
Abstract
This paper examines the association between religious identity, religiosity (internal vs external), and psychological well-being during the COVID-19 pandemic. Data from two cross-sectional surveys were used to test these associations among Malaysians from the three major religious groups—Muslims, Christians, and Buddhists—as well as mixed qualitative coding on illness beliefs and helpful resources. During the pandemic, higher religiosity was associated with less perceived stress, external religiosity was negatively associated with stress, and internal religiosity was positively associated with life satisfaction among young adults. Thematic coding also confirmed a variety of illness beliefs and helpful resources relevant to social and religious norms. Different pathways of religious coping were utilized during the pandemic.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Extant research suggests that religious support and resources could be beneficial to one’s psychological well-being during the COVID-19 pandemic. In Malaysia, a multiethnic Southeast Asian nation with a population of 32.4 million, Islam is the official religion and is practiced by 63.5% of the population (Department of Statistics Malaysia, 2022). Malays, the dominant ethnic group in Malaysia (50.8%), make up most of the Islam practitioners given that they are legally required to be registered as Muslim at birth. The second largest religion practiced in Malaysia, Buddhism (18.7%), is typically endorsed by the second largest ethnic group in Malaysia, the Chinese, who make up 23.3% or the overall population (Department of Statistics Malaysia, 2022). The third largest religion is Christianity (9.1%), followed by Hinduism (6.1%). Hinduism is largely practiced by Indians, who make up 6.7% of the Malaysian population. These percentages reflect a high intersection between religion and ethnicity in Malaysia (Department of Information, Ministry of Communications and Multimedia, Malaysia, 2015), which provides a unique cultural backdrop for studying the impact of ethno-religions on the psychological well-being of a variety of believers.
Religion, religiosity, and psychological well-being
The influence of religion on one’s psychological processes can shape one’s health perceptions and coping behaviors (Milstein et al., 2019). While organized religions involve institutionalized membership and doctrines that vary across world religions, religiosity is a psychological concept that captures one’s degree of endorsement of the religious practices and beliefs of a particular religion. Past findings suggest that one’s degree of religiosity or spirituality plays a prominent role in shaping well-being regardless of religious group membership (Abdel-Khalek, 2019; Steffen et al., 2017; Villani et al., 2019). For instance, religious individuals tend to better utilize religious resources to cope with psychological crises, which contributes to better mental health outcomes (Khodaveirdyzadeh et al., 2016; Oman & Syme, 2018; Pargament et al., 2000; Weber & Pargament, 2014). Additionally, the psychological benefits of religious coping have been shown in a clinical context. For instance, Roger and Hatala (2018) found that patients with chronic illnesses who practice more religious coping report better quality of life, sense of meaning, mental health, acceptance, source of comfort, and hope.
The impact of religiosity on personal illnesses can be explained by the self-regulatory model (Leventhal et al., 1998). The model proposed that illness-related perceptions of, for example, consequences, timeline, personal control, treatment control, identity, concern, and emotional response are significantly correlated with anxiety and depression (Zhang et al., 2016). However, cognitive appraisal and coping strategies serve as the self-regulated pathway between illness representation and mental health outcomes. Therefore, higher religiosity reduces the psychological distress that arises because of illness-related perceptions.
Findings from several studies conducted with Malaysian populations (Ahmadi et al., 2019; Shaw et al., 2018; Ting & Ng, 2012) support the important contribution of religiosity and spirituality to an individual’s health beliefs and behaviors. Recently, Tan et al. (2020) found that a stronger belief in a higher power was associated with reduced psychological distress among Malaysian older adults. There is also evidence of the utility of religious coping (external vs internal; positive vs negative) in promoting physical and psychological well-being among Malaysians during the COVID-19 pandemic (Che Rahimi et al., 2021; Ting et al., 2021). Furthermore, illness perception and religious coping are heavily influenced by religious beliefs. A recent systematic review of pandemic perceptions (Yap et al., 2022) also found that different religious traditions hold differing beliefs regarding the transmission of infectious diseases such as AIDS. For example, Malay Muslims believe that illness and suffering are trials from God by which one’s sins are removed and that they are a part of one’s life journey to an everlasting world (Attum et al., 2022). Illnesses tend to be perceived as opportunities for spiritual growth and rewards (Al-Khayat, 2004). For Buddhists in Malaysia, the beliefs of karma and reincarnation lead to the perception that illness and suffering are the results of sin in the believer’s past life (Ahmad, 2007; Samuels, 2016; Tang, 2015). Taken together, the evidence suggests that there is a possibility of an interaction effect between religious traditions and different types of religiosities on the psychological well-being of believers, and Malaysia provides an ideal context to test such a model since there is a high but diverse representation of religious identity with major religious traditions. Also, the effect of pandemic exposure on individuals’ religiosity remains understudied.
Research aims and questions
The aim of the current research was to examine the associations between religious identity, religiosity, and psychological well-being during the COVID-19 pandemic. In Study 1, we adopted a mixed-methods approach to examine (1) the degree of religiosity and psychological well-being and their associations among the major religious groups in Malaysia during the first COVID-19 pandemic lockdown and (2) the pandemic-relevant beliefs—perceptions of illness and helpful resources—of each religious group. In Study 2, we tested whether the association between religiosity and psychological well-being was moderated by exposure to the pandemic.
Study 1: Methods
The purpose of Study 1 was to examine whether the major religious groups in Malaysia varied in their degree of religiosity and psychological well-being during the COVID-19 pandemic. Specifically, we tested quantitatively whether perceived stress varied between individuals who identified as Muslim, Buddhist, and Christian and whether the stress varied according to their self-reported degree of religiosity. Narratives on illness beliefs and helpful resources by the religious believers were also solicited to provide a richer and more comprehensive interpretation of the quantitative results.
Participants and procedure
Data for Study 1 were collected using a cross-sectional online survey (designed by the first author’s lab) that was hosted on Qualtrics during the Movement Control Order implemented in Malaysia from April–July 2020. This study was approved by the Human Research Ethics Committee of the authors’ institution. Participants were recruited using convenience sampling and informed at the start of the survey that their completion of the questionnaire implied consent. Inclusion criteria were (1) Malaysian citizens residing in Malaysia during the Movement Control Order and (2) age 18–66 years. Study 1 only extracted and analyzed the 608 Malaysian citizens who reported affiliation with one of the three major religious groups (Buddhist, Christian, or Muslim) in Malaysia. Four did not report their gender and were excluded from the quantitative analyses (N = 604). The responses from all participants were included in the qualitative analyses.
The 604 participants included in the quantitative analyses were 34.7 years old on average and mostly identified as female, of Chinese ethnicity, and Christian (see Table 1). About half of the Chinese participants reported being either Buddhist (49.3%) or Christian (50.5%). All Malays identified as Muslims, and all Indians identified as Christians. As for the rest of the participants, 9.1% identified as Buddhist, 77.3% as Christian, and 13.6% as Muslim.
Measures
All online survey items were provided in English, Mandarin, and Malay, which are the most common languages among Malaysians. The items were translated by a trilingual research team and backtranslated by Mandarin and Malay native speakers with psychology-related academic qualifications. The survey consisted of the following sections.
The five-item Duke University Religion Index (DUREL; Koenig & Büssing, 2010) was used to measure the degree of religiosity. Participants rated their agreement (1 = definitely not true of me, 5 = definitely true of me) with three items that tapped into intrinsic or subjective religiosity (i.e., “In my life, I experience the presence of the Divine,” “My religious beliefs are what really lie behind my whole approach to life,” “I try hard to carry my religion over into all other dealings in life”). The other two items, which were rated on a scale of 1 (once a year or less) to 5 (more than once per week) captured engagement in organized or public religious activity (“How often do you attend church or other religious meetings?”) and engagement in nonorganized or private religious activity (“How often do you spend time in private religious activities, such as prayer, meditation, etc.?”). The five item scores were averaged to form the overall religiosity score (α = .89). Scores of the three items that tapped into intrinsic religiosity were averaged to form the intrinsic religiosity score (α = .87). The remaining two items were examined individually as single-item measures of public practice and private practice.
Stress was measured using the Perceived Stress Scale (PSS; Cohen et al., 1983). Participants rated 10 items (e.g., “In the last month, how often have you felt nervous and stressed?”) on a scale of 0 (never) to 4 (very often). After reverse-scoring items four, five, seven, and eight (e.g., “In the last month, how often have you felt that you were on the top of things?”), the 10 item scores were averaged to form a stress score (α = .86).
To elicit pandemic-relevant beliefs, participants were presented with two open-ended textual questions. First, we adapted a question from the Brief Illness Perception Questionnaire (BIPQ; Broadbent et al., 2006) to the pandemic context and asked participants to indicate what they believed to be the key causes of COVID-19 (i.e., “Please list in rank order the three most important factors that you believe caused the COVID-19 pandemic”). The second question asked participants to state the resources that they perceived as helpful for them during the lockdown (i.e., “What do you think will be helpful for you to overcome the challenges mentioned above? Please describe in as much detail as possible”). The participants were allowed to type their responses in their mother tongue, such as Mandarin or Bahasa Malaysia, as well as in English.
Qualitative coding
Multilingual research assistants coded and translated the open-ended written responses regarding illness beliefs and helpful resources using an inductive-deductive thematic analysis approach following Braun and Clarke (2006) and Hill et al.’s (1997) consensus qualitative research (CQR) guidelines. Morse (2015) rigor in qualitative inquiry criteria were used to guide the coding process, as follows:
-
1.
To produce an overall data table, the data collected were organized and entered into a spreadsheet prepared with multiple rows and columns (Vaughn & Turner, 2016). Using the repeated reading technique of CQR (Hill et al., 1997), two research assistants independently read through the participants’ responses several times for familiarization. The coding process was carried out manually. First-level codes were assigned to meaningful phrases and keywords in the responses.
-
2.
Next, the first-level codes were analyzed and integrated into second-level coding called subthemes. The subthemes were grouped into third-level main themes inductively and deductively. A three-tier codebook was set up to ensure consistency and reduce redundancy of codings.
-
3.
To increase internal consistency, two research assistants and the principal investigator independently reviewed and coded the data. Then, discrepancies were rectified through consensus discussion among the two coders and the principal investigator, who acted as the auditor. Following that, all codes and themes were evaluated and analyzed based on their internal homogeneity and external heterogeneity (Patton, 1990). Internal homogeneity implies that data within a theme should be cohesive and meaningful, whereas external heterogeneity suggests that data within a theme should vary and be distinguishable from all other themes (Braun & Clarke, 2006).
-
4.
Finally, the frequency and percentages of responses per theme and subtheme across the three religious groups were computed and tabulated.
Study 1: Results
The means, standard deviations, and frequencies for all variables are summarized in Table 1. See Table S1 in the supplementary materials for bivariate correlations between continuous and dichotomous variables.
Religious group differences in religiosity and stress
One-way independent-measures analyses of variance (ANOVA) were run to examine the difference in religiosity and psychological well-being across the religious groups, and their results are summarized in Table 2. Results revealed that Christians were significantly older and more religious overall than Buddhists and Muslims (ps < .01). Muslims were marginally older than Buddhists (p = .055). Buddhists were less religious overall than Muslims (p < .001). Regarding intrinsic religiosity and private practice, Buddhists were significantly lower than Muslims and Christians (ps < .001). No differences in intrinsic religiosity and private practices were observed among Muslims and Christians (ps > .10). Public practices were significantly higher among Christians than Muslims and were higher among Muslims than Buddhists (ps < .001).
Buddhists were significantly more stressed than Christians (p < .001) and marginally more stressed than Muslims (p = .052). No differences were found between Christians and Muslims (p > .10) in terms of stress level. Given that age varied significantly by religious group and was significantly associated with religiosity (see Table S1 in the supplementary materials), an analysis of covariance (ANCOVA) was run to examine religious group differences in stress, with age controlled for as covariate. ANCOVA results revealed that religious group differences in stress were no longer significant after controlling for age, F(2, 600) = 2.46, p = .086, np2 = .008. This suggests that age may be a key driver in the religious group differences in stress. That is, Christians may be less stressed than Buddhists, not because of their religious beliefs and practices but because they were generally older than Buddhists in the current study.Footnote 1
The relationship between religiosity and stress
Multiple linear regression analyses were run to examine the role of the degree of religiosity in stress. Given the significant association between age and stress, age was included as a covariate in the models. The role of each component of religiosity (i.e., overall religiosity or the composite score, intrinsic religiosity, private practice, and public practice) was tested in separate models. These models were tested for multicollinearity, multivariate outliers, normality, and homoscedasticity of residuals, and all assumptions were met. As shown in Table 3, overall religiosity was negatively associated with stress when age was controlled for. However, it appears that this association is primarily driven by the public and private practice of religiosity (ps < 0.05) rather than intrinsic religiosity, p = .067.
B represents unstandardized regression coefficients. CI represents the lower and upper limits of the confidence intervals of the unstandardized regression coefficients. β represents the standardized coefficients. A significant t-statistic indicates that that the regression coefficient varied significantly from zero, i.e., a significant association between predictor and outcome variables. The F-ratio, its accompanying df (degrees of freedom) and R2 are indicators of model fit.
We also conducted bivariate correlations between religiosity variables and stress separately for participants aged 18–30 years and those aged above 30 years and found consistent associations between religiosity (i.e., overall religiosity, public practice, and private practice) and stress.
Causes of the pandemic as perceived by religious believers
In sum, 608 participants provided 1,841 open-ended responses to the question on the perceived causes of the COVID-19 pandemic. As shown in Table 4, people most commonly (30.09%) believed the pandemic was a consequence of human behaviors, which included poor public health behavior (e.g., “lack of hygiene,” “no social distancing,” “not washing hands enough”), unusual eating choices and behavior (e.g., “consuming wildlife,” “consumption of exotic meat”), and the public’s failure to follow government protocols (e.g., “citizens not following MCO [Movement Control Order] rules,” “human disobedience”). The second most mentioned theme (25.53%) was related to people’s poor attitudes. This is defined as poor awareness and education (e.g., “lack of awareness and education regarding the virus and its severity,” “awareness in society not enough”), flawed human character (e.g., “arrogance,” “selfishness of humans”), and human ignorance (e.g., “ignorant individuals who refused to be tested,” “human negligence”). The third-ranked major theme (13.58%) encompassed sociopolitical reasons, which included ineffective government (e.g., “no borders security,” “government’s effectiveness in decision and action”), human-caused disaster (e.g., “bioweapons,” “man-made virus”), and poor medical resources (e.g., “insufficient medical equipment for front-line health personnel,” “lack of funding for preventive measures and healthcare in general”). Other possible explanations of the COVID-19 pandemic included social factors (12.38%) such as social gatherings and human interactions. Some participants adopted a medical explanation (11.24%) as the cause of the pandemic, such as “having a poor immune system, virus transmission, infections, and bio-mutation.” A minority (4.78%) endorsed an ecological explanation defined by environmental problems, natural processes, animal contact, overpopulation, and natural disasters. Only 2.39% of the overall sample adopted religious/spiritual explanations for the pandemic, such as human karma or sin, the will of God, or a punishment from God.
Overall, though these findings suggest a universal tendency among participants to attribute the cause of the pandemic to human behaviors and attitudes, the percentages of the themes varied across the three religious groups. More Muslims (37.94%) believed that human behaviors caused the pandemic compared to Buddhists (28.51%) and Christians (28.81%). Muslims also reported the lowest percentage in human attitude themes (18.09%). This is in accordance with the Muslim belief and emphasis on external behavioral adherence in Islam doctrine known as the Virtuous Deed (Religion of Islam, 2009). Compared to Buddhists and Muslims, Christians were more likely to identify medical explanations as a cause of the pandemic (13.46%) and less likely to mention social factors (9.33%). Christians (3.54%) and Muslims (2.84%) also endorsed a higher percentage of religious/spiritual explanations of the pandemic (3.54%) than Buddhists (0.84%) did. This pattern of results parallels our quantitative finding that the Christians and Muslims in our study were generally more religious than the Buddhists.
Helpful resources as perceived by religious believers
A total of 965 written responses were recorded for the perceived helpful resources, as shown in Table 5. The resource that was perceived to be the most helpful was self-management coping behaviors (27.25%), which included practicing self-care behaviors (e.g., “going outside to breathe some fresh air,” “consume healthy food,” “increase frequency of sleep”), practicing safety precautions (e.g., “social distancing,” “stay at home,” “get tested”), and investing in self-growth (e.g., “learn to be independent,” “cook at home”). Personal cognitive adjustment was the second major theme (16.06%), and this included establishing a sense of control (e.g., “focus on what needs to be done,” “remain as calm as possible,” “take things slow, one at a time”), having a positive mindset (e.g., “stay optimistic,” “prepare your mental attitude in the right mindset”), and being adaptive (e.g., “adapt to new routines,” “learn to adapt the new style of learning”). The third most endorsed theme (14.30%) was social and emotional support, which included support from family (e.g., “understanding of family members,” “help from partner”), support from friends (e.g., “peer support”), and general support (e.g., “my cat”). Other possible helpful resources were governmental actions (9.84%), which included government aid and flexibility in mobility; and religious/spiritual resources (9.74%), which included private religious activities, having faith in God, and God’s wisdom. Less cited resources were job support (4.46%; e.g., flexible work arrangements, employer support), financial resources (4.15%; e.g., personal finance management), public cooperation (4.04%; e.g., public compliance with government protocols), living necessities (3.01%; e.g., online shopping and delivery services), career opportunities (2.90%; e.g., a stable career and market), academic support (2.80%; e.g., better communication from the school), and medical resources (1.45%; e.g., development of a cure).
Noticeable differences were found when comparing the percentages of the aforementioned themes across the three religious groups. More Buddhists (31.39%) reported self-management coping behaviors compared to Christians (25.05%) and Muslims (23.88%). Christians were least likely to propose personal cognitive adjustment (13.38%) but most likely to propose religious/spiritual resources (17.41%) as potentially useful resources. This is aligned with the quantitative finding that Christians had the highest religiosity score in Studies 1 and 2. In addition, the Muslim group relied more on social and emotional support (17.91%) and governmental actions (11.19%) than the two other religious groups.
Study 1 summary and justification for Study 2
Our preliminary findings from Study 1 suggested that Buddhists were particularly vulnerable to stress and generally less religious than Christians and Muslims during the COVID-19 pandemic. However, further analyses revealed that these differences were predominantly due to the difference in age of the participants in the religious groups. While there were no religious group differences in stress, we found significant associations between religiosity and stress. More externally oriented religiosity, in particular, was associated with less perceived stress.
Despite Study 1’s supporting the role of religiosity in psychological well-being among Malaysians during the pandemic (Che Rahimi et al., 2021; Ting et al., 2021), it remains unclear from Study 1 whether the protective function of religiosity was specific to the context of the pandemic. Moreover, Study 1 found that the younger age group seemed to suffer more stress during the pandemic. Hence, a separate study that focuses on the younger generation’s religiosity and psychological well-being before and during the pandemic would complement Study 1.
Study 2: Methods
To complement the scope of Study 1, Study 2 zoomed in on young adult populations, examined depressive symptoms and satisfaction with life as outcome variables, and tested whether the associations between religiosity and psychological well-being were moderated by the presence of the pandemic.
Participants and procedure
Data used in Study 2 were collected from a cross-sectional convenience sample of Malaysian young adults aged 18–30 years as part of a larger project on the topic of “interpersonal experiences and well-being among Malaysian young adults” (archived by the second author’s lab), which was approved by the ethics committee of the authors’ institution. The inclusion criteria were (1) Malaysian by nationality, (2) age 18–30 years, (3) fluent and able to complete a survey in English (the survey was presented only in English), and (4) comfortable responding to questions about their close relationships and sexual experiences. We were able to test the role of the pandemic as a moderator because one group of participants completed the study in June–August 2019 (Phase 1: Pre-pandemic) while a separate group of participants completed the study in May–July 2020 (Phase 2: During the pandemic).
Of the 780 recorded responses to the survey, 159 were duplicates or incomplete responses and 120 did not identify as either Muslim, Buddhist, or Christian. Our final sample comprised 235 participants who were on average 20.95 years old in the pre-pandemic group and 266 participants with a mean age of 23.06 years in the pandemic group. More than half of the participants from the two groups identified as female and of Chinese ethnicity (see Table 1). Of the ethnically Chinese participants, 67.5% identified as Buddhist, 31.9% as Christian, and 0.6% as Muslim. All Malays identified as Muslim. All but one Indian identified as Christian (97.1%; 2.9% Muslim). The remainder of the participants were 21.2% Muslim, 10.5% Buddhist, and 68.4% Christian.
Measures
Similar to Study 1, the DUREL (Koenig & Büssing, 2010) and PSS (Cohen et al., 1983) were used to measure religiosity and perceived stress. Depressive symptoms over the past two weeks were measured using the Patient Health Questionnaire (PHQ-9; Kroenke et al., 2001), which consisted of nine items (e.g., “Hopeless”) rated on a scale from 0 (not at all) to 3 (nearly every day). To measure life satisfaction, participants completed the Satisfaction with Life Scale (SWLS; Diener et al., 1985), where they rated their agreement with five statements (e.g., “The conditions of my life are excellent”) on a 7-point scale (1 = strongly disagree, 7 = strongly agree). Item scores were averaged to compute variable scores, and all alpha values were above 0.80 (see Table S2 in the supplementary materials).
In addition to age and gender, participants in Study 2 also reported their relationship status (i.e., in a committed relationship or not), whether they had experienced any health difficulties in the past 12 months on a scale of 1 (no) to 6 (yes, and it has caused my inability to carry out my daily activities), and their subjective socioeconomic status on a scale of 1 (low) to 10 (high) using the MacArthur Scale of Subjective Social Scale (Adler et al., 2000) for sociodemographic variables.
Study 2: Results
Religious group differences in religiosity and psychological well-being
Independent-measures ANOVAs were run separately for the pre-pandemic and pandemic groups. As shown in the middle and bottom rows of Table 2, religious group differences were found for religiosity in all participants but were found only among the pre-pandemic group for depression and satisfaction with life. No religious group differences were found for pre-pandemic stress or any of the psychological well-being indices during the pandemic.
Pre-pandemic, Muslim young adults reported more depression (p = .002) and less satisfaction with life (p = .029) than Buddhists. Muslims were marginally more depressed than Christians (p = .051). Overall and intrinsic religiosity was lower among Buddhists than among Muslims and Christians (ps < .001). Public religious practice among Muslims was higher than among Buddhists (p = .004) and lower than among Christians (p < .001). Private religious practice was significantly lower among Buddhists than among Muslims and Christians (ps < .001).
In the pandemic group, Buddhists consistently scored lower than Muslims and Christians in overall and intrinsic religiosity (ps < .001). Public practice of religion was significantly higher among Christians compared to Muslims and Buddhists (ps < .001). Private practice, while consistently lower among Buddhists compared to Muslims and Christians, was also lower among Christians than among Muslims (p < .001).
Exposure to the pandemic as a moderator of the association between religiosity and psychological well-being
To examine whether the association between religiosity and psychological well-being differed between the pre-pandemic group versus the pandemic-exposed group, moderation analyses using the PROCESS macro for SPSS (Hayes, 2022; Model 1) with 10,000 bootstrapped resamples accelerated at 95% confidence interval were employed. Subjective socioeconomic status, gender, relationship status, and health difficulties, correlated with at least one of the psychological well-being markers (see Table S2 in the supplementary materials for bivariate correlations), were included as covariates in the analyses. Similar to Study 1 analyses, the role of each component of religiosity was tested in separate models, and these models were applied for stress, depression, and satisfaction with life as dependent variables. The examination of statistical assumptions relevant to a hierarchical linear regression for all models revealed no violations of assumptions. Results from these analyses are summarized in Table 6.
All analyses initially included gender (0 = male, 1 = female), relationship status (0 = not in committed relationship, 1 = in committed relationship), subjective SES, and health difficulty as covariates. However, relationship status was not a significant predictor of stress and gender was not a significant predictor of satisfaction with life, so these were removed from the final models.
After controlling for the proposed covariates, the association between religiosity and depression was nonsignificant in both the pre-pandemic and pandemic groups. Depression was higher among those who experienced more health difficulties within the past year, who were not in a committed relationship, who were of lower socioeconomic status, and who completed the study during the pandemic rather than pre-pandemic.
As for stress and satisfaction with life, there was a significant moderation of pandemic exposure on the association between religiosity and psychological well-being, as indicated by significant interactions between religiosity markers and the study phase. Simple slopes analyses revealed that overall religiosity was negatively associated with stress (b = − 0.08, p = .015) and positively associated with satisfaction with life (b = 0.28, p < .001) among participants who were exposed to the pandemic. These associations were not significant among those who completed the study before the pandemic (stress: b = 0.02, p = .625; satisfaction with life: b = 0.05, p = .474).
Pandemic exposure also significantly moderated the association between the degree of private religious practice and satisfaction with life as well as the association between the degree of public religious practice and stress. As illustrated in Fig. 1, individuals who reported more public practice of religion tend to be less stressed and those who reported more private religious practice tend to be more satisfied with their lives during the pandemic. These associations were nonsignificant among individuals who completed the study before the pandemic.

Simple slopes analyses: a The association between public practice and stress by pandemic exposure; b The association between private practice and satisfaction with life by pandemic exposure
Study 2 summary
Findings from Study 2 largely supported those from Study 1: (1) Buddhists were found to be the least religious in their intrinsic beliefs and practices compared to Christians and Muslims, (2) religious groups did not differ in their perceived stress before or during the pandemic, and (3) the significant association between religiosity and psychological well-being during the pandemic appear to be primarily driven by extrinsic religiosity and not intrinsic religiosity. Religious groups were found to differ in other markers of psychological well-being. Muslims reported the most depressive symptoms and the least satisfaction with life. However, this was unique to the pre-pandemic sample; these differences were not found in the pandemic sample. Lastly, our findings from Study 2 also suggest a nonsignificant contribution of religious beliefs and practices to depressive symptoms.
Discussion
Even though religiosity has often been found to be associated with positive health outcomes, its pathways to different psychological well-being markers during the COVID-19 pandemic have not been fully examined – particularly in non-Western and multireligious populations. Findings from the current study contribute to the literature on the psychology of religion by affirming the positive link between religiosity and mental health outcomes in three major religious groups (Christian, Muslim, and Buddhist) from a Southeast Asian country (Malaysia). We found that perceived stress did not vary significantly by religious identification (group membership) after accounting for age effects. In all three religious groups, religious practices played a more important role than intrinsic religiosity (belief in God or a higher power) in promoting psychological well-being. In particular, more public religious practice was associated with lower stress while more private religious practice was associated with satisfaction with life. Among young adults, the protective benefits of religious practices were only present in those who completed the study during the COVID-19 pandemic and not in those who completed the study before the pandemic. It is possible that the especially heightened existential crisis and mental vulnerability of the young adult generation during the pandemic (Liu et al., 2020; Organisation for Economic Co-operation and Development, 2020; Tomaszek & Muchacka-Cymerman, 2020; Wangchuk, 2021) motivated them to turn to religious resources. Religious practices provide new meaning to life in times of uncertainty and loss of control, which could in turn alleviate the mental stress and trauma experienced during the pandemic (Spitzenstätter & Schnell, 2020; Van Tongeren & Showalter Van Tongeren, 2021; Yıldırım & Arslan, 2021). Moreover, private religious practices such as prayer and worship, which typically entail some mindfulness practice, may assist with the reduction of stress at a biological level (AlAbdulwahab et al., 2013; Rosmarin et al., 2011).
Theoretical implications for religious coping
We propose a more nuanced religious coping model (see Fig. 2) to explain the relationship between religious practices and mental health outcomes based on our findings. The literature on religious coping has generally assumed that all religious practices can be utilized as a way of positive coping as long as it is approach- rather than avoidance-driven (Krägeloh et al., 2012; Thomas & Barbato, 2020). There is also evidence that intrinsic religiosity may be a more effective form of religious coping than extrinsic religiosity (Banazadeh et al., 2019; Chau et al., 1990). However, our findings challenge the universality of these assumptions. We found that the significant associations between religiosity and psychological well-being during the pandemic appear to be primarily driven by private religious practices for satisfaction with life and by public religious practices for stress. These findings imply that not all aspects of religiosity were contributing to the same domains of psychological well-being during the pandemic. This is especially true for more traditional Asian regions where external manipulation of cognitive resources and a concrete thinking style are privileged (Ting & Sundararajan, 2018). Public religious practices (such as attending mosque or temples) are still important in regulating the stress pathway as they emphasize communal participation in rituals. The presence of religious icons and the guidance of religious leaders, according to semiotic analysis, has an effect on emotion regulation (Sundararajan, 2011) and hence could be associated with the stress regulation pathway in coping theory (Sundararajan et al., 2022). On the other hand, private religious practices such as private prayer were not associated with stress regulation but were associated with positive satisfaction with life, which is part of one’s subjective well-being (Pavot & Diener, 1993). The subjective evaluation pathway takes self-reflection and metacognition in self-appraisal (Scheer & Jansen, 2018; Toffalini et al., 2014), hence private religious practices (internal manipulation of cognitive resources) have a more direct effect on this upper-level pathway. Nevertheless, our findings suggest that both pathways became more active and efficient during the COVID-19 pandemic, particularly among younger-generation Malaysians.

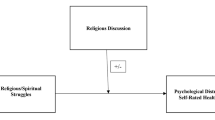
Proposed conceptual model of religious coping during the COVID-19 pandemic
Diversity in rationality among religious groups
While our quantitative analyses generally found differences among religious groups in the degree of religiosity but not psychological well-being, our qualitative findings shed light on how the different religious groups perceived the cause of the pandemic and what they considered to be potentially helpful resources. Traditionally, it has been explained that religious groups’ perception of illnesses is shaped by their worldviews, doctrines, and values (external vs internal attributions) and that their illness beliefs also lead to different perceived helpful resources (external vs internal; religious vs secular). Instead, we propose an ecological rationality model to explain this diversity of religious rationality (strong-ties vs weak-ties rationality) among Malaysian believers (Ting et al., 2021). Though Malaysia as a nation has been found to be oriented to collectivism and interdependence due to its Asian heritage (Hofstede, 1980), the religious diversity within the countries can be plotted on the spectrum of high vs low strong-ties ecological orientation. In the literature, Islam tends to resemble the ancestral niche of kinship networks, whereas Christianity is more representative of the weak-ties niche with inclusion of strangers (Thong et al., 2023; Yap et al., 2022). In Malaysia, Islam is the ethno-religion (strong-ties) of the Malay-majority population, for whom religious membership is automatically granted from birth (if one’s parents have already converted to Islam; Samuri & Quraishi, 2014). Simply put, a strong-ties ecology stems from and is rooted in local communities involving familiar, close kinship networks (e.g., extended family, tribal villagers, and clan members), where membership is typically determined by geography, ethnicity, and bloodlines (Sundararajan, 2020). In contrast, a weak-ties religion (such as Christianity) is founded on the ideal of the inclusion of strangers, thereby privileging weak-ties (non-kin) networks that have the transnational capacity to reach global membership (Granovetter, 1973). Although Buddhism and Islam also have a concern for and inclusiveness of strangers, they focus less on the weakening of kinship-based relations such as extended family compared to Christianity (Schulz et al., 2019). This is shown in our study; compared to their counterparts, a higher percentage of Muslims attributed the pandemic to human behavioral problems and found externally manipulated strategies such as behavioral coping and social and emotional support from family important. In contrast, a higher percentage of Christians adopted abstract explanations of the pandemic (medical explanations and religious explanations) and perceived personal adjustment (weak-ties rationality) as helpful during the pandemic. This pattern of religious difference in rationality was also consistent with a recent empirical study conducted among three religious communities of the indigenous people in Malaysia on changes in their ecological rationality (Thong et al., 2023).
Mental health implications for believers
The study sheds light on the importance of religious practice in regulating pandemic stress, especially among young adults in Malaysia. Our findings suggest that private religious practices (such as personal meditation) could compensate for the lack of access to public religious practices during the lockdown and promote satisfaction with life during the pandemic. Hence, it is important for religious institutions to promote virtual or private religious practice through online platforms. Because being older appears to be a protective factor against stress among participants in our study, the religious community could develop mentoring programs in which younger members are paired with older members to learn about wisdom in life and spiritual support. Religious leaders could also frequently remind the believers to appraise their life positively through meaning-making pathways (e.g., cultivate a gratitude mindset) and exercise meta-cognition (e.g., reflexivity) as positive coping. As most of the believers perceived personal behavioral coping and cognitive adjustment to be helpful during the pandemic, integrating spiritual resources into self-care habits and mindset restructuring would be another strategy to sustain their mental health. Mental health practitioners could also assess different cognitive styles and coping strategies privileged by their religious clients before providing culturally relevant and appropriate interventions, either through cognitive restructuring or behavioral intervention.
Limitations and future direction
While our findings are predominantly aligned with the literature and effort was taken to control for confounding variables such as age, a more rigorous design in future studies would clarify further the proposed mechanism of religious coping. As both studies in the current article relied on cross-sectional data, cause-and-effect relationships between religiosity and psychological outcomes could not be established. Future studies could utilize longitudinal designs where participants provide repeated measurements over a period of time. This would allow us to more accurately capture the pandemic’s effect on the association between religiosity and well-being and, more importantly, the sustainability of reliance on religious practices in well-being regulation.
Another limitation was the use of convenience and snowball sampling, which may limit the generalizability of the findings. For instance, the participants were mostly Malaysian Chinese in ethnicity, with more than half of the participants growing up in urban areas. This limits the generalizability regarding Muslims, who comprised only 15.6% of the participants in Study 1 and 24.5% of those in Study 2. Undeniably, the intersectionality between religious identity and ethnic identity creates an interesting complexity in the spectrum of rationality. However it is impossible to separate a certain religion (such as Islam) from the ethnic group (Malay) in Malaysia. Hence, we could only interpret the religious differences through the lens of “cultural intersectionality” to account for potential ethnic variances. The use of only English-fluent participants in the study would also be a biased sample because it would exclude non-English-speaking believers. Moreover, the measurement of religiosity (DUREL) may not fully capture the religious practice of Buddhism in Southeast Asia, which is non-monotheistic and less institutionalized than elsewhere. Future studies could be conducted in multilingual surveys consistent with culturally adapted and validated measurements. Lastly, in the qualitative study, the authors’ ethnicity/religious background might have resulted in cultural blind spots in the interpretation of results as the first author is a second-generation Chinese Christian, the second author agnostic and not religious, and the third author a second-generation Chinese Buddhist.
Conclusion
Our mixed-method study affirms that the protective role of religion in psychological well-being during the COVID-19 pandemic appears to be driven predominantly by public and private religious practices rather than internal religiosity or religious group identity. The religious groups differed in their religious rationality and levels of religiosity, but psychological well-being during the COVID-19 pandemic did not vary by religious groups. These findings contribute to the literature on the psychology of religion by highlighting the different pathways of religious coping during pandemic exposure and the mental health implications on stress management and life satisfaction. Future studies could continue to explore the underlying religious mechanism in non-West countries through ecological rationality theory.
Notes
A post hoc analysis was run to test the role of religiosity and age as parallel mediators of the association between religious groups and perceived stress. Results revealed significant indirect effects through age and not religiosity, thus confirming our interpretation.
References
Abdel-Khalek, A. M. (2019). Religiosity and well-being. In V. Zeigler-Hill & T. Shackelford (Eds.), Encyclopedia of personality and individual differences (pp. 4407–4415). Springer, Cham. https://doi.org/10.1007/978-3-319-28099-8_2335-1
Adler, N. E., Epel, E. S., Castellazzo, G., & Ickovics, J. R. (2000). Relationship of subjective and objective social status with psychological and physiological functioning: Preliminary data in healthy white women. Health Psychology, 19(6), 586–592. https://doi.org/10.1037//0278-6133.19.6.586
Ahmad, Z. (2007). Multiculturalism and religio-ethnic plurality. Culture and Religion, 8(2), 139–153. https://doi.org/10.1080/14755610701424008
Ahmadi, F., Mohamed Hussin, N. A., & Mohammad, M. T. (2019). Religion, culture and meaning-making coping: A study among cancer patients in Malaysia. Journal of Religion and Health, 58(6), 1909–1924. https://doi.org/10.1007/s10943-018-0636-9
AlAbdulwahab, S. S., Kachanathu, S. J., & Oluseye, K. (2013). Physical activity associated with prayer regimes improves standing dynamic balance of healthy people. Journal of Physical Therapy Science, 25(12), 1565–1568. https://doi.org/10.1589/jpts.25.1565
Al-Khayat, M. H. (2004). Health as a human right in Islam. In M. H. Al-Khayat (Ed.), The right path to health: Health education through religion. World Health Organization.
Attum, B., Hafiz, S., Malik, A., & Shamoon, Z. (2022). Cultural competence in the care of Muslim patients and their families. StatPearls Publishing.
Banazadeh, N., Sabahi, A., Ziaadini, H., Jalali-Khalilabadi, A., & Banazadeh, M. (2019). The relationship between extrinsic and intrinsic religious orientation with perceived stress and cigarette addiction among university students. Addiction & Health, 11(2), 73–80. https://doi.org/10.22122/ahj.v11i2.226
Braun, V., & Clarke, V. (2006). Using thematic analysis in psychology. Qualitative Research in Psychology, 3(2), 77–101. https://doi.org/10.1191/1478088706qp063oa
Broadbent, E., Petrie, K. J., Main, J., & Weinman, J. (2006). The brief illness perception questionnaire. Journal of Psychosomatic Research, 60(6), 631–637. https://doi.org/10.1016/j.jpsychores.2005.10.020
Chau, L. L., Johnson, R. C., Bowers, J. K., Darvill, T. J., & Danko, G. P. (1990). Intrinsic and extrinsic religiosity as related to conscience, adjustment, and altruism. Personality and Individual Differences, 11(4), 397–400. https://doi.org/10.1016/0191-8869(90)90222-d
Che Rahimi, A., Bakar, R. S., & Mohd Yasin, M. A. (2021). Psychological well-being of Malaysian university students during COVID-19 pandemic: Do religiosity and religious coping matter? Healthcare, 9(11), 1535. https://doi.org/10.3390/healthcare9111535
Cohen, S., Kamarck, T., & Mermelstein, R. (1983). A global measure of perceived stress. Journal of Health and Social Behavior, 24(4), 385–396. https://doi.org/10.2307/2136404
Department of Information, Ministry of Communications and Multimedia, Malaysia. (2015). Population by states and ethnic group. Archived from the original on 12 February 2016, Retrieved April 1, 2023, from https://web.archive.org/web/20160212125740/http://pmr.penerangan.gov.my/index.php/info-terkini/19463-unjuran-populasi-penduduk-2015.html
Department of Statistics Malaysia. (2022). Population and housing census of Malaysia 2020. Retrieved April 1, 2023, from https://www.dosm.gov.my/v1/index.php?r=column/cthemeByCat&cat=117&bul_id=akliVWdIa2g3Y2VubTVSMkxmYXp1UT09&menu_id=L0pheU43NWJwRWVSZklWdzQ4TlhUUT09
Diener, E., Emmons, R. A., Larsen, R. J., & Griffin, S. (1985). The Satisfaction with Life Scale. Journal of Personality Assessment, 49(1), 71–75. https://doi.org/10.1207/s15327752jpa4901_13
Granovetter, M. S. (1973). The strength of weak ties. American Journal of Sociology, 78(6), 1360–1380. Retrieved August 27, 2022, from http://www.jstor.org/stable/2776392
Hayes, A. F. (2022). Introduction to mediation, moderation, and conditional process analysis: A regression-based approach (3rd ed.). Guilford Press.
Hill, C. E., Thompson, B. J., & Williams, E. N. (1997). A guide to conducting consensual qualitative research. The Counseling Psychologist, 25(4), 517–572. https://doi.org/10.1177/0011000097254001
Hofstede, G. (1980). Culture’s consequences. Sage.
Khodaveirdyzadeh, R., Rahimi, R., Rahmani, A., Ghahramanian, A., Kodayari, N., & Eivazi, J. (2016). Spiritual/religious coping strategies and their relationship with illness adjustment among Iranian breast cancer patients. Asian Pacific Journal of Cancer Prevention, 17(8), 4095–4099. Retrieved September 6, 2022, from https://pubmed.ncbi.nlm.nih.gov/27644667/
Koenig, H. G., & Büssing, A. (2010). The Duke University Religion Index (DUREL): A five-item measure for use in epidemiological studies. Religions, 1(1), 78–85. https://doi.org/10.3390/rel1010078
Krägeloh, C. U., Chai, P. P., Shepherd, D., & Billington, R. (2012). How religious coping is used relative to other coping strategies depends on the individual’s level of religiosity and spirituality. Journal of Religion and Health, 51(4), 1137–1151. https://doi.org/10.1007/s10943-010-9416-x
Kroenke, K., Spitzer, R. L., & Williams, J. B. W. (2001). The PHQ-9. Journal of General Internal Medicine, 16(9), 606–613. https://doi.org/10.1046/j.1525-1497.2001.016009606.x
Leventhal, H., Leventhal, E. A., & Contrada, R. J. (1998). Self-regulation, health, and behavior: A perceptual-cognitive approach. Psychology and Health, 13(4), 717–733. https://doi.org/10.1080/08870449808407425
Liu, C. H., Zhang, E., Wong, G. T. F., Hyun, S., & Hahm, H. C. (2020). Factors associated with depression, anxiety, and PTSD symptomatology during the COVID-19 pandemic: Clinical implications for U.S. young adult mental health. Psychiatry Research, 290, 113172. https://doi.org/10.1016/j.psychres.2020.113172
Milstein, G., Palitsky, R., & Cuevas, A. (2019). The religion variable in community health promotion and illness prevention. Journal of Prevention & Intervention in the Community, 48(1), 1–6. https://doi.org/10.1080/10852352.2019.1617519
Morse, J. M. (2015). Critical analysis of strategies for determining rigor in qualitative inquiry. Qualitative Health Research, 25(9), 1212–1222. https://doi.org/10.1177/1049732315588501
Oman, D., & Syme, S. L. (2018). Weighing the evidence: What is revealed by 100+ meta-analyses and systematic reviews of religion/spirituality and health? In D. Oman (Ed.), Why religion and spirituality matter for public health (pp. 261–281). Springer, Cham. https://doi.org/10.1007/978-3-319-73966-3_15
Organisation for Economic Co-operation and Development. (2020, June 11). Youth and COVID-19: Response, recovery and resilience. https://read.oecd-ilibrary.org/view/?ref=134_134356-ud5kox3g26&title=Youth-and-COVID-19-Response-Recovery-and-Resilience
Pargament, K. I., Koenig, H. G., & Perez, L. M. (2000). The many methods of religious coping: Development and initial validation of the RCOPE. Journal of Clinical Psychology, 56(4), 519–543. https://doi.org/10.1002/(sici)1097-4679(200004)56:4%3c519::aid-jclp6%3e3.0.co;2-1
Patton, M. Q. (1990). Qualitative evaluation and research methods. SAGE.
Pavot, W., & Diener, E. (1993). Review of the Satisfaction with Life Scale. Psychological Assessment, 5(2), 164–172. https://doi.org/10.1037/1040-3590.5.2.164
Religion of Islam, The. (2009, January 25). Moral system of Islam (part 1 of 2): The standard of morality. https://www.islamreligion.com/articles/1174/moral-system-of-islam-part-1/
Roger, K. S., & Hatala, A. (2018). Religion, spirituality & chronic illness: A scoping review and implications for health care practitioners. Journal of Religion & Spirituality in Social Work: Social Thought, 37(1), 24–44. https://doi.org/10.1080/15426432.2017.1386151
Rosmarin, D. H., Wachholtz, A., & Ai, A. (2011). Beyond descriptive research: Advancing the study of spirituality and health. Journal of Behavioral Medicine, 34(6), 409–413. https://doi.org/10.1007/s10865-011-9370-4
Samuels, J. (2016). Contemporary Buddhism in Malaysia. In M. Jerryson (Ed.), The Oxford handbook of contemporary Buddhism (pp. 258–273). Oxford University Press. https://doi.org/10.1093/oxfordhb/9780199362387.013.1
Samuri, M. A. A., & Quraishi, M. (2014). Negotiating apostasy: Applying to “leave Islam” in Malaysia. Islam and Christian-Muslim Relations, 25(4), 507–523. https://doi.org/10.1080/09596410.2014.907054
Scheer, C., & Jansen, P. (2018). Greater happiness through music practice. Journal of Psychology & Psychotherapy. https://doi.org/10.4172/2161-0487-c1-024
Schulz, J. F., Bahrami-Rad, D., Beauchamp, J. P., & Henrich, J. (2019). The church, intensive kinship, and global psychological variation. Science, 366(6466), eaau5141. https://doi.org/10.1126/science.aau5141
Shaw, T., Ishak, D., Lie, D., Menon, S., Courtney, E., Li, S.-T., & Ngeow, J. (2018). The influence of Malay cultural beliefs on breast cancer screening and genetic testing: A focus group study. Psycho-Oncology, 27(12), 2855–2861. https://doi.org/10.1002/pon.4902
Spitzenstätter, D., & Schnell, T. (2020). The existential dimension of the pandemic: Death attitudes, personal worldview, and coronavirus anxiety. Death Studies, 46(5), 1031–1041. https://doi.org/10.1080/07481187.2020.1848944
Steffen, P. R., Masters, K. S., & Baldwin, S. (2017). What mediates the relationship between religious service attendance and aspects of well-being? Journal of Religion and Health, 56(1), 158–170. https://doi.org/10.1007/s10943-016-0203-1
Sundararajan, L. (2011). Spiritual transformation and emotion: A semiotic analysis. Journal of Spirituality in Mental Health, 13(1), 78–90. https://doi.org/10.1080/19349637.2011.547141
Sundararajan, L. (2020). Strong-ties and weak-ties rationalities: Toward an expanded network theory. Review of General Psychology, 24(2), 134–143. https://doi.org/10.1177/1089268020916438
Sundararajan, L., Ting, R.S.-K., Hsieh, S.-K., & Kim, S.-H. (2022). Religion, cognition, and emotion: What can automated text analysis tell us about culture? The Humanistic Psychologist, 50(2), 213–233. https://doi.org/10.1037/hum0000201
Tan, M. M., Su, T. T., Ting, R.S.-K., Allotey, P., & Reidpath, D. (2020). Religion and mental health among older adults: Ethnic differences in Malaysia. Aging & Mental Health, 25(11), 2116–2123. https://doi.org/10.1080/13607863.2020.1799939
Tang, C. P. (2015). The diversity of Malaysian Chinese Buddhism. Journal of Chinese Literature and Culture, 3(2), 32–50. Retrieved August 20, 2022, from https://ejournal.um.edu.my/index.php/JCLC/article/view/13205
Thomas, J., & Barbato, M. (2020). Positive religious coping and mental health among Christians and Muslims in response to the COVID-19 pandemic. Religions, 11(10), 498. https://doi.org/10.3390/rel11100498
Thong, J.J.-A., Ting, R.S.-K., Jobson, L., & Sundararajan, L. (2023). In the wake of religious conversions: Differences in cognition and emotion across three religious communities of an indigenous tribe in Malaysia. Advance online publication. https://doi.org/10.1037/rel0000493
Ting, R.S.-K., & Ng, A. L. O. (2012). Use of religious resources in psychotherapy from a tradition-sensitive approach: Cases from Chinese in Malaysia. Pastoral Psychology, 61(5–6), 941–957. https://doi.org/10.1007/s11089-011-0365-4
Ting, R.S.-K., Aw Yong, Y.-Y., Tan, M.-M., & Yap, C.-K. (2021). Cultural responses to Covid-19 pandemic: Religions, illness perception, and perceived stress. Frontiers in Psychology, 12, 634863. https://doi.org/10.3389/fpsyg.2021.634863
Ting, R.S.-K., & Sundararajan, L. (2018). Culture, cognition, and emotion in China’s religious ethnic minorities: Voices of suffering among the Yi. Palgrave Macmillan. https://doi.org/10.1007/978-3-319-66059-2
Toffalini, E., Veltri, A., & Cornoldi, C. (2014). Metacognitive aspects influence subjective well-being in parents of children with cancer. Psycho-Oncology, 24(2), 175–180. https://doi.org/10.1002/pon.3622
Tomaszek, K., & Muchacka-Cymerman, A. (2020). Thinking about my existence during COVID-19, I feel anxiety and awe—The mediating role of existential anxiety and life satisfaction on the relationship between PTSD symptoms and post-traumatic growth. International Journal of Environmental Research and Public Health, 17(19), 7062. https://doi.org/10.3390/ijerph17197062
Van Tongeren, D. R., & Showalter Van Tongeren, S. A. (2021). Finding meaning amidst COVID-19: An existential positive psychology model of suffering. Frontiers in Psychology, 12, 641747. https://doi.org/10.3389/fpsyg.2021.641747
Vaughn, P., & Turner, C. (2016). Decoding via coding: Analyzing qualitative text data through thematic coding and survey methodologies. Journal of Library Administration, 56(1), 41–51. https://doi.org/10.1080/01930826.2015.1105035
Villani, D., Sorgente, A., Iannello, P., & Antonietti, A. (2019). The role of spirituality and religiosity in subjective well-being of individuals with different religious status. Frontiers in Psychology, 10, 1525. https://doi.org/10.3389/fpsyg.2019.01525
Wangchuk, P. (2021). Humankind’s existential crisis amid COVID-19 pandemic: A theoretical perspective. Asian Journal of Education and Social Studies, 20(1), 1–9. https://doi.org/10.9734/ajess/2021/v20i130474
Weber, S. R., & Pargament, K. I. (2014). The role of religion and spirituality in mental health. Current Opinion in Psychiatry, 27(5), 358–363. https://doi.org/10.1097/yco.0000000000000080
Yap, C. K., Ting, R. S.-K., Tan, N. L.-T., Yue Yun, A. Y., & Tan, M-M. (2022). Religion, illness perception and coping in pandemics: A systematic review. In R. W. Hood Jr., & S. Cheruvallil-Contractor (Eds.), Research in the social scientific study of religion, volume 32: Lesser heard voices in studies of religion (pp. 427–468). Brill. Retrieved August 20, 2022, from https://brill.com/view/title/61509
Yıldırım, M., & Arslan, G. (2021). A moderated mediation effect of stress-related growth and meaning in life in the association between coronavirus suffering and satisfaction with life: Development of the stress-related growth measure. Frontiers in Psychology, 12, 648236. https://doi.org/10.3389/fpsyg.2021.648236
Zhang, M., Hong, L., Zhang, T., Lin, Y., Zheng, S., Zhou, X., Fan, R., Wang, Z., Zhang, C., & Zhong, J. (2016). Illness perceptions and stress: Mediators between disease severity and psychological well-being and quality of life among patients with Crohn’s disease. Patient Preference and Adherence, 10, 2387–2396. https://doi.org/10.2147/PPA.S118413
Acknowledgements
We would like to thank research assistants Aw Yong Yue-Yun, Choong Min-Jun, and other Culture and Health Lab volunteers in data collection and coding..
Funding
Open Access funding enabled and organized by CAUL and its Member Institutions.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ting, R.SK., Goh, P.H. & Ong, E.ZM. A Mixed-Methods Study on Religiosity, Pandemic Beliefs, and Psychological Well-Being During the COVID-19 Pandemic in Malaysia. Pastoral Psychol 73, 107–132 (2024). https://doi.org/10.1007/s11089-023-01080-0
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11089-023-01080-0