.1371/journal.pone.0223538
Sköld, P., & Axelsson, P. (2008). The northern population development; colonization and mortality in Swedish Sapmi, 1776–1895. International Journal of Circumpolar Health, 67(1), 27–42. Retrieved from <Go to ISI>://WOS:000254724500005.
Sköld, P., Axelsson, P., Karlsson, L., & Smith, L. (2011). Infant mortality of Sami and settlers in Northern Sweden: the era of colonization 1750-1900. Global Health Action 4. https://doi.org/10.3402/gha.v4i0.8441
SMHI (2021). Open Data. Retrieved from https://www.smhi.se/data/utforskaren-oppna-data/
Solar, O., & Irwin, A. (2010). A conceptual framework for the action on the social determinants of health. WHO Document Production Services.
Son, J.-Y., Lee, J.-T., & Bell, M. L. (2017). Is ambient temperature associated with risk of infant mortality? A multi-city study in Korea. Environmental Research, 158, 748–752. https://doi.org/10.1016/j.envres.2017.07.034
Strand, L. B., Barnett, A. G., & Tong, S. (2011). The influence of season and ambient temperature on birth outcomes: a review of the epidemiological literature. Environmental Research, 111(3), 451–462. https://doi.org/10.1016/j.envres.2011.01.023
Stråth, B. (2012). Sveriges historia. : [kungarna och eliterna, unionen Sverige-Norge, borgerligheten, kvinnorörelsen och könsrollerna, riksdagsreformen, arbetarrörelsen, massmedierna, nyodlingsprojekten, industrialiseringen, emigrationen, befolkningsökningen, fattigdom och välfärd, vetenskap och konst] 1830–1920. Stockholm: Stockholm : Norstedt.
Sundin, J., & Willner, S. (2007). Social change and health in Sweden : 250 years of politics and practice. [Stockholm]: Swedish National Institute of Public Health.
Swedish Meteorological and Hydrological Institute, S. (2019). Retrieved from https://www.smhi.se
Thorvaldsen, G. (2008). Was there a European breastfeeding pattern? History of the Family, 13(3), 283–295. https://doi.org/10.1016/j.hisfam.2008.08.001
Van De Putte, B., & Miles, A. (2005). A class scheme for historical occupational data: the analysis of marital mobility in industrial cities in 19th century Flanders and England. Historical Methods, 38(2), 61-92.
Van, Leeuwen., M. (2002). HISCO : historical international standard classification of occupations. Leuven: Leuven : Leuven University Press.
Victora, C. G., Vaughan, J. P., & Barros, F. C. (1985). The seasonality of infant deaths due to diarrheal and respiratory diseases in southern Brazil, 1974–1978. Bull Pan Am Health Organ, 19(1), 29–39. Retrieved from https://www.ncbi.nlm.nih.gov/pubmed/4027452
Westberg, A., Engberg, E., & Edvinsson, S. (2016). A unique source for innovative longitudinal research: The POPLINK database. Historical Life Course Studies, 3, 20-31.
Woods, R. (2009). Death before birth : fetal health and mortality in historical perspective. Oxford University Press.
Xu, Z., Etzel, R. A., Su, H., Huang, C., Guo, Y., & Tong, S. (2012). Impact of ambient temperature on children’s health: a systematic review. Environmental Research, 117, 120–131. https://doi.org/10.1016/j.envres.2012.07.002
Zetterström, R., & Eriksson, M. (1987). Hälsa och social klass : spädbarnsdödlighet och graviditetsutfall. Socialmedicinsk Tidskrift, 64(1).
Funding
Open access funding provided by Umea University. This study was supported by the Swedish Foundation for Humanities and Social Sciences (Riksbankens Jubileumsfond), Grant number P17-0033:1.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Ethics approval
Ethical approval was obtained from the regional ethics committee (Regionala etikprövningsnämnden i Umeå), Number 2017/509-31.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Appendix
Appendix

SES distribution over time and region

Sensitivity analysis, HR and CI of association between temperature and neonatal mortality, adjusting for a seasonal effect varying by region
Rights and permissions
Open access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Karlsson, L., Junkka, J., Schumann, B. et al. Socioeconomic disparities in climate vulnerability: neonatal mortality in northern Sweden, 1880–1950. Popul Environ 43, 149–180 (2021). https://doi.org/10.1007/s11111-021-00383-9
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11111-021-00383-9