
Abstract
Purpose
Glioblastomas (GBM) with subventricular zone (SVZ) contact have previously been associated with a specific epigenetic fingerprint. We aim to validate a reported bulk methylation signature to determine SVZ contact.
Methods
Methylation array analysis was performed on IDHwt GBM patients treated at our institution. The v11b4 classifier was used to ensure the inclusion of only receptor tyrosine kinase (RTK) I, II, and mesenchymal (MES) subtypes. Methylation-based assignment (SVZM ±) was performed using hierarchical cluster analysis. Magnetic resonance imaging (MRI) (T1ce) was independently reviewed for SVZ contact by three experienced readers.
Results
Sixty-five of 70 samples were classified as RTK I, II, and MES. Full T1ce MRI-based rater consensus was observed in 54 cases, which were retained for further analysis. Epigenetic SVZM classification and SVZ were strongly associated (OR: 15.0, p = 0.003). Thirteen of fourteen differential CpGs were located in the previously described differentially methylated LRBA/MAB21L2 locus. SVZ + tumors were linked to shorter OS (hazard ratio (HR): 3.80, p = 0.02) than SVZM + at earlier time points (time-dependency of SVZM, p < 0.05). Considering the SVZ consensus as the ground truth, SVZM classification yields a sensitivity of 96.6%, specificity of 36.0%, positive predictive value (PPV) of 63.6%, and negative predictive value (NPV) of 90.0%.
Conclusion
Herein, we validated the specific epigenetic signature in GBM in the vicinity of the SVZ and highlighted the importance of methylation of a part of the LRBA/MAB21L2 gene locus. Whether SVZM can replace MRI-based SVZ assignment as a prognostic and diagnostic tool will require prospective studies of large, homogeneous cohorts.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Glioblastoma (GBM) is the most common malignant primary brain tumor in adults [1]. Despite trimodal treatment consisting of surgery, radiotherapy, and chemotherapy, the prognosis remains poor [2]. GBM may originate from self-renewing tumorigenic cancer stem cells (CSC) that rely on signals from their cellular milieu to maintain stem cell properties [3]. The subventricular zone (SVZ) is the most abundant location for neuronal stem cells (NSC) lining the lateral ventricles. It is actively involved in neurogenesis and may contribute to tumorigenesis in GBM. Tumors in this location may maintain a distinct immunosuppressed microenvironment [4,5,6,7]. A clonal relationship exists between driver mutations in SVZ tissue and GBM tissue, providing possible evidence that SVZ NSCs could be the cell of origin [5, 6, 8]. DNA methylation analysis has improved the molecular characterization of central nervous system tumors and led to the discovery of further tumor entities [9, 10]. GBM with SVZ contact might show a distinct molecular signature as they are closely related to a stem cell-rich zone that can also harbor GBM stem cells [3, 6, 11, 12]. Consequently, DNA methylation analysis and characterization could be important in understanding the role of the SVZ in GBM formation, self-renewal, and therapy resistance. A specific methylation signature recently reported distinguishes between GBM with and without SVZ involvement in isocitrate dehydrogenase (IDH) wild type (IDHwt) GBM, an approach that has the potential to improve patient risk stratification and to individualize future patient care [12, 13]. This study aimed to validate the accuracy and usefulness of a DNA methylation-based SVZ classifier (SVZM).
Methods
Methylation array analysis of IDHwt GBM patients treated at our institution was performed with Illumina Infinium Methylation 850 k profiling arrays (Illumina Inc., San Diego, CA, USA). Further classification of methylation profiles was done using the v11b4 classifier from the German Cancer Research Center (DKFZ, Heidelberg, Germany). Only receptor tyrosine kinase (RTK) I, II, and mesenchymal (MES) GBM subtypes were included. Treatment, molecular, and histopathological data were obtained from the patients’ medical records and institutional databases. Preoperative magnetic resonance imaging (MRI) was independently reviewed by three experienced readers, two neuroradiologists, and one radiation oncologist (JK, CCS, FE), who assessed GBM SVZ contact on T1-weighted contrast-enhanced MRI (T1ce) scored as a binary variable (SVZ contact [SVZ +] vs. no contact [SVZ-]). Readers were mutually blinded to each other's assessments. Tumor contact with the SVZ was defined as T1ce tumor lesions being present within a 5 mm area adjacent to the lateral ventricles. Patients were labeled as SVZ + or SVZ- when all three readers unanimously agreed on the SVZ contact assessment, and only these samples were retained for subsequent analysis. Contrast-enhancing tumor lesion volume on T1ce and the shortest distance from the outline of the contrast-enhancing GBM to the SVZ were assessed in the EclipseTM treatment planning system (Varian Medical Systems Inc., Palo Alto, CA, USA). A consensual SVZ contact assessment based on MRI was used to validate the SVZM signature [12]. Methylation data was analyzed using the minfi package in R [14]. Idat files were normalized using minfis’ preprocessFunnorm() function, subsequent analyses were performed with M-values (log2 ratio of the methylated versus unmethylated probe intensities). As previously described, the 15 CpG SVZM signature was used to assign samples using hierarchical cluster analysis (Euclidean distance, average linkage) by identifying two main clusters [12]. Manual comparison of overall cluster methylation patterns and of mean methylation of the 15 CpG signature was used to define clusters as SVZM + and SVZM- (Suppl. Fig. 1). Differential methylation between SVZM ± samples was tested using the tTest function from the dataAnalysisMisc package. P-values were adjusted for multiplicity using the Bonferroni method [15]. We used a significance level α of 0.05. We compared the molecular SVZM signature to our consensual T1ce SVZ assessment using Fisher’s exact test, and calculated sensitivity, specificity, positive predictive value (PPV), and negative predictive values (NPV).
Overall survival (OS) was calculated from the date of surgery to the date of death by any cause. Progression-free survival (PFS) was calculated from the date of surgery to tumor progression determined by MRI or death by any reason. Censoring for OS and PFS occurred without prespecified events at the last available follow-up. Univariable analyses were performed with Cox-PH models (survival package) [16]. The proportionality assumption was evaluated visually for identity (time), log(time), and log(time + offset) (offset: = 10) transformations (Suppl. Fig. 2), and tested using the cox.zph function. For time-dependent coefficients, we used the time-transform (tt) functionality in Cox models. This study was approved by the local institutional review board (EA1/061/22).
Results
Patient characteristics
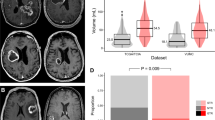
We identified and analyzed 70 IDHwt GBM patients that underwent treatment between 2006 and 2021. Sixty-five of the samples were classified as MES (n = 23)/RTK I (n = 16)/RTK II (n = 26) GBM using the brain tumor classifier v11b4, and only these were retained for subsequent analysis [10]. In 54 of 65 cases (83.1%), all three independent viewers unanimously agreed on either contact or no contact with the SVZ (Fig. 1A-B). Eleven cases (16.9%) without agreement (Fig. 1C) were excluded from the analysis. Baseline characteristics for the 54 included patients are shown in Table 1.

Representative axial T1ce MRI for SVZ contact assessment and three examples. A SVZ + , B SVZ-, and (C) missing consensus amongst readers. SVZ = green, GBM = red
Thirty-two patients had gross total resections (59.3%), six subtotal resections (11.1%), and 16 a biopsy (29.6%). Thirty-nine patients (72.2%) underwent radiochemotherapy, and 41 patients (75.9%) received chemotherapy with temozolomide (TMZ). Median contrast-enhancing tumor volume was 22.9 cm3 (range: 0.1 cm3 to 114.6 cm3). GBM were mainly located in the frontal (17 patients, 31.5%), followed by temporal (twelve patients, 22.2%), and parietal lobes (five patients, 9.3%). Fourteen patients (25.9%) had multifocal disease at diagnosis. Twenty-two (40.7%) tumors showed O6-methylguanine-DNA-methyltransferase (MGMT) promoter methylation.
Image and methylation-based classification
Twenty-nine cases (53.7%) were classified as SVZ + , and 25 (46.3%) cases as SVZ-. Patients with SVZ + assigned tumors showed larger contrast-enhancing tumor volume (median 51.8 vs. 5.5 cm3) and a higher fraction of Karnofsky performance status (KPS) < 80% (n = 7, 24.1% vs n = 3, 12.0%), MGMT promoter methylation was less common (n = 9, 31.0% vs. n = 13, 52.0%). Figure 2. shows the hierarchical clustering of M-values of the previously reported 15 CpG SVZM signature used for SVZM classification. The proportion of SVZ ± samples was balanced (n = 29, 53.7% vs n = 25, 46.2%). Considering SVZM, only 18.5% (n = 10) of samples were classified as SVZM-.

Clustering of the 15 CpG signature SVZM versus T1ce MRI assessment. M-values visualized as blue/hypomethylated (-6) to red/hypermethylated (+ 6). The columns represent one patient assigned to the SVZM + or SVZM- based on hierarchical clustering. Each row depicts a CpG
Fisher’s exact test indicated a strong association between MRI-based SVZ classification and SVZM with an odds ratio (OR) of 15.0 (95% confidence interval (CI): 1.8–711.5, p = 0.003) (Fig. 3). This corresponds to 28 true positives (TP), 16 false positives (FP), one false negative (FN), and nine true negatives (TN) if consensus SVZ classification is considered the ground truth. This leads to a sensitivity of 96.6%, specificity of 36.0%, PPV of 63.6%, and NPV of 90.0% for SVZM.

Identification of the patient cohort and SVZ/SVZM results. Fishers’ exact test indicated a strong association between MRI-based SVZ classification and SVZM with an odds ratio (OR) of 15.0 (95% CI: 1.8–711.5, p = 0.003)
We further assessed which CpGs are most strongly correlated with SVZ/SVZM assignment. We found no CpGs associated with SVZ for a conservative p-value adjustment but 14 CpGs associated with SVZM. Thirteen out of these 14 CpGs were located on the LRBA/MAB21L2 locus, including all 4 LRBA/MAB21L2 CpGs from the 15 CpG signature (Suppl. Fig. 3). This underlines the role of the LRBA/MAB21L2 locus on chr 4 (pos 151,502,935–151,505,084; hg19) for the classification signature.
Prognostic value of SVZ and SVZM
We evaluated the prognostic value of SVZ and SVZM for OS in univariable analyses (Fig. 4). We observed non-proportionality of hazards for SVZM but not for SVZ (Suppl. Fig. 2), indicating a time-dependency of hazards. Patients with SVZ + consensus-classified tumors had shorter survival times (hazard ratio (HR) 3.80 [1.23–11.75], p = 0.02) than patients with SVZM + classified tumors (SVZM + : HR 7.45 [1.23–45.20], p = 0.03), especially at earlier time points (tt(SVZM +): 0.89 [0.80–0.98], p = 0.01). Median OS was comparable for SVZ + (12.6 months, 95% CI [7.18–17.5]) and SVZM + (13.0 months, 95% CI [8.59–17.9]). At two years, no patients from the SVZ + group (0%, 95%CI [0–11.7]) and two patients (4.5%, 95% CI [0.13–15.14]) from the SVZM + group were still alive (trend towards a better separation of SVZ +). Next, we performed a univariable analysis of PFS (Suppl. Fig. 4). For SVZ, no prognostic separation could be observed, for SVZM- patients, a tendency towards longer PFS was observed (p = 0.09).

a Overall survival stratified by SVZ contact, b Overall survival stratified by the methylation-based signature
Discussion
Herein, we report the validation results of a previously established methylation-based signature for SVZ contact of GBM [12]. To our knowledge, this is the first attempt to validate the reported SVZ methylation signature. The first step to verify the molecular classifier was the imaging assessment of SVZ contact. We chose a multi-reader, interdisciplinary approach to reduce misclassification biases. However, eleven cases (16.9%) had no agreement on SVZ contact. This is partly due to the definition of the SVZ, which, while formally standardized, still holds the potential for differing interpretation. Precise measurement is crucial as only a few millimeters differences can determine SVZ contact. Adeberg et al. also experienced a variability of 38% in the validation process of their findings [12]. However, only one rater assessed the imaging at three different time points, indicating an intraobserver variability in contrast to our interobserver variability. Such differences in MRI-based GBM SVZ contact assessment have been previously described, but the clinical implications are still ambiguous and need further clarification [13, 17].
In the neuroradiological assessment of high-grade gliomas usually two- or even three neuroradiologists assess the available imaging and find a consensus on tumor location and its spatial extension. This helps to improve the accuracy, consistency, and reliability of radiological assessment of gliomas. In addition, advanced imaging techniques such as diffusion tensor imaging, perfusion-weighted imaging, magnetic resonance spectroscopy, and positron emission tomography-computed tomography are becoming more regularly used. They can provide additional information about the spatial configuration of tumors [18]. Nevertheless, more precise and reliable methods are necessary to determine SVZ contact, given its potential role for risk stratification and future individualization of patient care [13, 19].
Next, we validated a previously described methylation-based signature to determine the tumors’ SVZ involvement and its role for OS [12]. The association between the MRI T1ce imaging rater assessment and SVZM was solid, with the signature showing a considerable performance concerning sensitivity and NPV. Moreover, the OS was reduced for T1-ce SVZ + and SVZM + compared to T1ce SVZ- and SVZM-. For methylation-based classification, we observed a prognostic separation, especially within the first year following diagnosis. Median OS was comparable between SVZ + (12.6 months) and SVZM + (13.0 months), hinting towards comparable prognostic separation. Consensus SVZ classification was time-independent – in contrast to SVZM – and thus conferred a more robust readout for this cohort. One can speculate that the close connection to the SVZ is indeed what enables these GBM to present such aggressive phenotypes. Besides, the SVZM signature yielded a high sensitivity and NPV, underlining the potential to utilize it as a screening tool for SVZ contact and to confirm the absence of it in case of corresponding imaging findings.
In our cohort, SVZM classified 81% of tumors as SVZ-associated, whereas in the original study, SVZM positive and negative GBM were equally distributed [12]. In most published studies that concentrate on MRI-based SVZ definition, the proportions of participants belonging to the SVZ-positive and SVZ-negative groups were relatively comparable, ranging from 54 to 70% [20, 21]. Barami et al. mentioned that 93 out of 100 of low- to high-grade glioma patients (53 GBM) had shown contact with the lateral ventricular wall based on MRI [22]. It is worth noting that in these studies, the criterion for defining SVZ contact was based on lateral contact with the lateral ventricles rather than contact with a 5 mm margin adjacent to the lateral ventricles. However, our findings suggest that a substantial proportion of GBM might be associated with the SVZ, with the limitation of potential sampling biases.
Adeberg et al. described an “epigenetic and transcriptional silencing of MAB21L2/LRBA in SVZM + tumors “, possibly resulting in transforming growth factor β activity and a dysregulated immune response. We were able to confirm the LRBA/BA21L2 locus as an important component of the SVZM signature. Adeberg et al. also noted a hypomethylation resulting in increased gene expression for 90% of the CpG that defines SVZM + [12]. It must be noted that some authors have reported that SVZ contact is not associated with any molecular signature, including methylation, while other authors have suggested specific changes in gene expression levels of GBMs with SVZ contact [23, 24]. Furthermore, a relationship may exist between driver mutations in both the healthy SVZ tissue and tumor tissue, suggesting that SVZ NSCs might be the source of GBM [6, 8]. Another area of interest is the role of cerebrospinal fluid (CSF) in GBM formation. As the SVZ is located close to the cerebrospinal fluid compartment, tumors contacting the SVZ could experience changes in their microenvironment and hence develop an altered methylation status. CSF has been shown to promote tumorigenic capacities in vitro and tumor growth in vivo and to cause transcriptomic changes in human GBM, leading to higher malignancy [25]. The altered DNA methylation signature in SVZ + tumors could possibly be connected to CSF exposure.
In our patient cohort, we noted that SVZ involvement was accompanied by a trend of larger tumor volume, worse KPS, and a higher incidence of multifocal tumor spread, which may all have negative implications for the observed OS (Suppl. Fig. 5). A plausible explanation for this observation is that larger tumors have a higher likelihood of contacting a specific area, in our case, the SVZ. Furthermore, the feasibility of surgical removal is hampered in large tumors where critical structures are more likely to be involved, which in turn results in worse performance status. Finally, infiltration of the ventricles is another factor that may occur in cases with SVZ contact, potentially exerting a negative influence on survival.
In our cohort, tumors with MRI-based SVZ involvement had a higher likelihood of presenting as multifocal at the date of diagnosis. This observation was also made by Lim et al., where 40% of SVZ-associated GBM presented as multifocal compared to 14% in the SVZ- group. Ahmadipour et al. showed similar results in their cohort in which 49% of SVZ + GBM were multifocal compared to 18% in the SVZ- group [26, 27]. Various studies have assessed the role of SVZ contact as a prognostic factor, with many of them confirming its negative association with survival [13, 28, 29].
DNA methylation analysis and the use of large-scale methylation arrays have enabled the classification of CNS tumors into different subtypes [10]. There is an ongoing search for genetic and epigenetic signatures that can help us to further understand the complex mechanisms involved in GBM formation. The described DNA methylome-based classifier of SVZ contact may be a valuable asset to improve diagnostic accuracy and patient stratification. This validation analysis provides further evidence on the potential utility of methylation signatures to improve patient and tumor stratification. Nevertheless, further evaluation with a higher number of patients who clearly show no signs of radiological SVZ involvement is needed to further validate its prognostic role.
This work has some limitations that should be considered when interpreting the results. The low number of cases that show no signs of SVZ involvement limits the generalizability of our findings. Multivariable analysis was limited due to the small number of patients and events. A much larger and more homogeneous patient population with balanced baseline characteristics and prospective study design is warranted to ultimately determine the validity of the DNA methylation-assisted classification of SVZ involvement in GBM. Finally, future research should also investigate ways to improve and tweak the SVZ signature given the potential for further refinement.
Conclusion
The reported and tested DNA methylation-based SVZ signature could become a valuable tool in advancing the molecularly and spatial characterization of GBM and may reduce inter- and intraobserver variability in the assessment of SVZ involvement. Its value as a prognostic marker warrants further studies with larger and more homogenous patient cohorts.
Data availability
The datasets generated and analyzed during the current study are not publicly available.
References
Ostrom QT et al (2022) CBTRUS statistical report: primary brain and other central nervous system tumors diagnosed in the United States in 2015–2019. Neuro-Oncology 24(Supplement_5):v1–v95
Weller M et al (2021) EANO guidelines on the diagnosis and treatment of diffuse gliomas of adulthood. Nat Rev Clin Oncol 18(3):170–186
Lathia JD et al (2015) Cancer stem cells in glioblastoma. Genes Dev 29(12):1203–1217
Lim DA, Alvarez-Buylla A (2016) The adult ventricular-subventricular zone (V-SVZ) and olfactory bulb (OB) neurogenesis. Cold Spring Harb Perspect Biol 8(5):a018820
Altmann C, Keller S, Schmidt MHH (2019) The role of SVZ stem cells in glioblastoma. Cancers 11(4):448
Lee JH et al (2018) Human glioblastoma arises from subventricular zone cells with low-level driver mutations. Nature 560(7717):243–247
Bartkowiak T et al (2023) An immunosuppressed microenvironment distinguishes lateral ventricle-contacting glioblastomas. JCI Insight 8(12):e160652
Sanai N, Alvarez-Buylla A, Berger MS (2005) Neural stem cells and the origin of gliomas. N Engl J Med 353(8):811–822
Louis DN et al (2021) The 2021 WHO classification of tumors of the central nervous system: a summary. Neuro Oncol 23(8):1231–1251
Capper D et al (2018) DNA methylation-based classification of central nervous system tumours. Nature 555(7697):469–474
Hira VVV et al (2021) Immunohistochemical detection of neural stem cells and glioblastoma stem cells in the subventricular zone of glioblastoma patients. J Histochem Cytochem 69(5):349–364
Adeberg S et al (2022) DNA-methylome-assisted classification of patients with poor prognostic subventricular zone associated IDH-wildtype glioblastoma. Acta Neuropathol 144(1):129–142
Mistry AM (2019) Clinical correlates of subventricular zone-contacting glioblastomas: a meta-analysis. J Neurosurg Sci 63(5):581–587
Aryee MJ et al (2014) Minfi: a flexible and comprehensive bioconductor package for the analysis of infinium DNA methylation microarrays. Bioinformatics 30(10):1363–1369
Knoll M (2020) DataAnalysisMisc: collection of functions for daily tasks. In: R package version 0.99.11
Therneau T, Grambsch P (2000) Modeling survival data: extending the cox model. Springer, New York
Kerkhof M et al (2016) Interobserver variability in the radiological assessment of magnetic resonance imaging (MRI) including perfusion MRI in glioblastoma multiforme. Eur J Neurol 23(10):1528–1533
Thust SC et al (2018) Glioma imaging in Europe: a survey of 220 centres and recommendations for best clinical practice. Eur Radiol 28(8):3306–3317
Nourallah B et al (2017) Irradiating the subventricular zone in glioblastoma patients: is there a case for a clinical trial? Clin Oncol (R Coll Radiol) 29(1):26–33
Jafri NF, Clarke JL, Weinberg V, Barani IJ, Cha S (2013) Relationship of glioblastoma multiforme to the subventricular zone is associated with survival. Neuro Oncol 15(1):91–6
Zhao K et al (2022) The imaging features and prognosis of gliomas involving the subventricular zone: an MRI study. Clin Neurol Neurosurg 222:107465
Barami K et al (2009) Relationship of gliomas to the ventricular walls. J Clin Neurosci 16(2):195–201
Mistry AM et al (2019) Ventricular-subventricular zone contact by glioblastoma is not associated with molecular signatures in bulk tumor data. Sci Rep 9(1):1842
Lin CA et al (2017) Comparative analyses identify molecular signature of MRI-classified SVZ-associated glioblastoma. Cell Cycle 16(8):765–775
Carrano A et al (2021) Human cerebrospinal fluid modulates pathways promoting glioblastoma malignancy. Front Oncol 11:624145
Lim DA et al (2007) Relationship of glioblastoma multiforme to neural stem cell regions predicts invasive and multifocal tumor phenotype. Neuro Oncol 9(4):424–429
Ahmadipour Y et al (2020) The influence of subventricular zone involvement in extent of resection and tumor growth pattern of glioblastoma. Innov Surg Sci 5(3–4):127–132
Hallaert G et al (2020) Subventricular zone contacting glioblastoma: tumor size, molecular biological factors and patient survival. Acta Oncol 59(12):1474–1479
Bender K et al (2021) What is the role of the subventricular zone in radiotherapy of glioblastoma patients? Radiother Oncol 158:138–145
Acknowledgements
Siyer Roohani is a participant in the BIH Charité Junior Clinician Scientist Program funded by the Charité – Universitätsmedizin Berlin, and the Berlin Institute of Health at Charité (BIH).
Funding
Open Access funding enabled and organized by Projekt DEAL. This study did not receive dedicated funding.
Author information
Authors and Affiliations
Contributions
Conceptualization: DK, MK; Methodology: DK, MK; Formal analysis: FE, OZ, DK, MK; Investigation: FE, OZ, MK, DK; Writing—Original Draft: FE, OZ, DK, MK; Writing—Review & Editing: All authors; Visualization: OZ, MK; Supervision: DK.
Corresponding authors
Ethics declarations
Ethics approval
This study was approved by the local institutional review board (EA1/061/22).
Consent for publication
Not applicable due to the use of routine data.
Competing interests
The authors declare no competing interests.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary Information
Below is the link to the electronic supplementary material.
Suppl. Figure 1.:
Mean methylation of 15CpG used for SVZM ± cluster assignment. p-value: linear model analysis. (JPG 146 kb)
Suppl. Figure 2.:
Evaluation of time dependency of covariates SVZM (upper row) and SVZ (bottom row) for the following transformations: identity(time), log(time), log(time + offset), offset: = 10. Plots: estimate of the time-dependent coefficient (cox.zph); scaled Schoenfeld residuals. For proportional hazards, fits would correspond to a horizontal line. p-values calculated with cox.zph. (JPG 832 kb)
Suppl. Figure 3.:
Left: all CpGs annotated with LRBA and/or MAB21L2. Right: Differential CpGs between SVZM ± , Bonferroni adjusted p -value < 0.05, t-test. Samples ordered by mean methylation. Rows ordered by position on chromosome. (JPG 2.49 mb)
Suppl. Figure 4.: a)
Progression-free survival stratified by SVZ contact b) Progression-free survival stratified by the methylation-based signature. (JPG 5.19 mb)
Suppl. Figure 5.:
T1ce based tumor volumes depending on SVZ/SVZM assignment. Left: values ranked by volume. Right: distribution by SVZ and SVZM. In four cases volume was not measurable due to a software error. Linear model p-value (Wald type). Red: mean values, with bootstrapped confidence limits. (JPG 1.22 mb)
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cite this article
Ehret, F., Zühlke, O., Schweizer, L. et al. Validation of a methylation-based signature for subventricular zone involvement in glioblastoma. J Neurooncol 167, 89–97 (2024). https://doi.org/10.1007/s11060-024-04570-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11060-024-04570-0